
Causes of Anemia in Polish Older Population—Results from the PolSenior Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Study Protocol
2.2. Definition, Causes, and Severity of Anemia
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Study Group and Morphometric Classification of Anemia
3.2. Etiology of Anemia in the Elderly Population
3.3. The Severity of Anemia in the Elderly Population
4. Discussion
4.1. Prevalence of Anemia
4.2. Criteria of Etiologic Classification of Anemia
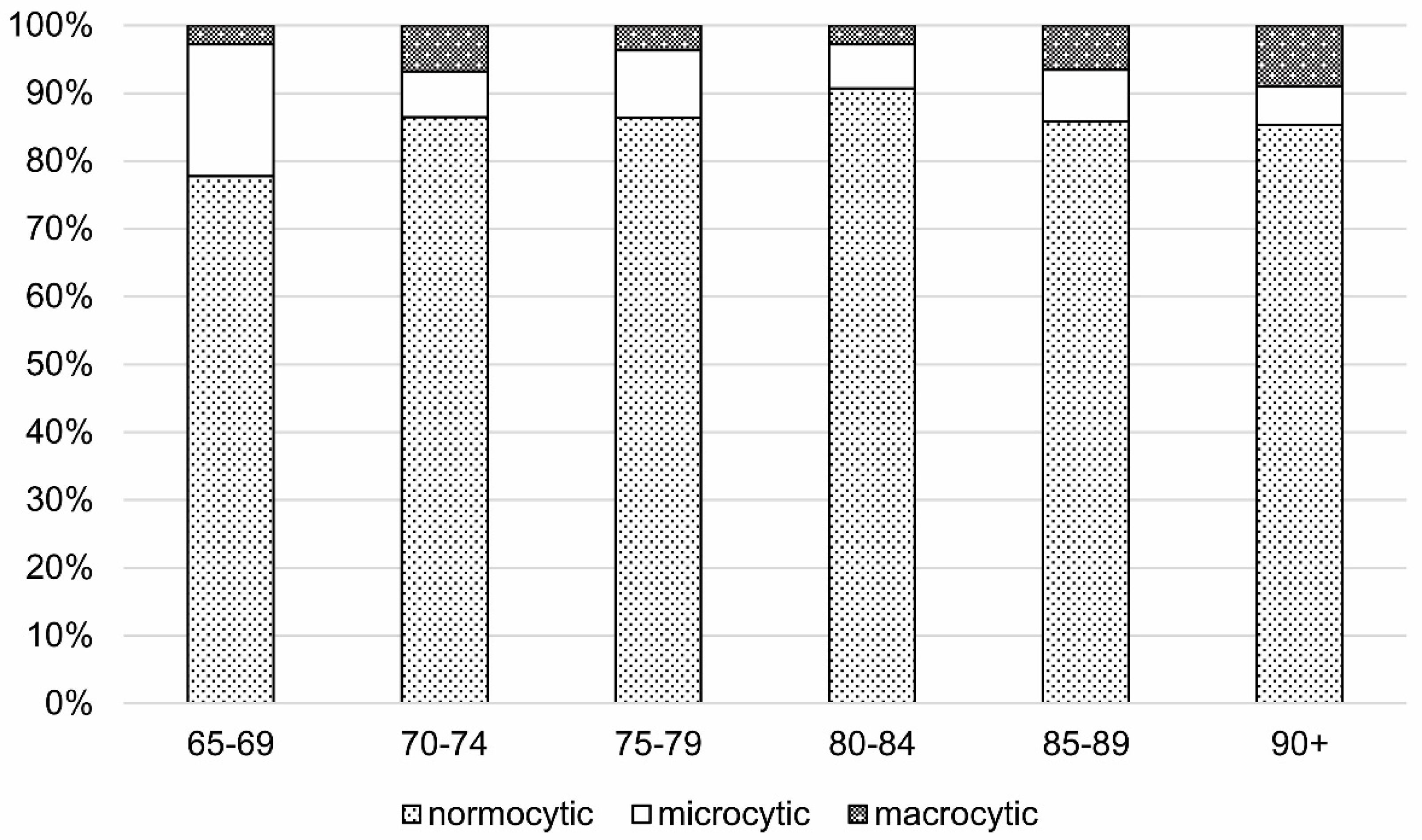
4.3. MCV and Etiologic Classification of Anemia
4.4. Anemia of Unknown Etiology
4.5. Severity of Anemia
4.6. Limitations
5. Conclusions
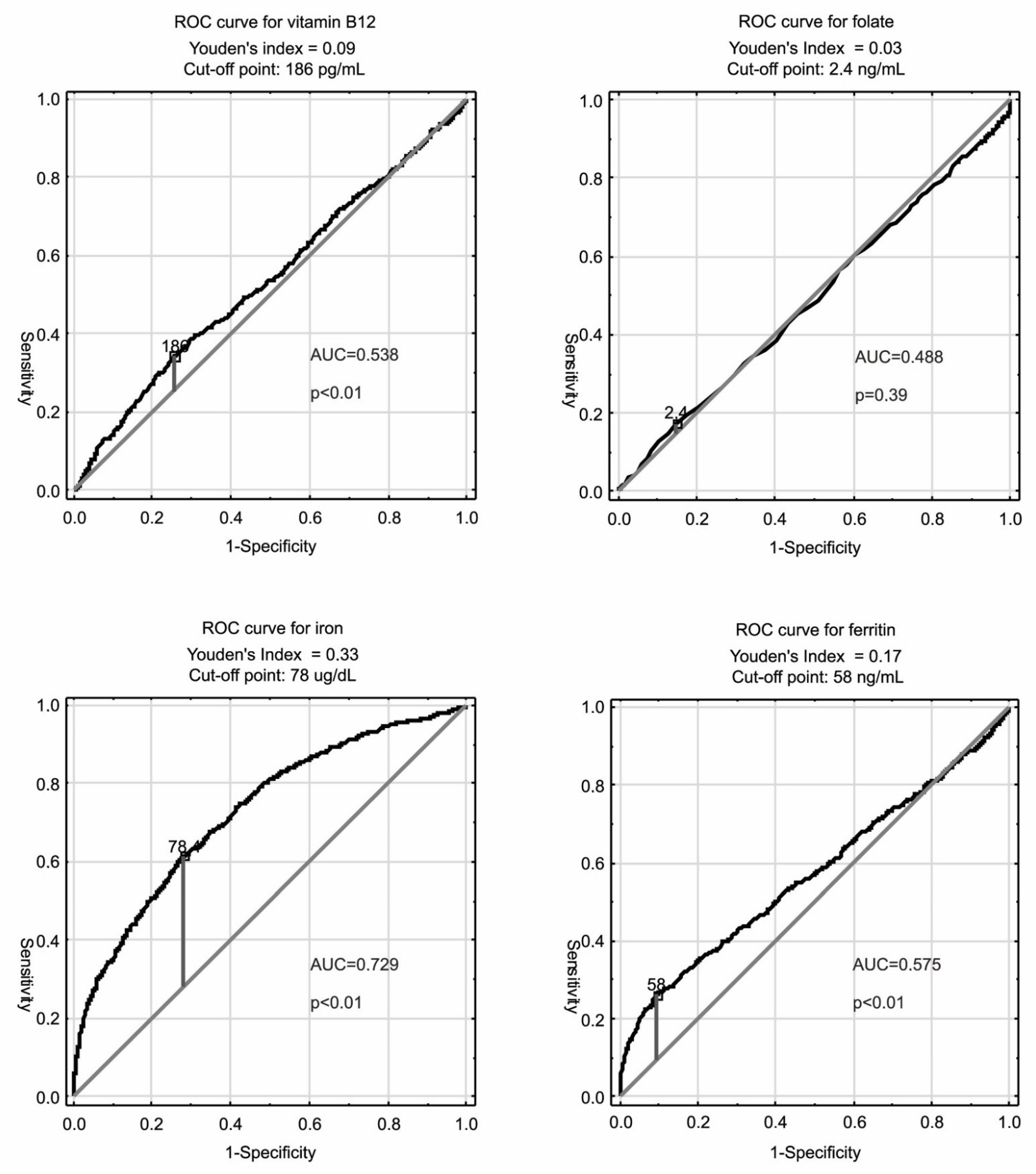
- In the etiological classification of anemia, it is necessary to adopt the age-specific criteria for the diagnosis of functional deficiency of nutrients such as iron, folates, and vitamin B12, because not every deficiency of these nutrients in older subjects may cause anemia.
- About half of the cases of anemia in old age are caused by nutritional deficiencies. Of the remaining causes, chronic kidney disease and chronic inflammation play a significant role. Every fifth case of anemia in old age has no clear explanation.
- MCV analyzed alone is of limited importance in the differential diagnosis of types of anemia in older adults, since most of the deficient anemia in the geriatric population remains normocytic. Therefore, it should be analyzed together with other red cell parameters, especially with RDW, which may increase the diagnostic possibilities of the morphological examination.
- In the older population with anemia, many subjects have a complex disease etiology resulting from the coexistence of deficiency and non-deficiency causes. Extensive laboratory analysis in old anemic patients may reveal many various combinations of etiologies of anemia and help to optimize the therapy.
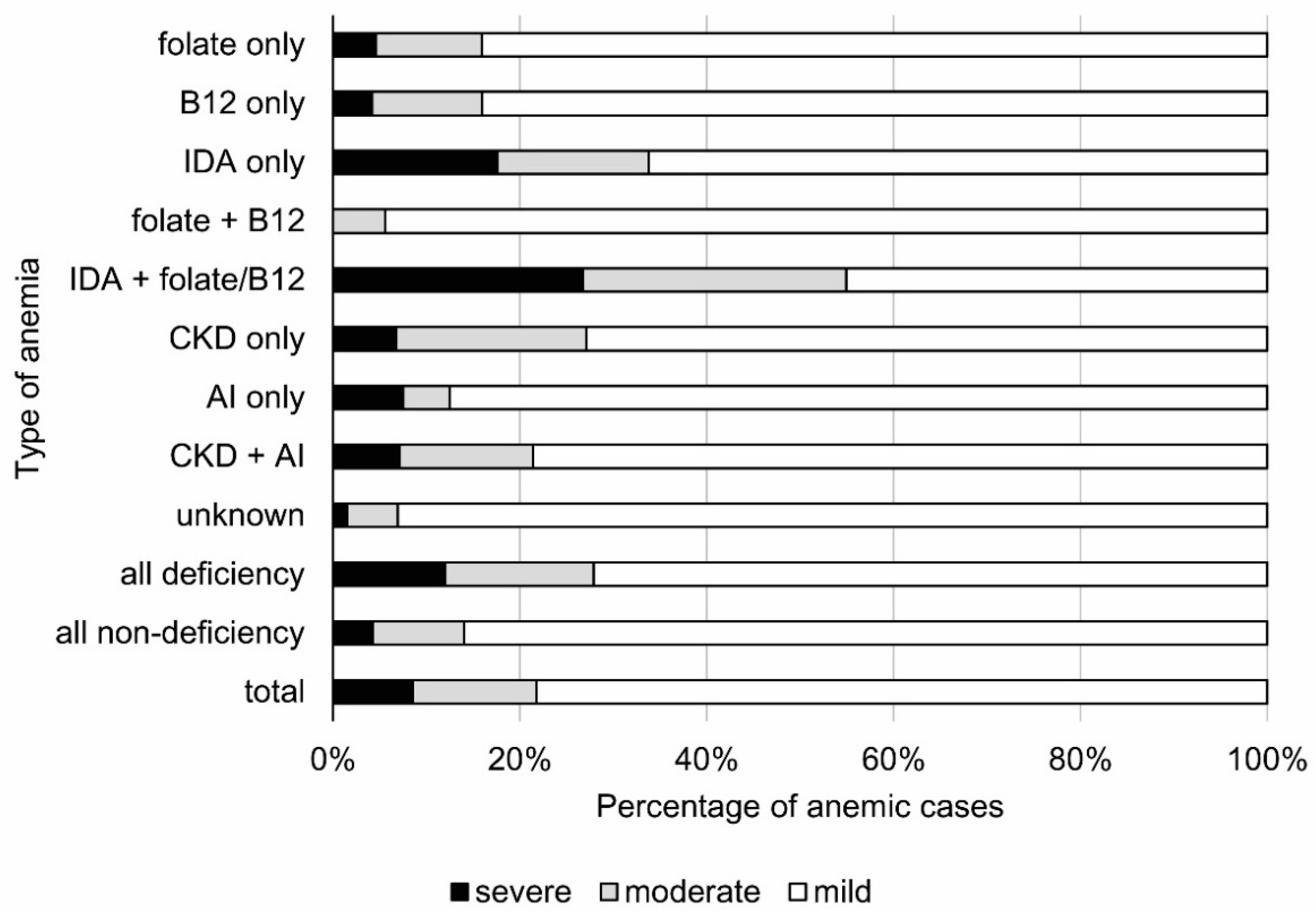
- Iron deficiency anemia is more severe than folate and vitamin B12 deficiency anemia. Severe anemia resulting from unexplained etiology is rare.
- Folic acid deficiency has little significance in the pathogenesis of anemia in old age.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations, Department of Economic and Social Affairs, Population Division. World Population Ageing 2019: Highlights (ST/ESA/SER.A/430); United Nations: New York, NY, USA, 2019. [Google Scholar]
- European Commission. The 2018 Ageing Report: Economic and Budgetary Projections for the EU Member States (2016–2070); European Commission: Brussels, Belgium, 2018. [Google Scholar]
- Penninx, B.W.; Pahor, M.; Woodman, R.C.; Guralnik, J.M. Anemia in old age is associated with increased mortality and hospitalization. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 74–79. [Google Scholar] [CrossRef] [Green Version]
- Penninx, B.W.; Pahor, M.; Cesari, M.; Corsi, A.M.; Woodman, R.C.; Bandinelli, S.; Guralnik, J.; Ferrucci, L. Anemia is associated with disability and decreased physical performance and muscle strength in the elderly. J. Am. Geriatr. Soc. 2004, 52, 719–724. [Google Scholar] [CrossRef] [PubMed]
- Penninx, B.W.; Pluijm, S.M.; Lips, P.; Woodman, R.; Miedema, K.; Guralnik, J.M.; Deeg, D.J. Late-life anemia is associated with increased risk of recurrent falls. J. Am. Geriatr. Soc. 2005, 53, 2106–2111. [Google Scholar] [CrossRef] [Green Version]
- Terekeci, H.M.; Kucukardali, Y.; Onem, Y.; Erikci, A.A.; Kucukardali, B.; Sahan, B.; Sayan, O.; Celik, S.; Gulec, M.; Sanisoglu, Y.S.; et al. Relationship between anemia and cognitive functions in elderly people. Eur. J. Intern. Med. 2010, 21, 87–90. [Google Scholar] [CrossRef] [PubMed]
- Putot, A.; Jeanmichel, M.; Chague, F.; Manckoundia, P.; Cottin, Y.; Zeller, M. Type 2 Myocardial Infarction: A Geriatric Population-based Model of Pathogenesis. Aging Dis. 2020, 11, 108–117. [Google Scholar] [CrossRef] [Green Version]
- Lanier, B.J.; Park, J.J.; Callahan, R.C. Anemia in Older Adults. Am. Fam. Physician 2018, 98, 437–442. [Google Scholar]
- Essama-Tjani, J.C.; Guilland, J.C.; Potier de Courcy, G.; Fuchs, F.; Richard, D. Folate status worsens in recently institutionalized elderly people without evidence of functional deterioration. J. Am. Coll. Nutr. 2000, 19, 392–404. [Google Scholar] [CrossRef] [PubMed]
- WHO. Serum and Red Blood Cell Folate Concentrations for Assessing Folate Status in Populations. Vitamin and Mineral Nutrition Information System. Geneva: World Health Organization. 2015. Available online: http://apps.who.int/iris/bitstream/10665/162114/1/WHO_NMH_NHD_EPG_15.01.pdf?ua=1 (accessed on 18 August 2021).
- WHO Department of Nutrition for Health and Development. Conclusions of a WHO Technical Consultation on folate and vitamin B12 deficiencies. Food Nutr. Bull. 2008, 29, 238–244. [Google Scholar] [CrossRef] [PubMed]
- WHO. Serum Ferritin Concentrations for the Assessment of Iron Status and Iron Deficiency in Populations. Vitamin and Mineral Nutrition Information System. Geneva, World Health Organization. 2008. (WHO/NMH/NHD/MNM/11.2). Available online: http://www.who.int/vmnis/indicators/serum_ferritin.pdf (accessed on 18 August 2021).
- WHO. Assessing the Iron Status of Populations: Report of a Joint World Health Organization/Centers for Disease Control and Prevention Technical Consultation on the Assessment of Iron Status at the Population Level, Geneva, Switzerland, 6–8 April 2004; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Ryden, I.; Lind, L.; Larsson, A. Reference values of thirty-one frequently used laboratory markers for 75-year-old males and females. Ups. J. Med. Sci. 2012, 117, 264–272. [Google Scholar] [CrossRef]
- Carlsson, L.; Lind, L.; Larsson, A. Reference Values for 27 Clinical Chemistry Tests in 70-Year-Old Males and Females. Gerontology 2010, 56, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Zweig, M.H.; Campbell, G. Receiver-operating characteristic (ROC) plots: A fundamental evaluation tool in clinical medicine. Clin. Chem. 1993, 39, 561–577. [Google Scholar] [CrossRef]
- Bledowski, P.; Mossakowska, M.; Chudek, J.; Grodzicki, T.; Milewicz, A.; Szybalska, A.; Wieczorowska-Tobis, K.; Wiecek, A.; Bartoszek, A.; Dabrowski, A.; et al. Medical, psychological and socioeconomic aspects of aging in Poland. Assumptions and objectives of the PolSenior project. Exp. Gerontol. 2011, 46, 1003–1009. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Coresh, J.; Greene, T.; Stevens, L.A.; Zhang, Y.L.; Hendriksen, S.; Kusek, J.W.; Lente, F.V. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann. Intern. Med. 2006, 145, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Delenaye, P.; Jager, K.J.; Boekenkamp, A.; Christensson, A.; Dubourg, L.; Eriksen, B.O.; Gaillard, F.; Gambaro, G.; Giet, M.D.; Glassock, R.J.; et al. CKD: A call for an age-adapted definition. J. Am. Soc. Nephrol. 2019, 30, 1785–1805. [Google Scholar] [CrossRef]
- WHO. Nutritional Anemia; Report of a WHO Scientific Group: Geneva, Switzerland, 1968. [Google Scholar]
- Weiss, G.; Ganz, T.; Goodnough, L.T. Anemia of inflammation. Blood 2019, 133, 40–50. [Google Scholar] [CrossRef] [Green Version]
- Linden, A. Measuring Diagnostic and Predictive Accuracy in Disease Management: An Introduction to Receiver Operating Characteristic (ROC) Analysis. J. Eval. Clin. Pract. 2006, 12, 132–139. [Google Scholar] [CrossRef]
- Guralnik, J.M.; Eisenstaedt, R.S.; Ferrucci, L.; Klein, H.G.; Woodman, R.C. Prevalence of anemia in persons 65 years and older in the United States: Evidence for a high rate of unexplained anemia. Blood 2004, 104, 2263–2268. [Google Scholar] [CrossRef] [Green Version]
- Pan, M.L.; Chen, L.R.; Tsao, H.M.; Chen, K.H. Iron Deficiency Anemia as a Risk Factor for Osteoporosis in Taiwan: A Nationwide Population-Based Study. Nutrients 2017, 9, 616. [Google Scholar] [CrossRef]
- Levi, M.; Simonetti, M.; Marconi, E.; Brignoli, O.; Cancian, M.; Masotti, A.; Pegoraro, V.; Heiman, F.; Cricelli, C. Francesco Lapi Gender differences in determinants of iron-deficiency anemia: A population-based study conducted in four European countries. Ann. Hematol. 2019, 98, 1573–1582. [Google Scholar] [CrossRef] [PubMed]
- Imai, E.; Nakade, M. Fish and meat intakes and prevalence of anemia among the Japanese elderly. Asia Pac. J. Clin. Nutr. 2019, 28, 276–284. [Google Scholar]
- Tettamanti, M.; Lucca, U.; Gandini, F.; Recchia, A.; Mosconi, P.; Apolone, G.; Nobili, A.; Tallone, M.V.; Detoma, P.; Giacomin, A.; et al. Prevalence, incidence and types of mild anemia in the elderly: The “Health and Anemia” population-based study. Haematologica 2010, 95, 1849–1856. [Google Scholar] [CrossRef] [Green Version]
- Styszyński, A.; Mossakowska, M.; Chudek, J.; Puzianowska-Kuźnicka, M.; Klich-Rączka, A.; Neumann-Podczaska, A.; Szybalska, A.; Wieczorowska-Tobis, K. Prevalence of anemia in relation to socio-economic factors in elderly Polish population: The results of PolSenior study. J. Physiol. Pharm. 2018, 69, 75–81. [Google Scholar]
- Wieczorowska-Tobis, K.; Niemir, Z.; Mossakowska, M.; Klich-Raczka, A.; Zyczkowska, J. Anemia in centenarians. J. Am. Geriatr. Soc. 2002, 50, 1311–1313. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, T.; Kitagawa, M.; Hirokawa, K. Age-related changes of human bone marrow: A histometric estimation of proliferative cells, apoptotic cells, T cells, B cells and macrophages. Mech. Ageing Dev. 2000, 117, 57–68. [Google Scholar] [CrossRef]
- Ferrucci, L.; Maggio, M.; Bandinelli, S.; Basaria, S.; Lauretani, F.; Ble, A.; Valenti, G.; Ershler, W.B.; Guralnik, J.M.; Longo, D.L. Low testosterone levels and the risk of anemia in older men and women. Arch. Intern. Med. 2006, 166, 1380–1388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jernigan, J.A.; Gudat, J.C.; Blake, J.L.; Bowen, L.; Lezotte, D.C. Reference values for blood findings in relatively fit elderly persons. J. Am. Geriatr. Soc. 1980, 28, 308–314. [Google Scholar] [CrossRef]
- Culleton, B.F.; Manns, B.J.; Zhang, J.; Tonelli, M.; Klarenbach, S.; Hemmelgarn, B.R. Impact of anemia on hospitalization and mortality in older adults. Blood 2006, 107, 3841–3846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Izaks, G.J.; Westendorp, R.G.; Knook, D.L. The definition of anemia in older persons. JAMA 1999, 281, 1714–1717. [Google Scholar] [CrossRef] [Green Version]
- Budd, M.; Naugler, C. Folate deficiency in an unselected population in Calgary, Alberta and its relationship with red blood cell macrocytosis. BMC Res. Notes 2015, 8, 314. [Google Scholar] [CrossRef] [Green Version]
- Schop, A.; Stouten, K.; Riedl, J.A.; van Houten, R.J.; Leening, M.J.G.; van Rosmalen, J.V.; Bindels, P.J.E.; Levin, M.-D. A new diagnostic work-up for defining anemia etiologies: A cohort study in patients ≥ 50 years in general practices. BMC Fam. Pract. 2020, 21, 167. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.J.; Kim, M.H.; Kim, A.S.; Chang, J.S. Age-related Deterioration of Hematopoietic Stem Cells. Int. J. Stem. Cells 2008, 1, 55–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joosten, E.; Pelemans, W.; Hiele, M.; Noyen, J.; Verhaeghe, R.; Boogaerts, M.A. Prevalence and causes of anaemia in a geriatric hospitalized population. Gerontology 1992, 38, 111–117. [Google Scholar] [CrossRef]
- Artz, A.S.; Fergusson, D.; Drinka, P.J.; Gerald, M.; Bidenbender, R.; Lechich, A.; Silverstone, F.; McCamish, M.A.; Dai, J.; Keller, E.; et al. Mechanisms of unexplained anemia in the nursing home. J. Am. Geriatr. Soc. 2004, 52, 423–427. [Google Scholar] [CrossRef] [PubMed]
- Bonadies, N.; Rovó, A.; Porret, N.; Bacher, U. When should we think of myelodysplasia or bone marrow failure in a thrombocytopenic patient? A practical approach to diagnosis. J. Clin. Med. 2021, 10, 1026. [Google Scholar] [CrossRef] [PubMed]
- Ma, X. Epidemiology of myelodysplastic syndromes. Am. J. Med. 2012, 125, 2–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makipour, S.; Kanapuru, B.; Ershler, W.B. Unexplained Anemia in the Elderly. Semin. Hematol. 2008, 45, 250–254. [Google Scholar] [CrossRef] [Green Version]
- Mast, A.E.; Blinder, M.A.; Gronowski, A.M.; Chumley, C.; Scott, M.G. Clinical utility of the soluble transferrin receptor and comparison with serum ferritin in several populations. Clin. Chem. 1998, 44, 45–51. [Google Scholar] [CrossRef] [Green Version]
- Beletić, A.; Mirković, D.; Dudvarski-Ilić, A.; Milenković, B.; Nagorni-Obradović, L.; Đorđević, V.; Ignjatović, S.; Singh, N.M. Questionable reliability of homocysteine as the metabolic marker for folate and vitamin B12 deficiency in patients with chronic obstructive pulmonary disease. J. Med. Biochem. 2015, 34, 467–472. [Google Scholar] [CrossRef] [Green Version]
- Girelli, D.; Nemeth, E.; Swinkels, D.W. Hepcidin in the diagnosis of iron disorders. Blood 2016, 127, 2809–2813. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Cohorts | Females | Males | ||
|---|---|---|---|---|
| Anemic | Non-Anemic | Anemic | Non-Anemic | |
| Age [years] | 83.0 ± 8.8 a | 77.6 ± 8.4 | 84.2 ± 7.8 a | 77.6 ± 8.1 |
| 65–69 years [% (n)] | 5.9 (18) | 94.1 (289) | 4.4 (13) | 95.6 (281) |
| 70–74 years [% (n)] | 7.8 (26) | 92.2 (309) | 11.8 (41) b | 88.2 (306) |
| 75–79 years [% (n)] | 9.9 (28) | 90.1 (254) | 14.0 (45) b | 86.0 (276) |
| 80–84 years [% (n)] | 12.3 (30) | 87.7 (213) | 21.6 (63) b | 78.4 (228) |
| 85–89 years [% (n)] | 17.4 (42) | 82.6 (200) | 32.0 (105) b | 68.0 (223) |
| 90 and over [% (n)] | 29.1 (65) | 70.9 (158) | 44.8 (107) b | 55.2 (132) |
| Total [% (n)] | 12.8 (209) | 87.2 (1423) | 20.5 (374) b | 79.5 (1446) |
| Comorbidity | ||||
| Gastrointestinal ulcer [% (n)] | 8.6 (16) | 8.5 (112) | 12.4 (41) | 10.8 (148) b |
| Parkinson’s disease [% (n)] | 2.7 (5) a | 1.6 (21) | 2.4 (8) | 3.1 (42) |
| Past stroke [% (n)] | 12.3 (23) a | 5.3 (70) | 9.4 (31) | 7.5 (103) |
| Dementia [% (n)] | 48.3 (101) a | 31.5 (448) | 37.4 (140) ab | 23.3 (337) |
| Obesity [% (n)] | 28.2 (59) a | 38.9 (554) | 15.2 (57) ab | 26.8 (388) b |
| Visceral obesity [% (n)] | 75.6 (158) a | 84.3 (1200) | 58.0 (217) ab | 72.4 (1047) b |
| Underweight [% (n)] | 1.0 (2) | 0.7 (10) | 1.6 (6) | 1.4 (20) |
| History of cancer [% (n)] | 4.8 (10) | 5.1 (72) | 6.5 (24) | 4.3 (62) |
| Chronic pain [% (n)] | 58.3 (109) a | 47.2 (626) | 39.7 (131) b | 36.3 (498) b |
| Chronic hepatitis [% (n)] | 4.8 (10) | 2.7 (38) | 3.2 (12) | 3.2 (46) |
| Chronic kidney disease [% (n)] | 33.0 (69) a | 14.1 (200) | 31.6 (118) a | 8.4 (122) b |
| Thyrotoxicosis [% (n)] | 4.8 (10) | 3.2 (45) | 2.7 (10) | 1.7 (24) b |
| Hypothyroidism [% (n)] | 7.7 (16) | 9.3 (133) | 5.6 (21) | 5.0 (72) b |
| Parameters | ||||
| White blood cells [103/µL] | 6.08 ± 1.68 a | 6.39 ± 2.07 | 6.6 ± 3.2 b | 6.7 ± 1.9 b |
| Red blood cells [106/µL] | 3.83 ± 0.41 a | 4.54 ± 0.40 | 4.0 ± 0.4 ab | 4.8 ± 0.4 b |
| Hemoglobin [g/dL] | 11.0 ± 1.2 a | 13.6 ± 1.0 | 11.8 ± 1.1 ab | 14.6 ± 1.0 b |
| Hematocrit [%] | 33.5 ± 3.5 a | 40.7 ± 3.2 | 35.7 ± 3.4 ab | 43.3 ± 3.4 b |
| MCV [fL] | 87.9 ± 8.6 a | 89.6 ± 5.6 | 90.5 ± 7.7 b | 91.0 ± 5.4 b |
| MCH [pg] | 28.8 ± 3.4 a | 30.0 ± 1.9 | 30.1 ± 3.0 ab | 30.8 ± 1.9 b |
| MCHC [g/dL] | 32.4 ± 3.2 a | 33.2 ± 2.3 | 32.9 ± 2.7 a | 33.5 ± 2.1 b |
| Platelets [103/µL] | 250 ± 93 a | 230 ± 68 | 219 ± 81 ab | 208 ± 73 b |
| Serum creatinine [mg/dL] | 1.03 ± 0.49 a | 0.85 ± 0.24 | 1.2 ± 0.6 ab | 1.0 ± 0.3 b |
| Serum iron [µg/dL] | 66.8 ± 28.2 a | 91.2 ± 29.1 | 74.8 ± 32.1 ab | 103.7 ± 32.7 b |
| Serum folate [ng/mL] | 6.5 ± 9.0 a | 5.0 ± 4.2 | 5.3 ± 6.2 a | 4.4 ± 3.7 b |
| Serum vitamin B12 [pg/mL] | 289 ± 249 | 304 ± 250 | 288 ± 282 | 287 ± 183 b |
| Serum ferritin [ng/mL] | 164 ± 199 a | 171 ± 129 | 227 ± 251 ab | 260 ± 216 b |
| eGFR-MDRD [mL/min/1.73 m2] | 55.2 ± 20.5 a | 64.5 ± 17.0 | 58.3 ± 20.7 a | 70.2 ± 17.3 b |
| ACR [mg/g] | 136 ± 701 a | 33 ± 161 | 120 ± 461 a | 39 ± 209 |
| Method | WHO | Lowest 2.5 Percentile | ROC | |||
|---|---|---|---|---|---|---|
| Type of Anemia (Parameter [Unit]) | Cut-Offs | % (n) | Cut-Offs | % (n) | Cut-Offs | % (n) |
| Anemia with Nutritional Deficiency | ||||||
| Iron only (serum ferritin [µg/L]) | <15 | 0.9 (5) | <25 | 9.1 (53) | <58 | 12.7 (74) |
| Folate only (serum folate [ng/mL]) | <3 | 18.4 (107) | <1.6 | 2.2 (13) | <2.4 | 7.5 (44) |
| B12 only (serum B12 [pg/mL]) | <200 | 26.9 (157) | <75 | 5.0 (29) | <186 | 20.4 (119) |
| Folate and B12 | see above | 9.4 (55) | see above | 0.0 (0) | see above | 3.1 (18) |
| Iron and folate or B12 or both | see above | 2.4 (14) | see above | 0.2 (1) | see above | 12.2 (71) |
| All deficiency anemias | see above | 58.0 (338) | see above | 16.5 (96) | see above | 55.9 (326) |
| Anemia without Nutritional Deficiency | ||||||
| CKD only (eGFR < 45 mL/min/1.73 m2 or ACR > 300 mg/g) | see in 1st column | 8.9 (52) | see in 1st column | 26.1 (152) | see in 1st column | 10.1 (59) |
| AI only (serum iron [µg/dL]; serum ferritin [µg/L]) | <60; ≥15 | 8.7 (51) | <35.1; ≥25 | 2.6 (15) | <78; ≥58 | 6.9 (40) |
| CKD/AI | see above | 4.8 (28) | see above | 3.3 (19) | see above | 4.8 (28) |
| Unknown | - | 19.6 (114) | - | 51.6 (301) | - | 22.3 (130) |
| All non-deficiency anemias | see above | 42.0 (245) | see above | 83.5 (487) | see above | 44.1 (257) |
| Total | - | 100 (583) | - | 100 (583) | - | 100 (583) |
| Type of Anemia | Normocytic % (n) | Microcytic % (n) | Macrocytic % (n) |
|---|---|---|---|
| Anemia with Nutritional Deficiency | |||
| Folate only | 7.8 (40) | 4.9 (2) | 6.5 (2) |
| B12 only | 20.4 (104) | 2.4 (1) a | 45.2 (14) a |
| IDA only | 11.4 (58) a | 39.0 (16) a | 0.0 (0) |
| Folate + B12 | 3.3 (17) | 0.0 (0) | 3.2 (1) |
| IDA + folate/B12 | 10.6 (54) a | 36.6 (15) a | 6.5 (2) |
| All deficiency anemias | 53.4 (273) a | 82.9 (34) a | 61.3 (19) |
| Anemia without Nutritional Deficiency | |||
| CKD only | 10.8 (55) | 2.4 (1) | 9.7 (3) |
| AI | 7.8 (40) a | 0.0 (0) | 0.0 (0) |
| CKD + AI | 4.9 (25) | 2.4 (1) | 6.5 (2) |
| Unknown | 23.1 (118) | 12.2 (5) | 22.6 (7) |
| All non-deficiency anemias | 46.6 (238) a | 17.1 (7) a | 38.7 (12) |
| Total | 100.0 (511) | 100.0 (41) | 100.0 (31) |
| Deficiency Anemia | Coexisting Non-Deficiency Cause % (n) | Deficiency Cause(s) Only % (n) |
|---|---|---|
| Normocytic a | 88.6 (117) | 80.4 (156) |
| Microcytic | 6.8 (9) | 12.9 (25) |
| Macrocytic | 4.5 (6) | 6.7 (13) |
| Folate only a | 63.6 (28) | 36.4 (16) |
| Vitamin B12 only a | 48.7 (58) | 51.3 (61) |
| IDA only | 32.4 (24) | 67.6 (50) |
| Folate + B12 | 44.4 (8) | 55.6 (10) |
| IDA + folate/B12 a | 19.7 (14) | 80.3 (57) |
| All deficiency anemias | 40.5 (132) | 59.5 (194) |
| Severe Anemia % (n) | Moderate Anemia % (n) | Mild Anemia % (n) | |
|---|---|---|---|
| Gender | |||
| Males a | 52.0 (26) | 44.2 (34) | 68.9 (314) |
| Females | 48.0 (24) | 55.8 (43) | 31.1 (142) |
| Age Cohorts | |||
| 65–69 | 10.0 (5) | 2.6 (2) | 5.3 (24) |
| 70–74 | 8.0 (4) | 6.5 (5) | 12.7 (58) |
| 75–79 | 10.0 (5) | 18.2 (14) | 11.8 (54) |
| 80–84 a | 6.0 (3) | 13.0 (10) | 17.5 (80) |
| 85–89 | 30.0 (15) | 26.0 (20) | 24.6 (112) |
| 90+ | 36.0 (18) | 33.8 (26) | 28.1 (128) |
| MCV | |||
| Normocytosis a | 58.0 (29) | 76.6 (59) | 92.8 (423) |
| Microcytosis a | 38.0 (19) | 13.0 (10) | 2.6 (12) |
| Macrocytosis | 4.0 (2) | 10.4 (8) | 4.6 (21) |
| Type of Anemia (Classified According to ROC Curve Analysis) | |||
| Anemia with Nutritional Deficiency | |||
| Folate only | 4.0 (2) | 6.5 (5) | 8.1 (37) |
| B12 only | 10.0 (5) | 18.2 (14) | 21.9 (100) |
| IDA only a | 26.0 (13) | 15.6 (12) | 10.7 (49) |
| Folate + B12 | 0.0 (0) | 1.3 (1) | 3.7 (17) |
| IDA + folate/B12 a | 38.0 (19) | 26.0 (20) | 7.0 (32) |
| All deficiency a | 78.0 (39) | 67.5 (52) | 51.5 (235) |
| Anemia without Nutritional Deficiency | |||
| CKD only | 12.6 (16) | 15.6 (12) | 9.4 (43) |
| AI | 3.9 (5) | 2.6 (2) | 7.7 (35) |
| CKD + AI | 4.7 (6) | 5.2 (4) | 4.8 (22) |
| Unknown a | 7.1 (9) | 9.1 (7) | 26.5 (121) |
| All non-deficiency a | 28.3 (36) | 32.5 (25) | 48.5 (221) |
| Total | 100.0 (50) | 100.0 (77) | 100.0 (456) |
| Study | Iron Deficiency | Vitamin B12 Deficiency | Folate Deficiency | Anemia of Inflammation |
|---|---|---|---|---|
| NHANES III | 2 or 3 of following:
| serum B12 < 200 pg/mL | RBC folate 102.6 ng/dL or serum folate 2.6 ng/mL | serum iron < 60 μg/dL without evidence of iron deficiency |
| Health and Anemia |
| serum B12 < 200 pg/mL and MCV > 95 fL | serum folate < 3.0 pg/mL and MCV > 95 fL |
|
| PolSenior (WHO criteria) | serum ferritin < 15 ng/mL | serum B12 < 200 pg/mL | serum folate < 3.0 pg/mL | serum iron < 60 μg/dL and sF ≥ 15 ng/mL |
| PolSenior (lowest 2.5 percentile) | serum ferritin < 25 ng/mL | serum B12 < 75 pg/mL | serum B12 < 1.6 pg/mL | serum iron < 35.1 μg/dL and sF ≥ 25 ng/mL |
| PolSenior (ROC analysis) | serum ferritin < 58 ng/mL | serum B12 < 186 pg/mL | serum B12 < 2.4 pg/mL | serum iron < 78 μg/dL and serum ferritin ≥ 78 ng/mL |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Styszyński, A.; Chudek, J.; Mossakowska, M.; Lewandowski, K.; Puzianowska-Kuźnicka, M.; Klich-Rączka, A.; Więcek, A.; Wieczorowska-Tobis, K. Causes of Anemia in Polish Older Population—Results from the PolSenior Study. Cells 2021, 10, 2167. https://doi.org/10.3390/cells10082167
Styszyński A, Chudek J, Mossakowska M, Lewandowski K, Puzianowska-Kuźnicka M, Klich-Rączka A, Więcek A, Wieczorowska-Tobis K. Causes of Anemia in Polish Older Population—Results from the PolSenior Study. Cells. 2021; 10(8):2167. https://doi.org/10.3390/cells10082167
Chicago/Turabian StyleStyszyński, Arkadiusz, Jerzy Chudek, Małgorzata Mossakowska, Krzysztof Lewandowski, Monika Puzianowska-Kuźnicka, Alicja Klich-Rączka, Andrzej Więcek, and Katarzyna Wieczorowska-Tobis. 2021. "Causes of Anemia in Polish Older Population—Results from the PolSenior Study" Cells 10, no. 8: 2167. https://doi.org/10.3390/cells10082167