
Decreased Concentration of Fibroblast Growth Factor 23 (FGF-23) as a Result of Supplementation with Selenium and Coenzyme Q10 in an Elderly Swedish Population: A Sub-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Biochemical Analyses
2.3. Determination of FGF-23
2.4. Statistical Methods
3. Results
3.1. FGF-23 and Atrial Fibrillation
3.2. FGF-23 and 10-Year Mortality
3.3. FGF-23 and Renal Function
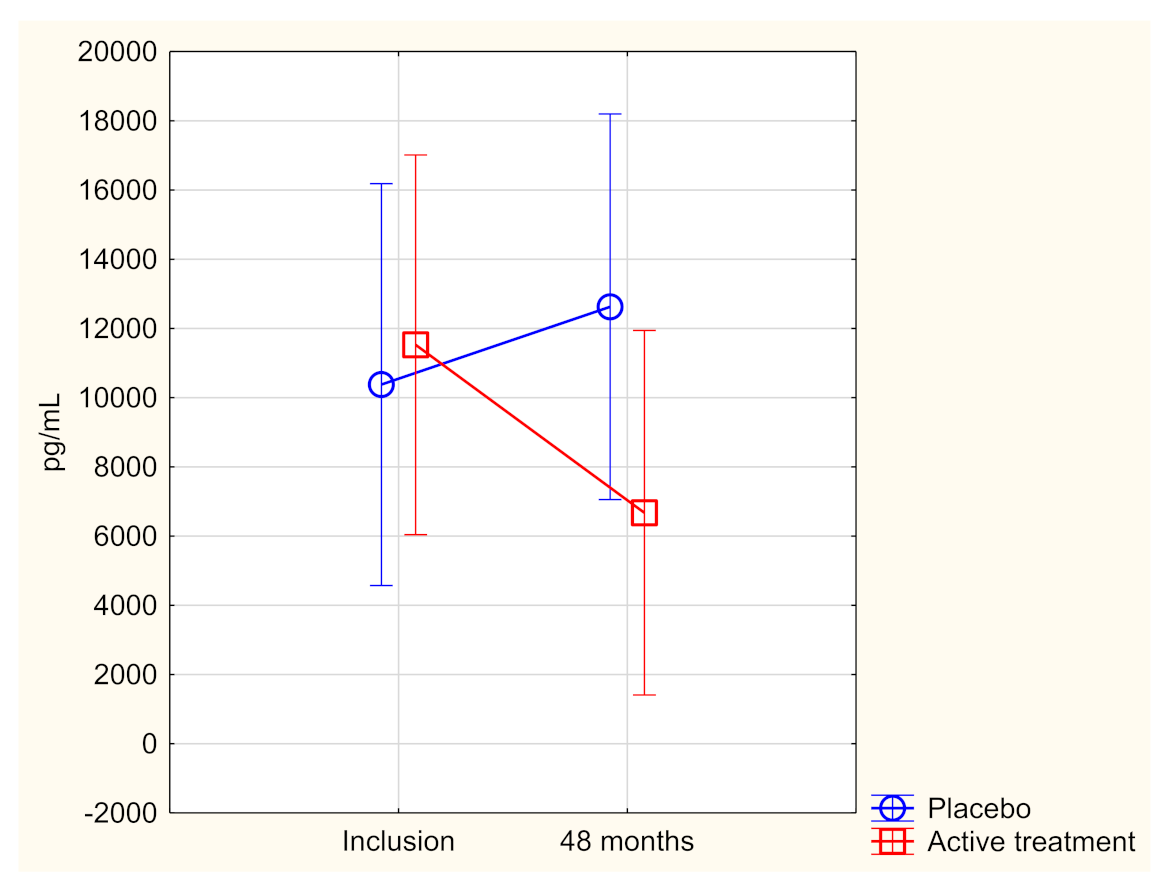
3.4. Effect of Supplementation on the Concentration of FGF-23
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACEI | ACE inhibitors |
| ANCOVA | Analysis of covariance |
| ARB | Angiotension receptor blockers |
| CRP | C-reactive protein |
| CV | Cardiovascular |
| EF | Ejection fraction |
| ECG | Electrocardiogram |
| Hs-CRP | High-sensitivity analysis of C-reactive protein |
| IHD | Ischaemic heart disease |
| NT-proBNP | N-terminal fragment of B-type natriuretic peptide |
| NYHA class | New York Heart Association functional class |
| SD | Standard deviation |
References
- Shimada, T.; Hasegawa, H.; Yamazaki, Y.; Muto, T.; Hino, R.; Takeuchi, Y.; Fujita, T.; Nakahara, K.; Fukumoto, S.; Yamashita, T. FGF-23 is a potent regulator of vitamin D metabolism and phosphate homeostasis. J. Bone Miner. Res. 2004, 19, 429–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, M.C.; Shiizaki, K.; Kuro-o, M.; Moe, O.W. Fibroblast growth factor 23 and Klotho: Physiology and pathophysiology of an endocrine network of mineral metabolism. Annu. Rev. Physiol. 2013, 75, 503–533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gutierrez, O.; Isakova, T.; Rhee, E.; Shah, A.; Holmes, J.; Collerone, G.; Juppner, H.; Wolf, M. Fibroblast growth factor-23 mitigates hyperphosphatemia but accentuates calcitriol deficiency in chronic kidney disease. J. Am. Soc. Nephrol. 2005, 16, 2205–2215. [Google Scholar] [CrossRef] [PubMed]
- Ix, J.H.; Katz, R.; Kestenbaum, B.R.; de Boer, I.H.; Chonchol, M.; Mukamal, K.J.; Rifkin, D.; Siscovick, D.S.; Sarnak, M.J.; Shlipak, M.G. Fibroblast growth factor-23 and death, heart failure, and cardiovascular events in community-living individuals: CHS (Cardiovascular Health Study). J. Am. Coll. Cardiol. 2012, 60, 200–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isakova, T.; Xie, H.; Yang, W.; Xie, D.; Anderson, A.H.; Scialla, J.; Wahl, P.; Gutierrez, O.M.; Steigerwalt, S.; He, J.; et al. Fibroblast growth factor 23 and risks of mortality and end-stage renal disease in patients with chronic kidney disease. JAMA 2011, 305, 2432–2439. [Google Scholar] [CrossRef] [Green Version]
- Wohlfahrt, P.; Melenovsky, V.; Kotrc, M.; Benes, J.; Jabor, A.; Franekova, J.; Lemaire, S.; Kautzner, J.; Jarolim, P. Association of Fibroblast Growth Factor-23 Levels and Angiotensin-Converting Enzyme Inhibition in Chronic Systolic Heart Failure. JACC Heart Fail. 2015, 3, 829–839. [Google Scholar] [CrossRef]
- Deo, R.; Katz, R.; de Boer, I.H.; Sotoodehnia, N.; Kestenbaum, B.; Mukamal, K.J.; Chonchol, M.; Sarnak, M.J.; Siscovick, D.; Shlipak, M.G.; et al. Fibroblast growth factor 23 and sudden versus non-sudden cardiac death: The Cardiovascular Health Study. Am. J. Kidney Dis. 2015, 66, 40–46. [Google Scholar] [CrossRef] [Green Version]
- Leifheit-Nestler, M.; Haffner, D. Paracrine Effects of FGF23 on the Heart. Front. Endocrinol. 2018, 9, 278. [Google Scholar] [CrossRef] [Green Version]
- Reindl, M.; Reinstadler, S.J.; Feistritzer, H.J.; Mueller, L.; Koch, C.; Mayr, A.; Theurl, M.; Kirchmair, R.; Klug, G.; Metzler, B. Fibroblast growth factor 23 as novel biomarker for early risk stratification after ST-elevation myocardial infarction. Heart 2017, 103, 856–862. [Google Scholar] [CrossRef]
- Chen, J.M.; Zhong, Y.T.; Tu, C.; Lan, J. Significance of serum fibroblast growth factor-23 and miR-208b in pathogenesis of atrial fibrillation and their relationship with prognosis. World J. Clin. Cases 2020, 8, 3458–3464. [Google Scholar] [CrossRef]
- Almahmoud, M.F.; Soliman, E.Z.; Bertoni, A.G.; Kestenbaum, B.; Katz, R.; Lima, J.A.C.; Ouyang, P.; Miller, P.E.; Michos, E.D.; Herrington, D.M. Fibroblast Growth Factor-23 and Heart Failure with Reduced Versus Preserved Ejection Fraction: MESA. J. Am. Heart Assoc. 2018, 7, e008334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roy, C.; Lejeune, S.; Slimani, A.; de Meester, C.; Ahn As, S.A.; Rousseau, M.F.; Mihaela, A.; Ginion, A.; Ferracin, B.; Pasquet, A.; et al. Fibroblast growth factor 23: A biomarker of fibrosis and prognosis in heart failure with preserved ejection fraction. ESC Heart Fail. 2020, 7, 2494–2507. [Google Scholar] [CrossRef] [PubMed]
- Koller, L.; Kleber, M.E.; Brandenburg, V.M.; Goliasch, G.; Richter, B.; Sulzgruber, P.; Scharnagl, H.; Silbernagel, G.; Grammer, T.B.; Delgado, G.; et al. Fibroblast Growth Factor 23 Is an Independent and Specific Predictor of Mortality in Patients With Heart Failure and Reduced Ejection Fraction. Circ. Heart Fail. 2015, 8, 1059–1067. [Google Scholar] [CrossRef]
- Holecki, M.; Chudek, J.; Owczarek, A.; Olszanecka-Glinianowicz, M.; Bozentowicz-Wikarek, M.; Dulawa, J.; Mossakowska, M.; Zdrojewski, T.; Skalska, A.; Wiecek, A. Inflammation but not obesity or insulin resistance is associated with increased plasma fibroblast growth factor 23 concentration in the elderly. Clin. Endocrinol. 2015, 82, 900–909. [Google Scholar] [CrossRef] [PubMed]
- Fairweather-Tait, S.J.; Bao, Y.; Broadley, M.R.; Collings, R.; Ford, D.; Hesketh, J.E.; Hurst, R. Selenium in human health and disease. Antioxid. Redox Signal. 2011, 14, 1337–1383. [Google Scholar] [CrossRef]
- Selenius, M.; Rundlof, A.K.; Olm, E.; Fernandes, A.P.; Bjornstedt, M. Selenium and the selenoprotein thioredoxin reductase in the prevention, treatment and diagnostics of cancer. Antioxid. Redox Signal. 2010, 12, 867–880. [Google Scholar] [CrossRef]
- Rayman, M.P. Selenium and human health. Lancet 2012, 379, 1256–1268. [Google Scholar] [CrossRef]
- Xia, Y.; Hill, K.E.; Li, P.; Xu, J.; Zhou, D.; Motley, A.K.; Wang, L.; Byrne, D.W.; Burk, R.F. Optimization of selenoprotein P and other plasma selenium biomarkers for the assessment of the selenium nutritional requirement: A placebo-controlled, double-blind study of selenomethionine supplementation in selenium-deficient Chinese subjects. Am. J. Clin. Nutr. 2010, 92, 525–531. [Google Scholar] [CrossRef] [Green Version]
- Brodin, O.; Hackler, J.; Misra, S.; Wendt, S.; Sun, Q.; Laaf, E.; Stoppe, C.; Bjornstedt, M.; Schomburg, L. Selenoprotein P as Biomarker of Selenium Status in Clinical Trials with Therapeutic Dosages of Selenite. Nutrients 2020, 12, 1067. [Google Scholar] [CrossRef] [Green Version]
- Al-Mubarak, A.A.; van der Meer, P.; Bomer, N. Selenium, Selenoproteins, and Heart Failure: Current Knowledge and Future Perspective. Curr. Heart Fail. Rep. 2021, 18, 122–131. [Google Scholar] [CrossRef]
- Manzanares, W.; Biestro, A.; Galusso, F.; Torre, M.H.; Manay, N.; Pittini, G.; Facchin, G.; Hardy, G. Serum selenium and glutathione peroxidase-3 activity: Biomarkers of systemic inflammation in the critically ill? Intensive Care Med. 2009, 35, 882–889. [Google Scholar] [CrossRef] [PubMed]
- Alehagen, U.; Johansson, P.; Bjornstedt, M.; Rosen, A.; Post, C.; Aaseth, J. Relatively high mortality risk in elderly Swedish subjects with low selenium status. Eur. J. Clin. Nutr. 2016, 70, 91–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalen, A.; Appelkvist, E.L.; Dallner, G. Age-related changes in the lipid compositions of rat and human tissues. Lipids 1989, 24, 579–584. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez-Mariscal, F.M.; Yubero-Serrano, E.M.; Villalba, J.M.; Lopez-Miranda, J. Coenzyme Q10: From bench to clinic in aging diseases, a translational review. Crit. Rev. Food Sci. Nutr. 2019, 59, 2240–2257. [Google Scholar] [CrossRef] [PubMed]
- Xia, L.; Nordman, T.; Olsson, J.M.; Damdimopoulos, A.; Bjorkhem-Bergman, L.; Nalvarte, I.; Eriksson, L.C.; Arner, E.S.; Spyrou, G.; Bjornstedt, M. The mammalian cytosolic selenoenzyme thioredoxin reductase reduces ubiquinone. A novel mechanism for defense against oxidative stress. J. Biol. Chem. 2003, 278, 2141–2146. [Google Scholar] [CrossRef] [Green Version]
- Norman, J.A.; Little, D.; Bolgar, M.; Di Donato, G. Degradation of brain natriuretic peptide by neutral endopeptidase: Species specific sites of proteolysis determined by mass spectrometry. Biochem. Biophys. Res. Commun. 1991, 175, 22–30. [Google Scholar] [CrossRef]
- Alehagen, U.; Johansson, P.; Bjornstedt, M.; Rosen, A.; Dahlstrom, U. Cardiovascular mortality and N-terminal-proBNP reduced after combined selenium and coenzyme Q10 supplementation: A 5-year prospective randomized double-blind placebo-controlled trial among elderly Swedish citizens. Int. J. Cardiol. 2013, 167, 1860–1866. [Google Scholar] [CrossRef] [Green Version]
- Alehagen, U.; Alexander, J.; Aaseth, J.; Larsson, A. Decrease in inflammatory biomarker concentration by intervention with selenium and coenzyme Q10: A subanalysis of osteopontin, osteoprotergerin, TNFr1, TNFr2 and TWEAK. J. Inflamm. 2019, 16, 5. [Google Scholar] [CrossRef] [Green Version]
- Alehagen, U.; Lindahl, T.L.; Aaseth, J.; Svensson, E.; Johansson, P. Levels of sP-selectin and hs-CRP Decrease with Dietary Intervention with Selenium and Coenzyme Q10 Combined: A Secondary Analysis of a Randomized Clinical Trial. PLoS ONE 2015, 10, e0137680. [Google Scholar] [CrossRef]
- Alehagen, U.; Alexander, J.; Aaseth, J.; Larsson, A.; Lindahl, T.L. Significant decrease of von Willebrand factor and plasminogen activator inhibitor-1 by providing supplementation with selenium and coenzyme Q10 to an elderly population with a low selenium status. Eur. J. Nutr. 2020, 59, 3581–3590. [Google Scholar] [CrossRef] [Green Version]
- Kuklinski, B.; Weissenbacher, E.; Fahnrich, A. Coenzyme Q10 and antioxidants in acute myocardial infarction. Mol. Asp. Med. 1994, 15, s143–s147. [Google Scholar] [CrossRef]
- Alehagen, U.; Alexander, J.; Aaseth, J. Supplementation with Selenium and Coenzyme Q10 Reduces Cardiovascular Mortality in Elderly with Low Selenium Status. A Secondary Analysis of a Randomised Clinical Trial. PLoS ONE 2016, 11, e0157541. [Google Scholar] [CrossRef] [PubMed]
- Jensen-Urstad, K.; Bouvier, F.; Hojer, J.; Ruiz, H.; Hulting, J.; Samad, B.; Thorstrand, C.; Jensen-Urstad, M. Comparison of different echocardiographic methods with radionuclide imaging for measuring left ventricular ejection fraction during acute myocardial infarction treated by thrombolytic therapy. Am. J. Cardiol. 1998, 81, 538–544. [Google Scholar] [CrossRef]
- van Royen, N.; Jaffe, C.C.; Krumholz, H.M.; Johnson, K.M.; Lynch, P.J.; Natale, D.; Atkinson, P.; Deman, P.; Wackers, F.J. Comparison and reproducibility of visual echocardiographic and quantitative radionuclide left ventricular ejection fractions. Am. J. Cardiol. 1996, 77, 843–850. [Google Scholar] [CrossRef]
- Mehta, R.; Cai, X.; Lee, J.; Xie, D.; Wang, X.; Scialla, J.; Anderson, A.H.; Taliercio, J.; Dobre, M.; Chen, J.; et al. Serial Fibroblast Growth Factor 23 Measurements and Risk of Requirement for Kidney Replacement Therapy: The CRIC (Chronic Renal Insufficiency Cohort) Study. Am. J. Kidney Dis. 2020, 75, 908–918. [Google Scholar] [CrossRef]
- Orskov, B.; Borresen, M.L.; Feldt-Rasmussen, B.; Ostergaard, O.; Laursen, I.; Strandgaard, S. Estimating glomerular filtration rate using the new CKD-EPI equation and other equations in patients with autosomal dominant polycystic kidney disease. Am. J. Nephrol. 2010, 31, 53–57. [Google Scholar] [CrossRef]
- Parker, B.D.; Schurgers, L.J.; Brandenburg, V.M.; Christenson, R.H.; Vermeer, C.; Ketteler, M.; Shlipak, M.G.; Whooley, M.A.; Ix, J.H. The associations of fibroblast growth factor 23 and uncarboxylated matrix Gla protein with mortality in coronary artery disease: The Heart and Soul Study. Ann. Intern. Med. 2010, 152, 640–648. [Google Scholar] [CrossRef] [Green Version]
- Udell, J.A.; Morrow, D.A.; Jarolim, P.; Sloan, S.; Hoffman, E.B.; O’Donnell, T.F.; Vora, A.N.; Omland, T.; Solomon, S.D.; Pfeffer, M.A.; et al. Fibroblast growth factor-23, cardiovascular prognosis, and benefit of angiotensin-converting enzyme inhibition in stable ischemic heart disease. J. Am. Coll. Cardiol. 2014, 63, 2421–2428. [Google Scholar] [CrossRef] [Green Version]
- Bernasconi, R.; Aeschbacher, S.; Blum, S.; Mongiat, M.; Girod, M.; Todd, J.; Estis, J.; Nolan, N.; Renz, H.; Risch, L.; et al. Fibroblast growth factor 23 and renal function among young and healthy individuals. Clin. Chem. Lab. Med. 2018, 56, 1483–1489. [Google Scholar] [CrossRef]
- Alehagen, U.; Aaseth, J.; Alexander, J.; Brismar, K.; Larsson, A. Selenium and Coenzyme Q10 Supplementation Improves Renal Function in Elderly Deficient in Selenium: Observational Results and Results from a Subgroup Analysis of a Prospective Randomised Double-Blind Placebo-Controlled Trial. Nutrients 2020, 12, 3780. [Google Scholar] [CrossRef]
- Voelkl, J.; Egli-Spichtig, D.; Alesutan, I.; Wagner, C.A. Inflammation: A putative link between phosphate metabolism and cardiovascular disease. Clin. Sci. 2021, 135, 201–227. [Google Scholar] [CrossRef] [PubMed]
- Hanks, L.J.; Casazza, K.; Judd, S.E.; Jenny, N.S.; Gutierrez, O.M. Associations of fibroblast growth factor-23 with markers of inflammation, insulin resistance and obesity in adults. PLoS ONE 2015, 10, e0122885. [Google Scholar] [CrossRef] [PubMed]
- Alehagen, U.; Opstad, T.B.; Alexander, J.; Larsson, A.; Aaseth, J. Impact of Selenium on Biomarkers and Clinical Aspects Related to Ageing. A Review. Biomolecules 2021, 11, 1478. [Google Scholar] [CrossRef] [PubMed]
- Urakawa, I.; Yamazaki, Y.; Shimada, T.; Iijima, K.; Hasegawa, H.; Okawa, K.; Fujita, T.; Fukumoto, S.; Yamashita, T. Klotho converts canonical FGF receptor into a specific receptor for FGF23. Nature 2006, 444, 770–774. [Google Scholar] [CrossRef] [PubMed]
- Pastor-Arroyo, E.M.; Gehring, N.; Krudewig, C.; Costantino, S.; Bettoni, C.; Knopfel, T.; Sabrautzki, S.; Lorenz-Depiereux, B.; Pastor, J.; Strom, T.M.; et al. The elevation of circulating fibroblast growth factor 23 without kidney disease does not increase cardiovascular disease risk. Kidney Int. 2018, 94, 49–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, X.; Cai, C.; Xiao, Z.; Quarles, L.D. FGF23 induced left ventricular hypertrophy mediated by FGFR4 signaling in the myocardium is attenuated by soluble Klotho in mice. J. Mol. Cell. Cardiol. 2020, 138, 66–74. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, E.A.; Han, X.; Xiao, Z.; Quarles, L.D. Role of Fibroblast Growth Factor-23 in Innate Immune Responses. Front. Endocrinol. 2018, 9, 320. [Google Scholar] [CrossRef]
- Wang, L.; Song, Y.; Manson, J.E.; Pilz, S.; Marz, W.; Michaelsson, K.; Lundqvist, A.; Jassal, S.K.; Barrett-Connor, E.; Zhang, C.; et al. Circulating 25-hydroxy-vitamin D and risk of cardiovascular disease: A meta-analysis of prospective studies. Circ. Cardiovasc. Qual. Outcomes 2012, 5, 819–829. [Google Scholar] [CrossRef] [Green Version]
- Alexander, J.; Alehagen, U.; Larsson, A.; Aaseth, J. Selenium in clinical medicine and medical biochemistry. Klin. Biokem. I Nord 2019, 31, 12–19. [Google Scholar]


{kind=link}
| Active Treatment Group N = 118 | Placebo Group N = 101 | p-Value | |
|---|---|---|---|
| Age years, mean (SD) | 76.2 (3.1) | 76.3 (3.1) | 0.74 |
| Gender, Males/Females | 58/60 | 43/58 | |
| History | |||
| Diabetes, n (%) | 20 (16.9) | 18 (17.8) | 0.87 |
| Smoking, n (%) | 8 (6.8) | 9 (8.9) | 0.56 |
| Hypertension, n (%) | 81 (68.6) | 72 (71.3) | 0.67 |
| IHD, n (%) | 22 (18.6) | 16 (15.8) | 0.59 |
| Atrial Fibrillation, n (%) | 8 (6.8) | 7 (6.9) | 0.96 |
| NYHA class I, n (%) | 71 (60.2) | 58 (57.4) | 0.68 |
| NYHA class II, n (%) | 29 (24.6) | 30 (29.7) | 0.39 |
| NYHA class III, n (%) | 18 (15.3) | 12 (11.9) | 0.47 |
| NYHA class IV, n (%) | 0 | 0 | |
| Unclassified, n | 0 | 1 | |
| Medications | |||
| ACEI/ARB, n (%) | 19 (16.1) | 21 (20.8) | 0.37 |
| Beta blockers, n (%) | 44 (37.3) | 33 (32.7) | 0.48 |
| Diuretics, n (%) | 39 (33.1) | 33 (32.7) | 0.95 |
| Statins, n (%) | 27 (22.9) | 17 (16.8) | 0.20 |
| Examinations | |||
| EF < 40%, n (%) | 7 (5.9) | 4 (4.0) | 0.51 |
| CV mortality, n (%) | 16 (13.6) | 24 (23.8) | 0.05 |
| Selenium conc. pre-intervention mean, µg/L (SD) | 66.6 (15.9) | 67.3 (17.2) | 0.56 |
| Effects | Sum of Squares | F | p |
|---|---|---|---|
| Intercept | 5.21 × 108 | 2.62 | 0.11 |
| Age | 6.1 × 108 | 3.06 | 0.08 |
| HsCRP | 1.3 × 108 | 0.66 | 0.42 |
| FGF-23 inclusion | 4.5 × 1010 | 225.3 | <0.0001 |
| NT-proBNP | 1.6 × 108 | 0.80 | 0.37 |
| Smoker | 1.3 × 107 | 0.07 | 0.80 |
| Hypertension | 3.0 × 108 | 1.49 | 0.23 |
| Diabetes | 1.1 × 109 | 5.51 | 0.02 |
| NYHA 3 | 6.0 × 107 | 0.28 | 0.60 |
| Hb < 120 g/L | 6.5 × 107 | 0.33 | 0.57 |
| Male | 2.4 × 107 | 0.12 | 0.73 |
| s-selenium microgr/L, incl. | 3.7 × 107 | 0.18 | 0.67 |
| Active treatment | 1.07 × 109 | 5.35 | 0.02 |
| Error | 1.6 × 1010 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alehagen, U.; Aaseth, J.; Larsson, A.; Alexander, J. Decreased Concentration of Fibroblast Growth Factor 23 (FGF-23) as a Result of Supplementation with Selenium and Coenzyme Q10 in an Elderly Swedish Population: A Sub-Analysis. Cells 2022, 11, 509. https://doi.org/10.3390/cells11030509
Alehagen U, Aaseth J, Larsson A, Alexander J. Decreased Concentration of Fibroblast Growth Factor 23 (FGF-23) as a Result of Supplementation with Selenium and Coenzyme Q10 in an Elderly Swedish Population: A Sub-Analysis. Cells. 2022; 11(3):509. https://doi.org/10.3390/cells11030509
Chicago/Turabian StyleAlehagen, Urban, Jan Aaseth, Anders Larsson, and Jan Alexander. 2022. "Decreased Concentration of Fibroblast Growth Factor 23 (FGF-23) as a Result of Supplementation with Selenium and Coenzyme Q10 in an Elderly Swedish Population: A Sub-Analysis" Cells 11, no. 3: 509. https://doi.org/10.3390/cells11030509