
Hematopoietic Stem Cell Transplantation in Refractory Crohn’s Disease: Should It Be Considered?

Abstract
:1. Introduction
1.1. Crohn’s Disease
1.2. Hematopoietic Stem Cell Transplantation (HSCT)
2. HSCT for Crohn’s Disease
2.1. First Evidence
2.2. Patient Selection for HSCT in CD
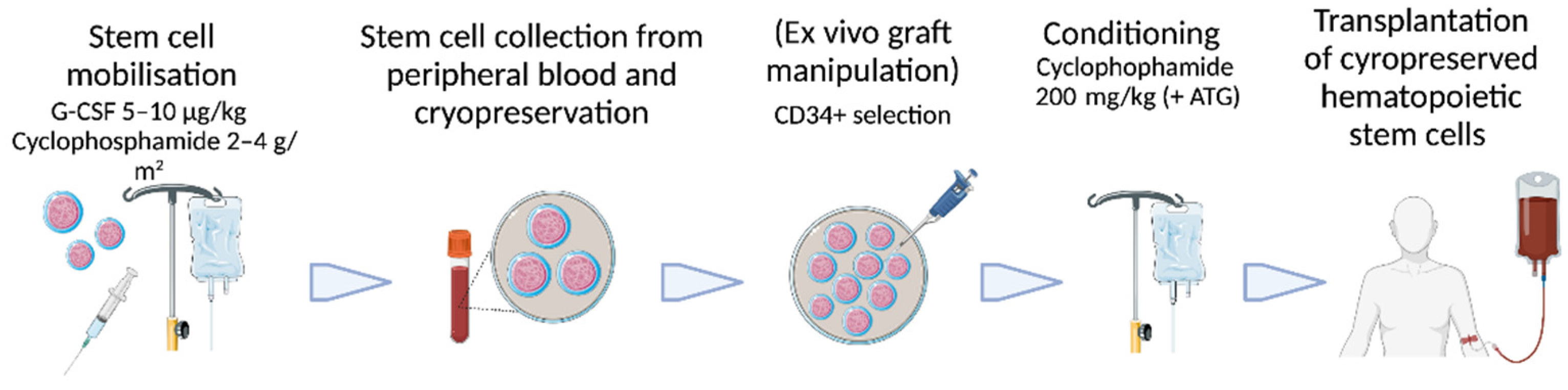
2.3. Technical Aspects of Autologous HSCT for CD
2.4. Actual Evidence for Autologous HSCT in CD
2.5. Actual Evidence for Allogenic HSCT in CD
2.6. Safety of HSCT in CD
3. Discussion
3.1. Risks and Benefits of HSCT in CD
3.2. Selecting CD Patients for HSCT
4. Future Perspectives and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Feuerstein, J.D.; Cheifetz, A.S. Crohn Disease: Epidemiology, Diagnosis, and Management. Mayo Clin. Proc. 2017, 92, 1088–1103. [Google Scholar] [CrossRef] [Green Version]
- Torres, J.; Mehandru, S.; Colombel, J.F.; Peyrin-Biroulet, L. Crohn’s disease. Lancet 2017, 389, 1741–1755. [Google Scholar] [CrossRef]
- Nambu, R.; Warner, N.; Mulder, D.J.; Kotlarz, D.; McGovern, D.P.B.; Cho, J.; Klein, C.; Snapper, S.B.; Griffiths, A.M.; Iwama, I.; et al. A Systematic Review of Monogenic Inflammatory Bowel Disease. Clin. Gastroenterol. Hepatol. 2022, 20, e653–e663. [Google Scholar] [CrossRef]
- Uhlig, H.H.; Schwerd, T.; Koletzko, S.; Shah, N.; Kammermeier, J.; Elkadri, A.; Ouahed, J.; Wilson, D.C.; Travis, S.P.; Turner, D.; et al. The diagnostic approach to monogenic very early onset inflammatory bowel disease. Gastroenterology 2014, 147, 990–1007.e1003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaser, A.; Zeissig, S.; Blumberg, R.S. Inflammatory bowel disease. Annu. Rev. Immunol. 2010, 28, 573–621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, N.A.; Rubin, D.T. New targets in inflammatory bowel disease therapy: 2021. Curr. Opin. Gastroenterol. 2021, 37, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Gade, A.K.; Douthit, N.T.; Townsley, E. Medical Management of Crohn’s Disease. Cureus 2020, 12, e8351. [Google Scholar] [CrossRef] [PubMed]
- Vermeire, S.; D’Haens, G.; Baert, F.; Danese, S.; Kobayashi, T.; Loftus, E.V.; Bhatia, S.; Agboton, C.; Rosario, M.; Chen, C.; et al. Efficacy and Safety of Subcutaneous Vedolizumab in Patients With Moderately to Severely Active Crohn’s Disease: Results From the VISIBLE 2 Randomised Trial. J. Crohn’s Colitis 2022, 16, 27–38. [Google Scholar] [CrossRef]
- Feagan, B.G.; Sandborn, W.J.; Gasink, C.; Jacobstein, D.; Lang, Y.; Friedman, J.R.; Blank, M.A.; Johanns, J.; Gao, L.L.; Miao, Y.; et al. Ustekinumab as Induction and Maintenance Therapy for Crohn’s Disease. N. Engl. J. Med. 2016, 375, 1946–1960. [Google Scholar] [CrossRef]
- Sandborn, W.J.; Hanauer, S.B.; Rutgeerts, P.; Fedorak, R.N.; Lukas, M.; MacIntosh, D.G.; Panaccione, R.; Wolf, D.; Kent, J.D.; Bittle, B.; et al. Adalimumab for maintenance treatment of Crohn’s disease: Results of the CLASSIC II trial. Gut 2007, 56, 1232–1239. [Google Scholar] [CrossRef]
- Sandborn, W.J.; Feagan, B.G.; Loftus, E.V., Jr.; Peyrin-Biroulet, L.; Van Assche, G.; D’Haens, G.; Schreiber, S.; Colombel, J.F.; Lewis, J.D.; Ghosh, S.; et al. Efficacy and Safety of Upadacitinib in a Randomized Trial of Patients with Crohn’s Disease. Gastroenterology 2020, 158, 2123–2138.e2128. [Google Scholar] [CrossRef] [PubMed]
- D’Haens, G.; Panaccione, R.; Baert, F.; Bossuyt, P.; Colombel, J.F.; Danese, S.; Dubinsky, M.; Feagan, B.G.; Hisamatsu, T.; Lim, A.; et al. Risankizumab as induction therapy for Crohn’s disease: Results from the phase 3 ADVANCE and MOTIVATE induction trials. Lancet 2022, 399, 2015–2030. [Google Scholar] [CrossRef]
- Torres, J.; Bonovas, S.; Doherty, G.; Kucharzik, T.; Gisbert, J.P.; Raine, T.; Adamina, M.; Armuzzi, A.; Bachmann, O.; Bager, P.; et al. ECCO Guidelines on Therapeutics in Crohn’s Disease: Medical Treatment. J. Crohn’s Colitis 2020, 14, 4–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osgood, E.E.; Riddle, M.C.; Mathews, T.J. Aplastic anemia treated with daily transfusions and intravenous marrow; case report. Ann. Intern. Med. 1939, 13, 357–367. [Google Scholar]
- Henig, I.; Zuckerman, T. Hematopoietic stem cell transplantation-50 years of evolution and future perspectives. Rambam Maimonides Med. J. 2014, 5, e0028. [Google Scholar] [CrossRef] [PubMed]
- Swart, J.F.; Delemarre, E.M.; van Wijk, F.; Boelens, J.J.; Kuball, J.; van Laar, J.M.; Wulffraat, N.M. Haematopoietic stem cell transplantation for autoimmune diseases. Nat. Rev. Rheumatol. 2017, 13, 244–256. [Google Scholar] [CrossRef] [PubMed]
- Hügle, T.; Daikeler, T. Stem cell transplantation for autoimmune diseases. Haematologica 2010, 95, 185–188. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, M.C.; Elias, J.B.; Moraes, D.A.; Simões, B.P.; Rodrigues, M.; Ribeiro, A.A.F.; Piron-Ruiz, L.; Ruiz, M.A.; Hamerschlak, N. A review of hematopoietic stem cell transplantation for autoimmune diseases: Multiple sclerosis, systemic sclerosis and Crohn’s disease. Position paper of the Brazilian Society of Bone Marrow Transplantation. Hematol. Transfus. Cell Ther. 2021, 43, 65–86. [Google Scholar] [CrossRef]
- Penack, O.; Peczynski, C.; Mohty, M.; Yakoub-Agha, I.; Styczynski, J.; Montoto, S.; Duarte, R.F.; Kröger, N.; Schoemans, H.; Koenecke, C.; et al. How much has allogeneic stem cell transplant-related mortality improved since the 1980s? A retrospective analysis from the EBMT. Blood Adv. 2020, 4, 6283–6290. [Google Scholar] [CrossRef]
- Pockley, A.G.; Lindsay, J.O.; Foulds, G.A.; Rutella, S.; Gribben, J.G.; Alexander, T.; Snowden, J.A. Immune Reconstitution After Autologous Hematopoietic Stem Cell Transplantation in Crohn’s Disease: Current Status and Future Directions. A Review on Behalf of the EBMT Autoimmune Diseases Working Party and the Autologous Stem Cell Transplantation In Refractory CD-Low Intensity Therapy Evaluation Study Investigators. Front. Immunol. 2018, 9, 646. [Google Scholar] [CrossRef]
- Musso, M.; Porretto, F.; Crescimanno, A.; Bondì, F.; Polizzi, V.; Scalone, R. Crohn’s disease complicated by relapsed extranodal Hodgkin’s lymphoma: Prolonged complete remission after unmanipulated PBPC autotransplant. Bone Marrow Transplant. 2000, 26, 921–923. [Google Scholar] [CrossRef] [PubMed]
- Ditschkowski, M.; Einsele, H.; Schwerdtfeger, R.; Bunjes, D.; Trenschel, R.; Beelen, D.W.; Elmaagacli, A.H. Improvement of inflammatory bowel disease after allogeneic stem-cell transplantation. Transplantation 2003, 75, 1745–1747. [Google Scholar] [CrossRef] [PubMed]
- Drakos, P.E.; Nagler, A.; Or, R. Case of Crohn’s disease in bone marrow transplantation. Am. J. Hematol. 1993, 43, 157–158. [Google Scholar] [CrossRef] [PubMed]
- Kashyap, A.; Forman, S.J. Autologous bone marrow transplantation for non-Hodgkin’s lymphoma resulting in long-term remission of coincidental Crohn’s disease. Br. J. Haematol. 1998, 103, 651–652. [Google Scholar] [CrossRef]
- Lopez-Cubero, S.O.; Sullivan, K.M.; McDonald, G.B. Course of Crohn’s disease after allogeneic marrow transplantation. Gastroenterology 1998, 114, 433–440. [Google Scholar] [CrossRef]
- Ruiz, M.A.; Kaiser Junior, R.L.; Piron-Ruiz, L.; Peña-Arciniegas, T.; Saran, P.S.; De Quadros, L.G. Hematopoietic stem cell transplantation for Crohn’s disease: Gaps, doubts and perspectives. World J. Stem Cells 2018, 10, 134–137. [Google Scholar] [CrossRef]
- Snowden, J.A.; Panés, J.; Alexander, T.; Allez, M.; Ardizzone, S.; Dierickx, D.; Finke, J.; Hasselblatt, P.; Hawkey, C.; Kazmi, M.; et al. Autologous Haematopoietic Stem Cell Transplantation (AHSCT) in Severe Crohn’s Disease: A Review on Behalf of ECCO and EBMT. J. Crohn’s Colitis 2018, 12, 476–488. [Google Scholar] [CrossRef] [Green Version]
- El-Ghammaz, A.M.S.; Ben Matoug, R.; Elzimaity, M.; Mostafa, N. Nutritional status of allogeneic hematopoietic stem cell transplantation recipients: Influencing risk factors and impact on survival. Support. Care Cancer 2017, 25, 3085–3093. [Google Scholar] [CrossRef]
- Lee, C.H.; Yoon, H.; Oh, D.J.; Lee, J.M.; Choi, Y.J.; Shin, C.M.; Park, Y.S.; Kim, N.; Lee, D.H.; Kim, J.S. The prevalence of sarcopenia and its effect on prognosis in patients with Crohn’s disease. Intest. Res. 2020, 18, 79–84. [Google Scholar] [CrossRef] [Green Version]
- Afessa, B.; Abdulai, R.M.; Kremers, W.K.; Hogan, W.J.; Litzow, M.R.; Peters, S.G. Risk factors and outcome of pulmonary complications after autologous hematopoietic stem cell transplant. Chest 2012, 141, 442–450. [Google Scholar] [CrossRef]
- Blaes, A.; Konety, S.; Hurley, P. Cardiovascular Complications of Hematopoietic Stem Cell Transplantation. Curr. Treat. Options Cardiovasc. Med. 2016, 18, 25. [Google Scholar] [CrossRef] [PubMed]
- Jessop, H.; Farge, D.; Saccardi, R.; Alexander, T.; Rovira, M.; Sharrack, B.; Greco, R.; Wulffraat, N.; Moore, J.; Kazmi, M.; et al. General information for patients and carers considering haematopoietic stem cell transplantation (HSCT) for severe autoimmune diseases (ADs): A position statement from the EBMT Autoimmune Diseases Working Party (ADWP), the EBMT Nurses Group, the EBMT Patient, Family and Donor Committee and the Joint Accreditation Committee of ISCT and EBMT (JACIE). Bone Marrow Transplant. 2019, 54, 933–942. [Google Scholar] [CrossRef] [PubMed]
- Arnaout, K.; Patel, N.; Jain, M.; El-Amm, J.; Amro, F.; Tabbara, I.A. Complications of allogeneic hematopoietic stem cell transplantation. Cancer Investig. 2014, 32, 349–362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burt, R.K.; Fassas, A.; Snowden, J.; van Laar, J.M.; Kozak, T.; Wulffraat, N.M.; Nash, R.A.; Dunbar, C.E.; Arnold, R.; Prentice, G.; et al. Collection of hematopoietic stem cells from patients with autoimmune diseases. Bone Marrow Transplant. 2001, 28, 1–12. [Google Scholar] [CrossRef]
- Statkute, L.; Verda, L.; Oyama, Y.; Traynor, A.; Villa, M.; Shook, T.; Clifton, R.; Jovanovic, B.; Satkus, J.; Loh, Y.; et al. Mobilization, harvesting and selection of peripheral blood stem cells in patients with autoimmune diseases undergoing autologous hematopoietic stem cell transplantation. Bone Marrow Transplant. 2007, 39, 317–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vasiliu, I.M.; Petri, M.A.; Baer, A.N. Therapy with granulocyte colony-stimulating factor in systemic lupus erythematosus may be associated with severe flares. J. Rheumatol. 2006, 33, 1878–1880. [Google Scholar] [PubMed]
- Scimè, R.; Cavallaro, A.M.; Tringali, S.; Santoro, A.; Rizzo, A.; Montalbano, L.; Casà, A.; Cottone, M. Complete clinical remission after high-dose immune suppression and autologous hematopoietic stem cell transplantation in severe Crohn’s disease refractory to immunosuppressive and immunomodulator therapy. Inflamm. Bowel Dis. 2004, 10, 892–894. [Google Scholar] [CrossRef]
- Burt, R.K.; Craig, R.M.; Milanetti, F.; Quigley, K.; Gozdziak, P.; Bucha, J.; Testori, A.; Halverson, A.; Verda, L.; de Villiers, W.J.; et al. Autologous nonmyeloablative hematopoietic stem cell transplantation in patients with severe anti-TNF refractory Crohn disease: Long-term follow-up. Blood 2010, 116, 6123–6132. [Google Scholar] [CrossRef]
- Cassinotti, A.; Annaloro, C.; Ardizzone, S.; Onida, F.; Della Volpe, A.; Clerici, M.; Usardi, P.; Greco, S.; Maconi, G.; Porro, G.B.; et al. Autologous haematopoietic stem cell transplantation without CD34+ cell selection in refractory Crohn’s disease. Gut 2008, 57, 211–217. [Google Scholar] [CrossRef]
- Hommes, D.W.; Duijvestein, M.; Zelinkova, Z.; Stokkers, P.C.; Ley, M.H.; Stoker, J.; Voermans, C.; van Oers, M.H.; Kersten, M.J. Long-term follow-up of autologous hematopoietic stem cell transplantation for severe refractory Crohn’s disease. J. Crohn’s Colitis 2011, 5, 543–549. [Google Scholar] [CrossRef] [Green Version]
- Hasselblatt, P.; Drognitz, K.; Potthoff, K.; Bertz, H.; Kruis, W.; Schmidt, C.; Stallmach, A.; Schmitt-Graeff, A.; Finke, J.; Kreisel, W. Remission of refractory Crohn’s disease by high-dose cyclophosphamide and autologous peripheral blood stem cell transplantation. Aliment. Pharmacol. Ther. 2012, 36, 725–735. [Google Scholar] [CrossRef] [PubMed]
- Snowden, J.A.; Ansari, A.; Sachchithanantham, S.; Jackson, G.; Thompson, N.; Lobo, A.; Sanderson, J.; Kazmi, M. Autologous stem cell transplantation in severe treatment-resistant Crohn’s disease: Long-term follow-up of UK patients treated on compassionate basis. QJM 2014, 107, 871–877. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jauregui-Amezaga, A.; Rovira, M.; Marín, P.; Salas, A.; Pinó-Donnay, S.; Feu, F.; Elizalde, J.I.; Fernández-Avilés, F.; Martínez, C.; Gutiérrez, G.; et al. Improving safety of autologous haematopoietic stem cell transplantation in patients with Crohn’s disease. Gut 2016, 65, 1456–1462. [Google Scholar] [CrossRef] [PubMed]
- López-García, A.; Rovira, M.; Jauregui-Amezaga, A.; Marín, P.; Barastegui, R.; Salas, A.; Ribas, V.; Feu, F.; Elizalde, J.I.; Fernández-Avilés, F.; et al. Autologous Haematopoietic Stem Cell Transplantation for Refractory Crohn’s Disease: Efficacy in a Single-Centre Cohort. J. Crohn’s Colitis 2017, 11, 1161–1168. [Google Scholar] [CrossRef] [Green Version]
- Hawkey, C.J.; Allez, M.; Clark, M.M.; Labopin, M.; Lindsay, J.O.; Ricart, E.; Rogler, G.; Rovira, M.; Satsangi, J.; Danese, S.; et al. Autologous Hematopoetic Stem Cell Transplantation for Refractory Crohn Disease: A Randomized Clinical Trial. JAMA 2015, 314, 2524–2534. [Google Scholar] [CrossRef]
- Lindsay, J.O.; Allez, M.; Clark, M.; Labopin, M.; Ricart, E.; Rogler, G.; Rovira, M.; Satsangi, J.; Farge, D.; Hawkey, C.J. Autologous stem-cell transplantation in treatment-refractory Crohn’s disease: An analysis of pooled data from the ASTIC trial. Lancet Gastroenterol. Hepatol. 2017, 2, 399–406. [Google Scholar] [CrossRef] [Green Version]
- Brierley, C.K.; Castilla-Llorente, C.; Labopin, M.; Badoglio, M.; Rovira, M.; Ricart, E.; Dierickx, D.; Vermeire, S.; Hasselblatt, P.; Finke, J.; et al. Autologous Haematopoietic Stem Cell Transplantation for Crohn’s Disease: A Retrospective Survey of Long-term Outcomes From the European Society for Blood and Marrow Transplantation. J. Crohn’s Colitis 2018, 12, 1097–1103. [Google Scholar] [CrossRef]
- Hernanz, N.; Sierra, M.; Volpato, N.; Núñez-Gómez, L.; Mesonero, F.; Herrera-Puente, P.; García-Gutiérrez, V.; Albillos, A.; López-San Román, A. Autologous haematopoietic stem cell transplantation in refractory Crohn’s disease: Experience in our centre. Gastroenterol. Hepatol. 2019, 42, 16–22. [Google Scholar] [CrossRef]
- Snowden, J.A.; Saccardi, R.; Allez, M.; Ardizzone, S.; Arnold, R.; Cervera, R.; Denton, C.; Hawkey, C.; Labopin, M.; Mancardi, G.; et al. Haematopoietic SCT in severe autoimmune diseases: Updated guidelines of the European Group for Blood and Marrow Transplantation. Bone Marrow Transplant. 2012, 47, 770–790. [Google Scholar] [CrossRef] [Green Version]
- Burt, R.K.; Craig, R.; Yun, L.; Halverson, A.; Quigley, K.; Arnautovic, I.; Han, X. A pilot feasibility study of non-myeloablative allogeneic hematopoietic stem cell transplantation for refractory Crohn Disease. Bone Marrow Transplant. 2020, 55, 2343–2346. [Google Scholar] [CrossRef]
- Kelsey, P.J.; Oliveira, M.C.; Badoglio, M.; Sharrack, B.; Farge, D.; Snowden, J.A. Haematopoietic stem cell transplantation in autoimmune diseases: From basic science to clinical practice. Curr. Res. Transl. Med. 2016, 64, 71–82. [Google Scholar] [CrossRef] [PubMed]
- Burt, R.K.; Traynor, A.; Oyama, Y.; Craig, R. High-dose immune suppression and autologous hematopoietic stem cell transplantation in refractory Crohn disease. Blood 2003, 101, 2064–2066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craig, R.M.; Traynor, A.; Oyama, Y.; Burt, R.K. Hematopoietic stem cell transplantation for severe Crohn’s disease. Bone Marrow Transplant. 2003, 32 (Suppl. 1), S57–S59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Nakeep, S.; Shawky, A.; Abbas, S.F.; Abdel Latif, O. Stem cell transplantation for induction of remission in medically refractory Crohn’s disease. Cochrane Database Syst. Rev. 2022, 5, Cd013070. [Google Scholar] [CrossRef]
- Mikulska, M.; Del Bono, V.; Bruzzi, P.; Raiola, A.M.; Gualandi, F.; Van Lint, M.T.; Bacigalupo, A.; Viscoli, C. Mortality after bloodstream infections in allogeneic haematopoietic stem cell transplant (HSCT) recipients. Infection 2012, 40, 271–278. [Google Scholar] [CrossRef]
- Busmail, A.; Penumetcha, S.S.; Ahluwalia, S.; Irfan, R.; Khan, S.A.; Rohit Reddy, S.; Vasquez Lopez, M.E.; Zahid, M.; Mohammed, L. A Systematic Review on Pulmonary Complications Secondary to Hematopoietic Stem Cell Transplantation. Cureus 2022, 14, e24807. [Google Scholar] [CrossRef]
- Giménez, E.; Torres, I.; Albert, E.; Piñana, J.L.; Hernández-Boluda, J.C.; Solano, C.; Navarro, D. Cytomegalovirus (CMV) infection and risk of mortality in allogeneic hematopoietic stem cell transplantation (Allo-HSCT): A systematic review, meta-analysis, and meta-regression analysis. Am. J. Transplant. 2019, 19, 2479–2494. [Google Scholar] [CrossRef]
- Tanaka, Y.; Kurosawa, S.; Tajima, K.; Tanaka, T.; Ito, R.; Inoue, Y.; Okinaka, K.; Inamoto, Y.; Fuji, S.; Kim, S.W.; et al. Analysis of non-relapse mortality and causes of death over 15 years following allogeneic hematopoietic stem cell transplantation. Bone Marrow Transplant. 2016, 51, 553–559. [Google Scholar] [CrossRef] [Green Version]
- Sorror, M.L.; Maris, M.B.; Storb, R.; Baron, F.; Sandmaier, B.M.; Maloney, D.G.; Storer, B. Hematopoietic cell transplantation (HCT)-specific comorbidity index: A new tool for risk assessment before allogeneic HCT. Blood 2005, 106, 2912–2919. [Google Scholar] [CrossRef] [Green Version]
- Petersdorf, E.W.; Stevenson, P.; Bengtsson, M.; De Santis, D.; Dubois, V.; Gooley, T.; Horowitz, M.; Hsu, K.; Madrigal, J.A.; Malkki, M.; et al. HLA-B leader and survivorship after HLA-mismatched unrelated donor transplantation. Blood 2020, 136, 362–369. [Google Scholar] [CrossRef]
- Fuchs, E.J.; McCurdy, S.R.; Solomon, S.R.; Wang, T.; Herr, M.R.; Modi, D.; Grunwald, M.R.; Nishihori, T.; Kuxhausen, M.; Fingerson, S.; et al. HLA informs risk predictions after haploidentical stem cell transplantation with posttransplantation cyclophosphamide. Blood 2022, 139, 1452–1468. [Google Scholar] [CrossRef] [PubMed]
- Burisch, J.; Kiudelis, G.; Kupcinskas, L.; Kievit, H.A.L.; Andersen, K.W.; Andersen, V.; Salupere, R.; Pedersen, N.; Kjeldsen, J.; D’Incà, R.; et al. Natural disease course of Crohn’s disease during the first 5 years after diagnosis in a European population-based inception cohort: An Epi-IBD study. Gut 2019, 68, 423–433. [Google Scholar] [CrossRef]
- Sandborn, W.J.; D’Haens, G.R.; Reinisch, W.; Panés, J.; Chan, D.; Gonzalez, S.; Weisel, K.; Germinaro, M.; Frustaci, M.E.; Yang, Z.; et al. Guselkumab for the Treatment of Crohn’s Disease: Induction Results From the Phase 2 GALAXI-1 Study. Gastroenterology 2022, 162, 1650–1664.e1658. [Google Scholar] [CrossRef] [PubMed]
- Mohty, M. Mechanisms of action of antithymocyte globulin: T-cell depletion and beyond. Leukemia 2007, 21, 1387–1394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loh, Y.; Oyama, Y.; Statkute, L.; Quigley, K.; Yaung, K.; Gonda, E.; Barr, W.; Jovanovic, B.; Craig, R.; Stefoski, D.; et al. Development of a secondary autoimmune disorder after hematopoietic stem cell transplantation for autoimmune diseases: Role of conditioning regimen used. Blood 2007, 109, 2643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grossberg, L.B.; Papamichael, K.; Cheifetz, A.S. Review article: Emerging drug therapies in inflammatory bowel disease. Aliment. Pharmacol. Ther. 2022, 55, 789–804. [Google Scholar] [CrossRef]
- Danese, S.; Parigi, T.L.; Peyrin-Biroulet, L.; Ghosh, S. Defining difficult-to-treat inflammatory bowel disease: Why and how. Lancet Gastroenterol. Hepatol. 2021, 6, 520–522. [Google Scholar] [CrossRef]
- Adamina, M.; Bonovas, S.; Raine, T.; Spinelli, A.; Warusavitarne, J.; Armuzzi, A.; Bachmann, O.; Bager, P.; Biancone, L.; Bokemeyer, B.; et al. ECCO Guidelines on Therapeutics in Crohn’s Disease: Surgical Treatment. J. Crohn’s Colitis 2020, 14, 155–168. [Google Scholar] [CrossRef] [Green Version]
- Lee, W.Y.; Park, K.J.; Cho, Y.B.; Yoon, S.N.; Song, K.H.; Kim, D.S.; Jung, S.H.; Kim, M.; Yoo, H.W.; Kim, I.; et al. Autologous adipose tissue-derived stem cells treatment demonstrated favorable and sustainable therapeutic effect for Crohn’s fistula. Stem Cells 2013, 31, 2575–2581. [Google Scholar] [CrossRef]
- Bettenworth, D.; Gustavsson, A.; Atreja, A.; Lopez, R.; Tysk, C.; van Assche, G.; Rieder, F. A Pooled Analysis of Efficacy, Safety, and Long-term Outcome of Endoscopic Balloon Dilation Therapy for Patients with Stricturing Crohn’s Disease. Inflamm. Bowel Dis. 2017, 23, 133–142. [Google Scholar] [CrossRef]
- Ozuner, G.; Fazio, V.W.; Lavery, I.C.; Milsom, J.W.; Strong, S.A. Reoperative rates for Crohn’s disease following strictureplasty. Long-term analysis. Dis. Colon Rectum 1996, 39, 1199–1203. [Google Scholar] [CrossRef]
- Bellolio, F.; Cohen, Z.; MacRae, H.M.; O’Connor, B.I.; Victor, J.C.; Huang, H.; McLeod, R.S. Strictureplasty in selected Crohn’s disease patients results in acceptable long-term outcome. Dis. Colon Rectum 2012, 55, 864–869. [Google Scholar] [CrossRef]
- Fedyk, E.R.; Wyant, T.; Yang, L.L.; Csizmadia, V.; Burke, K.; Yang, H.; Kadambi, V.J. Exclusive antagonism of the α4 β7 integrin by vedolizumab confirms the gut-selectivity of this pathway in primates. Inflamm. Bowel Dis. 2012, 18, 2107–2119. [Google Scholar] [CrossRef]


{kind=link}
| First Author | Year of Publication | Study Design | Included Patients | Conditioning Regimen | CD34+ Selection | Outcomes | Reported Adverse Events during the Transplantation Phase | Relapse Rates | Transplantation-Related Mortality | Length of Follow-Up |
|---|---|---|---|---|---|---|---|---|---|---|
| Burt et al. [52] | 2003 | Case series | 2 | Cy 200 mg/kg + ATG | Yes | 2/2 clinical remission, 2/2 endoscopic improvement | Febrile neutropenia (2) | None | None | 12 and 15 months |
| Craig et al. [53] | 2003 | Case series | 4 | Cy 200 mg/kg + ATG | Unknown | 4/4 clinical remission | Febrile neutropenia (4) | None | None | 2 weeks to one year |
| Scimè et al. [37] | 2004 | Case report | 1 | Cy 200 mg/kg + ATG | Yes | 1/1 clinical remission, 1/1 endoscopic improvement | Staphylococcus epidermidis bacteremia during neutropenia (1) | None | None | 5 months |
| Cassinotti et al. [39] | 2007 | Phase I/II, prospective | 4 | CY 200 mg/kg + ATG | No | 4/4 clinical remission, 2/3 endoscopic remission at 3 months | Febrile neutropenia (4), perianal abscess (1), pleural and pericardial effusions (1), BK virus-related macrohematuria (1) | 1/4 | None | 11–20 months |
| Burt et al. [38] | 2010 | Phase I/II, prospective | 24 | CY 200 mg/kg + ATG | Yes | clinical relapse-free survival: 91% after 1 year, 19% at 5 years | Febrile neutropenia, bacteremia (6) | 15/23 | None, 1 accidental death | 6 months to 5 years |
| Hommes et al. [40] | 2011 | Case series | 3 (2 transplanted) | CY 200 mg/kg + ATG | Yes | 2/2 clinical and endoscopic improvement at 8 to 10 weeks | Febrile neutropenia, allergic reaction to ATG, bacteremia (1), C. difficile infection (1), Rotavirus Infection (2) | 2/2 | None | 5–6 years |
| Hasselblatt et al. [41] | 2012 | Phase I/II, prospective | 12 (9 transplanted) | CY 200 mg/kg | Yes | 4/8 clinical remission after 6 months, 5/9 mucosal healing at 9 months | Febrile neutropenia, bacteremia (2), C. difficile infection (2) | 7/9 | None | 6 months to 10 years |
| Snowden et al. [42] | 2014 | Retrospective case series | 6 | CY 200 mg/kg + ATG | 2 out of 6 | 5/6 clinical remissison at 3 months, 5/6 endoscopic remission | Febrile neutropenia, bacteremia, upper gastrointestinal hemorrhage (1) | 6/6 | None | 50–123 months |
| Hawkey et al. [45] | 2015 | Phase II, open-label, randomized 1:1 | 45 (23 transplanted) | CY 200 mg/kg + ATG | No | 2/23 sustained disease remission at 1 year | 76 serious adverse events (viral infections (9), neutropenic sepsis (8) | 20/21 | 1 (SOS) | One year (primary endpoint) |
| Jauregui-Amezaga et al. [43] | 2016 | Phase I/II, prospective | 28 (21 transplanted) | CY 200 mg/kg + ATG | No | Not reported | Febrile neutropenia (20), bacteremia (8), septic shock (3), CMV infections (2: one death, one colectomy) | Not reported | 1 (CMV infection) | One year (primary endpoint) |
| Lindsay et al. [46] | 2017 | ASTIC trial post hoc analysis | 40 | CY 200 mg/kg + ATG | No | 13/34 steroid-free clinical remission, 19/38 endoscopic healing at 1 year | 76 serious adverse events in 23 patients | 7/38 restarted anti-TNF therapy | 1 (SOS) | One year (primary endpoint) |
| López-García et al. [44] | 2017 | Phase I/II, prospective | 35 (29 transplanted) | CY 200 mg/kg + ATG | No | Clinical and endoscopic relapse-free survival: 61% at one year, 15% at five years | Febrile neutropenia (23), septic shock (1), CMV infections (2: one death, one colectomy) | 15/28 | 1 (CMV infection) | 6–60 months |
| Ruiz et al. [26] | 2017 | Phase I/II, prospective | 14 | CY 200 mg/kg + ATG | No | 13/14 clinical remission at 30 days | 5 identified bacterial infections | 1/14 | None | 30 days |
| Brierley and Castilla-Llorente et al. [47] | 2018 | Retrospective survey | 82 | CY 200 mg/kg + ATG | 9 out of 82 | 51/80 clincial remission at 100 days | Infection within 1 year (22), secondary autoimmune diseases (9), malignancies (5) | 60/82 | 1 (CMV infection), 1 (sepsis at 8 years) | 6–174 months |
| Hernanz et al. [48] | 2018 | Retrospective case series | 7 | CY 200 mg/kg + ATG | No | 3/7 clinical and endoscopic remission, 1/7 clinical improvement at 6 months | Febrile neutropenia (6), C. difficile infection (1) | 5/7 | None | 17–78 months |
| Burt et al. [50] | 2020 | Pilot study | 9 | CY 200 mg/kg + Fludarabine + Alemtuzumab | No | 8/8 remission at 5 years | C. difficile infection (1), bacteremia (3), chronic limited GvHD (1) | 0/8 | 1 (adenovirus infection) | 5 years |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reider, S.; Binder, L.; Fürst, S.; Hatzl, S.; Blesl, A. Hematopoietic Stem Cell Transplantation in Refractory Crohn’s Disease: Should It Be Considered? Cells 2022, 11, 3463. https://doi.org/10.3390/cells11213463
Reider S, Binder L, Fürst S, Hatzl S, Blesl A. Hematopoietic Stem Cell Transplantation in Refractory Crohn’s Disease: Should It Be Considered? Cells. 2022; 11(21):3463. https://doi.org/10.3390/cells11213463
Chicago/Turabian StyleReider, Simon, Lukas Binder, Stefan Fürst, Stefan Hatzl, and Andreas Blesl. 2022. "Hematopoietic Stem Cell Transplantation in Refractory Crohn’s Disease: Should It Be Considered?" Cells 11, no. 21: 3463. https://doi.org/10.3390/cells11213463