
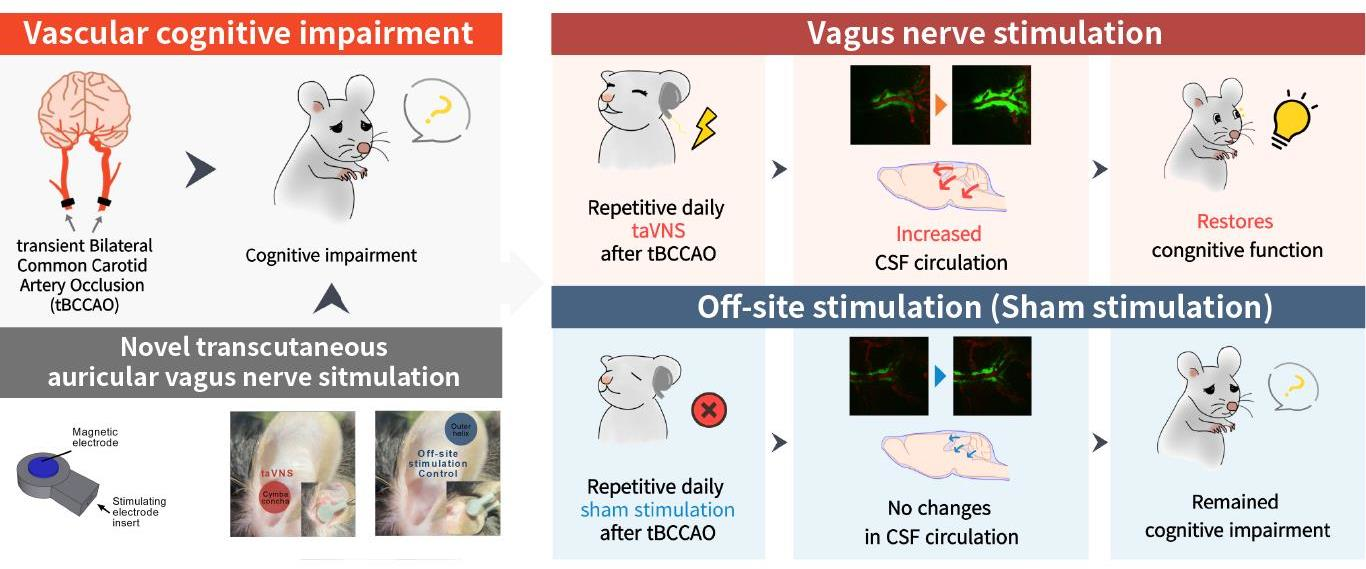
Transcutaneous Auricular Vagus Nerve Stimulation Enhances Cerebrospinal Fluid Circulation and Restores Cognitive Function in the Rodent Model of Vascular Cognitive Impairment

Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Electrode System
2.3. Stimulation Parameters
2.4. Procedures of Electrical Stimulation
2.5. Transient Global Cerebral Ischemia
2.6. Behavioral Assessments
2.7. Novel Object Recognition (NOR) Test
2.8. Y-maze Test
2.9. In Vivo Two-Photon Imaging
2.10. Data Analysis
3. Results
3.1. Development of the Preclinical taVNS Device and the Experimental Setup
3.2. taVNS Promoted CSF Circulation
3.3. Transient Bilateral Common Carotid Artery Occlusion (tBCCAO) Induced Cognitive Impairment
3.4. Repetitive taVNS Restored Impaired Cognitive Function
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- O’Brien, J.T.; Erkinjuntti, T.; Reisberg, B.; Roman, G.; Sawada, T.; Pantoni, L.; Bowler, J.V.; Ballard, C.; DeCarli, C.; Gorelick, P.B.; et al. Vascular Cognitive Impairment. Lancet Neurol. 2003, 2, 89–98. [Google Scholar] [CrossRef]
- Rost, N.S.; Brodtmann, A.; Pase, M.P.; van Veluw, S.J.; Biffi, A.; Duering, M.; Hinman, J.D.; Dichgans, M. Post-Stroke Cognitive Impairment and Dementia. Circ. Res. 2022, 130, 1252–1271. [Google Scholar] [CrossRef]
- Venkat, P.; Chopp, M.; Chen, J. Models and Mechanisms of Vascular Dementia. Exp. Neurol. 2015, 272, 97–108. [Google Scholar] [CrossRef]
- Iadecola, C. The Pathobiology of Vascular Dementia. Neuron 2013, 80, 844–866. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, J.T.; Thomas, A. Vascular Dementia. Lancet 2015, 386, 1698–1706. [Google Scholar] [CrossRef]
- Battle, C.E.; Abdul-Rahim, A.H.; Shenkin, S.D.; Hewitt, J.; Quinn, T.J. Cholinesterase Inhibitors for Vascular Dementia and Other Vascular Cognitive Impairments: A Network Meta-analysis. Cochrane Database Syst. Rev. 2021, 2021, CD013306. [Google Scholar] [CrossRef]
- Woodbury, D.M.; Woodbury, J.W. Effects of Vagal Stimulation on Experimentally Induced Seizures in Rats. Epilepsia 1990, 31, S7–S19. [Google Scholar] [CrossRef]
- McLachlan, R.S. Suppression of Interictal Spikes and Seizures by Stimulation of the Vagus Nerve. Epilepsia 1993, 34, 918–923. [Google Scholar] [CrossRef] [PubMed]
- Schachter, S.C.; Saper, C.B. Vagus Nerve Stimulation. Epilepsia 1998, 39, 677–686. [Google Scholar] [CrossRef]
- Vonck, K.; Raedt, R.; Naulaerts, J.; Vogelaere, F.D.; Thiery, E.; Roost, D.V.; Aldenkamp, B.; Miatton, M.; Boon, P. Vagus Nerve Stimulation…25 Years Later! What Do We Know about the Effects on Cognition? Neurosci. Biobehav. Rev. 2014, 45, 63–71. [Google Scholar] [CrossRef]
- Sanders, T.H.; Weiss, J.; Hogewood, L.; Chen, L.; Paton, C.; McMahan, R.L.; Sweatt, J.D. Cognition-Enhancing Vagus Nerve Stimulation Alters the Epigenetic Landscape. J. Neurosci. 2019, 39, 2407–2418. [Google Scholar] [CrossRef] [PubMed]
- Clark, K.B.; Krahl, S.E.; Smith, D.C.; Jensen, R.A. Post-Training Unilateral Vagal Stimulation Enhances Retention Performance in the Rat. Neurobiol. Learn Mem. 1995, 63, 213–216. [Google Scholar] [CrossRef] [PubMed]
- Clark, K.B.; Naritoku, D.K.; Smith, D.C.; Browning, R.A.; Jensen, R.A. Enhanced Recognition Memory Following Vagus Nerve Stimulation in Human Subjects. Nat. Neurosci. 1999, 2, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Sjogren, M.J.C.; Hellstrom, P.T.O.; Jonsson, M.A.G.; Runnerstam, M.; Silander, H.C.; Ben-Menachem, E.; Sjögren, J.C.; Hellström, P.T.O. Cognition-Enhancing Effect of Vagus Nerve Stimulation in Patients With Alzheimer’s Disease: A Pilot Study. J. Clin. Psychiatry 2002, 63, 972–980. [Google Scholar] [CrossRef]
- Merrill, C.A.; Jonsson, M.A.G.; Minthon, L.; Ejnell, H.; Silander, H.C.; Blennow, K.; Karlsson, M.; Nordlund, A.; Rolstad, S.; Warkentin, S.; et al. Vagus Nerve Stimulation in Patients with Alzheimer’s Disease: Additional Follow-Up Results of a Pilot Study Through 1 Year. J. Clin. Psychiatry 2006, 67, 1171–1178. [Google Scholar] [CrossRef]
- Kaan, E.; Aguiar, I.D.; Clarke, C.; Lamb, D.G.; Williamson, J.B.; Porges, E.C. A Transcutaneous Vagus Nerve Stimulation Study on Verbal Order Memory. J. Neurolinguist 2021, 59, 100990. [Google Scholar] [CrossRef]
- Jacobs, H.I.L.; Riphagen, J.M.; Razat, C.M.; Wiese, S.; Sack, A.T. Transcutaneous Vagus Nerve Stimulation Boosts Associative Memory in Older Individuals. Neurobiol. Aging 2015, 36, 1860–1867. [Google Scholar] [CrossRef]
- Vázquez-Oliver, A.; Brambilla-Pisoni, C.; Domingo-Gainza, M.; Maldonado, R.; Ivorra, A.; Ozaita, A. Auricular Transcutaneous Vagus Nerve Stimulation Improves Memory Persistence in Naïve Mice and in an Intellectual Disability Mouse Model. Brain Stimul. 2020, 13, 494–498. [Google Scholar] [CrossRef]
- Sakka, L.; Coll, G.; Chazal, J. Anatomy and Physiology of Cerebrospinal Fluid. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2011, 128, 309–316. [Google Scholar] [CrossRef]
- Brinker, T.; Stopa, E.; Morrison, J.; Klinge, P. A New Look at Cerebrospinal Fluid Circulation. Fluids Barriers Cns. 2014, 11, 10. [Google Scholar] [CrossRef] [Green Version]
- Orešković, D.; Klarica, M. The Formation of Cerebrospinal Fluid: Nearly a Hundred Years of Interpretations and Misinterpretations. Brain. Res. Rev. 2010, 64, 241–262. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Kitamura, A.; Beverley, J.; Koudelka, J.; Duncombe, J.; Lennen, R.; Jansen, M.A.; Marshall, I.; Platt, B.; Wiegand, U.K.; et al. Impaired Glymphatic Function and Pulsation Alterations in a Mouse Model of Vascular Cognitive Impairment. Front. Aging Neurosci. 2022, 13, 788519. [Google Scholar] [CrossRef] [PubMed]
- Attier-Zmudka, J.; Sérot, J.-M.; Valluy, J.; Saffarini, M.; Macaret, A.-S.; Diouf, M.; Dao, S.; Douadi, Y.; Malinowski, K.P.; Balédent, O. Decreased Cerebrospinal Fluid Flow Is Associated With Cognitive Deficit in Elderly Patients. Front. Aging Neurosci. 2019, 11, 87. [Google Scholar] [CrossRef] [PubMed]
- Cheng, K.P.; Brodnick, S.K.; Blanz, S.L.; Zeng, W.; Kegel, J.; Pisaniello, J.A.; Ness, J.P.; Ross, E.; Nicolai, E.N.; Settell, M.L.; et al. Clinically-Derived Vagus Nerve Stimulation Enhances Cerebrospinal Fluid Penetrance. Brain Stimul. 2020, 13, 1024–1030. [Google Scholar] [CrossRef] [PubMed]
- Butt, M.F.; Albusoda, A.; Farmer, A.D.; Aziz, Q. The Anatomical Basis for Transcutaneous Auricular Vagus Nerve Stimulation. J. Anat. 2020, 236, 588–611. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, K.; Tubbs, R.S.; Satoh, S.; Zomorodi, A.R.; Liedtke, W.; Labidi, M.; Friedman, A.H.; Fukushima, T. Isolated Deep Ear Canal Pain: Possible Role of Auricular Branch of Vagus Nerve—Case Illustrations with Cadaveric Correlation. World Neurosurg. 2016, 96, 293–301. [Google Scholar] [CrossRef]
- He, W.; Jing, X.-H.; Zhu, B.; Zhu, X.-L.; Li, L.; Bai, W.-Z.; Ben, H. The Auriculo-Vagal Afferent Pathway and Its Role in Seizure Suppression in Rats. BMC Neurosci. 2013, 14, 85. [Google Scholar] [CrossRef]
- Soares, L.M.; Schiavon, A.P.; Milani, H.; Oliveira, R.M.W. de Cognitive Impairment and Persistent Anxiety-Related Responses Following Bilateral Common Carotid Artery Occlusion in Mice. Behav. Brain. Res. 2013, 249, 28–37. [Google Scholar] [CrossRef]
- Antunes, M.; Biala, G. The Novel Object Recognition Memory: Neurobiology, Test Procedure, and Its Modifications. Cogn. Process 2012, 13, 93–110. [Google Scholar] [CrossRef]
- Taglialatela, G.; Hogan, D.; Zhang, W.-R.; Dineley, K.T. Intermediate- and Long-Term Recognition Memory Deficits in Tg2576 Mice Are Reversed with Acute Calcineurin Inhibition. Behav. Brain. Res. 2009, 200, 95–99. [Google Scholar] [CrossRef] [Green Version]
- Denninger, J.K.; Smith, B.M.; Kirby, E.D. Novel Object Recognition and Object Location Behavioral Testing in Mice on a Budget. J. Vis. Exp. 2018, 141, e58593. [Google Scholar] [CrossRef] [PubMed]
- Miedel, C.J.; Patton, J.M.; Miedel, A.N.; Miedel, E.S.; Levenson, J.M. Assessment of Spontaneous Alternation, Novel Object Recognition and Limb Clasping in Transgenic Mouse Models of Amyloid-β and Tau Neuropathology. J. Vis. Exp. JoVE 2017, 123, e55523. [Google Scholar] [CrossRef] [PubMed]
- Eguchi, K.; Shindo, T.; Ito, K.; Ogata, T.; Kurosawa, R.; Kagaya, Y.; Monma, Y.; Ichijo, S.; Kasukabe, S.; Miyata, S.; et al. Whole-Brain Low-Intensity Pulsed Ultrasound Therapy Markedly Improves Cognitive Dysfunctions in Mouse Models of Dementia—Crucial Roles of Endothelial Nitric Oxide Synthase. Brain Stimul. 2018, 11, 959–973. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.K.; Hayashi, H.; Ishikawa, T.; Shibata, K.; Shigetomi, E.; Shinozaki, Y.; Inada, H.; Roh, S.E.; Kim, S.J.; Lee, G.; et al. Cortical Astrocytes Rewire Somatosensory Cortical Circuits for Peripheral Neuropathic Pain. J. Clin. Investig. 2016, 126, 1983–1997. [Google Scholar] [CrossRef]
- Iliff, J.J.; Wang, M.; Liao, Y.; Plogg, B.A.; Peng, W.; Gundersen, G.A.; Benveniste, H.; Vates, G.E.; Deane, R.; Goldman, S.A.; et al. A Paravascular Pathway Facilitates CSF Flow Through the Brain Parenchyma and the Clearance of Interstitial Solutes, Including Amyloid β. Sci. Transl. Med. 2012, 4, 147ra111. [Google Scholar] [CrossRef]
- Kim, S.K.; Nabekura, J. Rapid Synaptic Remodeling in the Adult Somatosensory Cortex Following Peripheral Nerve Injury and Its Association with Neuropathic Pain. J. Neurosci. 2011, 31, 5477–5482. [Google Scholar] [CrossRef]
- Xavier, A.L.R.; Hauglund, N.L.; von Holstein-Rathlou, S.; Li, Q.; Sanggaard, S.; Lou, N.; Lundgaard, I.; Nedergaard, M. Cannula Implantation into the Cisterna Magna of Rodents. J. Vis. Exp. 2018, 135, e57378. [Google Scholar] [CrossRef]
- Burger, A.M.; D’Agostini, M.; Verkuil, B.; Diest, I.V. Moving beyond Belief: A Narrative Review of Potential Biomarkers for Transcutaneous Vagus Nerve Stimulation. Psychophysiology 2020, 57, e13571. [Google Scholar] [CrossRef]
- Ojeda, D.; Rolle, V.L.; Romero-Ugalde, H.M.; Gallet, C.; Bonnet, J.-L.; Henry, C.; Bel, A.; Mabo, P.; Carrault, G.; Hernández, A.I. Sensitivity Analysis of Vagus Nerve Stimulation Parameters on Acute Cardiac Autonomic Responses: Chronotropic, Inotropic and Dromotropic Effects. PLoS ONE 2016, 11, e0163734. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Shioda, N.; Han, F.; Moriguchi, S.; Nakajima, A.; Yokosuka, A.; Mimaki, Y.; Sashida, Y.; Yamakuni, T.; Ohizumi, Y.; et al. Nobiletin Improves Brain Ischemia-Induced Learning and Memory Deficits through Stimulation of CaMKII and CREB Phosphorylation. Brain Res. 2009, 1295, 218–229. [Google Scholar] [CrossRef]
- Jiwa, N.S.; Garrard, P.; Hainsworth, A.H. Experimental Models of Vascular Dementia and Vascular Cognitive Impairment: A Systematic Review. J. Neurochem. 2010, 115, 814–828. [Google Scholar] [CrossRef] [PubMed]
- Lv, T.; Zhao, B.; Hu, Q.; Zhang, X. The Glymphatic System: A Novel Therapeutic Target for Stroke Treatment. Front. Aging Neurosci. 2021, 13, 689098. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Li, Y.; Lenahan, C.; Ou, Y.; Wang, M.; He, Y. Glymphatic System in the Central Nervous System, a Novel Therapeutic Direction Against Brain Edema After Stroke. Front. Aging Neurosci. 2021, 13, 698036. [Google Scholar] [CrossRef]
- Tarasoff-Conway, J.M.; Carare, R.O.; Osorio, R.S.; Glodzik, L.; Butler, T.; Fieremans, E.; Axel, L.; Rusinek, H.; Nicholson, C.; Zlokovic, B.V.; et al. Clearance Systems in the Brain—Implications for Alzheimer Disease. Nat. Rev. Neurol. 2015, 11, 457–470. [Google Scholar] [CrossRef] [PubMed]
- Simard, J.M.; Kent, T.A.; Chen, M.; Tarasov, K.V.; Gerzanich, V. Brain Oedema in Focal Ischaemia: Molecular Pathophysiology and Theoretical Implications. Lancet Neurol. 2007, 6, 258–268. [Google Scholar] [CrossRef]
- Arbel-Ornath, M.; Hudry, E.; Eikermann-Haerter, K.; Hou, S.; Gregory, J.L.; Zhao, L.; Betensky, R.A.; Frosch, M.P.; Greenberg, S.M.; Bacskai, B.J. Interstitial Fluid Drainage Is Impaired in Ischemic Stroke and Alzheimer’s Disease Mouse Models. Acta Neuropathol. 2013, 126, 353–364. [Google Scholar] [CrossRef]
- Mestre, H.; Du, T.; Sweeney, A.M.; Liu, G.; Samson, A.J.; Peng, W.; Mortensen, K.N.; Stæger, F.F.; Bork, P.A.R.; Bashford, L.; et al. Cerebrospinal Fluid Influx Drives Acute Ischemic Tissue Swelling. Science 2020, 367, eaax7171. [Google Scholar] [CrossRef]
- Wang, F.; Liang, Z.; Hou, Q.; Xing, S.; Ling, L.; He, M.; Pei, Z.; Zeng, J. Nogo-A Is Involved in Secondary Axonal Degeneration of Thalamus in Hypertensive Rats with Focal Cortical Infarction. Neurosci. Lett. 2007, 417, 255–260. [Google Scholar] [CrossRef]
- Ong, L.K.; Zhao, Z.; Kluge, M.; Walker, F.R.; Nilsson, M. Chronic Stress Exposure Following Photothrombotic Stroke Is Associated with Increased Levels of Amyloid Beta Accumulation and Altered Oligomerisation at Sites of Thalamic Secondary Neurodegeneration in Mice. J. Cereb. Blood Flow Metab. 2016, 37, 1338–1348. [Google Scholar] [CrossRef]
- Van Groen, T.; Puurunen, K.; Mäki, H.-M.; Sivenius, J.; Jolkkonen, J. Transformation of Diffuse β-Amyloid Precursor Protein and β-Amyloid Deposits to Plaques in the Thalamus After Transient Occlusion of the Middle Cerebral Artery in Rats. Stroke 2005, 36, 1551–1556. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; Qi, D.; Li, J.; Deng, X.; Wang, D. Vagus Nerve Stimulation Enhances the Cholinergic Anti-Inflammatory Pathway to Reduce Lung Injury in Acute Respiratory Distress Syndrome via STAT3. Cell Death Discov. 2021, 7, 63. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Hao, X.; Li, C.; Sun, C.; Wang, X.; Yin, L.; Zhang, X.; Tian, J.; Yang, Y. Impaired Glymphatic System in Secondary Degeneration Areas after Ischemic Stroke in Rats. J. Stroke Cerebrovasc. Dis. 2020, 29, 104828. [Google Scholar] [CrossRef] [PubMed]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, S.; Jang, D.C.; Chung, G.; Kim, S.K. Transcutaneous Auricular Vagus Nerve Stimulation Enhances Cerebrospinal Fluid Circulation and Restores Cognitive Function in the Rodent Model of Vascular Cognitive Impairment. Cells 2022, 11, 3019. https://doi.org/10.3390/cells11193019
Choi S, Jang DC, Chung G, Kim SK. Transcutaneous Auricular Vagus Nerve Stimulation Enhances Cerebrospinal Fluid Circulation and Restores Cognitive Function in the Rodent Model of Vascular Cognitive Impairment. Cells. 2022; 11(19):3019. https://doi.org/10.3390/cells11193019
Chicago/Turabian StyleChoi, Seunghwan, Dong Cheol Jang, Geehoon Chung, and Sun Kwang Kim. 2022. "Transcutaneous Auricular Vagus Nerve Stimulation Enhances Cerebrospinal Fluid Circulation and Restores Cognitive Function in the Rodent Model of Vascular Cognitive Impairment" Cells 11, no. 19: 3019. https://doi.org/10.3390/cells11193019