
Cerebral Autoregulation Assessment Using the Near Infrared Spectroscopy ‘NIRS-Only’ High Frequency Methodology in Critically Ill Patients: A Prospective Cross-Sectional Study

 , ,
, ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Near infrared spectroscopy (NIRS) Measurements
2.3. Data Collection
2.4. Data Preparation
2.4.1. Transfer Function Analysis (TFA)
- In the NIRS-only methodology, the transfer function analysis (TFA) phase shifts between oxyhemoglobin (oxyHb) and deoxyhemoglobin (deoxyHb) are corrected for phase shifts caused by two physiological factors not related to cerebral autoregulation (CA) effects. First, a constant microvascular transit time (TT blood flow, referred to as TT in the main text) effect, resulting in different phase shifts for different frequencies (‘group delay phenomenon’). Second, the ‘washout effect’, expressed as the ratio between slow changes in blood flow (BF) and blood volume (BV), results in phase shifts (BV expressed as the percentage of BF oscillations, %BF) [9].
![Cells 11 02254 i001]()
- Intact CA
- TFA-phase shift plot showing the high-pass filter principle (i.e., higher phase shift for lower frequencies). An example is shown here in the figure.
- Impaired CA
- TFA-phase shift plot showing low phase shifts (around zero) for all frequencies (i.e., ‘flat line’, not shown in this figure).
- Schematic representation of the TFA phase shift plot. The different curves show (1) the uncorrected oxyHb—deoxyHb phase shift (solid line), (2) the best linear fit on the phase shifts in the high frequency (HF) range, called HF trend line (dotted straight line), and the corrected oxyHb—deoxyHb phase shift (dashdotted line). Phase shift correction is performed by subtracting the extrapolated linear HF trend line from the uncorrected phase shifts over the very low frequency (VLF) and low frequency (LF) ranges. %BF is determined by the y-axis intercept of the linear HF trend line.* The TT(BF) is determined by the x-axis intercept of the linear HF trend line. *
- * calculations described in Elting et al. [9].

2.4.2. Selection of Transfer Function Analysis (TFA) Segments
2.5. Statistical Analysis
3. Results
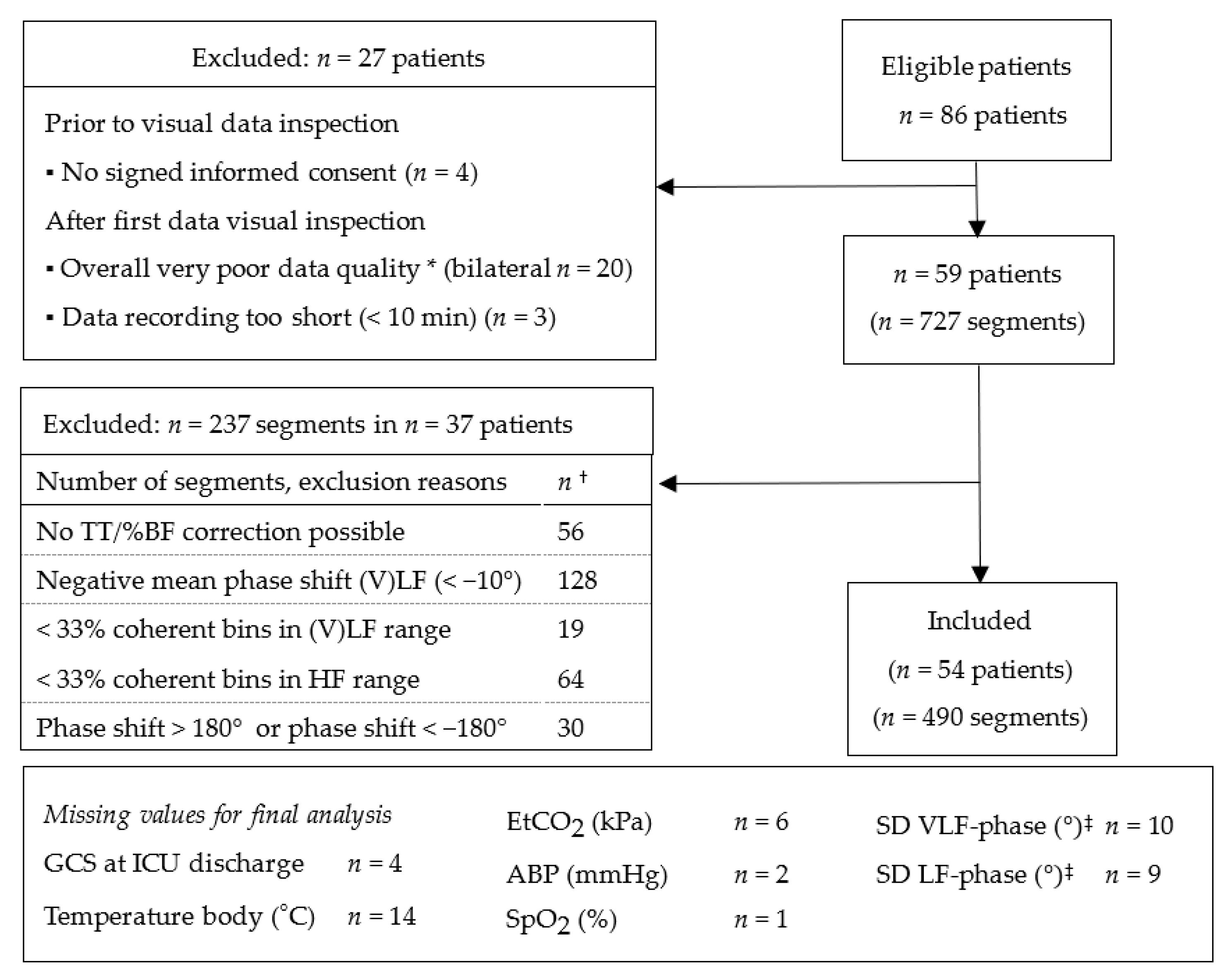
3.1. Selection of Transfer Function Analysis (TFA) Segments
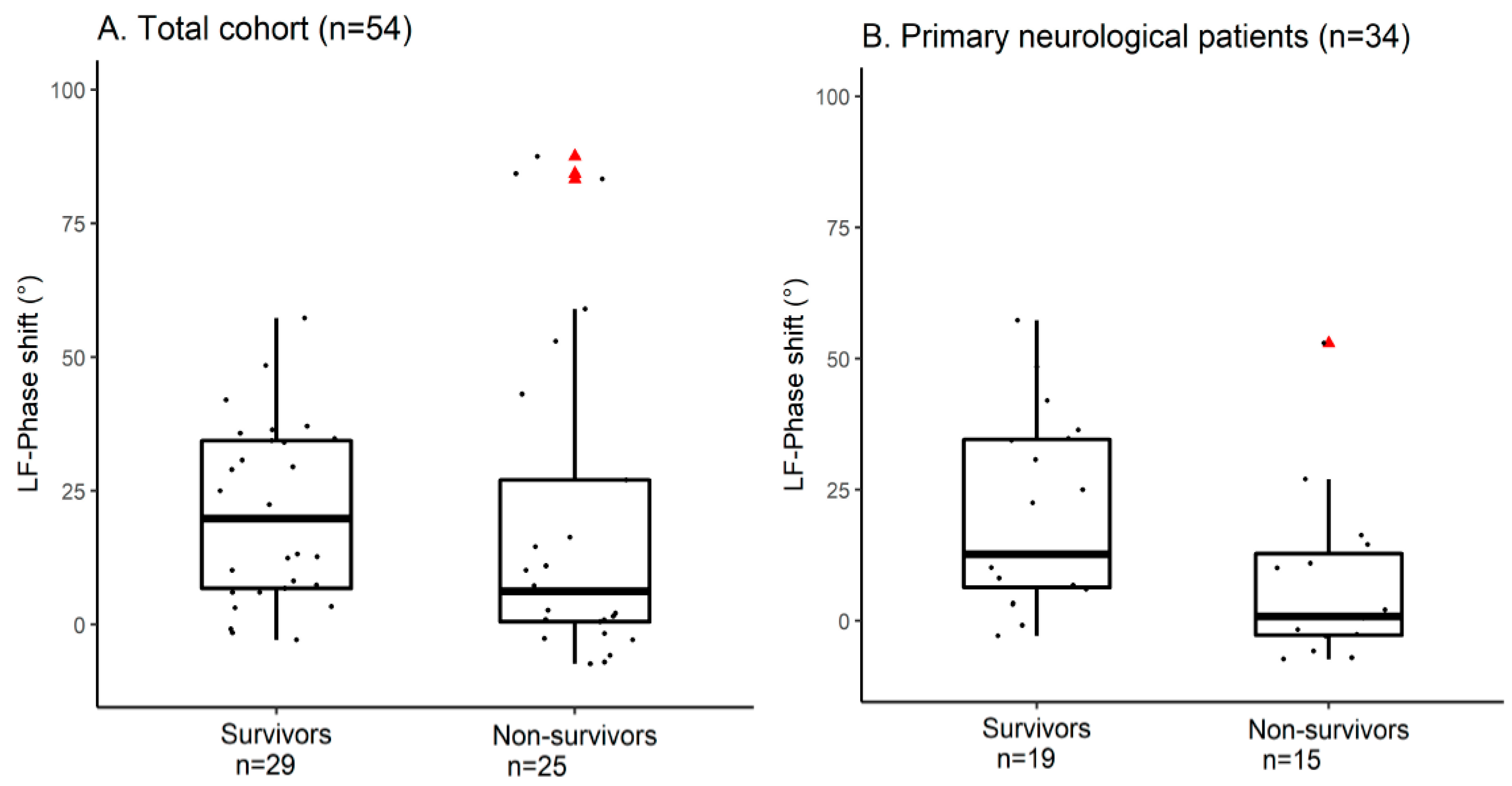
3.2. Cerebral Autoregulation (CA) Parameters
3.3. Primary Neurological Admission Diagnosis
4. Discussion
4.1. Data segment Selection
4.2. Clinical Interpretation
4.3. Limitations
4.4. Future Perspectives
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Czosnyka, M.; Smielewski, P.; Kirkpatrick, P.; Laing, R.J.; Menon, D.; Pickard, J.D. Continuous Assessment of the Cerebral Vasomotor Reactivity in Head Injury. Neurosurgery 1997, 41, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Ameloot, K.; Genbrugge, C.; Meex, I.; Jans, F.; Boer, W.; Vander Laenen, M.; Ferdinande, B.; Mullens, W.; Dupont, M.; Dens, J.; et al. An Observational Near-Infrared Spectroscopy Study on Cerebral Autoregulation in Post-Cardiac Arrest Patients: Time to Drop “one-Size-Fits-All” Hemodynamic Targets? Resuscitation 2015, 90, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Rätsep, T.; Asser, T. Cerebral Hemodynamic Impairment after Aneurysmal Subarachnoid Hemorrhage as Evaluated Using Transcranial Doppler Ultrasonography: Relationship to Delayed Cerebral Ischemia and Clinical Outcome. J. Neurosurg. 2001, 95, 393–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schramm, P.; Klein, K.U.; Falkenberg, L.; Berres, M.; Closhen, D.; Werhahn, K.J.; David, M.; Werner, C.; Engelhard, K. Impaired Cerebrovascular Autoregulation in Patients with Severe Sepsis and Sepsis-Associated Delirium. Crit. Care 2012, 16, R181. [Google Scholar] [CrossRef] [Green Version]
- Ono, M.; Arnaoutakis, G.J.; Fine, D.M.; Brady, K.; Easley, R.B.; Zheng, Y.; Brown, C.; Katz, N.M.; Grams, M.E.; Hogue, C.W. Blood Pressure Excursions below the Cerebral Autoregulation Threshold during Cardiac Surgery Are Associated with Acute Kidney Injury. Crit. Care Med. 2013, 41, 464–471. [Google Scholar] [CrossRef] [Green Version]
- Weiss, M.; Meyfroidt, G.; Aries, M.J.H. Individualized Cerebral Perfusion Pressure in Acute Neurological Injury: Are We Ready for Clinical Use? Curr. Opin. Crit. Care 2022, 28, 123–129. [Google Scholar] [CrossRef]
- Lee, K.F.; Wood, M.D.; Maslove, D.M.; Muscedere, J.G.; Boyd, J.G. Dysfunctional Cerebral Autoregulation Is Associated with Delirium in Critically Ill Adults. J. Cereb. Blood Flow Metab. Off. J. Int. Soc. Cereb. Blood Flow Metab. 2019, 39, 2512–2520. [Google Scholar] [CrossRef]
- Claassen, J.A.H.R.; Meel-van den Abeelen, A.S.S.; Simpson, D.M.; Panerai, R.B. Transfer Function Analysis of Dynamic Cerebral Autoregulation: A White Paper from the International Cerebral Autoregulation Research Network. J. Cereb. Blood Flow Metab. Off. J. Int. Soc. Cereb. Blood Flow Metab. 2016, 36, 665–680. [Google Scholar] [CrossRef] [Green Version]
- Elting, J.W.J.; Tas, J.; Aries, M.J.; Czosnyka, M.; Maurits, N.M. Dynamic Cerebral Autoregulation Estimates Derived from near Infrared Spectroscopy and Transcranial Doppler Are Similar after Correction for Transit Time and Blood Flow and Blood Volume Oscillations. J. Cereb. blood flow Metab. Off. J. Int. Soc. Cereb. Blood Flow Metab. 2020, 40, 135–149. [Google Scholar] [CrossRef] [Green Version]
- Elting, J.W.; Sanders, M.L.; Panerai, R.B.; Aries, M.; Bor-Seng-Shu, E.; Caicedo, A.; Chacon, M.; Gommer, E.D.; Van Huffel, S.; Jara, J.L.; et al. Assessment of Dynamic Cerebral Autoregulation in Humans: Is Reproducibility Dependent on Blood Pressure Variability? PLoS ONE 2020, 15, e0227651. [Google Scholar] [CrossRef] [Green Version]
- Lang, E.W.; Diehl, R.R.; Timmermann, L.; Baron, R.; Deuschl, G.; Mehdorn, H.M.; Zunker, P. Spontaneous Oscillations of Arterial Blood Pressure, Cerebral and Peripheral Blood Flow in Healthy and Comatose Subjects. Neurol. Res. 1999, 21, 665–669. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Lu, H.; Zhang, P.; Mo, X.; Ou, A.; Liu, J.; Zhong, J. The Effect of Data Length on the Assessment of Dynamic Cerebral Autoregulation with Transfer Function Analysis in Neurological ICU Patients. Neurocrit. Care 2021, 36, 21–29. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [Green Version]
- World Medical Association. Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yam, A.T.; Lang, E.W.; Lagopoulos, J.; Yip, K.; Griffith, J.; Mudaliar, Y.; Dorsch, N.W.C. Cerebral Autoregulation and Ageing. J. Clin. Neurosci. Off. J. Neurosurg. Soc. Australas. 2005, 12, 643–646. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. A Language and Environment for Statistical Computing; R Foundation for Statistical Computig: Vienna, Austria, 2021. [Google Scholar]
- Claassen, J.A.H.R.; Levine, B.D.; Zhang, R. Dynamic Cerebral Autoregulation during Repeated Squat-Stand Maneuvers. J. Appl. Physiol. 2009, 106, 153–160. [Google Scholar] [CrossRef] [Green Version]
- Tas, J.; Beqiri, E.; van Kaam, R.C.; Czosnyka, M.; Donnelly, J.; Haeren, R.H.; van der Horst, I.C.C.; Hutchinson, P.J.; van Kuijk, S.M.J.; Liberti, A.L.; et al. Targeting Autoregulation-Guided Cerebral Perfusion Pressure after Traumatic Brain Injury (COGiTATE): A Feasibility Randomized Controlled Clinical Trial. J. Neurotrauma 2021, 38, 2790–2800. [Google Scholar] [CrossRef]
- Zweifel, C.; Dias, C.; Smielewski, P.; Czosnyka, M. Continuous Time-Domain Monitoring of Cerebral Autoregulation in Neurocritical Care. Med. Eng. Phys. 2014, 36, 638–645. [Google Scholar] [CrossRef]
- Claassen, J.A.H.R.; Thijssen, D.H.J.; Panerai, R.B.; Faraci, F.M. Regulation of cerebral blood flow in humans: Physiology and clinical implications of autoregulation. Physiol. Rev. 2021, 101, 1487–1559. [Google Scholar] [CrossRef]
- Zeiler, F.A.; Donnelly, J.; Menon, D.K.; Smielewski, P.; Zweifel, C.; Brady, K.; Czosnyka, M. Continuous autoregulatory indices derived from multi-modal monitoring: Each one is not like the other. J. Neurotrauma 2017, 34, 3070–3080. [Google Scholar] [CrossRef]
- Eleveld, N.; Hoedemaekers, C.W.E.; van Kaam, C.R.; Leijte, G.P.; van den Brule, J.M.D.; Pickkers, P.; Aries, M.J.H.; Maurits, N.M.; Elting, J.W.J. Near-Infrared Spectroscopy-Derived Dynamic Cerebral Autoregulation in Experimental Human Endotoxemia-An Exploratory Study. Front. Neurol. 2021, 12, 695705. [Google Scholar] [CrossRef] [PubMed]
- Klaessens, J.H.G.M.; Hopman, J.C.W.; Liem, K.D.; van Os, S.H.G.; Thijssen, J.M. Effects of Skin on Bias and Reproducibility of Near-Infrared Spectroscopy Measurement of Cerebral Oxygenation Changes in Porcine Brain. J. Biomed. Opt. 2005, 10, 44003. [Google Scholar] [CrossRef] [PubMed]
- Mol, A.; Meskers, C.G.M.; Sanders, M.L.; Müller, M.; Maier, A.B.; van Wezel, R.J.A.; Claassen, J.A.H.R.; Elting, J.W.J. Cerebral Autoregulation Assessed by Near-Infrared Spectroscopy: Validation Using Transcranial Doppler in Patients with Controlled Hypertension, Cognitive Impairment and Controls. Eur. J. Appl. Physiol. 2021, 121, 2165–2176. [Google Scholar] [CrossRef] [PubMed]
- Duncan, A.; Meek, J.H.; Clemence, M.; Elwell, C.E.; Fallon, P.; Tyszczuk, L.; Cope, M.; Delpy, D.T. Measurement of Cranial Optical Path Length as a Function of Age Using Phase Resolved near Infrared Spectroscopy. Pediatr. Res. 1996, 39, 889–894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Beek, A.H.; Claassen, J.A.; Rikkert, M.G.O.; Jansen, R.W. Cerebral Autoregulation: An Overview of Current Concepts and Methodology with Special Focus on the Elderly. J. Cereb. blood flow Metab. Off. J. Int. Soc. Cereb. Blood Flow Metab. 2008, 28, 1071–1085. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Assumptions | Criteria to Exclude a Segment | Reference |
|---|---|---|
| (I) The physiological high-pass filter characteristics of CA are observed in the VLF and LF range; (II) Reliable correction for serial time effects using the HF data (correction for TT and %BF) is performed [9]. | Correction for TT and %BF was not possible, i.e., no HF trend line was available. | [9], Box 1, Supplementary Figure S2, Supplementary Table S2 |
| A negative mean VLF and/or LF-phase shift of <−10° was present. | [8] | |
| Mean VLF and/or LF-phase shift values of >180° or <−180° (likely caused by persistence of ‘phase wrap around’) were present. | [8], Supplementary Table S2 | |
| <33% of the frequency bins in the VLF + LF or the HF-range had a coherence value above the significance threshold (meaning <6 bins available for the VLF + LF range and <10 bins for the HF range). | Figure S3 |
| Median (q1–q3) | Total (n = 54) | Survivors (n = 29) | Non-Survivors (n = 25) |
|---|---|---|---|
| Age (years) | 58 (43–72) | 49 (40–57) | 71 (59–77) |
| Sex, male, n (%) | 46 (85) | 22 (76) | 24 (96) |
| Admission diagnosis, primary neurological *, n (%) | 34 (63) | 15 (52) | 19 (76) |
| Admission APACHE IV score | 84 (51–111) | 65 (41–94) | 102 (72–120) |
| SOFA score (on day of measurement) | 9 (6–10) | 8 (6 -10) | 10 (7–11) |
| Length of ICU stay (days) | 12 (6–17) | 15 (6.2–20) | 8.4 (5.9–15) |
| Days on mechanical ventilation | 7.2 (2.9–12) | 8.5 (2.9–14) | 7.2 (3.6–11) |
| Mortality at ICU discharge, n (%) | 19 (34) | 0 | 19 (76) ‡ |
| GCS at ICU discharge †, n (%) | |||
| GCS score 3–5 | 1 (1.9) | 0 | 1 (4) |
| GCS score 6–8 | 1 (1.9) | 0 | 1 |
| GCS score 9–12 | 8 (15) | 7 (25) | 1 |
| GCS score 13–15 | 21 (39) | 19 (72) | 2 |
| GOSE at 6 months, n (%) | |||
| Favorable outcome, GOSE 5–8 | 25 (46) | 25 (86) | 0 |
| Unfavorable outcome, | 4 (7.4) | 4 (14) | 0 |
| GOSE 2–4 | |||
| Mortality GOSE 1 | 25 (46) | 0 | 25 (100) |
| Median (q1–q3) | Total (n = 54) | Survivors (n = 29) | Non-Survivors (n = 25) |
|---|---|---|---|
| Bilateral measurements, n (%) | 40 (74) | 19 (54) | 21 (84) |
| Start measurement after ICU admission (h) | 29 (16–77) | 44 (20–84) | 22 (13–45) |
| Duration bedside recording (min) | 77 (59–130) | 71 (68–59) | 79 (63–125) |
| Artifact free NIRS recording (min) * | 61 (47–121) | 54 (53–46) | 67 (48–122) |
| NIRS data removed † (%) | 9.5 (2–26) | 11 (2.9–27) | 8.8 (1.6–17) |
| Number of segments per patient * | 4 (2–7) | 4 (2–6) | 5 (2–7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tas, J.; Eleveld, N.; Borg, M.; Bos, K.D.J.; Langermans, A.P.; van Kuijk, S.M.J.; van der Horst, I.C.C.; Elting, J.W.J.; Aries, M.J.H. Cerebral Autoregulation Assessment Using the Near Infrared Spectroscopy ‘NIRS-Only’ High Frequency Methodology in Critically Ill Patients: A Prospective Cross-Sectional Study. Cells 2022, 11, 2254. https://doi.org/10.3390/cells11142254
Tas J, Eleveld N, Borg M, Bos KDJ, Langermans AP, van Kuijk SMJ, van der Horst ICC, Elting JWJ, Aries MJH. Cerebral Autoregulation Assessment Using the Near Infrared Spectroscopy ‘NIRS-Only’ High Frequency Methodology in Critically Ill Patients: A Prospective Cross-Sectional Study. Cells. 2022; 11(14):2254. https://doi.org/10.3390/cells11142254
Chicago/Turabian StyleTas, Jeanette, Nick Eleveld, Melisa Borg, Kirsten D. J. Bos, Anne P. Langermans, Sander M. J. van Kuijk, Iwan C. C. van der Horst, Jan Willem J. Elting, and Marcel J. H. Aries. 2022. "Cerebral Autoregulation Assessment Using the Near Infrared Spectroscopy ‘NIRS-Only’ High Frequency Methodology in Critically Ill Patients: A Prospective Cross-Sectional Study" Cells 11, no. 14: 2254. https://doi.org/10.3390/cells11142254