1. Introduction
Atherosclerotic occlusions that develop in the lower extremities can result in a moderate to severe decrease in blood flow, resulting in tissue ischemia, which causes Peripheral Artery Disease (PAD). PAD is a large contributor to the global cardiovascular disease burden with >200 million patients worldwide [
1]. Approximately ~10% of PAD patients develop a severe form of PAD, critical limb ischemia (CLI), where tissue necrosis is a common incidence and is associated with high mortality [
2]. Improving blood flow by inducing angiogenesis in the ischemic muscle is an established approach to increase perfusion and improve walking and/or salvage the limb from amputation in PAD patients [
3]. Angiogenesis, the formation of new blood vessels from existing vasculature by vascular endothelial growth factor (VEGF)-A is perhaps the most extensively studied angiogenic pathway.
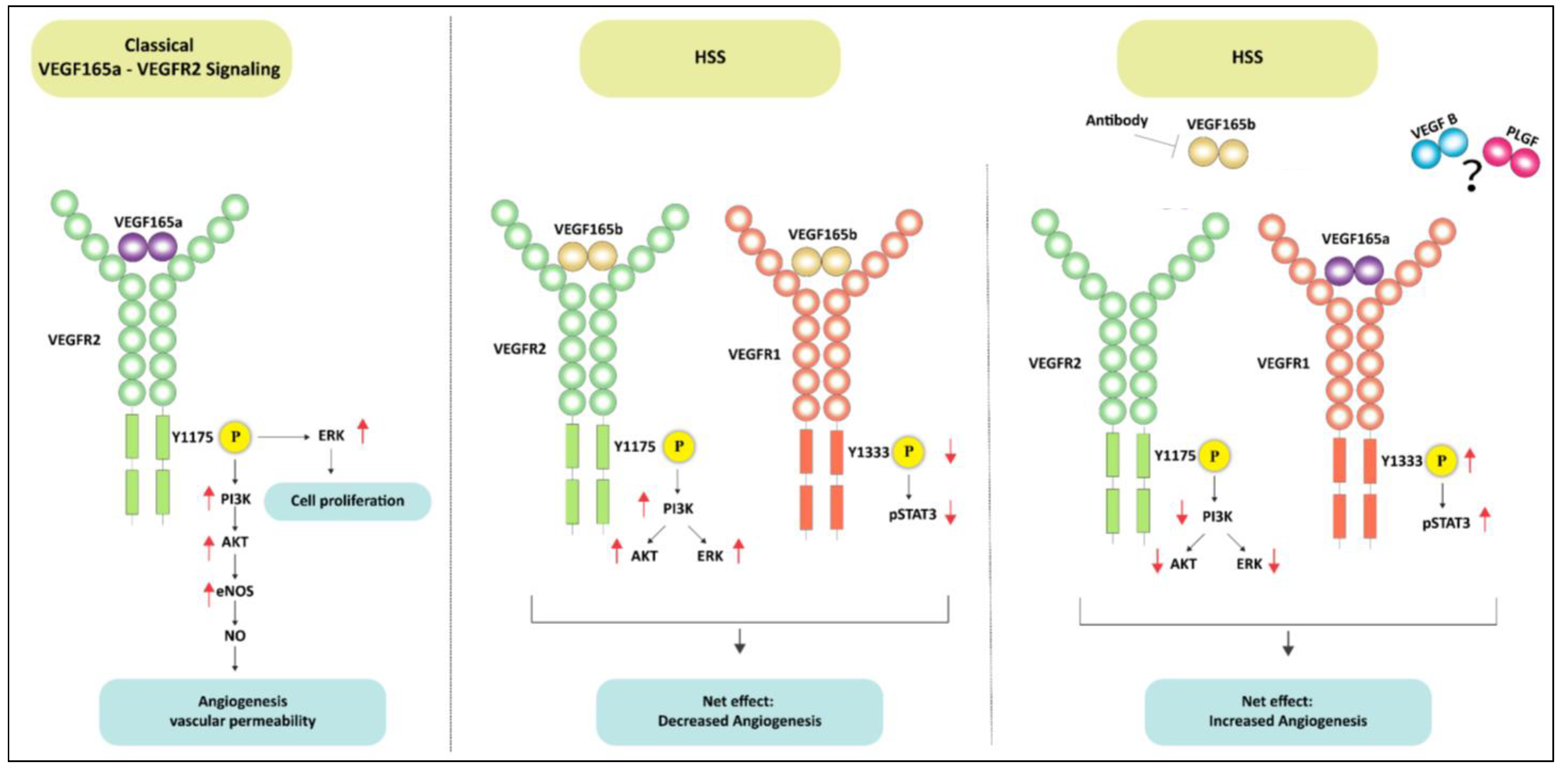
One of the major mechanisms by which VEGF-A regulates angiogenesis is by activating VEGFR2-AKT-ERK-eNOS signaling, which produces NO to induce angiogenesis. However, despite its ability to induce a strong pro-angiogenic phenotype in vitro and in vivo PAD models, none of the VEGF-A clinical trials or NO supplementation by L-arginine showed any clinical benefit in PAD [
4,
5,
6,
7]. A possible reason for their failures in PAD clinical trials could be explained based on the relatively recent recognition of increased anti-angiogenic VEGF
165b isoform production in ischemic muscle over pro-angiogenic VEGF
165a isoform [
8,
9]. The anti-angiogenic VEGF
165b isoforms occur by alternative splicing in the 8th exon of VEGF-A. These isoforms are considered to be ‘inactive competitive inhibitors’ of VEGFR2 signaling that act by competing with pro-angiogenic VEGF-A isoforms for binding sites on VEGFR2 [
10]. Previous studies have indicated that, unlike VEGF
165a, VEGF
165b is a weak agonist of VEGFR2 that can induce VEGFR2-phosphorylation, but not downstream signaling, needed to elicit an angiogenic response. As such VEGF
165b was thought to be an ‘inactive blocker’ of VEGF-A-induced VEGFR2 signaling [
11,
12,
13]. Limited information exists on VEGF
165b–VEGFR1 interactions in regulating endothelial function in cardiovascular pathologies [
14]. We have recently shown that VEGF
165b inhibits ischemic angiogenesis by decreasing VEGFR1 activation [
8]. Additionally, a previous study by Glass et al. [
14] showed the role of VEGF
165b–VEGFR1 interactions in regulating microvascular hydraulic conductivity in rat mesenteric vessels.
The rationale of this study is based on our data that (1) in human PAD muscle biopsies increased VEGF
165b binding to VEGFR2 correlated with increased VEGFR2 activation, whereas increased VEGF
165b binding to VEGFR1 correlated with decreased VEGFR1 activation vs. non-PAD controls, and (2) in in vitro competition studies, exogenous VEGF
165b-induced VEGFR2 activation almost to the same extent as VEGF
165a in ECs and (3) VEGF
165b inhibition-induced VEGFR1 activation without changes in VEGFR2 activation [
8]. Despite the ability to induce VEGFR2 activation, exogenous VEGF
165b treatment did not increase the angiogenic potential of normal or ischemic endothelial cells [
8]. Whereas depleting VEGF
165b using an isoform-specific monoclonal antibody against VEGF
165b isoform-induced angiogenesis by activating VEGFR1 signaling [
8,
15]. Consistent with our data, previous studies by Kawamura et al. [
13] and Catena et al. [
12] also showed that VEGF
165b induces VEGFR2 activation in pulmonary arterial endothelial (PAE) cells and Chinese Hamster Ovarian (CHO) cells that express VEGFR2, respectively [
12,
13]. On the contrary, Li et al. [
16] have shown that overexpressing VEGF
165b in ovarian cancer cell lines, including SKOV3 and OVCAR3, inhibits VEGFR2 signaling. However, the role of VEGF
165b in regulating VEGFR1 vs. VEGFR2 signaling in ischemic endothelial cells is not clear.
Based on these data, we questioned whether VEGFR1 activation achieved by VEGF
165b inhibition has the ability to induce ischemic angiogenesis even when VEGFR2-eNOS-NO signaling is impaired e.g., diabetic-PAD [
17,
18]. We used three preclinical PAD models, including (1) C57BL/6 mice on a high-fat diet (type 2 diabetic model well known to have impaired VEGFR2-eNOS-NO signaling [
17,
18], (2) eNOS deficient mice (eNOS-KO, that have defective NO generation [
19]), and (3) Myoglobin transgenic mice (Mg-Tg, which show defective angiogenesis due to impaired Nitric Oxide (NO) bioavailability [
20,
21]) in ischemic muscle to determine whether VEGFR1 activation is sufficient to induce angiogenesis and increase perfusion recovery in PAD.
2. Materials and Methods
2.1. Cells and Cell Culture
Human Umbilical Vein endothelial cells (HUVECs) were purchased and cultured in an all-in-one complete endothelial growth medium that contains 5 mM Glucose (Cat No.: 211-500) from Cell Applications Inc. (San Diego, CA, USA). HUVECs were purchased from Cell Applications and cultured in HUVEC growth medium [
8]. C57BL/6 Mouse Primary Skeletal Muscle Microvascular Endothelial Cells (Cat No.: C57-6220) were purchased and cultured in Complete Mouse Endothelial Cell Medium (Cat: M1168) from Cell Biologics (Chicago, IL, USA).
2.2. Recombinant Proteins and Reagents
Recombinant human VEGF165a (Cat No.: 293-VE) and recombinant human/murine VEGF165b (Cat No.: 3045-VE) were purchased from R&D (Minneapolis, MN, USA). Recombinant mouse VEGF165a (Cat No.: 200-34) was purchased from Shenandoah Biotechnology (Warwick, PA, USA). STATTIC (Cat No.: 27-981-0) was purchased from Tocris Biosciences (Minneapolis, MN, USA). BSA-Palmitate Saturated Fatty Acid Complex (5 mM, Cat No.: 29558) was purchased from Cayman Chemicals (Ann Arbor, MI, USA).
2.3. Cell Transfection
Non-targeting (Cat No.: D-001206-13-20) and VEGFR1 siRNA (Cat No.: M-003136-03-0005) were purchased from Horizon Discovery (Cambridge, UK). RNAiMax (Cat No.: 13778150) was purchased from ThermoFisher Scientific (Waltham, MA, USA). HUVECs were transfected with 150 nM control or VEGFR1 siRNA using RNAiMAX for 48 h according to the manufacturer’s instructions.
2.4. Antibodies
Antibodies against pVEGFR1 (Y1333-Cat No.: SAB4504006, Y1048-Cat No.: SAB4504649), pVEGFR2 (Y1175, Cat No.: SAB4504567), and VEGFR2 (Cat No.: SAB4501643) were purchased from Sigma-Aldrich, St. Louis, MO, USA; Flt1 (Cat No.: SC-316, raised against C-terminus amino acids between 1288–1338, and hence cannot bind to soluble Flt1) and VEGF-A (Cat No.: SC-7269) were purchased from Santa Cruz Biotechnology Inc., Dallas, TX, USA; VEGFR1 (Cat No.: PA5-16493) and CD31 (Cat No.: MA3105) purchased from ThermoFisher Scientific, Grand Island, NY, USA; VEGFR2 (Cat No.: 55B11), pAKT (Cat No.: 4060), AKT (Cat No.: 4691), pERK1/2 (Cat No.: 4370), ERK1/2 (Cat No.: 9102), pSTAT3 (Cat No.: 9145), and STAT3 (Cat No.: 12640) were purchased for Cell Signaling and Technology, Danvers, MA, USA; eNOS (Cat No.: 610299) was purchased from BD Pharmingen, San Jose, CA, USA; peNOS (Cat No.: 66127) from Abcam, Cambridge, MA, USA; VEGF-B (Cat No.: MAB751) and VEGF165b (Cat No.: MAB3045), used in Western blotting as well as to block VEGF165b in vitro and in vivo, was purchased from R&D, Minneapolis, MN, USA. PlGF antibody (Cat No.: SC1883, Santa Cruz Biotechnology) was a kind gift from Dr. Yao Liang Tang, Vascular Biology Center, Augusta University.
2.5. Cell Treatments
Confluent endothelial cells were treated with VEGF165a (50 ng/mL) or VEGF165b (50 ng/mL) for 10 min under normal growth conditions. HUVECs were challenged with hypoxia serum starvation for 24 h followed by treatment with VEGF165a (50 ng/mL) or VEGF165b (50 ng/mL) for 10 min.
2.6. Hypoxia Serum Starvation
Cells were incubated in an endothelial starvation medium purchased from Cell applications Inc. that contained 5 mM Glucose (Cat No.: 209-250) and were subjected to hypoxia (2% O2) for 24 h [
8,
15].
2.7. STAT3 Inhibition
Confluent ECs were treated with varying concentrations of STATTIC ranging from 0.1 μM to 1.0 μM for 24 h under normal growth conditions or HSS. Control cells received the same volume of DMSO as 1.0 μM STATTIC.
2.8. Palmitic Acid Treatment
Confluent ECs were treated with 500 μM BSA-Palmitate under HSS conditions for 24 h. Control cells received the same amount of BSA matching the amount of BSA-Palmitate.
2.9. In Vitro Diabetic-PAD Model
As an in vitro model for diabetic-PAD, HUVECs were incubated with 500 μM BSA-Palmitate in endothelial starvation medium and challenged with 2% hypoxia for 24 h. HUVECs treated with 500 μM BSA-Palmitate in a normal growth medium under normal growth conditions were used as a model for diabetes. Cells treated with an equal volume of BSA matching BSA-Palmitate treatment were used as a control in these experiments.
2.10. In Vitro Angiogenesis (Capillary-like Loop Formation) Assay
Endothelial cells post-treatments were trypsinized and the cell number was quantified using Corning CytoSmart cell counter. An equal number of cells (~15,000) were plated on growth factor reduced matrigel (Cat No.: 356231, R&D) to avoid any interference from VEGF-A present in the matrigel. Capillary-like tubes formed on the matrigel were photographed at 1 h, 2 h, and 3 h at the center concave, and the number of nodes was quantified by at least 2 people who were blinded to the treatments using NIH Image J Angiogenesis Analyzer [
8,
22].
2.11. Cell Proliferation
Endothelial cells were plated in 96 well plates at equal density. Post-treatment, cells were incubated with CCK9 at 1–2 h according to the manufacturer’s instructions. Post incubation, the plates were colorimetrically read at 450 nM using a BioTek Synergy LX Multi-Mode Plate Reader.
2.12. Mice
All animal experiments were approved by the Augusta University IACUC and conformed to the Guide for the Care and Use of Laboratory Animals published by the US National Institutes of Health. C57BL/6 mice on 60 kCal (high-fat diet) for 4 months were purchased from Jackson laboratories (DIO C57BL/6J Mice). Only males on a high-fat diet were used in T2D-PAD studies. Fasting glucose levels in these mice on a high-fat diet were measured by performing a glucose tolerance test using One Touch Ultra Glucometer and Strips according to our previous publications [
23,
24]. The basal glucose levels in the fasting mice used in the study were 189.7 ± 12.8 mg/dL, and the approximate weight of these mice at the time of performing hind limb ischemia experiments was ~43.6 ± 2.1 gm. Wild type C57BL/6, eNOS-KO mice, and Myoglobin transgenic mice were bred in the University of Virginia and Augusta University animal breeding facility. Both males and females were used in eNOS-KO and Mg-Tg studies.
2.13. Murine Model of Hind Limb Ischemia (HLI) and Microvascular Blood Flow Quantification
HLI was performed as described previously [
8,
16]. A combination of Ketamine (Ketathesia, (ZooPharm, 90 mg/kg) and Xylazine (Anased, Akorn, 10 mg/kg) was injected intraperitoneally (single dose) at 10 μL/gm mouse to induce anesthesia and perform unilateral femoral artery ligation and excision as a model of experimental PAD. Briefly, the femoral artery was ligated and resected from just above the inguinal ligament to its bifurcation at the origin of saphenous and popliteal arteries. Perfusion recovery was measured by quantifying microvascular blood flow by laser Doppler imaging (Perimed, Inc., Ardmore, PA, USA) on days 0, 3, 7, and 14 post-HLI. Perfusion in the ischemic limb was normalized to a non-ischemic limb for each mouse [
8,
15]. Mice were sacrificed with an overdose (20 μL/gm mouse) of Ketamine and Xylazine combination followed by cervical dislocation.
2.14. Necrosis Scores
The extent of necrosis was scored as follows: Grade I—involving only toes, Grade II—extending to dorsum pedis, Grade III—extending to crus, and Grade IV—extending to the thigh or complete necrosis [
8,
15].
2.15. Immunostaining
Gastrocnemius muscle tissues were fixed in 4% paraformaldehyde overnight at 4 °C, followed by RT for another 24 h. Later, tissues were incubated in 30% sucrose for ~24 h (until the tissues sink to the bottom) and embedded in OCT for cryosectioning. Thick cryosections of 5 µM were processed for immunostaining 12–14. Briefly, sections were washed in PBS twice followed by antigen retrieval in citrate buffer (Cat no: H3300, Vector Laboratories, Burlingame, CA, USA), blocked in 5% goat serum for 1 h, followed by incubation in CD31 antibody overnight at 4 °C. Later, sections were washed (PBS) and incubated in secondary antibodies conjugated to AlexaFluor-555 (Cat No.: A31572, ThermoFisher Scientific, Grand Island, NY, USA) for 2 h at RT. Sections were washed (PBS) and mounted using Prolong gold anti-fade mounting media (Cat No.: P36935, ThermoFisher Scientific, Grand Island, NY, USA). Immunofluorescent images were obtained using an EVOS-M5000 fluorescent microscope.
2.16. Terminal Deoxy-Uridine Nick End Labeling (TUNEL) Analysis
TUNEL assay was performed using Click-iT
® TUNEL Alexa Fluor
® 488 Imaging Assay (Cat No.: C10245) purchased from ThermoFisher Scientific, Grand Island, NY, USA, according to the manufacturer’s instructions, followed by immunostaining with CD31 antibody as described above. Four random images per section were photographed on EVOS M5000 fluorescent microscope and quantified as an average of TUNEL+ ECs per image between treatment groups [
8,
15].
2.17. Western Blot Analysis
At least 50 μgm of tissue or 20 μgm of cell lysates were resolved on SDS-PAGE and transferred onto nitrocellulose membrane for Western blotting as previously described, using the iBright Imaging System [
8,
15,
22].
2.18. Immunoprecipitation
~1 µg of the antibody was incubated in 50 μgm of protein lysates overnight at 4 °C in an end-to-end mixer. Antibody–antigen complexes were isolated by adding Goat-Anti-Rabbit (Cat No.: 21356) or Goat-Anti-Mouse (Cat No.: 21354) conjugated magnetic beads (ThermoFisher, Grand Island, NY, USA) for 2–3 h at room temperature. Antibody–antigen complexes were separated by boiling in sample buffer (Cat No.: BP-111R, Boston Bioproducts, Ashland, MA, USA) for 5–10 min, resolved in SDS-PAGE and Western blotted, as previously described [
8,
15].
2.19. Statistical Analysis
GraphPad Prism 9 was used to analyze the statistical significance of the data and generate graphical representations. An unpaired t-test was used to compare 2 specific groups. One-way ANOVA with Bonferroni select pair comparison or Dunnett’s post-tests were used to compare more than 2 groups. Repeated measures ANOVA was used for time-course laser doppler perfusion recovery measurements. A nonparametric Mann–Whitney test was used for necrosis scores. Statistical tests used to determine the significance of a specific experiment accompanied each figure legend. p < 0.05 is considered significant for all experiments. Data are presented as Mean ± SEM for all experiments.
3. Results
VEGF165b activates VEGFR2 signaling in normal and hypoxia serum starved ECs in vitro. Hypoxia is a known inducer of VEGF-A [
25,
26,
27]. To determine whether hypoxia serum starvation (HSS), an in vitro PAD model [
8,
15,
28,
29,
30] also induces VEGF-A levels, we performed a Western blot analysis of VEGF-A in normal and HSS HUVECs using a pan-VEGF-A antibody that recognizes all the VEGF-A isoforms (pro- and anti-angiogenic) [
8,
15,
31,
32,
33,
34]. Western blot analysis showed a numerical increase in total VEGF-A levels in HSS-challenged HUVECs vs. normal (
Supplementary Figure S1). Using an isoform-specific monoclonal antibody [
8], we have previously shown that HSS induces significantly higher VEGF
165b levels in HUVECs [
8]. More importantly, in human PAD, we observed that the fraction of VEGF
165b is ~3X higher than the pro-angiogenic VEGF-A levels [
8]. Taken together, our current data indicate that the fraction of pro-angiogenic VEGF
165a is decreased, and the fraction of anti-angiogenic VEGF
165b isoform is increased in HSS HUVECs vs. normoxic controls.
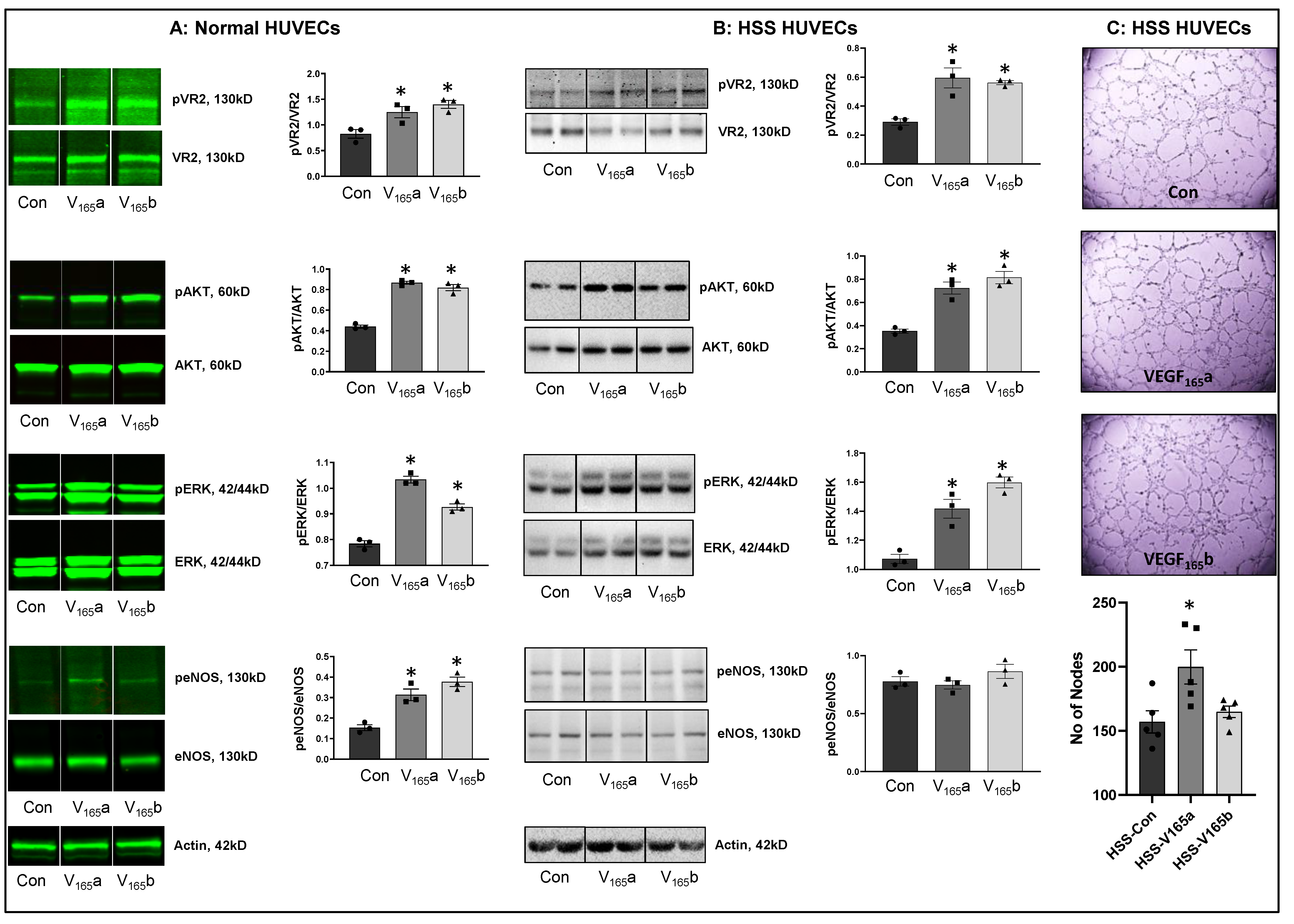
We next determined whether VEGF
165b-induced VEGFR2-phosphorylation results in the activation of downstream AKT-ERK-eNOS signaling similar to VEGF
165a in confluent ECs under normoxia or challenged with HSS (an in vitro model of PAD, HSS-HUVECs). The immunoblots of normal HUVECs treated with recombinant-VEGF
165b or recombinant-VEGF
165a showed a significant increase in pVEGFR2
Y1175 (V
165a: ~1.5-fold, V
165b: ~1.7-fold), pAKT (V
165a: ~1.9-fold, V
165b: ~1.9-fold), pERK (V
165a: ~1.3-fold, V
165b: ~1.2-fold), and peNOS (V
165a: ~2.0-fold, V
165b: ~2.4-fold) activation almost to the same extent vs. untreated controls (
Figure 1A). These data indicate that VEGF
165b activates this VEGFR2-AKT-ERK signaling to the same extent as VEGF
165a in normal ECs, confirming the data from previously published data from other groups [
12,
13,
33,
35].
We next examined the role of VEGF
165b in regulating VEGFR2 signaling in HSS-HUVECs. Immunoblot analysis showed that both VEGF
165b and VEGF
165a induced pVEGFR2
Y1175 (~2-fold), pAKT (~2-fold), and pERK activation to the same extent in HSS-HUVECs vs. untreated controls (
Figure 1B). Interestingly, no significant difference in eNOS activation was observed in HSS-HUVECs treated with VEGF
165a or VEGF
165b (
Figure 1B). These data indicate that VEGF
165b is not a competitive inhibitor but an activator of VEGFR2 signaling even in HSS-HUVECs. Despite the ability of VEGF
165b to activate the pro-angiogenic VEGFR2 signaling, VEGF
165b did not induce the angiogenic capacity of HSS-HUVECs vs. untreated controls (
Figure 1C), suggesting that the anti-angiogenic function of VEGF
165b is not dependent on inhibiting VEGFR2 signaling. Furthermore, immunoblot analysis showed that while VEGF
165a significantly decreased total VEGFR2 and AKT levels, VEGF
165b treatment did not induce significant differences in their expression. Both VEGF
165a and VEGF
165b significantly induced ERK levels without affecting the expression of eNOS or VEGFR1 vs. untreated controls (
Supplementary Figure S2).
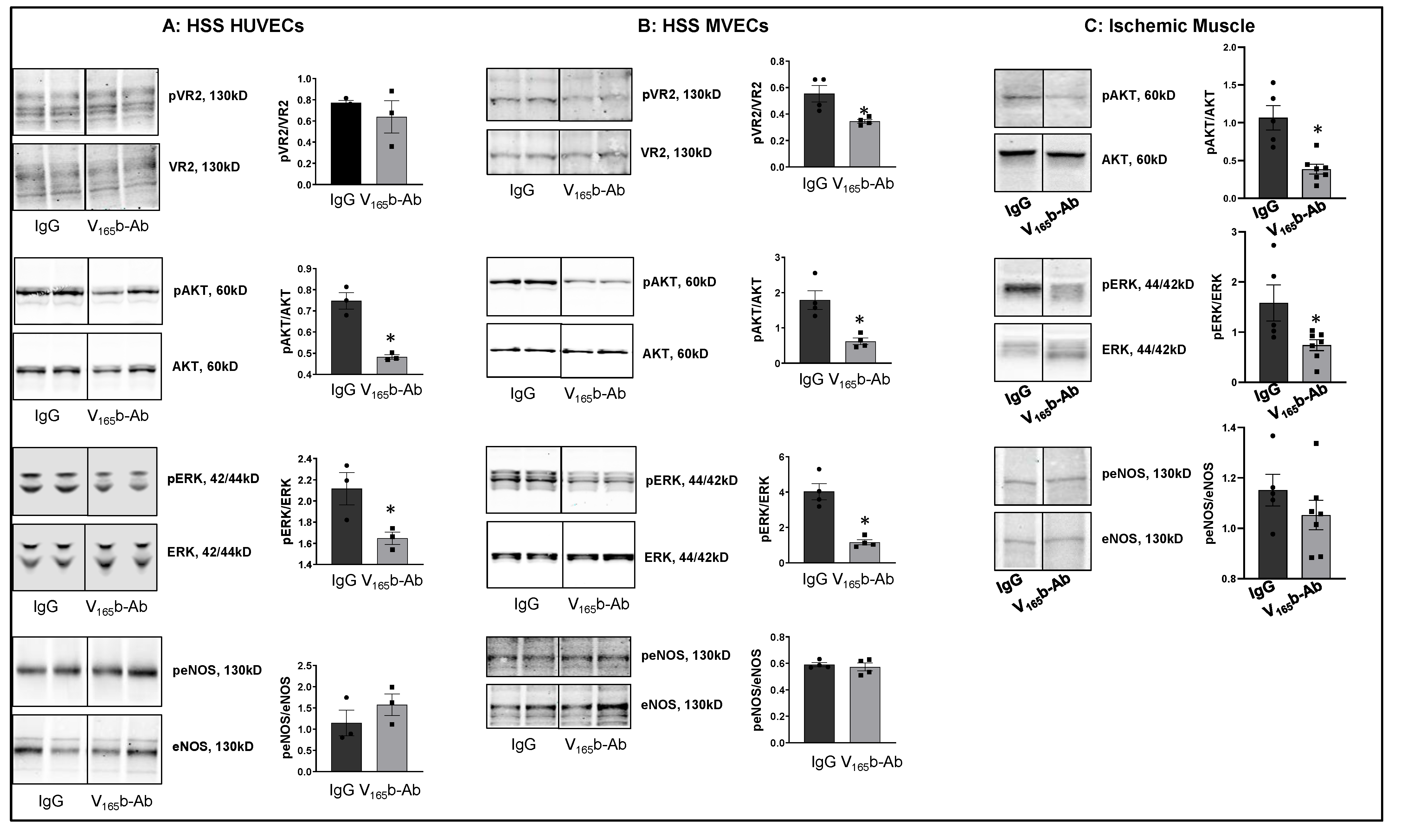
VEGF165b inhibition decreases VEGFR2 signaling in ischemic ECs in vitro and in vivo. To determine the role of VEGF
165b inhibition in regulating VEGFR1 vs. VEGFR2 activation, we treated HSS-HUVECs or HSS-mouse skeletal muscle ECs (HSS-MVECs) with isotype-matched IgG or VEGF
165b-Ab (10 μg/mL [
8,
15]). HSS-HUVECs treated with VEGF
165b-Ab showed no significant difference in pVEGFR2
Y1175 activation but significantly decreased pAKT (~1.5-fold), and pERK (~1.3-fold) activation (
Figure 2A). HSS-MVECs treated with VEGF
165b-Ab showed a significant decrease in pVEGFR2
Y1175 (~1.8-fold), pAKT (~3.6-fold) and pERK (~3.9-fold) activation vs. IgG (
Figure 2B). No significant difference in peNOS was observed in VEGF
165b-Ab-treated HSS-HUVECs or HSS-MVECs vs. IgG (
Figure 2A,B).
To confirm the role of VEGF
165b inhibition in regulating VEGFR2 signaling in vivo, we performed immunoblot analysis of day 3 ischemic muscle samples treated with IgG or VEGF
165b-Ab (200 µg, i.m, three non-overlapping sites in Balb/c mice gastrocnemius and tibialis anterior muscles). Immunoblot analysis showed that VEGF
165b-Ab significantly decreased pAKT (~5.1-fold) and pERK (~2.9-fold) activation with no changes in peNOS activation vs. IgG (
Figure 2C).
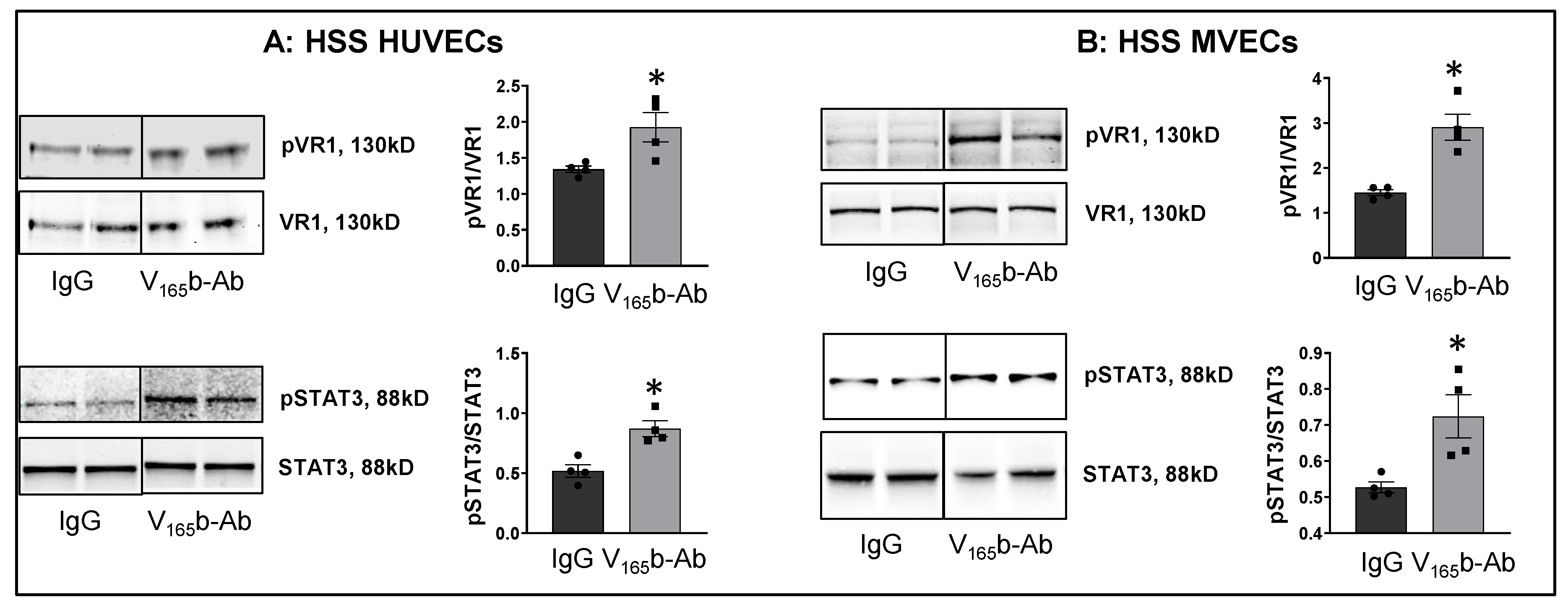
We next examined whether VEGF
165b-Ab induces VEGFR1 activation in HSS-HUVECs and HSS-MVECs. Immunoblot analysis showed that VEGF
165b-Ab-treated HSS-HUVECs and HSS-MVECs have significantly higher pVEGFR1
Y1333 (HSS-HUVEC: ~1.6-fold, HSS-MVEC: ~1.4-fold) and pSTAT3 (HSS-HUVEC: ~1.3-fold, HSS-MVEC: ~1.6-fold) activation vs. IgG (
Figure 3A,B). While HSS increases VEGF
165b levels in HUVECs [
8], a significant decrease in VEGF-B and PLGF (VEGFR1 specific ligands) levels was observed in HSS-HUVECs (
Supplementary Figure S3). These data suggest that endogenously produced VEGF
165b acts as an autocrine inhibitor of VEGFR1 in HSS-HUVECs.
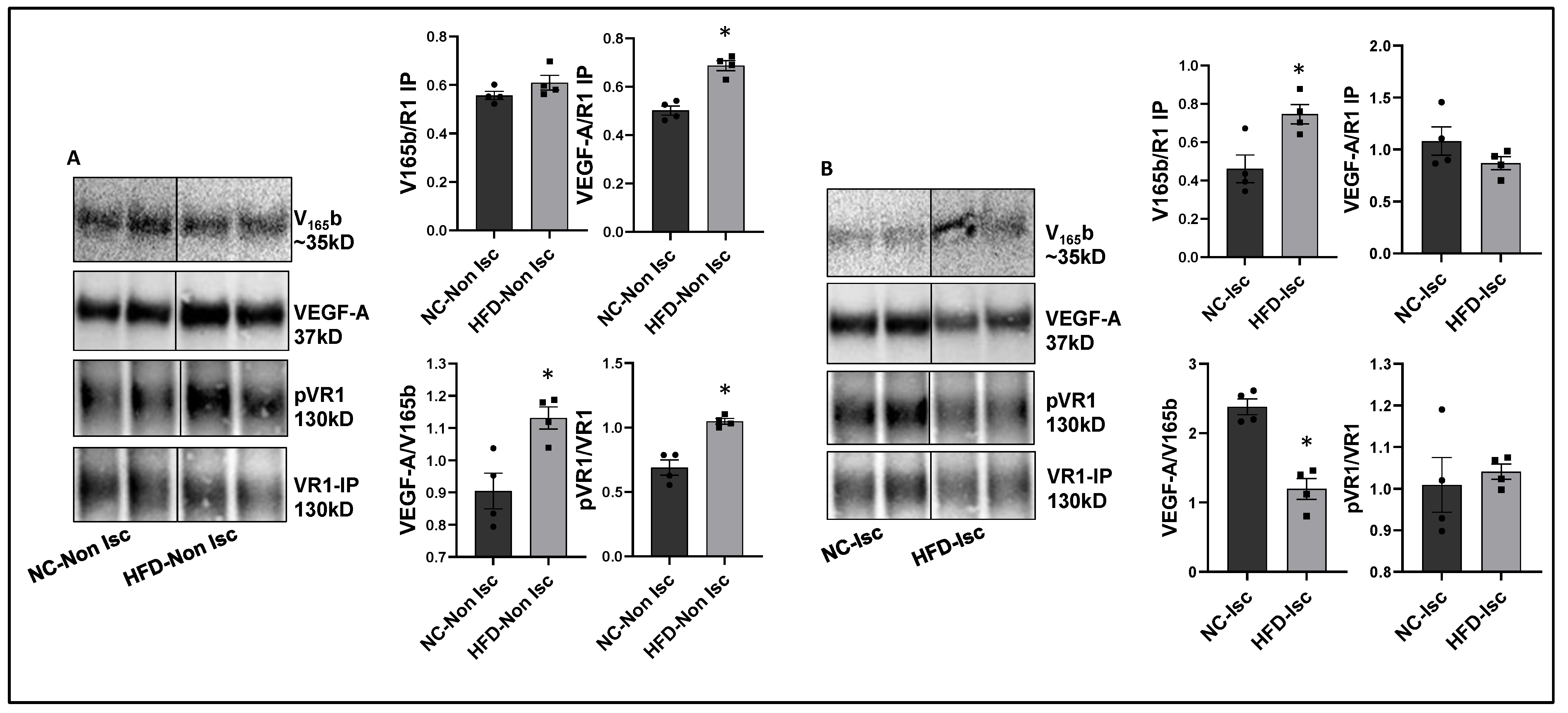
VEGF165b inhibition enhances perfusion in Type-2 diabetic-PAD mice. Immunoblot analysis to determine the relative levels of VEGF
165b and total VEGF-A showed no significant differences between a non-ischemic high-fat diet (HFD, 60 kCal for 4 months) vs. normal chow-fed mice skeletal muscle samples (
Supplementary Figure S4A). However, VEGFR1 pull-down fractions from non-ischemic HFD vs. non-ischemic normal chow samples showed a significant decrease in the fraction of VEGF
165b bound to VEGFR1 (~1.3-fold,
Figure 4A), which inversely correlated with increased pVEGFR1
Y1333 activation in non-ischemic HFD samples vs. non-ischemic normal chow samples (~1.5-fold,
Figure 4A).
We next examined the relative levels of VEGF
165b and total VEGF-A in ischemic HFD samples vs. ischemic normal chow samples at day 3 post-HLI, a time point at which the extent of perfusion recovery is comparable between the two groups. Immunoblot analysis showed no significant difference in VEGF
165b or total VEGF-A levels between ischemic HFD samples vs. ischemic normal chow samples (
Supplementary Figure S4B). Interestingly, VEGFR1 pull-down fractions showed a significant increase in the bound VEGF
165b fraction in HFD-ischemic samples vs. ischemic normal chow samples (~1.2-fold). No significant difference in pVEGFR1
Y1333 activation was observed between HFD-ischemic samples vs. normal chow ischemic samples (
Figure 4B) suggesting that increased VEGF
165b binding to VEGFR1 in HFD-ischemic muscle blocked VEGFR1 activation. No significant difference in pVEGFR1
Y1333 (
Supplementary Figure S5A), pVEGFR2
Y1175, or pAKT activation was observed in HFD-ischemic muscle vs. normal chow ischemic muscle (
Supplementary Figures S4C and S5B). However, a significant increase in pERK activation was observed in HFD-ischemic muscle vs. normal chow ischemic muscle (
Supplementary Figure S5D) suggesting that a VEGFR2-independent mechanism regulates ERK activation in HFD-ischemic muscle.
After confirming that ischemia induces VEGF
165b binding to VEGFR1 in HFD skeletal muscle, we determined the functional role of VEGF
165b-Ab in regulating perfusion recovery in HFD-ischemic muscle. VEGF
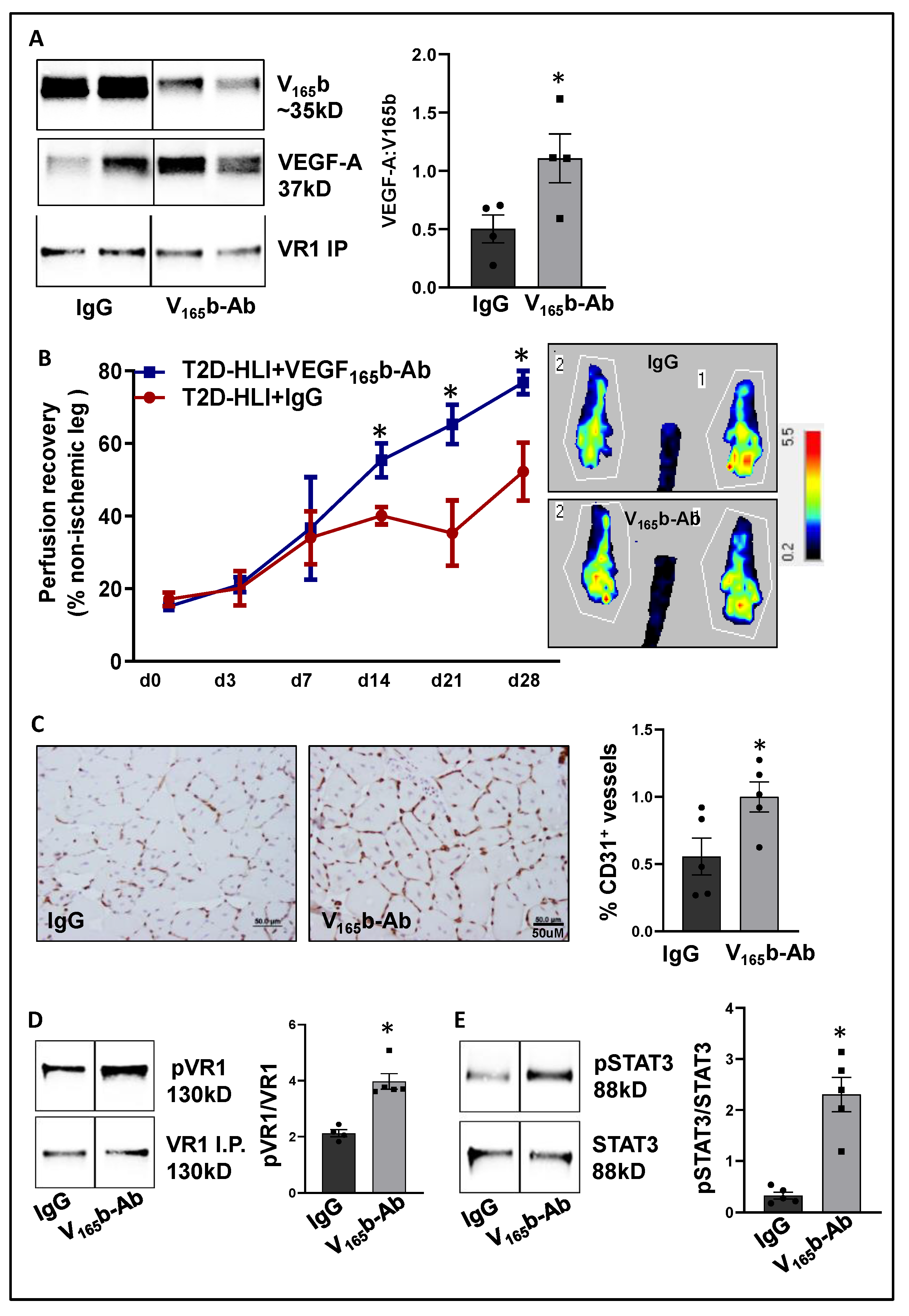
165b-Ab or isotype-matched IgG (200 µg/100 μL PBS/mouse) was injected intramuscularly into HFD mouse gastrocnemius (two non-overlapping sites) and tibialis anterior (one site) immediately after HLI (d0) and days 3, 7, 14, and 21 post-HLI. VEGFR1 pull-down at day 3 post HLI with IgG or VEGF
165b-Ab-treated samples showed a significant increase in total VEGF-A bound to VEGFR1 indicating that VEGF
165b binding to VEGFR1 was reduced by VEGF
165b-Ab treatment (
Figure 5A). Laser Doppler showed that VEGF
165b-Ab significantly improved limb perfusion (day 14: IgG-40.1 ± 2.4 vs. V
165b-Ab-55.35 ± 4.7; day 21: IgG-35.3 ± 9.0 vs. V
165b-Ab-65.22 ± 5.4; day 28: IgG-52.1 ± 8 vs. V
165b-Ab-76.7 ± 3.2) in HFD-ischemic muscle vs. IgG (
Figure 5B). The immunohistochemical analysis of CD31 at day 28 post-HLI samples showed a significant increase in microvascular density in VEGF
165b-Ab-treated HFD-ischemic muscle vs. IgG (
Figure 5C).
We next performed immunoblot analysis to determine changes in VEGFR1 vs. VEGFR2 signaling in VEGF
165b-Ab vs. IgG-treated HFD-ischemic muscle on day 3 post-HLI. Immunoblot analysis showed a significant increase in pVEGFR1
Y1333 (~1.5-fold,
Figure 5D) and pSTAT3 (~1.5-fold,
Figure 5E) activation in VEGF
165b-Ab-treated HFD-ischemic muscle vs. IgG. While no significant differences in pVEGFR2
Y1175, pERK, or peNOS were observed between VEGF
165b-Ab vs. IgG-treated HFD-ischemic muscle samples, a significant increase in pAKT (~1.8-fold) activation was observed in VEGF
165b-Ab-treated HFD-ischemic muscle vs. IgG (
Supplementary Figure S6). We have previously shown that VEGFR1 directly interacts with STAT3 to induce STAT3 activation [
8]. To test whether STAT3 regulates AKT activation, normal or HSS-HUVECs were treated with STAT3 inhibitor, STATTIC [
36] in a dose-dependent manner. Immunoblot analysis showed that 1.0 μM STATTIC significantly decreased AKT activation in both normal and HSS-HUVECs (
Supplementary Figure S7A,B), indicating that STAT3 can regulate AKT activation in the endothelium. Furthermore, the immunoblot analysis of Bcl2, Bax (downstream effectors of STAT3 in regulating apoptosis [
30]), and caspase-3 at day 3 post-HLI showed a significant increase in the ratio of Bcl2/Bax (~2.9-fold,
Supplementary Figure S8A) and a significant decrease in activated caspase-3 levels (~2.3-fold,
Supplementary Figure S8B) in VEGF
165b-Ab-treated HFD-ischemic muscle vs. IgG. These data suggested that activation of VEGFR1-STAT3 signaling by blocking VEGF
165b decreased cell death and increased microvascular density to enhance perfusion recovery in HFD-ischemic muscle.
VEGF165b inhibition decreases limb necrosis in eNOS-KO mice. eNOS-KO mice have a severely impaired response to HLI. More importantly, VEGF-A superfusion failed to induce angiogenesis in eNOS-KO mice [
19,
37]. Hence, we used eNOS-KO mice to determine whether VEGF
165b-Ab can improve tissue perfusion/recovery in preclinical PAD. The immunoblot analysis of VEGF
165b and total VEGF-A at day 3 post-HLI showed a significant decrease in the ratio of VEGF-A:VEGF
165b levels (~2.7-fold,
Supplementary Figure S9A) in eNOS-KO vs. WT ischemic muscle, indicating that VEGF
165b levels predominate in eNOS-KO mice ischemic muscle vs. WT. Furthermore, the immunoblot analysis of VEGFR1 activation showed a significant decrease in pVEGFR1
Y1333 activation (~1.4-fold,
Supplementary Figure S9B) in eNOS-KO ischemic muscle vs. WT. These data show that a significant increase in VEGF
165b levels decreases pVEGFR1
Y1333 activation in eNOS-KO ischemic muscle vs. WT. Total protein was used to normalize due to differences in Actin expression between WT vs. eNOS-KO ischemic muscle (Supplemental immunoblots for
Figure 5).
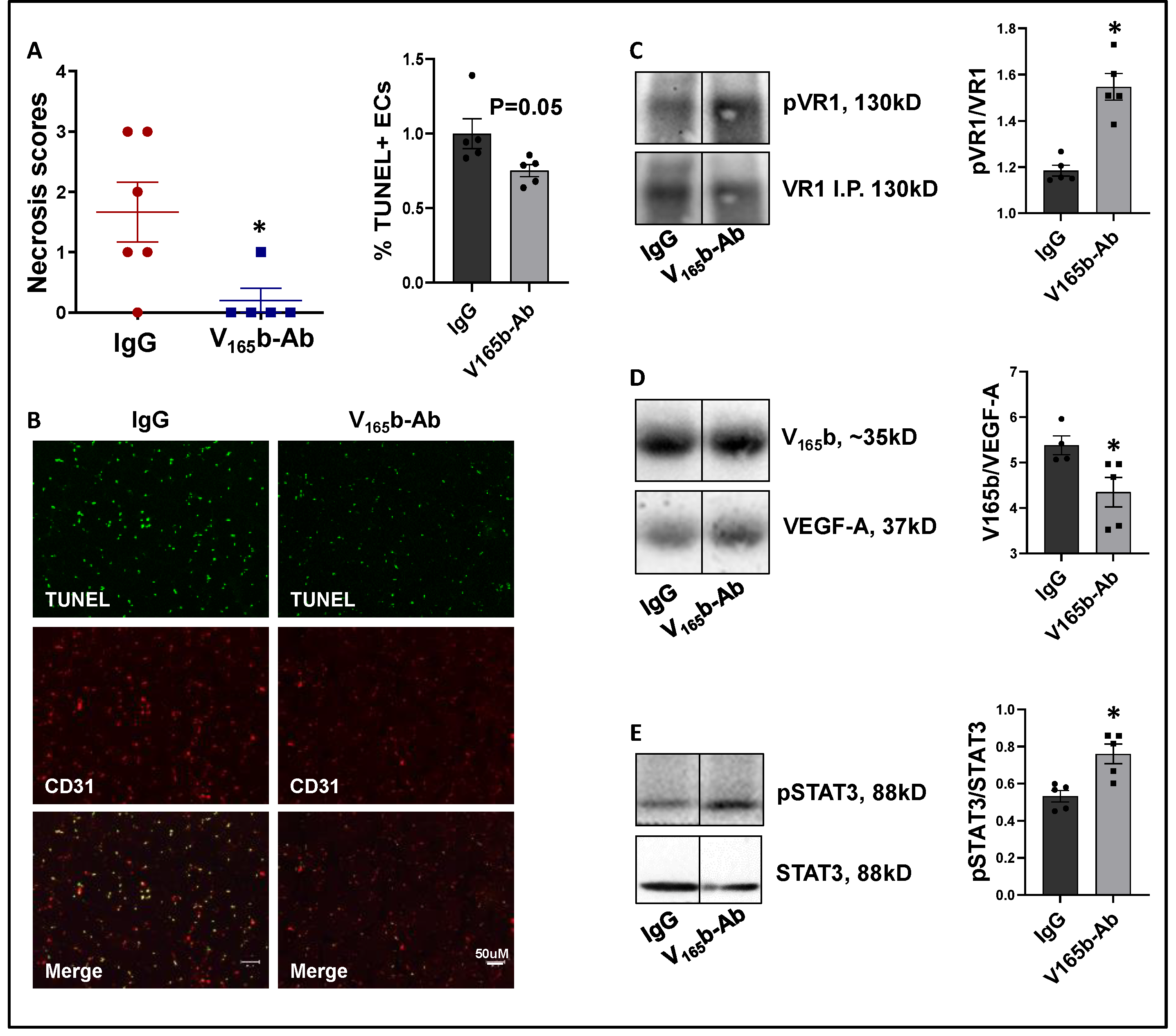
VEGF
165b-Ab significantly decreased limb necrosis in eNOS-KO ischemic muscle vs. IgG-treated eNOS-KO ischemic muscle (
Figure 6A). TUNEL analysis to determine the extent of EC death showed that VEGF
165b-Ab decreased TUNEL
+ (Green) CD31
+ (Red) apoptotic ECs (
p = 0.05,
Figure 6B) in eNOS-KO ischemic muscle vs. IgG. We next examined whether decreased limb necrosis and cell death in VEGF
165b-Ab-treated eNOS-KO ischemic muscle are due to activation of VEGFR1 signaling. VEGFR1 pulldown fractions in eNOS-KO ischemic muscle treated with VEGF
165b-Ab or IgG showed a significant decrease in the fraction of VEGF
165b bound to VEGFR1 (~1.2-fold,
Figure 6C) in eNOS-KO ischemic muscle vs. IgG. A significant increase in pVEGFR1
Y1333 activation (~1.3-fold,
Figure 6D) was observed in VEGFR1 pull-down fractions in eNOS-KO ischemic muscle treated with VEGF
165b-Ab vs. IgG. VEGFR1 activation resulted in a significant increase in pSTAT3 activation (~1.4-fold,
Figure 6E) in eNOS-KO muscle treated with VEGF
165b-Ab vs. IgG. These data indicate that decreased VEGF
165b binding to VEGFR1 in eNOS-KO muscle treated with VEGF
165b-Ab allowed for the activation of VEGFR1-STAT3 signaling that protected eNOS-KO ischemic muscle from necrosis.
We next performed immunoblot analysis to examine whether VEGF
165b-Ab modulated the VEGFR2 signaling intermediates AKT and ERK. VEGF
165b-Ab in eNOS-KO ischemic muscle did not induce any changes in pAKT activation (
Supplementary Figure S10A) but induced pERK activation (~1.2-fold,
Supplementary Figure S10B) vs. IgG.
VEGF165b inhibition enhances perfusion in myoglobin transgenic (Mg-Tg) PAD mice that have impaired NO bioavailability. Excessive myoglobin expression in Mg-Tg mice skeletal muscle functions as a nitric oxide sink and impairs perfusion recovery [
20,
21,
38]. Hence, we determined whether VEGF
165b-Ab could induce perfusion recovery despite the lack of the capacity to increase NO bioavailability. Immunoblot analysis to determine relative changes in VEGF
165b vs. total VEGF-A at day 3 post-HLI, (a time point where the perfusion recovery between WT and Mg-Tg mice is comparable) showed no significant difference in the ratio of total VEGF-A to VEGF
165b between WT vs. Mg-Tg ischemic muscle (
Supplementary Figure S11A). Immunoblot analysis, used to determine changes in VEGFR1 activation between WT vs. Mg-Tg, showed that the total VEGFR1 levels are significantly lower in Mg-Tg ischemic muscle vs. WT (~3.5-fold decrease, (
Supplementary Figure S11B). Since there was a significant decrease in total VEGFR1 levels in Mg-Tg ischemic muscle vs. WT, the extent of pVEGFR1
Y1333 activation was compared with total protein levels (Ponceau), which showed a significant decrease in Mg-Tg ischemic muscle vs. WT, correlating with decreased VEGFR1 levels (
Supplementary Figure S11B). Total protein was used to normalize due to differences in Actin expression between WT vs. Mg-Tg ischemic muscle (Supplemental immunoblots for
Figure 6).
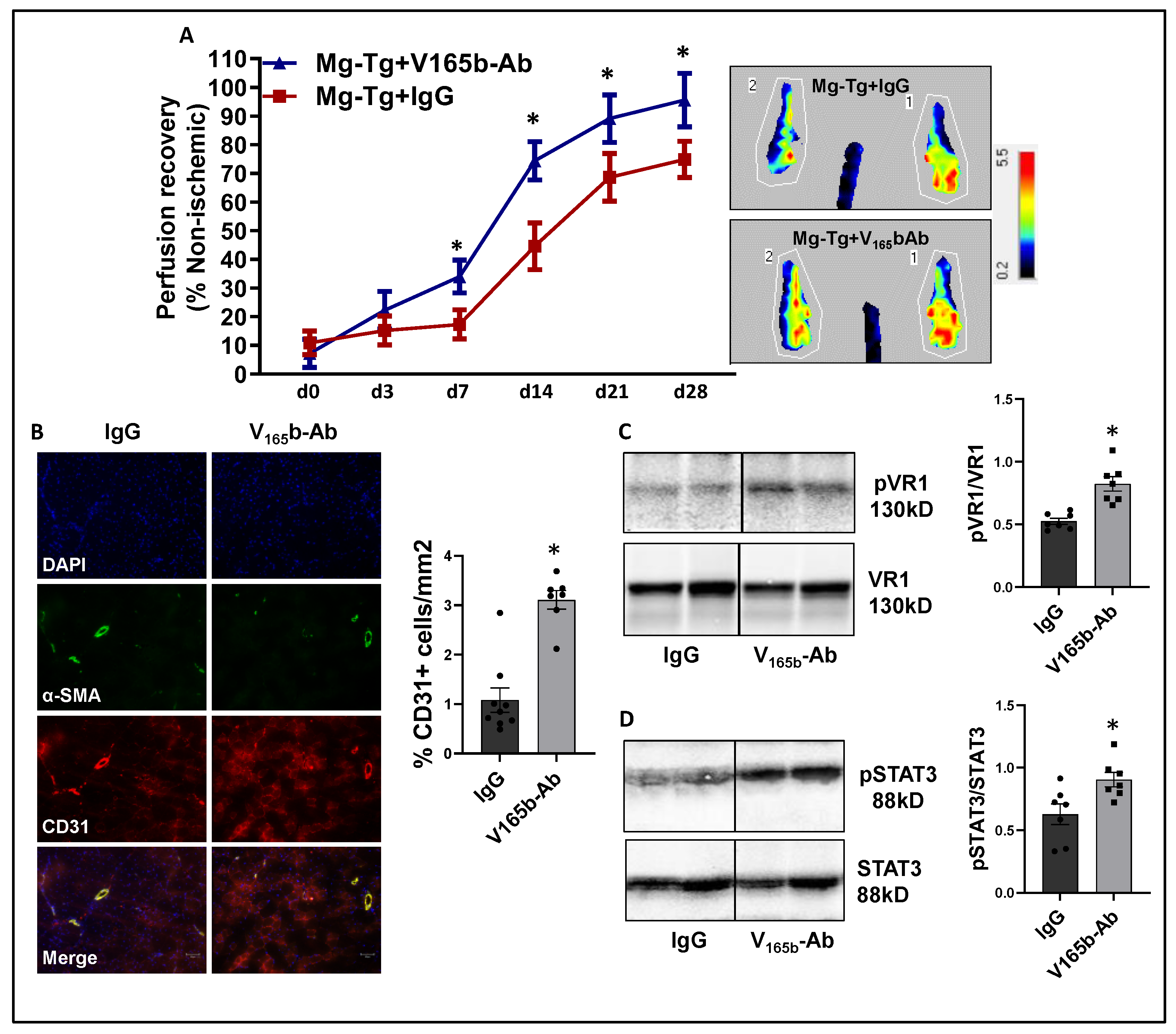
Laser Doppler showed that VEGF
165b-Ab in Mg-Tg ischemic muscle significantly enhanced perfusion recovery (d7: IgG-17.3 ± 1.7 vs. V
165b-Ab-34.0 ± 2.1; d14: IgG-44.6 ± 2.9 vs. V
165b-Ab-74.4 ± 2.5; d21: IgG-68.6 ± 2.7 vs. V
165b-Ab-89.1 ± 3.1; d28: IgG-74.8 ± 2.1 vs. V
165b-Ab-95.6 ± 3.5) vs. IgG (
Figure 7A). The immunohistochemistry of CD31 showed a significant increase in CD31+ cells (~3-fold) in Mg-Tg ischemic muscle treated with VEGF
165b-Ab vs. IgG, indicating that VEGF
165b inhibition can induce microvascular density despite a lack of NO bioavailability (
Figure 7B). We next performed immunoblot analysis to determine whether enhanced perfusion and microvascular density are due to activation of VEGFR1-STAT3 signaling in VEGF
165b-Ab-treated Mg-Tg ischemic muscle. Immunoblot analysis showed a significant increase in pVEGFR1
Y1333 activation (~1.5-fold,
Figure 7C) and pSTAT3 activation (~1.3-fold,
Figure 7D) in VEGF
165b-Ab-treated Mg-Tg ischemic muscle vs. IgG indicating that the activation of VEGFR1-STAT3 signaling by VEGF
165b inhibition-induced microvascular density and promoted perfusion recovery in Mg-Tg ischemic muscle. Finally, we performed immunoblot analysis of VEGFR2 signaling intermediates, including pAKT and pERK in Mg-Tg ischemic muscle. VEGF
165b inhibition in Mg-Tg ischemic muscle significantly decreased pAKT activation (~1.6-fold,
Supplementary Figure S12A) but not pERK activation vs. IgG (
Supplementary Figure S12B).
VEGF165b inhibition induces an angiogenic response by activating VEGFR1 signaling in an in vitro diabetic-PAD model of impaired VEGFR2 signaling. Previous studies have demonstrated that plasma levels of palmitic acid (PA) have a strong association with Type-2 diabetes patients [
39,
40] and inhibit AKT, ERK, and eNOS activation as well as a VEGF-A-induced tube-like formation on Matrigel [
41,
42,
43]. Based on these data, we developed an in vitro model of diabetic-PAD, wherein HUVECs were challenged with HSS in the presence of palmitic acid (PA, as an in vitro model for diabetes) to determine an EC-specific role of VEGF
165b-VEGFR1 signaling in regulating angiogenesis in a pathologically relevant in vitro model with impaired VEGFR2 signaling.
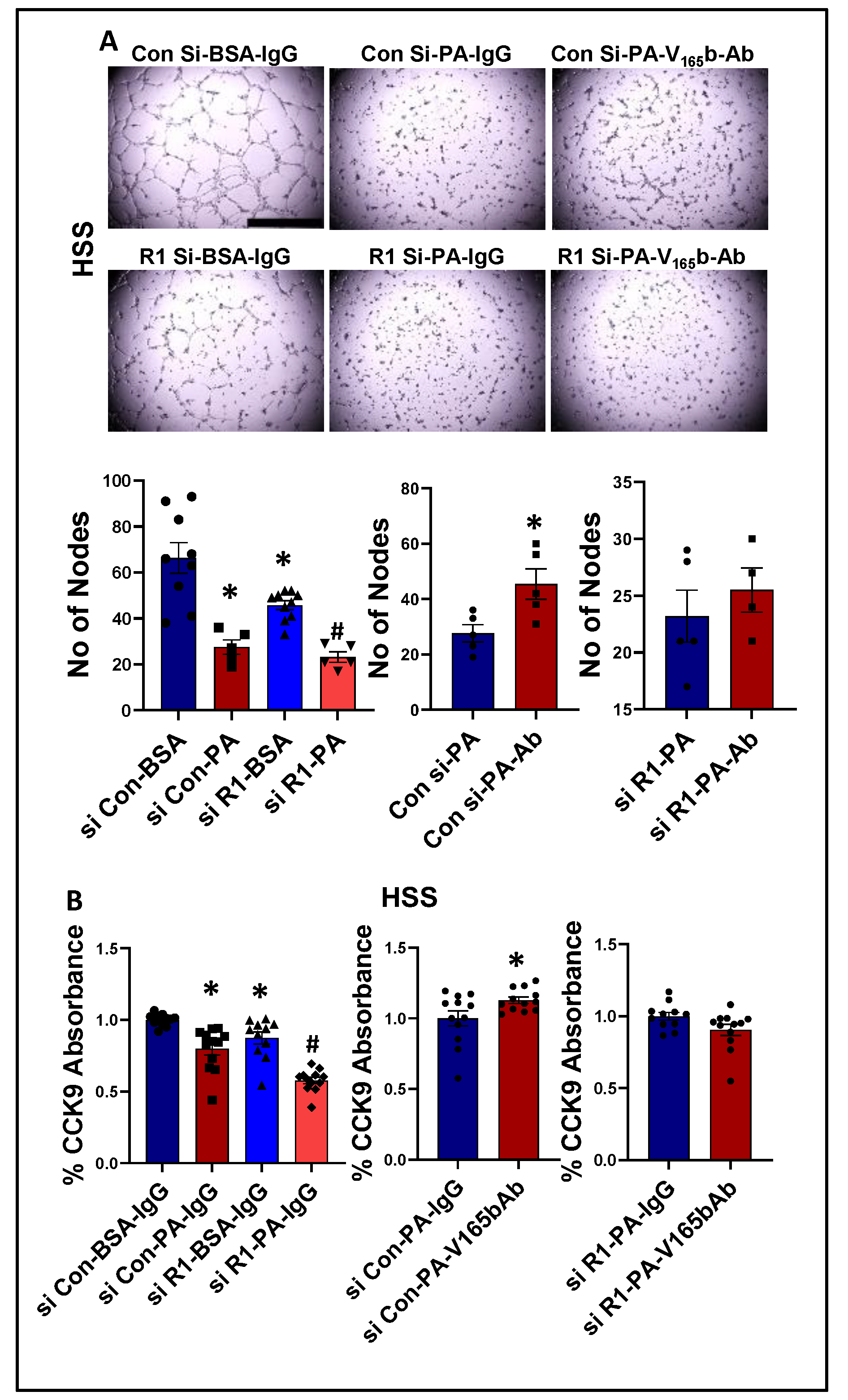
We next determined whether PA impairs endothelial angiogenic capacity and VEGF
165b inhibition can rescue the PA-induced angiogenic inhibition. Matrigel analysis showed a significant decrease in the angiogenic capacity in normal (~2.2-fold,
Supplementary Figure S13A) and HSS (~2.4-fold,
Figure 8A)-HUVECs treated with PA vs. BSA. VEGFR1-silencing (
Supplementary Figure S14) further decreased the angiogenic capacity of PA-treated normal HUVECs (~3-fold,
Supplementary Figure S13A). However, due to a severe angiogenic inhibition in PA-treated HSS-HUVECs, we were not able to observe a further inhibition in the angiogenic capacity of VEGFR1-silenced HSS-HUVECs treated with PA (
Figure 8A). VEGF
165b-Ab significantly increased the angiogenic capacity of PA treated normal (~1.5-fold,
Supplementary Figure S13A) and HSS-HUVECs (~1.6-fold,
Figure 8A) vs. IgG. VEGF
165b-Ab did not affect the angiogenic capacity of VEGFR1-silenced normal or HSS-HUVECs treated with PA (
Supplementary Figure S13A,
Figure 8A), indicating that VEGFR1 is necessary for VEGF
165b-Ab to rescue PA-induced angiogenic impairment. We further confirmed these findings by performing cell survival assays in in vitro diabetic-PAD models. PA treated normal (
Supplementary Figure S13B) or HSS (
Figure 8B) HUVECs showed a significant decrease in cell proliferation/survival vs. BSA. VEGFR1 silencing further decreased the angiogenic capacity of PA-treated normal and HSS-HUVECs (
Supplementary Figure S13B,
Figure 8B). While VEGF
165b-Ab significantly increased the cell proliferation/survival in normal and HSS-HUVECs treated with PA; VEGF
165b-Ab did not affect the cell proliferation/survival in VEGFR1 silenced normal or HSS-HUVECs treated with PA (
Supplementary Figure S13B,
Figure 8B).
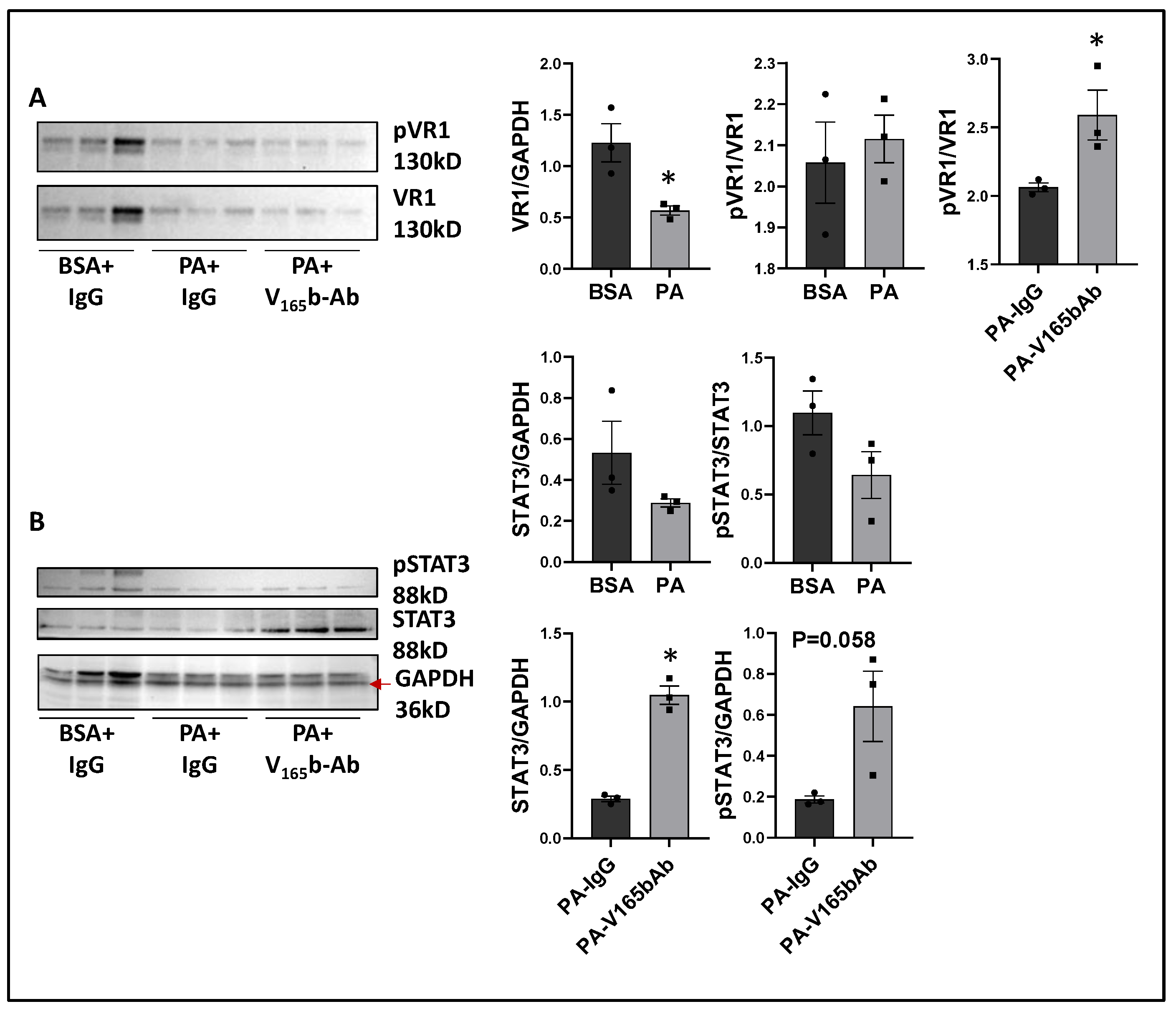
We next determined the signaling changes induced by PA in HSS-HUVECs and the signaling induced by VEGF
165b-Ab in PA-treated HSS-HUVECs that resulted in increased angiogenesis. Immunoblot analysis showed no significant difference in VEGF
165b vs. total VEGF-A levels between PA vs. BSA-treated HSS-HUVECs (
Supplementary Figure S15). However, PA significantly decreased total VEGFR1 levels vs. BSA-treated HSS-HUVECs (~1.8-fold,
Figure 9A). VEGF
165b-Ab did not affect total VEGFR1 levels in PA-treated HSS-HUVECs but induced pVEGFR1
Y1333 activation vs. IgG (
p = 0.046, ~1.4-fold,
Figure 9A). We next performed immunoblot analysis of pSTAT3 activation to confirm VEGFR1 signaling activation. No significant difference in STAT3 levels was observed between PA vs. BSA-treated HSS-HUVECs (
Figure 9B). Interestingly, VEGF
165b-Ab induced a dramatic upregulation of STAT3 levels and only a numeric but non-significant increase in pSTAT3 levels (
p = 0.058) vs. IgG-treated PA-HSS-HUVECs (
Figure 9B).
We next performed the immunoblot analysis of pVEGFR2
Y1175, pAKT, and pERK activation to examine whether PA impairs VEGFR2 signaling in HSS-HUVECs; and whether VEGF
165b-Ab modulates VEGFR2 signaling in PA-treated HSS-HUVECs. Immunoblot analysis of VEGFR2 showed a significant decrease in VEGFR2 levels in PA-treated HSS-HUVECs vs. BSA (
Supplementary Figure S16A). VEGF
165b-Ab did not affect total VEGFR2 levels or pVEGFR2
Y1175 activation in PA-treated HSS-HUVECs vs. IgG. Immunoblot analysis of AKT showed no significant difference in AKT levels between PA- and BSA-treated HUVECs (
Supplementary Figure S16B). VEGF
165b-Ab did not affect pAKT activation in PA-treated HSS-HUVECs vs. IgG. The immunoblot analysis of ERK showed no significant difference in ERK levels in PA-treated HSS-HUVECs vs. BSA (
Supplementary Figure S16C). However, a significant increase in pERK activation was observed between PA- vs. BSA-treated HSS-HUVECs. VEGF
165b-Ab did not affect pERK activation in PA-treated HSS-HUVECs vs. IgG (
Supplementary Figure S16C).
4. Discussion
Attempts to promote therapeutic angiogenesis in humans have been underway for almost two decades but the studies have been met with limited success. VEGF was one of the extensively studied agents [
44]. Potential explanations for the lack of success with VEGF include inadequate dosing to activate VEGFR signaling in ischemic tissue, but the inability of humans to activate VEGFR2-Akt-eNOS-NO in an ischemic environment remains a plausible explanation. In a prior experimental PAD study, where the VEGFR2-Akt-eNOS-NO system could be activated, we demonstrated that VEGF
165b was upregulated and acted as an anti-angiogenic agent via VEGFR1, but not via VEGFR2 [
8,
15]. Here we demonstrate that a monoclonal antibody targeting VEGF
165b [
8,
9] was able to promote therapeutic angiogenesis in systems where NO production is impaired and/or its bioavailability is reduced. These data fill important gaps in the consideration of therapeutics for PAD.
In mice models, and in humans, diabetes further impairs arteriogenesis and angiogenesis in PAD muscle compared with PAD muscle alone [
18,
23]. Attenuated VEGFR2 signaling in murine Type-2 diabetic (high-fat diet) ischemic muscle (T2D-HLI) has been shown to play a causal role in inhibiting perfusion recovery [
17,
18,
45]. We hypothesized that an induction in VEGF
165b isoform in T2D-HLI muscle plays a causal role in inhibiting angiogenesis in T2D-HLI. We have previously shown that ischemia induces anti-angiogenic VEGF
165b levels in endothelial cells challenged with hypoxia serum starvation vs. normal growth conditions; and in endothelial cells from ischemic muscle vs. non-ischemic muscle [
8]. However, treating endothelial cells with Palmitate and hypoxia serum starvation as a model for T2D-PAD did not further increase VEGF
165b levels. Accordingly, no significant differences in either total VEGF-A or VEGF
165b levels were observed between normal vs. T2D ischemic muscle. However, the fraction of VEGF
165b bound to VEGFR1 was significantly higher resulting in the loss of VEGFR1 activation in the ischemic muscle from T2D-PAD mice vs. ischemic muscle from mice on normal chow. Removing the inhibitory effect of VEGF
165b bound to VEGFR1 allowed VEGFR1-STAT3 signaling activation that resulted in increased angiogenesis and perfusion recovery in T2D-HLI muscle. A previous study by Kikuchi et al. showed that VEGF
165b inhibition increased both collateral (assessed as SMA+ vessels) and microvascular density in diabetic mouse models, including the high fat-high sucrose diet model and Ob-Ob mice model [
9]. Taken together, VEGF
165b inhibition induces both arteriogenesis and angiogenesis in ischemic diabetic muscle to enhance perfusion recovery. The ability of VEGFR1-STAT3 signaling to induce angiogenesis and perfusion recovery in the T2D-HLI model presented a critical role of VEGFR1-STAT3 signaling to induce therapeutic angiogenesis in PAD.
Previous reports have shown that VEGF
165b, an alternatively spliced VEGF-A isoform blocks VEGF-A-induced angiogenesis by inhibiting VEGFR2 activation. On the contrary VEGF
165b has been shown to be a weak activator of VEGFR2 albeit under normal growth conditions [
12,
13,
33,
35]. Consistently, our results show that VEGF
165b induces VEGFR2 and downstream AKT-ERK-eNOS signaling to a similar extent as VEGF
165a both under normal growth conditions, and when challenged with HSS, an in vitro model used to simulate the PAD muscle that is deprived of oxygen and growth factors [
3,
8,
15]. Despite its ability to activate VEGFR2, the angiogenic capacity of VEGF
165b is lower vs. VEGF
165a indicating that VEGF
165b inhibits angiogenesis independent of VEGFR2 in ischemic vasculature. Accordingly, VEGF
165b inhibition decreased VEGFR2 signaling in HSS-HUVECs, indicating that VEGF
165b is a potent activator of VEGFR2. A schematic of these data is presented in
Figure 10.
To confirm the role of VEGF
165b inhibition in activating VEGFR1 in T2D-PAD vasculature, we developed an in vitro model of T2D-PAD. Diabetes is one of the most important risk factors for amputation in PAD patients [
46]. Microvascular abnormalities and impaired angiogenesis result in ulcers and decreased wound healing in patients with PAD and diabetes [
47]. Hence, we wanted to establish an in vitro model for diabetic-PAD. Previous studies have shown that palmitic acid induces reactive oxygen species, induces cell death, inhibits cell proliferation, and impairs angiogenesis in vitro [
48,
49]. Multivariate regression analysis of the data collected from the Insulin Resistance Atherosclerosis Study (IRAS) showed a strong association of palmitic acid with Type-2 diabetes risk independent of insulin sensitivity [
50]. Furthermore, Reynoso et al. [
51] have suggested that high palmitic acid levels lead to insulin resistance [
51]. Taking these studies into consideration, we have employed a treatment where ECs are treated with starvation medium supplemented with palmitic acid followed by subjecting them to hypoxia. We hypothesized that this combinatorial treatment will be closer in vitro model for diabetic-PAD. Consistent with our hypothesis, ECs treated with palmitic acid showed a significant loss in their angiogenic capacity vs. normal controls; and ECs treated with serum starvation + palmitic acid under hypoxic conditions showed further loss of angiogenic capacity vs. serum starvation + hypoxia. Inhibiting VEGF
165b in the context of this in vitro T2D-PAD model was able to rescue impaired angiogenesis. More importantly, VEGF
165b inhibition induced VEGFR1 activation without affecting VEGFR2 activation or downstream signaling.
To confirm whether VEGFR1 activation can induce therapeutic angiogenesis and perfusion independent of NO, we used eNOS-KO mice [
19] and Myoglobin-transgenic mice [
20,
21] in the HLI model. Interestingly, while VEGF-A levels are significantly lower in eNOS-KO mice ischemic muscle; VEGF-A levels are significantly increased in Myoglobin-transgenic mice vs. their respective controls. NO has been shown to regulate VEGF-A synthesis [
20,
52]. In eNOS-KO ischemic muscle, a severe decrease in NO production could have resulted in decreased VEGF-A levels. Whereas in Myoglobin-transgenic mice, scavenging of NO by skeletal muscle, could have resulted in higher VEGF-A production/levels by skeletal muscle cells. Interestingly, while VEGF
165b inhibition-induced ERK activation without changes in AKT activation in eNOS-KO ischemic muscle, VEGF
165b inhibition in Mg-Tg ischemic muscle-inhibited AKT activation with no changes in ERK suggesting distinct VEGFR1 signaling events are activated post-VEGF
165b inhibition across these mouse models.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}









