
Harmful Impact of Tobacco Smoking and Alcohol Consumption on the Atrial Myocardium


Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Materials and Methods
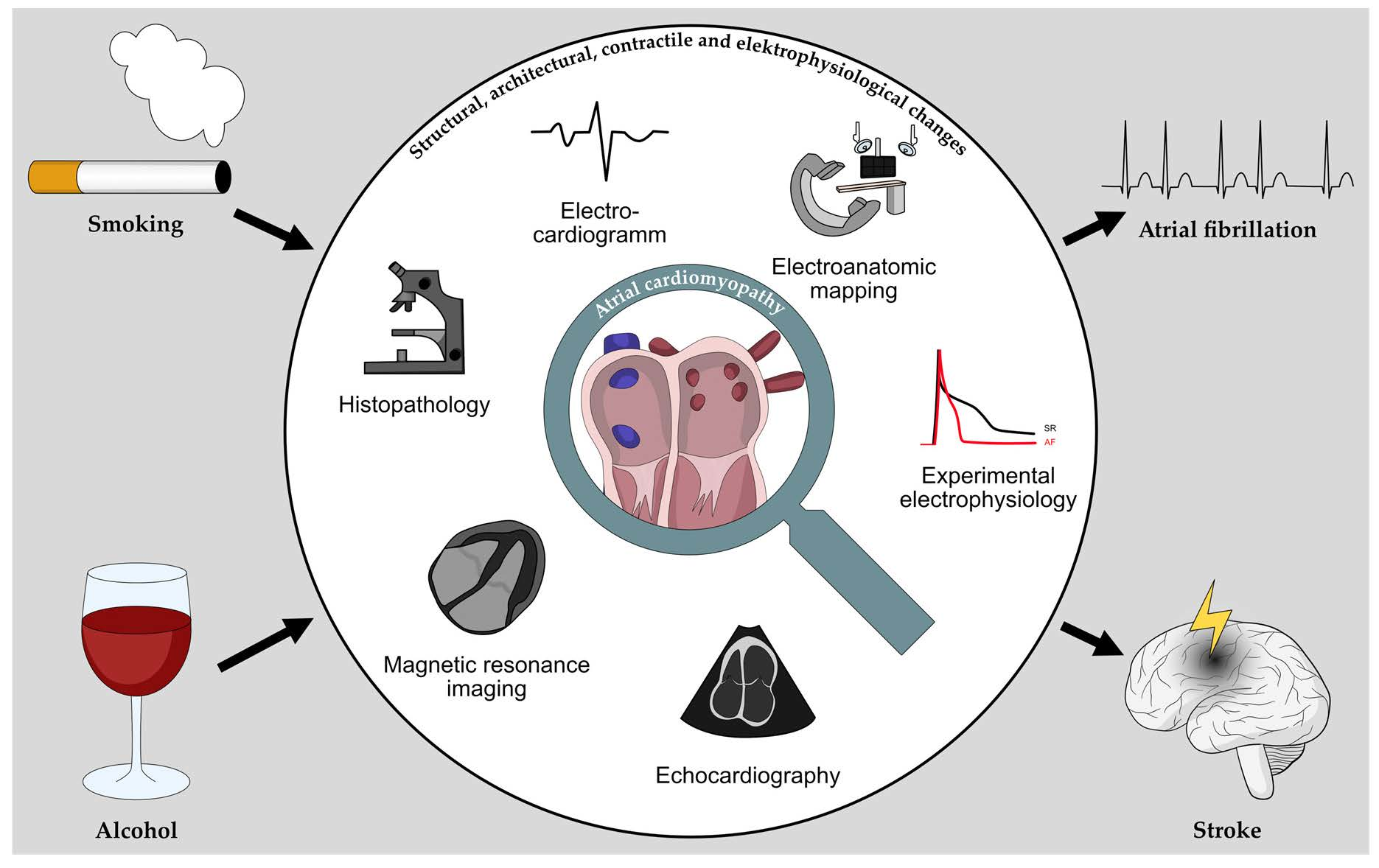
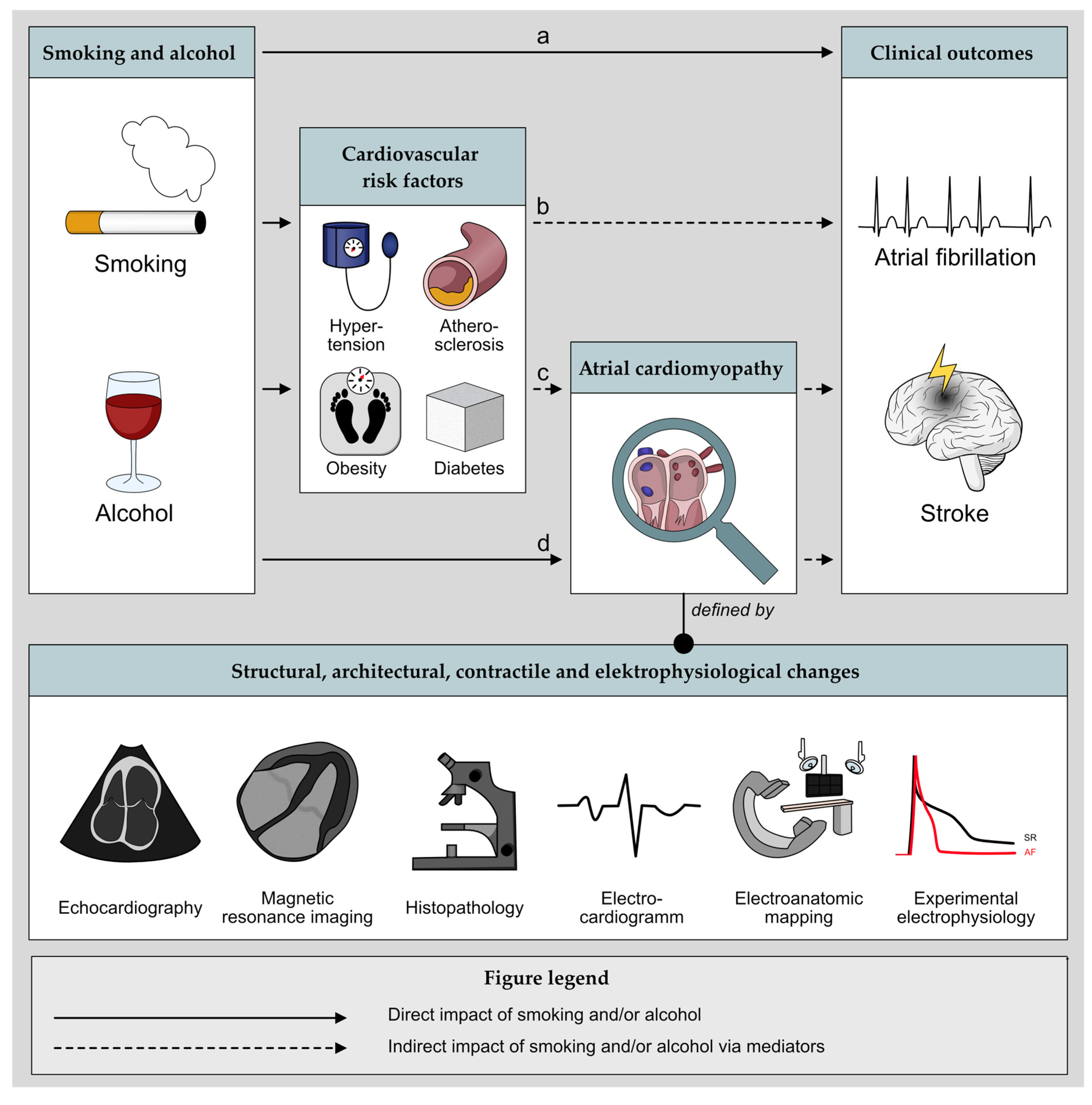
3. Atrial Myocardium and Tobacco Smoking
3.1. Structural, Architectural, and Contractile Changes
3.1.1. Echocardiography
Atrial Size
Atrial Strain
3.1.2. MRI and CT
Atrial Size
Atrial Fibrosis and Scarring
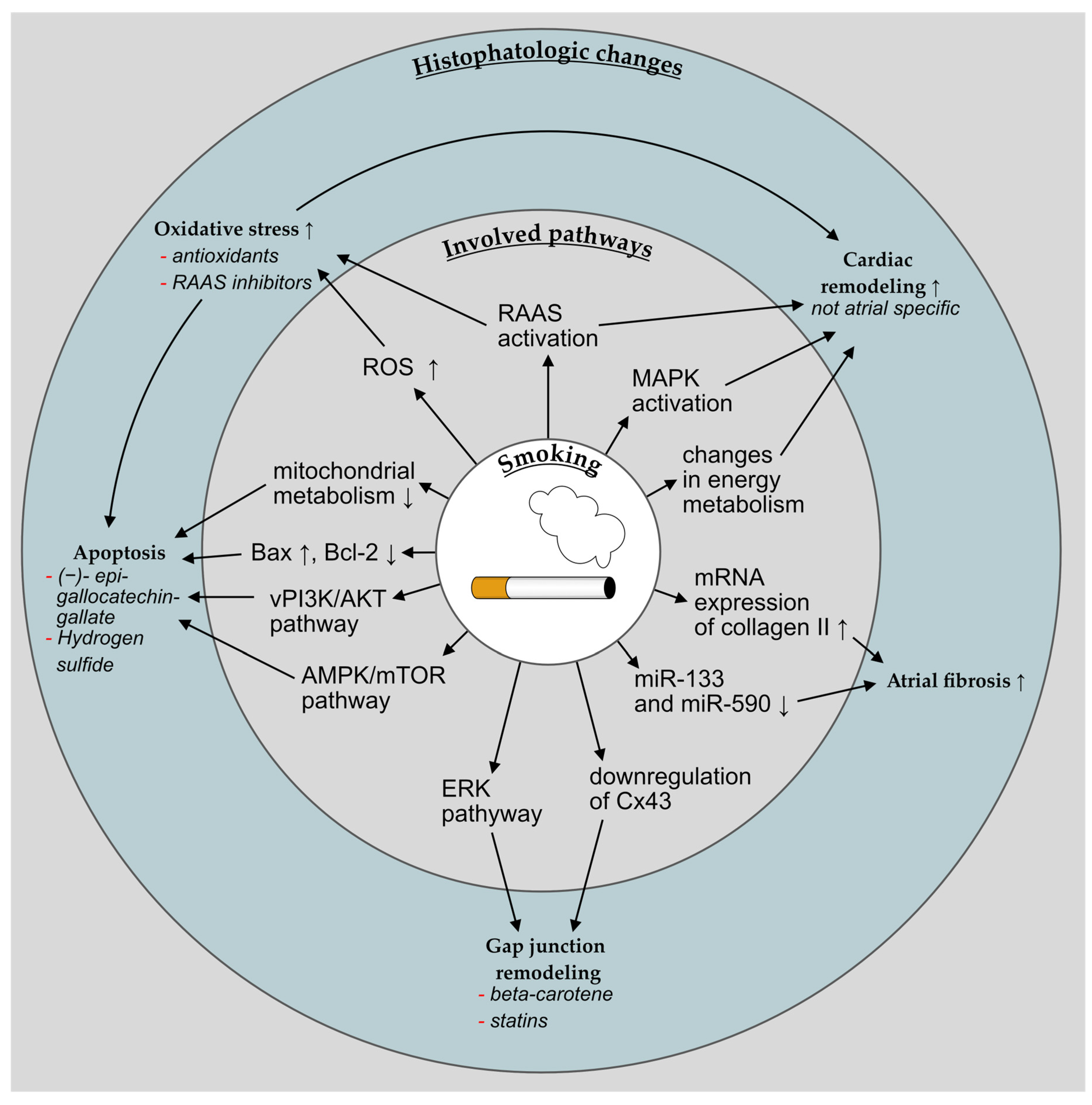
3.1.3. Histopathology
Fibrosis
3.2. Electrophysiological Changes
3.2.1. ECG
Autonomous Nervous System
P-Wave Alterations
3.2.2. Electroanatomic Mapping
3.2.3. Experimental Electrophysiology
3.3. Clinical Outcomes
3.3.1. Atrial Fibrillation
Smoking Cessation
Non-Cigarette Nicotine Consumption
3.3.2. Stroke and Thromboembolism
Risk of Stroke and Thromboembolism in AF
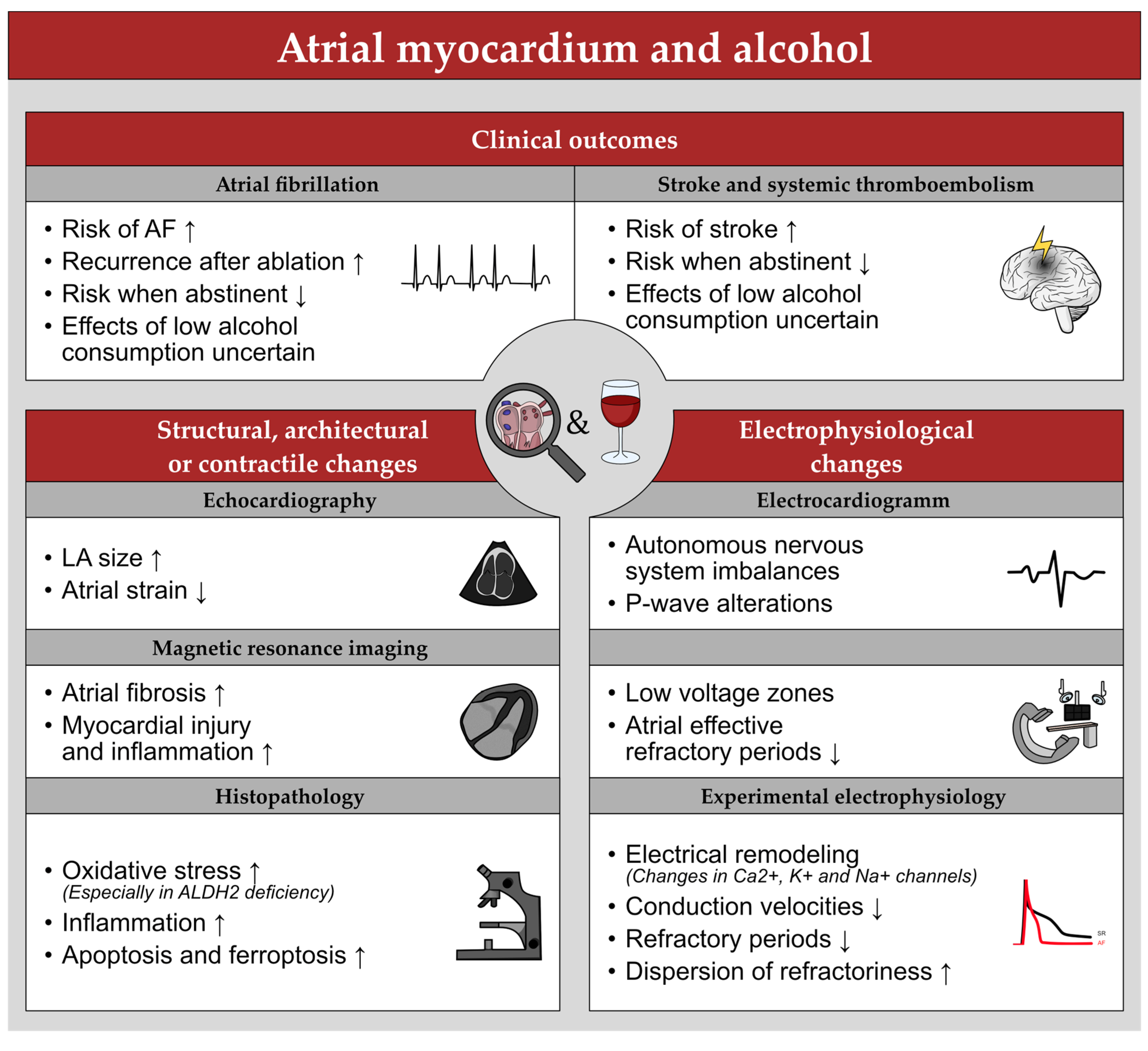
4. Atrial Myocardium and Alcohol
4.1. Structural, Architectural, and Contractile Changes
4.1.1. Echocardiography
Atrial Size
Atrial Strain
4.1.2. MRI
Atrial Size
Myocardial Injury
4.1.3. Histopathology
Oxidative Stress, Inflammation, and Apoptosis
ALDH2 Deficiency
Biomarkers
4.2. Electrophysiological Changes
4.2.1. ECG
Autonomous Nervous System
P-Wave Alterations
4.2.2. Electroanatomic Mapping
4.2.3. Experimental Electrophysiology
4.3. Clinical Outcomes
4.3.1. Atrial Fibrillation
Mild to Moderate Alcohol Consumption
Alcohol Abstinence
AF Recurrence after Ablation
ALDH2 Deficiency
4.3.2. Stroke and Thromboembolism
Mild to Moderate Alcohol Consumption
Alcohol Abstinence
ALDH2 Deficiency
5. Limitations
6. Summary and Perspectives
Funding
Conflicts of Interest
Abbreviations
References
- Goette, A.; Kalman, J.M.; Aguinaga, L.; Akar, J.; Cabrera, J.A.; Chen, S.A.; Chugh, S.S.; Corradi, D.; D’Avila, A.; Dobrev, D.; et al. EHRA/HRS/APHRS/SOLAECE Expert Consensus on Atrial Cardiomyopathies: Definition, Characterization, and Clinical Implication. EP Eur. 2016, 18, 1455–1490. [Google Scholar] [CrossRef] [PubMed]
- Vergara, G.R.; Marrouche, N.F. Tailored Management of Atrial Fibrillation Using a LGE-MRI Based Model: From the Clinic to the Electrophysiology Laboratory. J. Cardiovasc. Electrophysiol. 2011, 22, 481–487. [Google Scholar] [CrossRef] [PubMed]
- Hijazi, Z.; Oldgren, J.; Siegbahn, A.; Granger, C.B.; Wallentin, L. Biomarkers in Atrial Fibrillation: A Clinical Review. Eur. Heart J. 2013, 34, 1475–1480. [Google Scholar] [CrossRef] [PubMed]
- Vílchez, J.A.; Roldán, V.; Hernández-Romero, D.; Valdés, M.; Lip, G.Y.H.; Marín, F. Biomarkers in Atrial Fibrillation: An Overview. Int. J. Clin. Pract. 2014, 68, 434–443. [Google Scholar] [CrossRef]
- Chang, K.-W.; Hsu, J.C.; Toomu, A.; Fox, S.; Maisel, A.S. Clinical Applications of Biomarkers in Atrial Fibrillation. Am. J. Med. 2017, 130, 1351–1357. [Google Scholar] [CrossRef]
- Global Status Report on Alcohol and Health 2018; World Health Organization: Geneva, Switzerland, 2018.
- WHO Global Report on Trends in Prevalence of Tobacco Smoking 2000–2025, 2nd ed.; World Health Organization: Geneva, Switzerland, 2018.
- Abed, H.S.; Wittert, G.A.; Leong, D.P.; Shirazi, M.G.; Bahrami, B.; Middeldorp, M.E.; Lorimer, M.F.; Lau, D.H.; Antic, N.A.; Brooks, A.G.; et al. Effect of Weight Reduction and Cardiometabolic Risk Factor Management on Symptom Burden and Severity in Patients With Atrial Fibrillation: A Randomized Clinical Trial. JAMA 2013, 310, 2050–2060. [Google Scholar] [CrossRef]
- Pathak, R.K.; Middeldorp, M.E.; Lau Dennis, H.; Mehta, A.B.; Mahajan, R.; Twomey, D.; Alasady, M.; Hanley, L.; Antic, N.A.; McEvoy, R.D.; et al. Aggressive Risk Factor Reduction Study for Atrial Fibrillation and Implications for the Outcome of Ablation. J. Am. Coll. Cardiol. 2014, 64, 2222–2231. [Google Scholar] [CrossRef]
- Pathak, R.K.; Evans, M.; Middeldorp, M.E.; Mahajan, R.; Mehta, A.B.; Meredith, M.; Twomey, D.; Wong, C.X.; Hendriks, J.M.L.; Abhayaratna, W.P.; et al. Cost-Effectiveness and Clinical Effectiveness of the Risk Factor Management Clinic in Atrial Fibrillation. JACC Clin. Electrophysiol. 2017, 3, 436–447. [Google Scholar] [CrossRef]
- Gessler, N.; Willems, S.; Steven, D.; Aberle, J.; Akbulak, R.O.; Gosau, N.; Hoffmann, B.A.; Meyer, C.; Sultan, A.; Tilz, R.; et al. Supervised Obesity Reduction Trial for AF Ablation Patients: Results from the SORT-AF Trial. EP Eur. 2021, 23, 1548–1558. [Google Scholar] [CrossRef]
- Rodgman, A.; Perfetti, T.A. The Chemical Components of Tobacco and Tobacco Smoke, 2nd ed.; CRC Press: Boca Raton, FL, USA, 2013. [Google Scholar]
- Vartiainen, E.; Seppälä, T.; Lillsunde, P.; Puska, P. Validation of Self Reported Smoking by Serum Cotinine Measurement in a Community-Based Study. J. Epidemiol. Community Health 2002, 56, 167. [Google Scholar] [CrossRef]
- Benjamin, E.J.; D’Agostino, R.B.; Belanger, A.J.; Wolf, P.A.; Levy, D. Left Atrial Size and the Risk of Stroke and Death. Circulation 1995, 92, 835–841. [Google Scholar] [CrossRef]
- Kizer, J.R.; Bella, J.N.; Palmieri, V.; Liu, J.E.; Best, L.G.; Lee, E.T.; Roman, M.J.; Devereux, R.B. Left Atrial Diameter as an Independent Predictor of First Clinical Cardiovascular Events in Middle-Aged and Elderly Adults: The Strong Heart Study (SHS). Am. Heart J. 2006, 151, 412–418. [Google Scholar] [CrossRef]
- Nagarajarao, H.S.; Penman, A.D.; Taylor, H.A.; Mosley, T.H.; Butler, K.; Skelton, T.N.; Samdarshi, T.E.; Aru, G.; Fox, E.R. The Predictive Value of Left Atrial Size for Incident Ischemic Stroke and All-Cause Mortality in African Americans. Stroke 2008, 39, 2701–2706. [Google Scholar] [CrossRef]
- Cuspidi, C.; Meani, S.; Valerio, C.; Fusi, V.; Catini, E.; Sala, C.; Zanchetti, A. Ambulatory Blood Pressure, Target Organ Damage and Left Atrial Size in Never-Treated Essential Hypertensive Individuals. J. Hypertens. 2005, 23, 1589–1595. [Google Scholar] [CrossRef]
- Armstrong, A.C.; Gidding, S.S.; Colangelo, L.A.; Kishi, S.; Liu, K.; Sidney, S.; Konety, S.; Lewis, C.E.; Correia, L.C.L.; Lima, J.A.C. Association of Early Adult Modifiable Cardiovascular Risk Factors with Left Atrial Size over a 20-Year Follow-up Period: The CARDIA Study. BMJ Open 2014, 4, e004001. [Google Scholar] [CrossRef]
- Can Bostan, O.; Ozben, B.; Bayram, T.; Sayar, N.; Eryuksel, E. The Effect of Smoking on Atrial and Ventricular Functions in Healthy Subjects: A Speckle Tracking Echocardiography Study. J. Clin. Ultrasound 2020, 48, 462–469. [Google Scholar] [CrossRef]
- Modin, D.; Biering-Sørensen, S.R.; Møgelvang, R.; Alhakak, A.S.; Jensen, J.S.; Biering-Sørensen, T. Prognostic Value of Left Atrial Strain in Predicting Cardiovascular Morbidity and Mortality in the General Population. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 804–815. [Google Scholar] [CrossRef]
- Alhakak, A.S.; Biering-Sørensen, S.R.; Møgelvang, R.; Modin, D.; Jensen, G.B.; Schnohr, P.; Iversen, A.Z.; Svendsen, J.H.; Jespersen, T.; Gislason, G.; et al. Usefulness of Left Atrial Strain for Predicting Incident Atrial Fibrillation and Ischaemic Stroke in the General Population. Eur. Heart J. Cardiovasc. Imaging 2022, 23, 363–371. [Google Scholar] [CrossRef]
- Fredgart, M.H.; Lindholt, J.S.; Brandes, A.; Steffensen, F.H.; Frost, L.; Lambrechtsen, J.; Karon, M.; Busk, M.; Urbonaviciene, G.; Egstrup, K.; et al. Association of Left Atrial Size Measured by Non-Contrast Computed Tomography with Cardiovascular Risk Factors—The Danish Cardiovascular Screening Trial (DANCAVAS). Diagnostics 2022, 12, 244. [Google Scholar] [CrossRef]
- Mahabadi, A.A.; Lehmann, N.; Sonneck, N.C.; Kälsch, H.; Bauer, M.; Kara, K.; Geisel, M.H.; Moebus, S.; Jöckel, K.-H.; Erbel, R.; et al. Left Atrial Size Quantification Using Non-Contrast-Enhanced Cardiac Computed Tomography–Association with Cardiovascular Risk Factors and Gender-Specific Distribution in the General Population: The Heinz Nixdorf Recall Study. Acta Radiol. 2014, 55, 917–925. [Google Scholar] [CrossRef]
- Zemrak, F.; Ambale-Venkatesh, B.; Captur, G.; Chrispin, J.; Chamera, E.; Habibi, M.; Nazarian, S.; Mohiddin, S.A.; Moon, J.C.; Petersen, S.E.; et al. Left Atrial Structure in Relationship to Age, Sex, Ethnicity, and Cardiovascular Risk Factors. Circ. Cardiovasc. Imaging 2017, 10, e005379. [Google Scholar] [CrossRef] [PubMed]
- Imai, M.; Ambale Venkatesh, B.; Samiei, S.; Donekal, S.; Habibi, M.; Armstrong, A.C.; Heckbert, S.R.; Wu, C.O.; Bluemke, D.A.; Lima, J.A.C. Multi-Ethnic Study of Atherosclerosis: Association between Left Atrial Function Using Tissue Tracking from Cine MR Imaging and Myocardial Fibrosis. Radiology 2014, 273, 703–713. [Google Scholar] [CrossRef] [PubMed]
- Detorakis, E.; Illing, R.; Lasithiotaki, I.; Foukarakis, E.; Raissaki, M. Role of Smoking in the Evolution of Cardiovascular Magnetic Resonance and Laboratory Findings of Acute Myocarditis. Heart Views 2020, 21, 22. [Google Scholar] [CrossRef]
- Chelu, M.G.; King, J.B.; Kholmovski, E.G.; Ma, J.; Gal, P.; Marashly, Q.; AlJuaid, M.A.; Kaur, G.; Silver, M.A.; Johnson, K.A.; et al. Atrial Fibrosis by Late Gadolinium Enhancement Magnetic Resonance Imaging and Catheter Ablation of Atrial Fibrillation: 5-Year Follow-Up Data. J. Am. Heart Assoc. 2018, 7, e006313. [Google Scholar] [CrossRef] [PubMed]
- Oakes, R.S.; Badger, T.J.; Kholmovski, E.G.; Akoum, N.; Burgon, N.S.; Fish, E.N.; Blauer, J.J.E.; Rao, S.N.; DiBella, E.V.R.; Segerson, N.M.; et al. Detection and Quantification of Left Atrial Structural Remodeling With Delayed-Enhancement Magnetic Resonance Imaging in Patients With Atrial Fibrillation. Circulation 2009, 119, 1758–1767. [Google Scholar] [CrossRef] [PubMed]
- Grunseich, K.; Mekonnen, B.; Simprini, L.A.; Mojibian, H.; Marieb, M.; Atteya, G.; Cornfeld, D.; Peters, D.C. Left Atrial Volume, Congestive Heart Failure, and Obesity Are Associated with Extent of Left Atrial Fibrosis by Late Gadolinium Enhancement. J. Cardiovasc. Magn. Reson. 2015, 17, P368. [Google Scholar] [CrossRef]
- Cucina, A.; Corvino, V.; Sapienza, P.; Borrelli, V.; Lucarelli, M.; Scarpa, S.; Strom, R.; Santoro-D’Angelo, L.; Cavallaro, A. Nicotine Regulates Basic Fibroblastic Growth Factor and Transforming Growth Factor Β1Production in Endothelial Cells. Biochem. Biophys. Res. Commun. 1999, 257, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Roman, J.; Ritzenthaler, J.D.; Gil-Acosta, A.; Rivera, H.N.; Roser-Page, S. Nicotine and Fibronectin Expression in Lung Fibroblasts: Implications for Tobacco-Related Lung Tissue Remodeling. FASEB J. 2004, 18, 1436–1438. [Google Scholar] [CrossRef]
- Morse, D.; Rosas, I.O. Tobacco Smoke–Induced Lung Fibrosis and Emphysema. Annu. Rev. Physiol. 2014, 76, 493–513. [Google Scholar] [CrossRef]
- Goette, A.; Lendeckel, U.; Kuchenbecker, A.; Bukowska, A.; Peters, B.; Klein, H.U.; Huth, C.; Rocken, C. Cigarette Smoking Induces Atrial Fibrosis in Humans via Nicotine. Heart 2007, 93, 1056–1063. [Google Scholar] [CrossRef]
- Shan, H.; Zhang, Y.; Lu, Y.; Zhang, Y.; Pan, Z.; Cai, B.; Wang, N.; Li, X.; Feng, T.; Hong, Y.; et al. Downregulation of MiR-133 and MiR-590 Contributes to Nicotine-Induced Atrial Remodelling in Canines. Cardiovasc. Res. 2009, 83, 465–472. [Google Scholar] [CrossRef]
- Burke, A.; FitzGerald, G.A. Oxidative Stress and Smoking-Induced Vascular Injury. Prog. Cardiovasc. Dis. 2003, 46, 79–90. [Google Scholar] [CrossRef]
- Carnevali, S.; Petruzzelli, S.; Longoni, B.; Vanacore, R.; Barale, R.; Cipollini, M.; Scatena, F.; Paggiaro, P.; Celi, A.; Giuntini, C. Cigarette Smoke Extract Induces Oxidative Stress and Apoptosis in Human Lung Fibroblasts. Am. J. Physiol. Lung Cell. Mol. Physiol. 2003, 284, L955–L963. [Google Scholar] [CrossRef]
- Khanna, A.; Guo, M.; Mehra, M.; Royal, W. Inflammation and Oxidative Stress Induced by Cigarette Smoke in Lewis Rat Brains. J. Neuroimmunol. 2013, 254, 69–75. [Google Scholar] [CrossRef]
- Goldkorn, T.; Filosto, S.; Chung, S. Lung Injury and Lung Cancer Caused by Cigarette Smoke-Induced Oxidative Stress: Molecular Mechanisms and Therapeutic Opportunities Involving the Ceramide-Generating Machinery and Epidermal Growth Factor Receptor. Antioxid. Redox Signal. 2014, 21, 2149–2174. [Google Scholar] [CrossRef]
- Reilly, M.; Delanty, N.; Lawson, J.A.; FitzGerald, G.A. Modulation of Oxidant Stress In Vivo in Chronic Cigarette Smokers. Circulation 1996, 94, 19–25. [Google Scholar] [CrossRef]
- Visioli, F.; Galli, C.; Plasmati, E.; Viappiani, S.; Hernandez, A.; Colombo, C.; Sala, A. Olive Phenol Hydroxytyrosol Prevents Passive Smoking–Induced Oxidative Stress. Circulation 2000, 102, 2169–2171. [Google Scholar] [CrossRef]
- Demiralay, R.; Gürsan, N.; Erdem, H. The Effects of Erdosteine, N-Acetylcysteine and Vitamin E on Nicotine-Induced Apoptosis of Cardiac Cells. J. Appl. Toxicol. 2007, 27, 247–254. [Google Scholar] [CrossRef]
- Hanna, N.; Cardin, S.; Leung, T.-K.; Nattel, S. Differences in Atrial versus Ventricular Remodeling in Dogs with Ventricular Tachypacing-Induced Congestive Heart Failure. Cardiovasc. Res. 2004, 63, 236–244. [Google Scholar] [CrossRef]
- Burstein, B.; Libby, E.; Calderone, A.; Nattel, S. Differential Behaviors of Atrial Versus Ventricular Fibroblasts. Circulation 2008, 117, 1630–1641. [Google Scholar] [CrossRef]
- Healey, J.S.; Morillo, C.A.; Connolly, S.J. Role of the Renin-Angiotensin-Aldosterone System in Atrial Fibrillation and Cardiac Remodeling. Curr. Opin. Cardiol. 2005, 20, 31–37. [Google Scholar] [PubMed]
- Wolke, C.; Bukowska, A.; Goette, A.; Lendeckel, U. Redox Control of Cardiac Remodeling in Atrial Fibrillation. Redox Regul. Differ.-Differ. 2015, 1850, 1555–1565. [Google Scholar] [CrossRef] [PubMed]
- Minicucci, M.; Oliveira, F.; Santos, P.; Polegato, B.; Roscani, M.; Fernandes, A.A.; Lustosa, B.; Paiva, S.; Zornoff, L.; Azevedo, P. Pentoxifylline Attenuates Cardiac Remodeling Induced by Tobacco Smoke Exposure. Arq. Bras. Cardiol. 2016, 106, 396–403. [Google Scholar] [CrossRef] [PubMed]
- Zornoff, L.A.M.; Matsubara, L.S.; Matsubara, B.B.; Okoshi, M.P.; Okoshi, K.; Dal Pai-Silva, M.; Carvalho, R.F.; Cicogna, A.C.; Padovani, C.R.; Novelli, E.L.; et al. Beta-Carotene Supplementation Attenuates Cardiac Remodeling Induced by One-Month Tobacco-Smoke Exposure in Rats. Toxicol. Sci. 2006, 90, 259–266. [Google Scholar] [CrossRef]
- Ramalingam, A.; Mohd Fauzi, N.; Budin, S.B.; Zainalabidin, S. Impact of Prolonged Nicotine Administration on Myocardial Function and Susceptibility to Ischaemia-Reperfusion Injury in Rats. Basic Clin. Pharmacol. Toxicol. 2021, 128, 322–333. [Google Scholar] [CrossRef]
- Ramalingam, A.; Budin, S.B.; Mohd Fauzi, N.; Ritchie, R.H.; Zainalabidin, S. Angiotensin II Type I Receptor Antagonism Attenuates Nicotine-Induced Cardiac Remodeling, Dysfunction, and Aggravation of Myocardial Ischemia-Reperfusion Injury in Rats. Front. Pharmacol. 2019, 10, 1493. [Google Scholar] [CrossRef]
- Ramalingam, A.; Budin, S.B.; Mohd Fauzi, N.; Ritchie, R.H.; Zainalabidin, S. Targeting Mitochondrial Reactive Oxygen Species-Mediated Oxidative Stress Attenuates Nicotine-Induced Cardiac Remodeling and Dysfunction. Sci. Rep. 2021, 11, 13845. [Google Scholar] [CrossRef]
- Talukder, M.A.H.; Johnson, W.M.; Varadharaj, S.; Lian, J.; Kearns, P.N.; El-Mahdy, M.A.; Liu, X.; Zweier, J.L. Chronic Cigarette Smoking Causes Hypertension, Increased Oxidative Stress, Impaired NO Bioavailability, Endothelial Dysfunction, and Cardiac Remodeling in Mice. Am. J. Physiol. Heart Circ. Physiol. 2011, 300, H388–H396. [Google Scholar] [CrossRef]
- Dikalov, S.; Itani, H.; Richmond, B.; Arslanbaeva, L.; Vergeade, A.; Rahman, S.M.J.; Boutaud, O.; Blackwell, T.; Massion, P.P.; Harrison, D.G.; et al. Tobacco Smoking Induces Cardiovascular Mitochondrial Oxidative Stress, Promotes Endothelial Dysfunction, and Enhances Hypertension. Am. J. Physiol. Heart Circ. Physiol. 2019, 316, H639–H646. [Google Scholar] [CrossRef]
- Hu, N.; Han, X.; Lane, E.K.; Gao, F.; Zhang, Y.; Ren, J. Cardiac-Specific Overexpression of Metallothionein Rescues against Cigarette Smoking Exposure-Induced Myocardial Contractile and Mitochondrial Damage. PLoS ONE 2013, 8, e57151. [Google Scholar] [CrossRef]
- Duarte, D.R.; Minicucci, M.F.; Azevedo, P.S.; Matsubara, B.B.; Matsubara, L.S.; Novelli, E.L.; Paiva, S.A.R.; Zornoff, L.A.M. The Role of Oxidative Stress and Lipid Peroxidation in Ventricular Remodeling Induced by Tobacco Smoke Exposure after Myocardial Infarction. Clinics 2009, 64, 691–697. [Google Scholar] [CrossRef]
- Rafacho, B.P.M.; Azevedo, P.S.; Polegato, B.F.; Fernandes, A.A.H.; Bertoline, M.A.; Fernandes, D.C.; Chiuso-Minicucci, F.; Roscani, M.G.; dos Santos, P.P.; Matsubara, L.S.; et al. Tobacco Smoke Induces Ventricular Remodeling Associated with an Increase in NADPH Oxidase Activity. Cell. Physiol. Biochem. 2011, 27, 305–312. [Google Scholar] [CrossRef]
- Duarte, D.R.; Minicucci, M.F.; Azevedo, P.S.; Chiuso-Minicucci, F.; Matsubara, B.B.; Matsubara, L.S.; Campana, A.O.; Paiva, S.A.R.; Zornoff, L.A.M. Influence of Lisinopril on Cardiac Remodeling Induced by Tobacco Smoke Exposure. Med. Sci. Monit. 2010, 16, BR255-9. [Google Scholar]
- Pereira, E.J.; Minicucci, M.; Polegato, B.; Portugal, P.; Batista, D.; Modesto, P.; Fernandes, A.A.; Rafacho, B.; Matsubara, L.; Zornoff, L.; et al. The Role of Green Tea and Oxidative Stress in Heart Remodeling Induced by Tobacco Smoke Exposure. FASEB J. 2012, 26, 1133.8. [Google Scholar] [CrossRef]
- Azevedo, P.S.; Polegato, B.; Portugal, P.; Batista, D.; Lustosa, B.; Rafacho, B.; Oliveira, F.; Mascoli, A.; Roscani, M.; Fernandes, A.A.; et al. Pentoxifylline Reduces Myocardial Oxidative Stress Induced by Exposure to Tobacco Smoke. FASEB J. 2012, 26, 1133.3. [Google Scholar] [CrossRef]
- Das, A.; Dey, N.; Ghosh, A.; Das, S.; Chattopadhyay, D.J.; Chatterjee, I.B. Molecular and Cellular Mechanisms of Cigarette Smoke-Induced Myocardial Injury: Prevention by Vitamin C. PLoS ONE 2012, 7, e44151. [Google Scholar] [CrossRef]
- Fried, N.D.; Morris, T.M.; Whitehead, A.; Lazartigues, E.; Yue, X.; Gardner, J.D. Angiotensin II Type 1 Receptor Mediates Pulmonary Hypertension and Right Ventricular Remodeling Induced by Inhaled Nicotine. Am. J. Physiol. Heart Circ. Physiol. 2021, 320, H1526–H1534. [Google Scholar] [CrossRef]
- Azevedo, P.S.; Pires, V.; Santos, P.; Gonçalves, A.; Okoshi, M.; Fernandes, A.A.; Roscani, M.; Polegato, B.; Paiva, S.; Zornoff, L.; et al. The Role of Insulin Resistance and SIRT-1 in Cardiac Remodeling Induced by Cigarette Smoke. FASEB J. 2016, 30, lb388. [Google Scholar] [CrossRef]
- Santos, P.P.; Oliveira, F.; Ferreira, V.C.M.P.; Polegato, B.F.; Roscani, M.G.; Fernandes, A.A.; Modesto, P.; Rafacho, B.P.M.; Zanati, S.G.; Di Lorenzo, A.; et al. The Role of Lipotoxicity in Smoke Cardiomyopathy. PLoS ONE 2014, 9, e113739. [Google Scholar] [CrossRef]
- Adikesavan, G.; Vinayagam, M.M.; Abdulrahman, L.A.; Chinnasamy, T. (−)-Epigallocatechin-Gallate (EGCG) Stabilize the Mitochondrial Enzymes and Inhibits the Apoptosis in Cigarette Smoke-Induced Myocardial Dysfunction in Rats. Mol. Biol. Rep. 2013, 40, 6533–6545. [Google Scholar] [CrossRef]
- Zhou, X.; An, G.; Chen, J. Hydrogen Sulfide Improves Left Ventricular Function in Smoking Rats via Regulation of Apoptosis and Autophagy. Apoptosis 2014, 19, 998–1005. [Google Scholar] [CrossRef]
- Zhou, X.; Zhao, L.; Mao, J.; Huang, J.; Chen, J. Antioxidant Effects of Hydrogen Sulfide on Left Ventricular Remodeling in Smoking Rats Are Mediated via PI3K/Akt-Dependent Activation of Nrf2. Toxicol. Sci. 2015, 144, 197–203. [Google Scholar] [CrossRef]
- Gu, L.; Pandey, V.; Geenen, D.L.; Chowdhury, S.A.K.; Piano, M.R. Cigarette Smoke-Induced Left Ventricular Remodelling is Associated with Activation of Mitogen-Activated Protein Kinases. Eur. J. Heart Fail. 2008, 10, 1057–1064. [Google Scholar] [CrossRef]
- Sumanasekera, W.K.; Tran, D.M.; Sumanasekera, T.U.; Le, N.; Dao, H.T.; Rokosh, G.D. Cigarette Smoke Adversely Affects Functions and Cell Membrane Integrity in C-Kit+ Cardiac Stem Cells. Cell Biol. Toxicol. 2014, 30, 113–125. [Google Scholar] [CrossRef]
- Tsai, C.-H.; Yeh, H.-I.; Tian, T.-Y.; Lee, Y.-N.; Lu, C.-S.; Ko, Y.-S. Down-Regulating Effect of Nicotine on Connexin43 Gap Junctions in Human Umbilical Vein Endothelial Cells Is Attenuated by Statins. Eur. J. Cell Biol. 2004, 82, 589–595. [Google Scholar] [CrossRef]
- Haussig, S.; Schubert, A.; Mohr, F.-W.; Dhein, S. Sub-Chronic Nicotine Exposure Induces Intercellular Communication Failure and Differential down-Regulation of Connexins in Cultured Human Endothelial Cells. Atherosclerosis 2008, 196, 210–218. [Google Scholar] [CrossRef]
- Novo, R.; Freire, C.M.; Felisbino, S.; Minicucci, M.F.; Azevedo, P.S.; Zornoff, L.A.M.; Paiva, S.A.R. Smoking is Associated with Remodeling of Gap Junction in the Rat Heart: Smoker’s Paradox Explanation? Arq. Bras. Cardiol. 2013, 100, 274–280. [Google Scholar] [CrossRef]
- Novo, R.; Azevedo, P.S.; Minicucci, M.F.; Zornoff, L.A.M.; Paiva, S.A.R. Effect of Beta-Carotene on Oxidative Stress and Expression of Cardiac Connexin 43. Arq. Bras. Cardiol. 2013, 101, 233–239. [Google Scholar] [CrossRef]
- Gepner, A.D.; Piper, M.E.; Leal, M.A.; Asthana, A.; Fiore, M.C.; Baker, T.B.; Stein, J.H. Electrocardiographic Changes Associated with Smoking and Smoking Cessation: Outcomes from a Randomized Controlled Trial. PLoS ONE 2013, 8, e62311. [Google Scholar] [CrossRef]
- Tseng, K.-K.; Li, J.; Tang, Y.-J.; Yang, C.W.; Lin, F.-Y. Healthcare Knowledge of Relationship between Time Series Electrocardiogram and Cigarette Smoking Using Clinical Records. BMC Med. Inform. Decis. Mak. 2020, 20, 127. [Google Scholar] [CrossRef]
- Huo, Y.; Mitrofanova, L.; Holmberg, P.; Orshanskaya, V.; Holmqvist, F.; Platonov, P. P-Wave Characteristics and Histological Atrial Abnormality. Eur. Heart J. 2013, 34, P4987. [Google Scholar] [CrossRef]
- Magnani, J.W.; Zhu, L.; Lopez, F.; Pencina, M.J.; Agarwal, S.K.; Soliman, E.Z.; Benjamin, E.J.; Alonso, A. P-Wave Indices and Atrial Fibrillation: Cross-Cohort Assessments from the Framingham Heart Study (FHS) and Atherosclerosis Risk in Communities (ARIC) Study. Am. Heart J. 2015, 169, 53–61.e1. [Google Scholar] [CrossRef] [PubMed]
- Junell, A.; Thomas, J.; Hawkins, L.; Sklenar, J.; Feldman, T.; Henrikson, C.A.; Tereshchenko, L.G. Screening Entire Healthcare System ECG Database: Association of Deep Terminal Negativity of P Wave in Lead V1 and ECG Referral with Mortality. Int. J. Cardiol. 2017, 228, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.A.; Junejo, R.T.; Thomas, G.N.; Fisher, J.P.; Lip, G.Y.H. Heart Rate Variability in Patients with Atrial Fibrillation and Hypertension. Eur. J. Clin. Investig. 2021, 51, e13361. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, G.; Jensen, S.H.; Poulsen, E.S.; Puthusserypady, S. Atrial Fibrillation Detection Using Heart Rate Variability and Atrial Activity: A Hybrid Approach. Expert Syst. Appl. 2021, 169, 114452. [Google Scholar] [CrossRef]
- Felber Dietrich, D.; Schwartz, J.; Schindler, C.; Gaspoz, J.-M.; Barthélémy, J.-C.; Tschopp, J.-M.; Roche, F.; von Eckardstein, A.; Brändli, O.; Leuenberger, P.; et al. Effects of Passive Smoking on Heart Rate Variability, Heart Rate and Blood Pressure: An Observational Study. Int. J. Epidemiol. 2007, 36, 834–840. [Google Scholar] [CrossRef]
- Girard, D.; Delgado-Eckert, E.; Schaffner, E.; Häcki, C.; Adam, M.; Stern, G.L.; Kumar, N.; Felber Dietrich, D.; Turk, A.; Pons, M.; et al. Long-Term Smoking Cessation and Heart Rate Dynamics in an Aging Healthy Cohort: Is It Possible to Fully Recover? Environ. Res. 2015, 143, 39–48. [Google Scholar] [CrossRef]
- Barutcu, I.; Esen, A.M.; Kaya, D.; Turkmen, M.; Karakaya, O.; Melek, M.; Esen, O.B.; Basaran, Y. Cigarette Smoking and Heart Rate Variability: Dynamic Influence of Parasympathetic and Sympathetic Maneuvers. Ann. Noninvasive Electrocardiol. 2005, 10, 324–329. [Google Scholar] [CrossRef]
- Yuksel, R.; Yuksel, R.; Sengezer, T.; Dane, S. Autonomic Cardiac Activity in Patients with Smoking and Alcohol Addiction by Heart Rate Variability Analysis. Clin. Investig. Med. 2016, 39, 147. [Google Scholar] [CrossRef]
- Ohta, Y.; Kawano, Y.; Hayashi, S.; Iwashima, Y.; Yoshihara, F.; Nakamura, S. Effects of Cigarette Smoking on Ambulatory Blood Pressure, Heart Rate, and Heart Rate Variability in Treated Hypertensive Patients. Clin. Exp. Hypertens. 2016, 38, 510–513. [Google Scholar] [CrossRef]
- Zhang, J.; Fang, S.C.; Mittleman, M.A.; Christiani, D.C.; Cavallari, J.M. Secondhand Tobacco Smoke Exposure and Heart Rate Variability and Inflammation among Non-Smoking Construction Workers: A Repeated Measures Study. Environ. Health 2013, 12, 83. [Google Scholar] [CrossRef]
- Chen, C.-Y.; Chow, D.; Chiamvimonvat, N.; Glatter, K.A.; Li, N.; He, Y.; Pinkerton, K.E.; Bonham, A.C. Short-Term Secondhand Smoke Exposure Decreases Heart Rate Variability and Increases Arrhythmia Susceptibility in Mice. Am. J. Physiol. Heart Circ. Physiol. 2008, 295, H632–H639. [Google Scholar] [CrossRef]
- Ramakrishnan, S.; Bhatt, K.; Dubey, A.K.; Roy, A.; Singh, S.; Naik, N.; Seth, S.; Bhargava, B. Acute Electrocardiographic Changes during Smoking: An Observational Study. BMJ Open 2013, 3, e002486. [Google Scholar] [CrossRef]
- Tereshchenko, L.G.; Shah, A.J.; Li, Y.; Soliman, E.Z. Electrocardiographic Deep Terminal Negativity of the P Wave in V1 and Risk of Mortality: The National Health and Nutrition Examination Survey III. J. Cardiovasc. Electrophysiol. 2014, 25, 1242–1248. [Google Scholar] [CrossRef]
- Irfan, A.; Li, Y.; Bhatnagar, A.; Soliman, E.Z. Association between Serum Cotinine Levels and Electrocardiographic Left Atrial Abnormality. Ann. Noninvasive Electrocardiol. 2019, 24, e12586. [Google Scholar] [CrossRef]
- Tuan, T.-C.; Chang, S.-L.; Tai, C.-T.; Lin, Y.-J.; Hu, Y.-F.; Lo, L.-W.; Wongcharoen, W.; Udyavar, A.R.; Chiang, S.-J.; Chen, Y.-J.; et al. Impairment of the Atrial Substrates by Chronic Cigarette Smoking in Patients with Atrial Fibrillation. J. Cardiovasc. Electrophysiol. 2008, 19, 259–265. [Google Scholar] [CrossRef]
- Kanazawa, H.; Yamabe, H.; Enomoto, K.; Koyama, J.; Morihisa, K.; Hoshiyama, T.; Matsui, K.; Ogawa, H. Importance of Pericardial Fat in the Formation of Complex Fractionated Atrial Electrogram Region in Atrial Fibrillation. Int. J. Cardiol. 2014, 174, 557–564. [Google Scholar] [CrossRef]
- Bébarová, M.; Matejovič, P.; Švecová, O.; Kula, R.; Šimurdová, M.; Šimurda, J. Nicotine at Clinically Relevant Concentrations Affects Atrial Inward Rectifier Potassium Current Sensitive to Acetylcholine. Naunyn. Schmiedebergs Arch. Pharmacol. 2017, 390, 471–481. [Google Scholar] [CrossRef]
- Wang, H.; Shi, H.; Wang, Z. Nicotine Depresses the Functions of Multiple Cardiac Potassium Channels. Life Sci. 1999, 65, PL143–PL149. [Google Scholar] [CrossRef]
- Wang, H.; Shi, H.; Zhang, L.; Pourrier, M.; Yang, B.; Nattel, S.; Wang, Z. Nicotine Is a Potent Blocker of the Cardiac A-Type K+ Channels. Circulation 2000, 102, 1165–1171. [Google Scholar] [CrossRef]
- Satoh, H. Modulation by Nicotine of the Ionic Currents in Guinea Pig Ventricular Cardiomyocytes: Relatively Higher Sensitivity to IKr and IK1. Vascul. Pharmacol. 2002, 39, 55–61. [Google Scholar] [CrossRef]
- Satoh, H. Effects of Nicotine on Spontaneous Activity and Underlying Ionic Currents in Rabbit Sinoatrial Nodal Cells. Gen. Pharmacol. Vasc. Syst. 1997, 28, 39–44. [Google Scholar] [CrossRef]
- Hayashi, H.; Omichi, C.; Miyauchi, Y.; Mandel, W.J.; Lin, S.-F.; Chen, P.-S.; Karagueuzian, H.S. Age-Related Sensitivity to Nicotine for Inducible Atrial Tachycardia and Atrial Fibrillation. Am. J. Physiol. Heart Circ. Physiol. 2003, 285, H2091–H2098. [Google Scholar] [CrossRef] [PubMed]
- Nakatani, T.; Nakashima, T.; Satoh, H. Negative Chronotropic and Inotropic Responses to Nicotine in Rat Right and Left Atria. Gen. Pharmacol. Vasc. Syst. 1994, 25, 865–873. [Google Scholar] [CrossRef]
- Abramochkin, D.V.; Haertdinov, N.N.; Porokhnya, M.V.; Zefirov, A.L.; Sitdikova, G.F. Carbon Monoxide Affects Electrical and Contractile Activity of Rat Myocardium. J. Biomed. Sci. 2011, 18, 40. [Google Scholar] [CrossRef]
- Heeringa, J.; Kors, J.A.; Hofman, A.; van Rooij, F.J.A.; Witteman, J.C.M. Cigarette Smoking and Risk of Atrial Fibrillation: The Rotterdam Study. Am. Heart J. 2008, 156, 1163–1169. [Google Scholar] [CrossRef]
- Rosengren, A.; Hauptman, P.J.; Lappas, G.; Olsson, L.; Wilhelmsen, L.; Swedberg, K. Big Men and Atrial Fibrillation: Effects of Body Size and Weight Gain on Risk of Atrial Fibrillation in Men. Eur. Heart J. 2009, 30, 1113–1120. [Google Scholar] [CrossRef]
- Smith, J.G.; Platonov, P.G.; Hedblad, B.; Engström, G.; Melander, O. Atrial Fibrillation in the Malmö Diet and Cancer Study: A Study of Occurrence, Risk Factors and Diagnostic Validity. Eur. J. Epidemiol. 2010, 25, 95–102. [Google Scholar] [CrossRef]
- Suzuki, S.; Otsuka, T.; Sagara, K.; Kano, H.; Matsuno, S.; Takai, H.; Kato, Y.; Uejima, T.; Oikawa, Y.; Nagashima, K.; et al. Association between Smoking Habits and the First-Time Appearance of Atrial Fibrillation in Japanese Patients: Evidence from the Shinken Database. J. Cardiol. 2015, 66, 73–79. [Google Scholar] [CrossRef]
- Chamberlain, A.M.; Agarwal, S.K.; Folsom, A.R.; Duval, S.; Soliman, E.Z.; Ambrose, M.; Eberly, L.E.; Alonso, A. Smoking and Incidence of Atrial Fibrillation: Results from the Atherosclerosis Risk in Communities (ARIC) Study. Heart Rhythm 2011, 8, 1160–1166. [Google Scholar] [CrossRef]
- Imtiaz Ahmad, M.; Mosley, C.D.; O’Neal, W.T.; Judd, S.E.; McClure, L.A.; Howard, V.J.; Howard, G.; Soliman, E.Z. Smoking and Risk of Atrial Fibrillation in the REasons for Geographic And Racial Differences in Stroke (REGARDS) Study. Risk Atr. Fibrillation 2018, 71, 113–117. [Google Scholar] [CrossRef]
- Zuo, H.; Nygård, O.; Vollset, S.E.; Ueland, P.M.; Ulvik, A.; Midttun, Ø.; Meyer, K.; Igland, J.; Sulo, G.; Tell, G.S. Smoking, Plasma Cotinine and Risk of Atrial Fibrillation: The Hordaland Health Study. J. Intern. Med. 2018, 283, 73–82. [Google Scholar] [CrossRef]
- Lu, Y.; Guo, Y.; Lin, H.; Wang, Z.; Zheng, L. Genetically Determined Tobacco and Alcohol Use and Risk of Atrial Fibrillation. BMC Med. Genomics 2021, 14, 73. [Google Scholar] [CrossRef]
- Aune, D.; Schlesinger, S.; Norat, T.; Riboli, E. Tobacco Smoking and the Risk of Atrial Fibrillation: A Systematic Review and Meta-Analysis of Prospective Studies. Eur. J. Prev. Cardiol. 2018, 25, 1437–1451. [Google Scholar] [CrossRef]
- Dixit, S.; Pletcher, M.J.; Vittinghoff, E.; Imburgia, K.; Maguire, C.; Whitman, I.R.; Glantz, S.A.; Olgin, J.E.; Marcus, G.M. Secondhand Smoke and Atrial Fibrillation: Data from the Health EHeart Study. Heart Rhythm 2016, 13, 3–9. [Google Scholar] [CrossRef]
- Groh, C.A.; Vittinghoff, E.; Benjamin, E.J.; Dupuis, J.; Marcus, G.M. Childhood Tobacco Smoke Exposure and Risk of Atrial Fibrillation in Adulthood. J. Am. Coll. Cardiol. 2019, 74, 1658–1664. [Google Scholar] [CrossRef]
- Staerk, L.; Wang, B.; Preis, S.R.; Larson, M.G.; Lubitz, S.A.; Ellinor, P.T.; McManus, D.D.; Ko, D.; Weng, L.-C.; Lunetta, K.L.; et al. Lifetime Risk of Atrial Fibrillation According to Optimal, Borderline, or Elevated Levels of Risk Factors: Cohort Study Based on Longitudinal Data from the Framingham Heart Study. BMJ 2018, 361, k1453. [Google Scholar] [CrossRef]
- Zhu, W.; Yuan, P.; Shen, Y.; Wan, R.; Hong, K. Association of Smoking with the Risk of Incident Atrial Fibrillation: A Meta-Analysis of Prospective Studies. Int. J. Cardiol. 2016, 218, 259–266. [Google Scholar] [CrossRef]
- Wang, Q.; Guo, Y.; Wu, C.; Yin, L.; Li, W.; Shen, H.; Xi, W.; Zhang, T.; He, J.; Wang, Z. Smoking as a Risk Factor for the Occurrence of Atrial Fibrillation in Men Versus Women: A Meta-Analysis of Prospective Cohort Studies. Heart Lung Circ. 2018, 27, 58–65. [Google Scholar] [CrossRef]
- Fukamizu, S.; Sakurada, H.; Takano, M.; Hojo, R.; Nakai, M.; Yuba, T.; Komiyama, K.; Tatsumoto, A.; Maeno, K.; Mizusawa, Y.; et al. Effect of Cigarette Smoking on the Risk of Atrial Fibrillation Recurrence after Pulmonary Vein Isolation. J. Arrhythmia 2010, 26, 21–29. [Google Scholar] [CrossRef]
- Aytemir, K.; Oto, A.; Canpolat, U.; Sunman, H.; Yorgun, H.; Şahiner, L.; Kaya, E.B. Immediate and Medium-Term Outcomes of Cryoballoon-Based Pulmonary Vein Isolation in Patients with Paroxysmal and Persistent Atrial Fibrillation: Single-Centre Experience. J. Interv. Card. Electrophysiol. 2013, 38, 187–195. [Google Scholar] [CrossRef]
- Cheng, W.-H.; Lo, L.-W.; Lin, Y.-J.; Chang, S.-L.; Hu, Y.-F.; Hung, Y.; Chung, F.-P.; Chang, T.-Y.; Huang, T.-C.; Yamada, S.; et al. Cigarette Smoking Causes a Worse Long-Term Outcome in Persistent Atrial Fibrillation Following Catheter Ablation. J. Cardiovasc. Electrophysiol. 2018, 29, 699–706. [Google Scholar] [CrossRef]
- Kinoshita, M.; Herges, R.M.; Hodge, D.O.; Friedman, L.; Ammash, N.M.; Bruce, C.J.; Somers, V.; Malouf, J.F.; Askelin, J.; Gilles, J.A.; et al. Role of Smoking in the Recurrence of Atrial Arrhythmias After Cardioversion. Am. J. Cardiol. 2009, 104, 678–682. [Google Scholar] [CrossRef]
- Lee, S.H.; Kim, B.J.; Kang, J.; Seo, D.C.; Lee, S.J. Association of Self-Reported and Cotinine-Verified Smoking Status with Atrial Arrhythmia. J. Korean Med. Sci. 2020, 35, e296. [Google Scholar] [CrossRef]
- Caponnetto, P.; Campagna, D.; Cibella, F.; Morjaria, J.B.; Caruso, M.; Russo, C.; Polosa, R. EffiCiency and Safety of an ELectronic CigAreTte (ECLAT) as Tobacco Cigarettes Substitute: A Prospective 12-Month Randomized Control Design Study. PLoS ONE 2013, 8, e66317. [Google Scholar] [CrossRef]
- Bullen, C.; Howe, C.; Laugesen, M.; McRobbie, H.; Parag, V.; Williman, J.; Walker, N. Electronic Cigarettes for Smoking Cessation: A Randomised Controlled Trial. Lancet 2013, 382, 1629–1637. [Google Scholar] [CrossRef]
- Brown, J.; Beard, E.; Kotz, D.; Michie, S.; West, R. Real-World Effectiveness of e-Cigarettes When Used to Aid Smoking Cessation: A Cross-Sectional Population Study. Addiction 2014, 109, 1531–1540. [Google Scholar] [CrossRef]
- Abouassali, O.; Chang, M.; Chidipi, B.; Martinez, J.L.; Reiser, M.; Kanithi, M.; Soni, R.; McDonald, T.V.; Herweg, B.; Saiz, J.; et al. In Vitro and in Vivo Cardiac Toxicity of Flavored Electronic Nicotine Delivery Systems. Am. J. Physiol. Heart Circ. Physiol. 2021, 320, H133–H143. [Google Scholar] [CrossRef] [PubMed]
- Monroy, A.E.; Hommel, E.; Smith, S.T.; Raji, M. Paroxysmal Atrial Fibrillation Following Electronic Cigarette Use in an Elderly Woman. Clin. Geriatr. 2012, 20, 28–32. [Google Scholar]
- Lowe, R.B.; Klingaman, C.; Golten, A.; Davis, T.W. Atrial Fibrillation with E-Cigarette Use in an Otherwise Healthy Adolescent Male. Pediatrics 2020, 146, 312–313. [Google Scholar] [CrossRef]
- Hergens, M.-P.; Galanti, R.; Hansson, J.; Fredlund, P.; Ahlbom, A.; Alfredsson, L.; Bellocco, R.; Eriksson, M.; Fransson, E.I.; Hallqvist, J.; et al. Use of Scandinavian Moist Smokeless Tobacco (Snus) and the Risk of Atrial Fibrillation. Epidemiology 2014, 25, 872–876. [Google Scholar] [CrossRef]
- Arefalk, G.; Hergens, M.-P.; Ingelsson, E.; Ärnlöv, J.; Michaëlsson, K.; Lind, L.; Ye, W.; Nyrén, O.; Lambe, M.; Sundström, J. Smokeless Tobacco (Snus) and Risk of Heart Failure: Results from Two Swedish Cohorts. Eur. J. Prev. Cardiol. 2012, 19, 1120–1127. [Google Scholar] [CrossRef]
- Stewart, P.M.; Catterall, J.R. Chronic Nicotine Ingestion and Atrial Fibrillation. Br. Heart J. 1985, 54, 222. [Google Scholar] [CrossRef]
- Rigotti, N.A.; Eagle, K.A. Atrial Fibrillation While Chewing Nicotine Gum. JAMA 1986, 255, 1018. [Google Scholar] [CrossRef]
- Nunes, J.P.L.; Barbosa, E.; Lopes, L.; Alves, C.; Gonçalves, F.R. Nicotine Nasal Inhalation, Atrial Fibrillation and Seizures. Cardiology 2001, 96, 58. [Google Scholar] [CrossRef]
- Korantzopoulos, P.; Liu, T.; Papaioannides, D.; Li, G.; Goudevenos, J.A. Atrial Fibrillation and Marijuana Smoking. Int. J. Clin. Pract. 2008, 62, 308–313. [Google Scholar] [CrossRef]
- Shinton, R.; Beevers, G. Meta-Analysis of Relation between Cigarette Smoking and Stroke. Br. Med. J. 1989, 298, 789. [Google Scholar] [CrossRef]
- Mucha, L.; Stephenson, J.; Morandi, N.; Dirani, R. Meta-Analysis of Disease Risk Associated with Smoking, by Gender and Intensity of Smoking. Gend. Med. 2006, 3, 279–291. [Google Scholar] [CrossRef]
- Peters, S.A.E.; Huxley, R.R.; Woodward, M. Smoking as a Risk Factor for Stroke in Women Compared With Men. Stroke 2013, 44, 2821–2828. [Google Scholar] [CrossRef]
- Pan, B.; Jin, X.; Jun, L.; Qiu, S.; Zheng, Q.; Pan, M. The Relationship between Smoking and Stroke: A Meta-Analysis. Medicine (Baltim) 2019, 98, e14872. [Google Scholar] [CrossRef]
- Wannamethee, S.G.; Shaper, A.G.; Whincup, P.H.; Walker, M. Smoking Cessation and the Risk of Stroke in Middle-Aged Men. JAMA 1995, 274, 155–160. [Google Scholar] [CrossRef]
- Kawachi, I.; Colditz, G.A.; Stampfer, M.J.; Willett, W.C.; Manson, J.E.; Rosner, B.; Speizer, F.E.; Hennekens, C.H. Smoking Cessation and Decreased Risk of Stroke in Women. JAMA 1993, 269, 232–236. [Google Scholar] [CrossRef] [PubMed]
- Lightwood, J.M.; Glantz, S.A. Short-Term Economic and Health Benefits of Smoking Cessation. Circulation 1997, 96, 1089–1096. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, K.; Hirai, T.; Ohara, K.; Fukuda, N.; Numa, S.; Taguchi, Y.; Dougu, N.; Takashima, S.; Nozawa, T.; Tanaka, K.; et al. Impact of Persistent Smoking on Long-Term Outcomes in Patients with Nonvalvular Atrial Fibrillation. J. Cardiol. 2015, 65, 429–433. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.; Chang, J.; Kim, K.; Kim, S.M.; Koo, H.-Y.; Cho, M.H.; Cho, I.Y.; Lee, H.; Son, J.S.; Park, S.M.; et al. Association of Smoking Cessation after Atrial Fibrillation Diagnosis on the Risk of Cardiovascular Disease: A Cohort Study of South Korean Men. BMC Public Health 2020, 20, 168. [Google Scholar] [CrossRef]
- Lee, S.-R.; Choi, E.-K.; Jung, J.-H.; Han, K.-D.; Oh, S.; Lip, G.Y.H. Smoking Cessation after Diagnosis of New-Onset Atrial Fibrillation and the Risk of Stroke and Death. J. Clin. Med. 2021, 10, 2238. [Google Scholar] [CrossRef]
- Epstein, K.A.; Viscoli, C.M.; Spence, J.D.; Young, L.H.; Inzucchi, S.E.; Gorman, M.; Gerstenhaber, B.; Guarino, P.D.; Dixit, A.; Furie, K.L.; et al. Smoking Cessation and Outcome after Ischemic Stroke or TIA. Neurology 2017, 89, 1723. [Google Scholar] [CrossRef]
- Chen, J.; Li, S.; Zheng, K.; Wang, H.; Xie, Y.; Xu, P.; Dai, Z.; Gu, M.; Xia, Y.; Zhao, M.; et al. Impact of Smoking Status on Stroke Recurrence. J. Am. Heart Assoc. 2019, 8, e011696. [Google Scholar] [CrossRef]
- Noubiap, J.J.; Fitzgerald, J.L.; Gallagher, C.; Thomas, G.; Middeldorp, M.E.; Sanders, P. Rates, Predictors, and Impact of Smoking Cessation after Stroke or Transient Ischemic Attack: A Systematic Review and Meta-Analysis. J. Stroke Cerebrovasc. Dis. 2021, 30, 106012. [Google Scholar] [CrossRef]
- Parikh, N.S.; Chatterjee, A.; Díaz, I.; Merkler, A.E.; Murthy, S.B.; Iadecola, C.; Navi, B.B.; Kamel, H. Trends in Active Cigarette Smoking Among Stroke Survivors in the United States, 1999 to 2018. Stroke 2020, 51, 1656–1661. [Google Scholar] [CrossRef]
- Ives, S.P.; Heuschmann, P.U.; Wolfe, C.D.A.; Redfern, J. Patterns of Smoking Cessation in the First 3 Years after Stroke: The South London Stroke Register. Eur. J. Cardiovasc. Prev. Rehabil. 2008, 15, 329–335. [Google Scholar] [CrossRef]
- Albertsen, I.E.; Rasmussen, L.H.; Lane, D.A.; Overvad, T.F.; Skjøth, F.; Overvad, K.; Lip, G.Y.H.; Larsen, T.B. The Impact of Smoking on Thromboembolism and Mortality in Patients With Incident Atrial Fibrillation. Chest 2014, 145, 559–566. [Google Scholar] [CrossRef]
- Kwon, Y.; Norby, F.L.; Jensen, P.N.; Agarwal, S.K.; Soliman, E.Z.; Lip, G.Y.H.; Longstreth, W.T., Jr.; Alonso, A.; Heckbert, S.R.; Chen, L.Y. Association of Smoking, Alcohol, and Obesity with Cardiovascular Death and Ischemic Stroke in Atrial Fibrillation: The Atherosclerosis Risk in Communities (ARIC) Study and Cardiovascular Health Study (CHS). PLoS ONE 2016, 11, e0147065. [Google Scholar] [CrossRef]
- Suzuki, S.; Otsuka, T.; Sagara, K.; Semba, H.; Kano, H.; Matsuno, S.; Takai, H.; Kato, Y.; Uejima, T.; Oikawa, Y.; et al. Effects of Smoking on Ischemic Stroke, Intracranial Hemorrhage, and Coronary Artery Events in Japanese Patients With Non-Valvular Atrial Fibrillation. Int. Heart J. 2017, 58, 506–515. [Google Scholar] [CrossRef]
- Zhu, W.; Guo, L.; Hong, K. Relationship between Smoking and Adverse Outcomes in Patients with Atrial Fibrillation: A Meta-Analysis and Systematic Review. Int. J. Cardiol. 2016, 222, 289–294. [Google Scholar] [CrossRef]
- Csordas, A.; Bernhard, D. The Biology behind the Atherothrombotic Effects of Cigarette Smoke. Nat. Rev. Cardiol. 2013, 10, 219–230. [Google Scholar] [CrossRef]
- McManus, D.D.; Yin, X.; Gladstone, R.; Vittinghoff, E.; Vasan, R.S.; Larson, M.G.; Benjamin, E.J.; Marcus, G.M. Alcohol Consumption, Left Atrial Diameter, and Atrial Fibrillation. J. Am. Heart Assoc. 2016, 5, e004060. [Google Scholar] [CrossRef]
- Miao, L.; Guo, X.; Sun, G.; Bai, Y.; Sun, Y.; Li, Z. Effect of Different Alcohol Consumption Levels on the Left Atrial Size: A Cross-Sectional Study in Rural China. Anatol. J. Cardiol. 2022, 26, 29–36. [Google Scholar] [CrossRef]
- Singh, K.J.; Cohen, B.E.; Na, B.; Regan, M.; Schiller, N.B.; Whooley, M.A. Alcohol Consumption and 5-Year Change in Left Atrial Volume Among Patients With Coronary Heart Disease: Results From the Heart and Soul Study. J. Card. Fail. 2013, 19, 183–189. [Google Scholar] [CrossRef]
- Barmano, N.; Charitakis, E.; Kronstrand, R.; Walfridsson, U.; Karlsson, J.-E.; Walfridsson, H.; Nystrom, F.H. The Association between Alcohol Consumption, Cardiac Biomarkers, Left Atrial Size and Re-Ablation in Patients with Atrial Fibrillation Referred for Catheter Ablation. PLoS ONE 2019, 14, e0215121. [Google Scholar] [CrossRef]
- Hung, C.-L.; Gonçalves, A.; Lai, Y.-J.; Lai, Y.-H.; Sung, K.-T.; Lo, C.-I.; Liu, C.-C.; Kuo, J.-Y.; Hou, C.J.-Y.; Chao, T.-F.; et al. Light to Moderate Habitual Alcohol Consumption Is Associated with Subclinical Ventricular and Left Atrial Mechanical Dysfunction in an Asymptomatic Population: Dose-Response and Propensity Analysis. J. Am. Soc. Echocardiogr. 2016, 29, 1043–1051.e4. [Google Scholar] [CrossRef]
- Hung, C.-L.; Sung, K.-T.; Chang, S.-C.; Liu, Y.-Y.; Kuo, J.-Y.; Huang, W.-H.; Su, C.-H.; Liu, C.-C.; Tsai, S.-Y.; Liu, C.-Y.; et al. Variant Aldehyde Dehydrogenase 2 (ALDH2*2) as a Risk Factor for Mechanical LA Substrate Formation and Atrial Fibrillation with Modest Alcohol Consumption in Ethnic Asians. Biomolecules 2021, 11, 1559. [Google Scholar] [CrossRef]
- Sengul, C.; Cevik, C.; Ozveren, O.; Sunbul, A.; Oduncu, V.; Akgun, T.; Can, M.M.; Semiz, E.; Dindar, I. Acute Alcohol Consumption Is Associated with Increased Interatrial Electromechanical Delay in Healthy Men. Cardiol. J. 2011, 18, 682–686. [Google Scholar] [CrossRef] [PubMed]
- Simon, J.; Fung, K.; Kolossváry, M.; Sanghvi, M.M.; Aung, N.; Paiva, J.M.; Lukaschuk, E.; Carapella, V.; Merkely, B.; Bittencourt, M.S.; et al. Sex-Specific Associations between Alcohol Consumption, Cardiac Morphology, and Function as Assessed by Magnetic Resonance Imaging: Insights Form the UK Biobank Population Study. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 1009–1016. [Google Scholar] [CrossRef] [PubMed]
- Voskoboinik, A.; Costello Benedict, T.; Kalman, E.; Prabhu, S.; Sugumar, H.; Wong, G.; Nalliah, C.; Ling, L.; McLellan, A.; Hettige, T.; et al. Regular Alcohol Consumption Is Associated With Impaired Atrial Mechanical Function in the Atrial Fibrillation Population. JACC Clin. Electrophysiol. 2018, 4, 1451–1459. [Google Scholar] [CrossRef] [PubMed]
- Zagrosek, A.; Messroghli, D.; Schulz, O.; Dietz, R.; Schulz-Menger, J. Effect of Binge Drinking on the Heart as Assessed by Cardiac Magnetic Resonance Imaging. JAMA 2010, 304, 1328–1330. [Google Scholar] [CrossRef] [PubMed]
- Cao, Z.; Wang, T.; Xia, W.; Zhu, B.; Tian, M.; Zhao, R.; Guan, D. A Pilot Metabolomic Study on Myocardial Injury Caused by Chronic Alcohol Consumption—Alcoholic Cardiomyopathy. Molecules 2021, 26, 2177. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Sun, F.; Armand, L.C.; Wu, R.; Xu, C. Chronic Ethanol Exposure Induces Deleterious Changes in Cardiomyocytes Derived from Human Induced Pluripotent Stem Cells. Stem Cell Rev. Rep. 2021, 17, 2314–2331. [Google Scholar] [CrossRef]
- Nakashima, M.A.; Silva, C.B.P.; Gonzaga, N.A.; Simplicio, J.A.; Omoto, A.C.M.; Tirapelli, L.F.; Tanus-Santos, J.E.; Tirapelli, C.R. Chronic Ethanol Consumption Increases Reactive Oxygen Species Generation and the Synthesis of Pro-Inflammatory Proteins in the Heart through TNFR1-Dependent Mechanisms. Cytokine 2019, 121, 154734. [Google Scholar] [CrossRef]
- Mouton, A.J.; El Hajj, E.C.; Ninh, V.K.; Siggins, R.W.; Gardner, J.D. Inflammatory Cardiac Fibroblast Phenotype Underlies Chronic Alcohol-Induced Cardiac Atrophy and Dysfunction. Life Sci. 2020, 245, 117330. [Google Scholar] [CrossRef]
- Yang, L.; Wang, S.; Ma, J.; Li, J.; Yang, J.; Bucala, R.; Ren, J. CD74 Knockout Attenuates Alcohol Intake-Induced Cardiac Dysfunction through AMPK-Skp2-Mediated Regulation of Autophagy. Biochim. Biophys. Acta BBA Mol. Basis Dis. 2019, 1865, 2368–2378. [Google Scholar] [CrossRef]
- Zhang, F.; Wang, K.; Zhang, S.; Li, J.; Fan, R.; Chen, X.; Pei, J. Accelerated FASTK MRNA Degradation Induced by Oxidative Stress Is Responsible for the Destroyed Myocardial Mitochondrial Gene Expression and Respiratory Function in Alcoholic Cardiomyopathy. Redox Biol. 2021, 38, 101778. [Google Scholar] [CrossRef]
- Guan, Z.; Lui, C.Y.; Morkin, E.; Bahl, J.J. Oxidative Stress and Apoptosis in Cardiomyocyte Induced by High-Dose Alcohol. J. Cardiovasc. Pharmacol. 2004, 44, 696–702. [Google Scholar] [CrossRef]
- Jing, L.; Jin, C.; Li, S.; Zhang, F.; Yuan, L.; Li, W.; Sang, Y.; Li, S.; Zhou, L. Chronic Alcohol Intake-Induced Oxidative Stress and Apoptosis: Role of CYP2E1 and Calpain-1 in Alcoholic Cardiomyopathy. Mol. Cell. Biochem. 2012, 359, 283–292. [Google Scholar] [CrossRef]
- Song, Y.; Li, H.; Ma, S.; Zhu, M.; Lu, W.; Lan, F.; Cui, M. Losartan Protects Human Stem Cell-Derived Cardiomyocytes from Angiotensin II-Induced Alcoholic Cardiotoxicity. Cell Death Discov. 2022, 8, 134. [Google Scholar] [CrossRef]
- Wang, Y.; Li, Z.; Zhang, Y.; Yang, W.; Sun, J.; Shan, L.; Li, W. Targeting Pin1 Protects Mouse Cardiomyocytes from High-Dose Alcohol-Induced Apoptosis. Oxid. Med. Cell. Longev. 2016, 2016, 4528906. [Google Scholar] [CrossRef]
- Ferrer-Curriu, G.; Guitart-Mampel, M.; Rupérez, C.; Zamora, M.; Crispi, F.; Villarroya, F.; Fernández-Solà, J.; Garrabou, G.; Planavila, A. The Protective Effect of Fibroblast Growth Factor-21 in Alcoholic Cardiomyopathy: A Role in Protecting Cardiac Mitochondrial Function. J. Pathol. 2021, 253, 198–208. [Google Scholar] [CrossRef]
- Sato, M.; Maulik, N.; Das, D.K. Cardioprotection with Alcohol. Ann. N. Y. Acad. Sci. 2002, 957, 122–135. [Google Scholar] [CrossRef]
- Umoh, N.A.; Walker, R.K.; Al-Rubaiee, M.; Jeffress, M.A.; Haddad, G.E. Acute Alcohol Modulates Cardiac Function as PI3K/Akt Regulates Oxidative Stress. Alcohol. Clin. Exp. Res. 2014, 38, 1847–1864. [Google Scholar] [CrossRef]
- Wang, Y.; Zhao, J.; Yang, W.; Bi, Y.; Chi, J.; Tian, J.; Li, W. High-Dose Alcohol Induces Reactive Oxygen Species-Mediated Apoptosis via PKC-β/P66Shc in Mouse Primary Cardiomyocytes. Biochem. Biophys. Res. Commun. 2015, 456, 656–661. [Google Scholar] [CrossRef]
- Dai, C.; Kong, B.; Qin, T.; Xiao, Z.; Fang, J.; Gong, Y.; Zhu, J.; Liu, Q.; Fu, H.; Meng, H.; et al. Inhibition of Ferroptosis Reduces Susceptibility to Frequent Excessive Alcohol Consumption-Induced Atrial Fibrillation. Toxicology 2022, 465, 153055. [Google Scholar] [CrossRef]
- Tian, G.; Yu, Y.; Deng, H.; Yang, L.; Shi, X.; Yu, B. Empagliflozin Alleviates Ethanol-Induced Cardiomyocyte Injury through Inhibition of Mitochondrial Apoptosis via a SIRT1/PTEN/Akt Pathway. Clin. Exp. Pharmacol. Physiol. 2021, 48, 837–845. [Google Scholar] [CrossRef]
- Guo, J.-M.; Liu, A.-J.; Zang, P.; Dong, W.-Z.; Ying, L.; Wang, W.; Xu, P.; Song, X.-R.; Cai, J.; Zhang, S.-Q.; et al. ALDH2 Protects against Stroke by Clearing 4-HNE. Cell Res. 2013, 23, 915–930. [Google Scholar] [CrossRef]
- Hsu, L.-A.; Tsai, F.-C.; Yeh, Y.-H.; Chang, C.-J.; Kuo, C.-T.; Chen, W.-J.; Tsai, H.-Y.; Chang, G.-J. Aldehyde Dehydrogenase 2 Ameliorates Chronic Alcohol Consumption-Induced Atrial Fibrillation through Detoxification of 4-HNE. Int. J. Mol. Sci. 2020, 21, 6678. [Google Scholar] [CrossRef]
- Hu, Y.-F.; Wu, C.-H.; Lai, T.-C.; Chang, Y.-C.; Hwang, M.-J.; Chang, T.-Y.; Weng, C.-H.; Chang, P.M.-H.; Chen, C.-H.; Mochly-Rosen, D.; et al. ALDH2 Deficiency Induces Atrial Fibrillation through Dysregulated Cardiac Sodium Channel and Mitochondrial Bioenergetics: A Multi-Omics Analysis. Biochim. Biophys. Acta BBA Mol. Basis Dis. 2021, 1867, 166088. [Google Scholar] [CrossRef]
- Montiel-Jaen, M.G.; Monsalvo-Villegas, A.; Ávila, G. Modulating ALDH2 Reveals a Differential Dependence on ROS for Hypertrophy and SR Ca2+ Release in Aldosterone-Treated Cardiac Myocytes. Biochem. Biophys. Res. Commun. 2021, 536, 7–13. [Google Scholar] [CrossRef]
- Doser, T.A.; Turdi, S.; Thomas, D.P.; Epstein, P.N.; Li, S.-Y.; Ren, J. Transgenic Overexpression of Aldehyde Dehydrogenase-2 Rescues Chronic Alcohol Intake–Induced Myocardial Hypertrophy and Contractile Dysfunction. Circulation 2009, 119, 1941–1949. [Google Scholar] [CrossRef]
- Brandt, M.; Garlapati, V.; Oelze, M.; Sotiriou, E.; Knorr, M.; Kröller-Schön, S.; Kossmann, S.; Schönfelder, T.; Morawietz, H.; Schulz, E.; et al. NOX2 Amplifies Acetaldehyde-Mediated Cardiomyocyte Mitochondrial Dysfunction in Alcoholic Cardiomyopathy. Sci. Rep. 2016, 6, 32554. [Google Scholar] [CrossRef] [PubMed]
- Lazo, M.; Chen, Y.; McEvoy, J.W.; Ndumele, C.; Konety, S.; Ballantyne, C.M.; Sharrett, A.R.; Selvin, E. Alcohol Consumption and Cardiac Biomarkers: The Atherosclerosis Risk in Communities (ARIC) Study. Clin. Chem. 2016, 62, 1202–1210. [Google Scholar] [CrossRef] [PubMed]
- Iakunchykova, O.; Averina, M.; Kudryavtsev, A.V.; Wilsgaard, T.; Soloviev, A.; Schirmer, H.; Cook, S.; Leon, D.A. Evidence for a Direct Harmful Effect of Alcohol on Myocardial Health: A Large Cross-Sectional Study of Consumption Patterns and Cardiovascular Disease Risk Biomarkers From Northwest Russia, 2015 to 2017. J. Am. Heart Assoc. 2020, 9, e014491. [Google Scholar] [CrossRef] [PubMed]
- Clergue-Duval, V.; Sivapalan, R.; Hispard, E.; Azuar, J.; Bellivier, F.; Bloch, V.; Vorspan, F.; Naccache, F.; Questel, F. BNP Worsens 12 Days after Alcohol Cessation While Other Cardiovascular Risk Biomarkers Improve: An Observational Study. Alcohol 2021, 90, 39–43. [Google Scholar] [CrossRef]
- Csengeri, D.; Sprünker, N.-A.; Di Castelnuovo, A.; Niiranen, T.; Vishram-Nielsen, J.K.; Costanzo, S.; Söderberg, S.; Jensen, S.M.; Vartiainen, E.; Donati, M.B.; et al. Alcohol Consumption, Cardiac Biomarkers, and Risk of Atrial Fibrillation and Adverse Outcomes. Eur. Heart J. 2021, 42, 1170–1177. [Google Scholar] [CrossRef]
- Patel, V.B.; Ajmal, R.; Sherwood, R.A.; Sullivan, A.; Richardson, P.J.; Preedy, V.R. Cardioprotective Effect of Propranolol From Alcohol-Induced Heart Muscle Damage as Assessed by Plasma Cardiac Troponin-T. Alcohol. Clin. Exp. Res. 2001, 25, 882–889. [Google Scholar] [CrossRef]
- Mäki, T.; Toivonen, L.; Koskinen, P.; Näveri, H.; Härkönen, M.; Leinonen, H. Effect of Ethanol Drinking, Hangover, and Exercise on Adrenergic Activity and Heart Rate Variability in Patients with a History of Alcohol-Induced Atrial Fibrillation. Am. J. Cardiol. 1998, 82, 317–322. [Google Scholar] [CrossRef]
- Perman, E.S. The Effect of Ethyl Alcohol on the Secretion from the Adrenal Medulla in Man. Acta Physiol. Scand. 1958, 44, 241–247. [Google Scholar] [CrossRef]
- Brunner, S.; Herbel, R.; Drobesch, C.; Peters, A.; Massberg, S.; Kääb, S.; Sinner, M.F. Alcohol Consumption, Sinus Tachycardia, and Cardiac Arrhythmias at the Munich Octoberfest: Results from the Munich Beer Related Electrocardiogram Workup Study (MunichBREW). Eur. Heart J. 2017, 38, 2100–2106. [Google Scholar] [CrossRef]
- Weise, F.; Krell, D.; Brinkhoff, N. Acute Alcohol Ingestion Reduces Heart Rate Variability. Drug Alcohol Depend. 1986, 17, 89–91. [Google Scholar] [CrossRef]
- Gonzalez Gonzalez, J.; Mendez Llorens, A.; Mendez Novoa, A.; Cordero Valeriano, J.J. Effect of Acute Alcohol Ingestion on Short-Term Heart Rate Fluctuations. J. Stud. Alcohol 1992, 53, 86–90. [Google Scholar] [CrossRef]
- Koskinen, P.; Virolainen, J.; Kupari, M. Acute Alcohol Intake Decreases Short-Term Heart Rate Variability in Healthy Subjects. Clin. Sci. 1994, 87, 225–230. [Google Scholar] [CrossRef]
- Süfke, S.; Fiedler, S.; Djonlagiç, H.; Kibbel, T. Continuous analysis of heart rate variability for examination of cardiac autonomic nervous system after alcohol intoxication. Med. Klin. (Munich) 2009, 104, 511–519. [Google Scholar] [CrossRef]
- Spaak, J.; Tomlinson, G.; McGowan, C.L.; Soleas, G.J.; Morris, B.L.; Picton, P.; Notarius, C.F.; Floras, J.S. Dose-Related Effects of Red Wine and Alcohol on Heart Rate Variability. Am. J. Physiol. Heart Circ. Physiol. 2010, 298, H2226–H2231. [Google Scholar] [CrossRef] [PubMed]
- Steinbigler, P.; Haberl, R.; König, B.; Steinbeck, G. P-Wave Signal Averaging Identifies Patients Prone to Alcohol-Induced Paroxysmal Atrial Fibrillation. Am. J. Cardiol. 2003, 91, 491–494. [Google Scholar] [CrossRef]
- Aasebø, W.; Aasebø, W.; Erikssen, J.; Jonsbu, J.; Stavem, K. ECG Changes in Patients with Acute Ethanol Intoxication. Scand. Cardiovasc. J. 2007, 41, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Uyarel, H.; Ozdöl, C.; Karabulut, A.; Okmen, E.; Cam, N. Acute Alcohol Intake and P-Wave Dispersion in Healthy Men. Anadolu Kardiyol. Derg. 2005, 5, 289–293. [Google Scholar]
- Baykara, S.; Ocak, D.; Berk, Ş.Ş.; Köroğlu, S. Analysis of QT Dispersion, Corrected QT Dispersion, and P-Wave Dispersion Values in Alcohol Use Disorder Patients With Excessive Alcohol Use. Prim. Care Companion CNS Disord. 2020, 22, 19m02541. [Google Scholar] [CrossRef]
- Marcus, G.M.; Dukes Jonathan, W.; Vittinghoff, E.; Nah, G.; Badhwar, N.; Moss Joshua, D.; Lee Randall, J.; Lee Byron, K.; Tseng Zian, H.; Walters Tomos, E.; et al. A Randomized, Double-Blind, Placebo-Controlled Trial of Intravenous Alcohol to Assess Changes in Atrial Electrophysiology. JACC Clin. Electrophysiol. 2021, 7, 662–670. [Google Scholar] [CrossRef]
- Qiao, Y.; Shi, R.; Hou, B.; Wu, L.; Zheng, L.; Ding, L.; Chen, G.; Zhang, S.; Yao, Y. Impact of Alcohol Consumption on Substrate Remodeling and Ablation Outcome of Paroxysmal Atrial Fibrillation. J. Am. Heart Assoc. 2015, 4, e002349. [Google Scholar] [CrossRef]
- Voskoboinik, A.; Wong, G.; Lee, G.; Nalliah, C.; Hawson, J.; Prabhu, S.; Sugumar, H.; Ling, L.-H.; McLellan, A.; Morton, J.; et al. Moderate Alcohol Consumption Is Associated with Atrial Electrical and Structural Changes: Insights from High-Density Left Atrial Electroanatomic Mapping. Heart Rhythm 2019, 16, 251–259. [Google Scholar] [CrossRef]
- Yan, J.; Thomson Justin, K.; Zhao, W.; Gao, X.; Huang, F.; Chen, B.; Liang, Q.; Song, L.; Fill, M.; Ai, X. Role of Stress Kinase JNK in Binge Alcohol-Evoked Atrial Arrhythmia. J. Am. Coll. Cardiol. 2018, 71, 1459–1470. [Google Scholar] [CrossRef]
- Piano, M.R.; Rosenblum, C.; Solaro, R.J.; Schwertz, D. Calcium Sensitivity and the Effect of the Calcium Sensitizing Drug Pimobendan in the Alcoholic Isolated Rat Atrium. J. Cardiovasc. Pharmacol. 1999, 33, 237–242. [Google Scholar] [CrossRef]
- Zhao, Y.; Sun, J.; Hu, J.; Bo, N.; Yu, B. Effect of ethanol and its metabolites on acetylcholine-sensitive K(+) channel Kir3.1 protein expression of neonatal rat primary atrial cardiomyocytes. Zhonghua Xin Xue Guan Bing Za Zhi 2015, 43, 609–613. [Google Scholar]
- Anadon, M.J.; Almendral, J.; González, P.; Zaballos, M.; Delcan, J.L.; De Guevara, J.L. Alcohol Concentration Determines the Type of Atrial Arrhythmia Induced in a Porcine Model of Acute Alcoholic Intoxication. Pacing Clin. Electrophysiol. 1996, 19, 1962–1967. [Google Scholar] [CrossRef]
- Laszlo, R.; Eick, C.; Schwiebert, M.; Schreiner, B.; Weig, H.-J.; Weretka, S.; Bosch, R.F.; Schreieck, J. Alcohol-Induced Electrical Remodeling: Effects of Sustained Short-Term Ethanol Infusion on Ion Currents in Rabbit Atrium. Alcohol. Clin. Exp. Res. 2009, 33, 1697–1703. [Google Scholar] [CrossRef]
- Chen, Y.-C.; Chen, S.-A.; Chen, Y.-J.; Tai, C.-T.; Chan, P.; Lin, C.-I. Effect of Ethanol on the Electrophysiological Characteristics of Pulmonary Vein Cardiomyocytes. Eur. J. Pharmacol. 2004, 483, 215–222. [Google Scholar] [CrossRef]
- Zhang, H.; Ruan, H.; Rahmutula, D.; Wilson, E.; Marcus, G.M.; Vedantham, V.; Olgin, J.E. Effect of Acute and Chronic Ethanol on Atrial Fibrillation Vulnerability in Rats. Heart Rhythm 2020, 17, 654–660. [Google Scholar] [CrossRef]
- Ettinger, P.O.; Wu, C.F.; Cruz, C.D.L.; Weisse, A.B.; Sultan Ahmed, S.; Regan, T.J. Arrhythmias and the “Holiday Heart”: Alcoholassociated Cardiac Rhythm Disorders. Am. Heart J. 1978, 95, 555–562. [Google Scholar] [CrossRef]
- Frost, L.; Vestergaard, P. Alcohol and Risk of Atrial Fibrillation or Flutter: A Cohort Study. Arch. Intern. Med. 2004, 164, 1993–1998. [Google Scholar] [CrossRef]
- Mukamal, K.J.; Tolstrup, J.S.; Friberg, J.; Jensen, G.; Grønbæk, M. Alcohol Consumption and Risk of Atrial Fibrillation in Men and Women. Circulation 2005, 112, 1736–1742. [Google Scholar] [CrossRef]
- Mukamal, K.J.; Psaty, B.M.; Rautaharju, P.M.; Furberg, C.D.; Kuller, L.H.; Mittleman, M.A.; Gottdiener, J.S.; Siscovick, D.S. Alcohol Consumption and Risk and Prognosis of Atrial Fibrillation among Older Adults: The Cardiovascular Health Study. Am. Heart J. 2007, 153, 260–266. [Google Scholar] [CrossRef]
- Conen, D.; Tedrow, U.B.; Cook, N.R.; Moorthy, M.V.; Buring, J.E.; Albert, C.M. Alcohol Consumption and Risk of Incident Atrial Fibrillation in Women. JAMA 2008, 300, 2489–2496. [Google Scholar] [CrossRef]
- Shen, J.; Johnson, V.M.; Sullivan, L.M.; Jacques, P.F.; Magnani, J.W.; Lubitz, S.A.; Pandey, S.; Levy, D.; Vasan, R.S.; Quatromoni, P.A.; et al. Dietary Factors and Incident Atrial Fibrillation: The Framingham Heart Study. Am. J. Clin. Nutr. 2011, 93, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Mente, A.; Yusuf, S.; Gao, P.; Sleight, P.; Zhu, J.; Fagard, R.; Lonn, E.; Teo, K.K. Alcohol Consumption and the Risk of Incident Atrial Fibrillation among People with Cardiovascular Disease. Can. Med. Assoc. J. 2012, 184, E857. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Drca, N.; Wolk, A. Alcohol Consumption and Risk of Atrial Fibrillation: A Prospective Study and Dose-Response Meta-Analysis. J. Am. Coll. Cardiol. 2014, 64, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Samokhvalov, A.V.; Irving, H.M.; Rehm, J. Alcohol Consumption as a Risk Factor for Atrial Fibrillation: A Systematic Review and Meta-Analysis. Eur. J. Cardiovasc. Prev. Rehabil. 2010, 17, 706–712. [Google Scholar] [CrossRef]
- Kodama, S.; Saito, K.; Tanaka, S.; Horikawa, C.; Saito, A.; Heianza, Y.; Anasako, Y.; Nishigaki, Y.; Yachi, Y.; Iida, K.T.; et al. Alcohol Consumption and Risk of Atrial Fibrillation. J. Am. Coll. Cardiol. 2011, 57, 427–436. [Google Scholar] [CrossRef]
- Gallagher, C.; Hendriks, J.M.L.; Elliott, A.D.; Wong, C.X.; Rangnekar, G.; Middeldorp, M.E.; Mahajan, R.; Lau, D.H.; Sanders, P. Alcohol and Incident Atrial Fibrillation—A Systematic Review and Meta-Analysis. Int. J. Cardiol. 2017, 246, 46–52. [Google Scholar] [CrossRef]
- Voskoboinik, A.; Prabhu, S.; Ling, L.; Kalman Jonathan, M.; Kistler, P.M. Alcohol and Atrial Fibrillation. J. Am. Coll. Cardiol. 2016, 68, 2567–2576. [Google Scholar] [CrossRef]
- Giannopoulos, G.; Anagnostopoulos, I.; Kousta, M.; Vergopoulos, S.; Deftereos, S.; Vassilikos, V. Alcohol Consumption and the Risk of Incident Atrial Fibrillation: A Meta-Analysis. Diagnostics 2022, 12, 479. [Google Scholar] [CrossRef]
- Bazal, P.; Gea, A.; Martínez-González, M.A.; Salas-Salvadó, J.; Asensio, E.M.; Muñoz-Bravo, C.; Fiol, M.; Muñoz, M.A.; Lapetra, J.; Serra-Majem, L.L.; et al. Mediterranean Alcohol-Drinking Pattern, Low to Moderate Alcohol Intake and Risk of Atrial Fibrillation in the PREDIMED Study. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 676–683. [Google Scholar] [CrossRef]
- Tu Samuel, J.; Gallagher, C.; Elliott Adrian, D.; Linz, D.; Pitman Bradley, M.; Hendriks Jeroen, M.L.; Lau Dennis, H.; Sanders, P.; Wong Christopher, X. Risk Thresholds for Total and Beverage-Specific Alcohol Consumption and Incident Atrial Fibrillation. JACC Clin. Electrophysiol. 2021, 7, 1561–1569. [Google Scholar] [CrossRef]
- Djoussé, L.; Levy, D.; Benjamin, E.J.; Blease, S.J.; Russ, A.; Larson, M.G.; Massaro, J.M.; D’Agostino, R.B.; Wolf, P.A.; Ellison, R.C. Long-Term Alcohol Consumption and the Risk of Atrial Fibrillation in the Framingham Study. Am. J. Cardiol. 2004, 93, 710–713. [Google Scholar] [CrossRef]
- Voskoboinik, A.; Kalman, J.M.; De Silva, A.; Nicholls, T.; Costello, B.; Nanayakkara, S.; Prabhu, S.; Stub, D.; Azzopardi, S.; Vizi, D.; et al. Alcohol Abstinence in Drinkers with Atrial Fibrillation. N. Engl. J. Med. 2020, 382, 20–28. [Google Scholar] [CrossRef]
- Dixit, S.; Alonso, A.; Vittinghoff, E.; Soliman, E.; Chen, L.Y.; Marcus, G.M. Past Alcohol Consumption and Incident Atrial Fibrillation: The Atherosclerosis Risk in Communities (ARIC) Study. PLoS ONE 2017, 12, e0185228. [Google Scholar] [CrossRef]
- Takigawa, M.; Takahashi, A.; Kuwahara, T.; Takahashi, Y.; Okubo, K.; Nakashima, E.; Watari, Y.; Nakajima, J.; Yamao, K.; Osaka, Y.; et al. Impact of Alcohol Consumption on the Outcome of Catheter Ablation in Patients With Paroxysmal Atrial Fibrillation. J. Am. Heart Assoc. 2016, 5, e004149. [Google Scholar] [CrossRef]
- Yamashita, T.; Arima, Y.; Hoshiyama, T.; Tabata, N.; Sueta, D.; Kawahara, Y.; Ito, M.; Kanazawa, H.; Ishii, M.; Yamanaga, K.; et al. Effect of the ALDH2 Variant on the Prevalence of Atrial Fibrillation in Habitual Drinkers. JACC Asia 2022, 2, 62–70. [Google Scholar] [CrossRef]
- Yang, J.-H.; Jeong, J.-A.; Kweon, S.-S.; Lee, Y.-H.; Choi, S.-W.; Ryu, S.-Y.; Nam, H.-S.; Park, K.-S.; Kim, H.-Y.; Shin, M.-H. Causal Association Between Alcohol Consumption and Atrial Fibrillation: A Mendelian Randomization Study. Korean Circ. J. 2022, 52, 220–230. [Google Scholar] [CrossRef]
- Kozararevic, D.J.; Vojvodic, N.; Dawber, T.; Mcgee, D.; Racic, Z.; Gordon, T.; Zukel, W. FREQUENCY OF ALCOHOL CONSUMPTION AND MORBIDITY AND MORTALITY: The Yugoslavia Cardiovascular Disease Study. Lancet 1980, 315, 613–616. [Google Scholar] [CrossRef]
- Blackwelder, W.C.; Yano, K.; Rhoads, G.G.; Kagan, A.; Gordon, T.; Palesch, Y. Alcohol and Mortality: The Honolulu Heart Study. Am. J. Med. 1980, 68, 164–169. [Google Scholar] [CrossRef]
- Stampfer, M.J.; Colditz, G.A.; Willett, W.C.; Speizer, F.E.; Hennekens, C.H. A Prospective Study of Moderate Alcohol Consumption and the Risk of Coronary Disease and Stroke in Women. N. Engl. J. Med. 1988, 319, 267–273. [Google Scholar] [CrossRef]
- Thun, M.J.; Peto, R.; Lopez, A.D.; Monaco, J.H.; Henley, S.J.; Heath, C.W.; Doll, R. Alcohol Consumption and Mortality among Middle-Aged and Elderly U.S. Adults. N. Engl. J. Med. 1997, 337, 1705–1714. [Google Scholar] [CrossRef]
- Leppälä, J.M.; Paunio, M.; Virtamo, J.; Fogelholm, R.; Albanes, D.; Taylor, P.R.; Heinonen, O.P. Alcohol Consumption and Stroke Incidence in Male Smokers. Circulation 1999, 100, 1209–1214. [Google Scholar] [CrossRef]
- Klatsky, A.L.; Armstrong, M.A.; Friedman, G.D.; Sidney, S. Alcohol Drinking and Risk of Hemorrhagic Stroke. Neuroepidemiology 2002, 21, 115–122. [Google Scholar] [CrossRef]
- Ikehara, S.; Iso, H.; Toyoshima, H.; Date, C.; Yamamoto, A.; Kikuchi, S.; Kondo, T.; Watanabe, Y.; Koizumi, A.; Wada, Y.; et al. Alcohol Consumption and Mortality From Stroke and Coronary Heart Disease Among Japanese Men and Women. Stroke 2008, 39, 2936–2942. [Google Scholar] [CrossRef]
- Lu, M.; Ye, W.; Adami, H.-O.; Weiderpass, E. Stroke Incidence in Women under 60 Years of Age Related to Alcohol Intake and Smoking Habit. Cerebrovasc. Dis. 2008, 25, 517–525. [Google Scholar] [CrossRef]
- Romelsjö, A.; Allebeck, P.; Andréasson, S.; Leifman, A. Alcohol, Mortality and Cardiovascular Events in a 35 Year Follow-up of a Nationwide Representative Cohort of 50,000 Swedish Conscripts up to Age 55. Alcohol Alcohol. 2012, 47, 322–327. [Google Scholar] [CrossRef]
- Yang, L.; Zhou, M.; Sherliker, P.; Cai, Y.; Peto, R.; Wang, L.; Millwood, I.; Smith, M.; Hu, Y.; Yang, G.; et al. Alcohol Drinking and Overall and Cause-Specific Mortality in China: Nationally Representative Prospective Study of 220 000 Men with 15 Years of Follow-Up. Int. J. Epidemiol. 2012, 41, 1101–1113. [Google Scholar] [CrossRef]
- Reynolds, K.; Lewis, B.; Nolen, J.D.L.; Kinney, G.L.; Sathya, B.; He, J. Alcohol Consumption and Risk of Stroke: A Meta-Analysis. JAMA 2003, 289, 579–588. [Google Scholar] [CrossRef]
- Patra, J.; Taylor, B.; Irving, H.; Roerecke, M.; Baliunas, D.; Mohapatra, S.; Rehm, J. Alcohol Consumption and the Risk of Morbidity and Mortality for Different Stroke Types-A Systematic Review and Meta-Analysis. BMC Public Health 2010, 10, 258. [Google Scholar] [CrossRef]
- Zhang, C.; Qin, Y.-Y.; Chen, Q.; Jiang, H.; Chen, X.-Z.; Xu, C.-L.; Mao, P.-J.; He, J.; Zhou, Y.-H. Alcohol Intake and Risk of Stroke: A Dose–Response Meta-Analysis of Prospective Studies. Int. J. Cardiol. 2014, 174, 669–677. [Google Scholar] [CrossRef]
- Larsson, S.C.; Wallin, A.; Wolk, A.; Markus, H.S. Differing Association of Alcohol Consumption with Different Stroke Types: A Systematic Review and Meta-Analysis. BMC Med. 2016, 14, 178. [Google Scholar] [CrossRef]
- Gill, J.S.; Zezulka, A.V.; Shipley, M.J.; Gill, S.K.; Beevers, D.G. Stroke and Alcohol Consumption. N. Engl. J. Med. 1986, 315, 1041–1046. [Google Scholar] [CrossRef] [PubMed]
- Grau, A.J.; Weimar, C.; Buggle, F.; Heinrich, A.; Goertler, M.; Neumaier, S.; Glahn, J.; Brandt, T.; Hacke, W.; Diener, H.-C. Risk Factors, Outcome, and Treatment in Subtypes of Ischemic Stroke. Stroke 2001, 32, 2559–2566. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.-M.; Lee, H.R.; Han, K.; Jeon, K.H.; Kim, D.; Yoo, J.E.; Cho, M.H.; Chun, S.; Lee, S.P.; Nam, K.-W.; et al. Association of Change in Alcohol Consumption With Risk of Ischemic Stroke. Stroke 2022, 53, 2488–2496. [Google Scholar] [CrossRef] [PubMed]
- Biddinger, K.J.; Emdin, C.A.; Haas, M.E.; Wang, M.; Hindy, G.; Ellinor, P.T.; Kathiresan, S.; Khera, A.V.; Aragam, K.G. Association of Habitual Alcohol Intake With Risk of Cardiovascular Disease. JAMA Netw. Open 2022, 5, e223849. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Burgess, S.; Mason, A.M.; Michaëlsson, K. Alcohol Consumption and Cardiovascular Disease. Circ. Genomic Precis. Med. 2020, 13, e002814. [Google Scholar] [CrossRef] [PubMed]
- Lankester, J.; Zanetti, D.; Ingelsson, E.; Assimes, T.L. Alcohol Use and Cardiometabolic Risk in the UK Biobank: A Mendelian Randomization Study. PLoS ONE 2021, 16, e0255801. [Google Scholar] [CrossRef] [PubMed]
- Rimm, E.B.; Williams, P.; Fosher, K.; Criqui, M.; Stampfer, M.J. Moderate Alcohol Intake and Lower Risk of Coronary Heart Disease: Meta-Analysis of Effects on Lipids and Haemostatic Factors. BMJ 1999, 319, 1523. [Google Scholar] [CrossRef]
- Huang, S.; Li, J.; Shearer, G.C.; Lichtenstein, A.H.; Zheng, X.; Wu, Y.; Jin, C.; Wu, S.; Gao, X. Longitudinal Study of Alcohol Consumption and HDL Concentrations: A Community-Based Study. Am. J. Clin. Nutr. 2017, 105, 905–912. [Google Scholar] [CrossRef]
- Yoon, S.-J.; Jung, J.-G.; Lee, S.; Kim, J.-S.; Ahn, S.; Shin, E.-S.; Jang, J.-E.; Lim, S.-H. The Protective Effect of Alcohol Consumption on the Incidence of Cardiovascular Diseases: Is It Real? A Systematic Review and Meta-Analysis of Studies Conducted in Community Settings. BMC Public Health 2020, 20, 90. [Google Scholar] [CrossRef]
- Rodgers, H.; Aitken, P.D.; French, J.M.; Curless, R.H.; Bates, D.; James, O.F. Alcohol and Stroke. A Case-Control Study of Drinking Habits Past and Present. Stroke 1993, 24, 1473–1477. [Google Scholar] [CrossRef]
- Wannamethee, S.G.; Shaper, A.G. Patterns of Alcohol Intake and Risk of Stroke in Middle-Aged British Men. Stroke 1996, 27, 1033–1039. [Google Scholar] [CrossRef]
- Lee, S.-R.; Choi, E.-K.; Jung, J.-H.; Han, K.-D.; Oh, S.; Lip, G.Y.H. Lower Risk of Stroke after Alcohol Abstinence in Patients with Incident Atrial Fibrillation: A Nationwide Population-Based Cohort Study. Eur. Heart J. 2021, 42, 4759–4768. [Google Scholar] [CrossRef]
- Sung, Y.-F.; Lu, C.-C.; Lee, J.-T.; Hung, Y.-J.; Hu, C.-J.; Jeng, J.-S.; Chiou, H.-Y.; Peng, G.-S. Homozygous ALDH2*2 Is an Independent Risk Factor for Ischemic Stroke in Taiwanese Men. Stroke 2016, 47, 2174–2179. [Google Scholar] [CrossRef]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ohlrogge, A.H.; Frost, L.; Schnabel, R.B. Harmful Impact of Tobacco Smoking and Alcohol Consumption on the Atrial Myocardium. Cells 2022, 11, 2576. https://doi.org/10.3390/cells11162576
Ohlrogge AH, Frost L, Schnabel RB. Harmful Impact of Tobacco Smoking and Alcohol Consumption on the Atrial Myocardium. Cells. 2022; 11(16):2576. https://doi.org/10.3390/cells11162576
Chicago/Turabian StyleOhlrogge, Amelie H., Lars Frost, and Renate B. Schnabel. 2022. "Harmful Impact of Tobacco Smoking and Alcohol Consumption on the Atrial Myocardium" Cells 11, no. 16: 2576. https://doi.org/10.3390/cells11162576