
Effects of Genotypes and Treatment on Oxygenscan Parameters in Sickle Cell Disease

 ,
,  , , , add
Show full author list
, , , add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Hematological and Oxygenscan Parameters
2.3. Statistics
3. Results
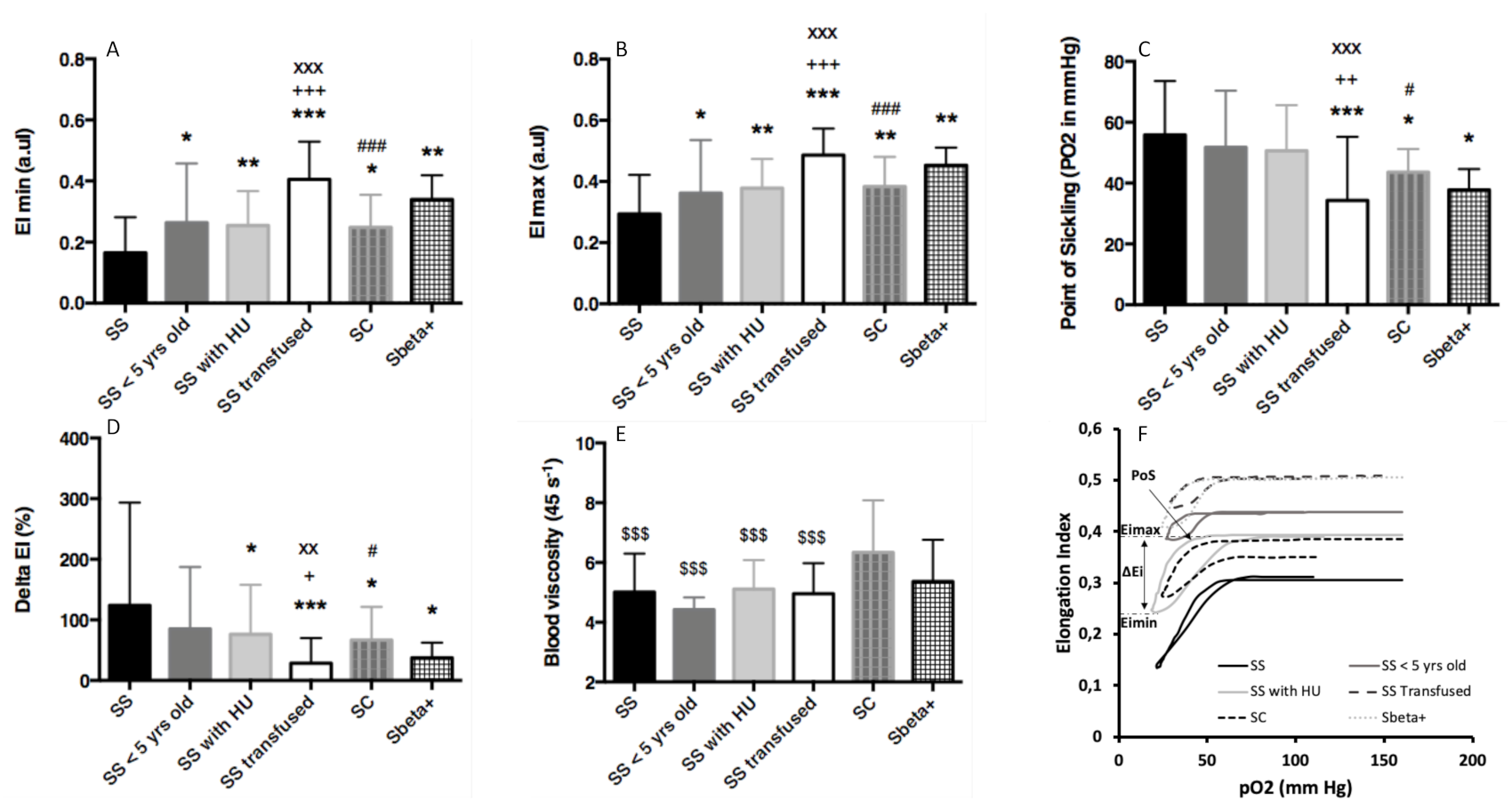
3.1. Comparisons between Groups
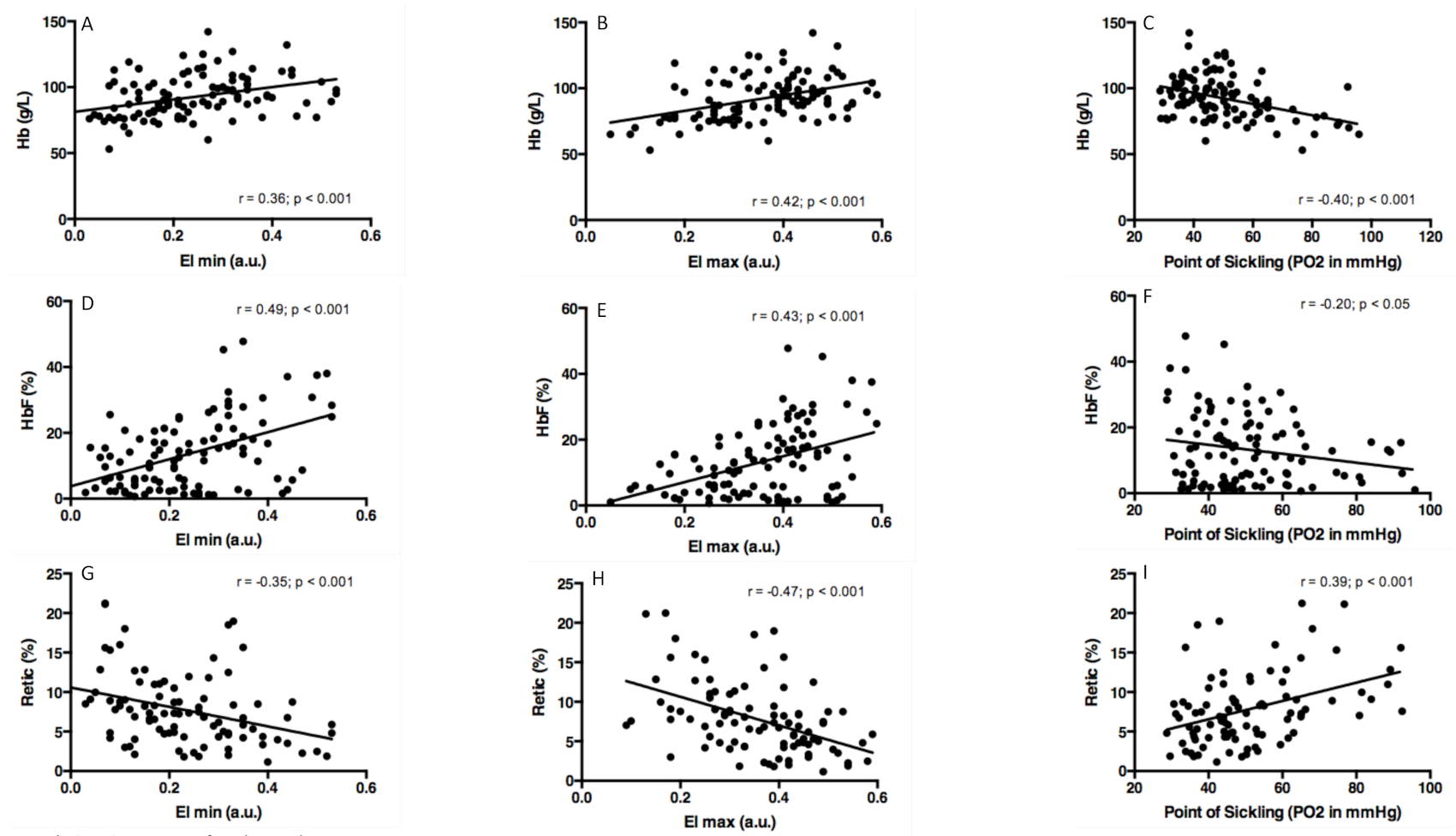
3.2. Associations between Oxygenscan and Hematological Parameters
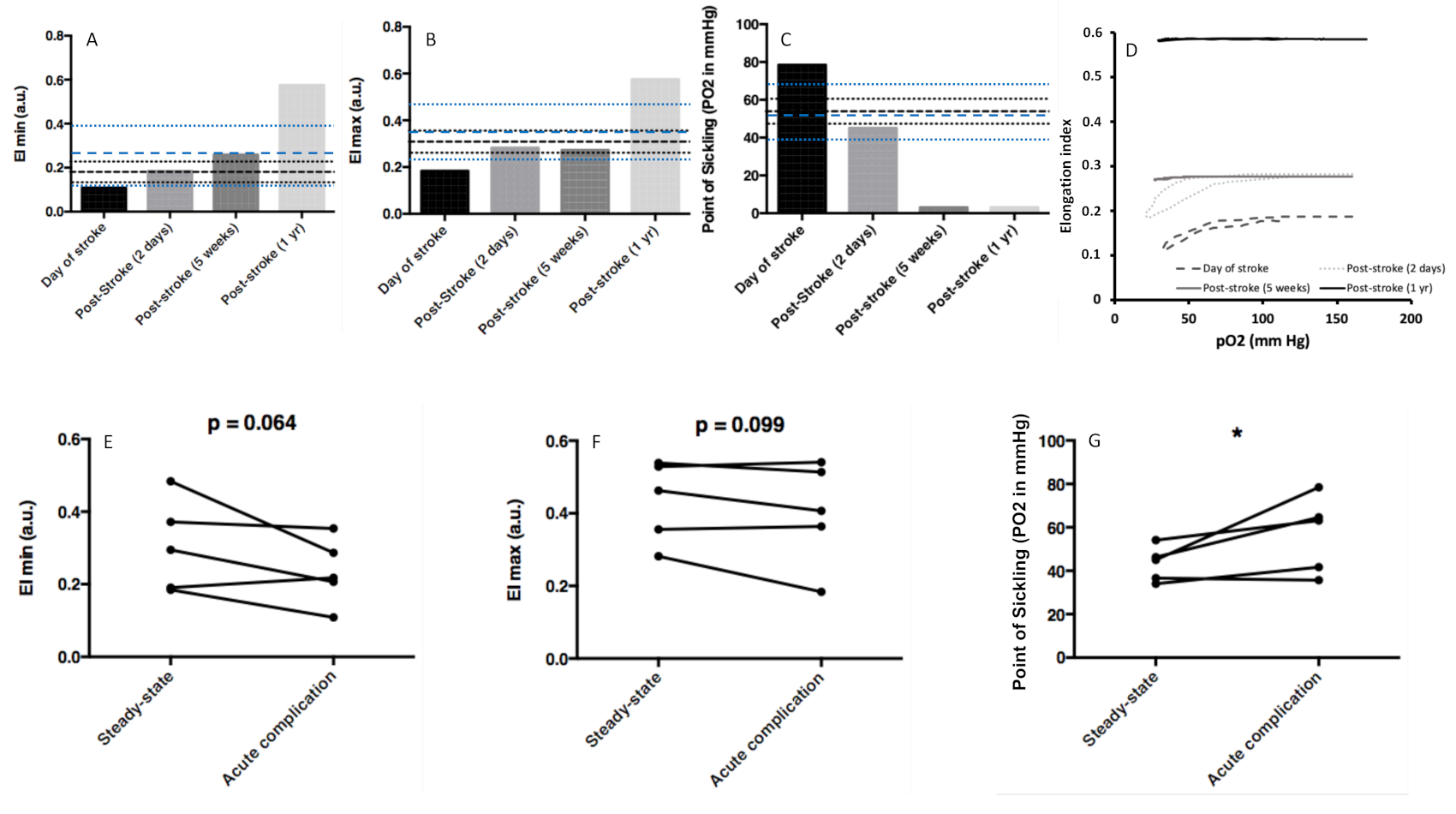
3.3. Oxygenscan Parameters and Acute Complication in SS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Serjeant, G.R. The natural history of sickle cell disease. Cold Spring Harb. Perspect. Med. 2013, 3, a011783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pauling, L.; Itano, H.A.; Singer, S.J.; Wells, I.C. Sickle cell anemia a molecular disease. Science 1949, 110, 543–548. [Google Scholar] [CrossRef] [PubMed]
- Feeling-Taylor, A.R.; Yau, S.T.; Petsev, D.N.; Nagel, R.L.; Hirsch, R.E.; Vekilov, P.G. Crystallization mechanisms of hemoglobin C in the R state. Biophys. J. 2004, 87, 2621–2629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagel, R.L.; Lawrence, C. The distinct pathobiology of sickle cell-hemoglobin C disease. Therapeutic implications. Hematol. Oncol. Clin. N. Am. 1991, 5, 433–451. [Google Scholar]
- Lemonne, N.; Lamarre, Y.; Romana, M.; Hardy-Dessources, M.D.; Lionnet, F.; Waltz, X.; Tarer, V.; Mougenel, D.; Tressieres, B.; Lalanne-Mistrih, M.L.; et al. Impaired blood rheology plays a role in the chronic disorders associated with sickle cell-hemoglobin C disease. Haematologica 2014, 99, 74–75. [Google Scholar] [CrossRef] [Green Version]
- Lionnet, F.; Hammoudi, N.; Stojanovic, K.S.; Avellino, V.; Grateau, G.; Girot, R.; Haymann, J.P. Hemoglobin sickle cell disease complications: A clinical study of 179 cases. Haematologica 2012, 97, 1136–1141. [Google Scholar] [CrossRef]
- Renoux, C.; Romana, M.; Joly, P.; Ferdinand, S.; Faes, C.; Lemonne, N.; Skinner, S.; Garnier, N.; Etienne-Julan, M.; Bertrand, Y.; et al. Effect of Age on Blood Rheology in Sickle Cell Anaemia and Sickle Cell Haemoglobin C Disease: A Cross-Sectional Study. PLoS ONE 2016, 11, e0158182. [Google Scholar] [CrossRef]
- Tripette, J.; Alexy, T.; Hardy-Dessources, M.D.; Mougenel, D.; Beltan, E.; Chalabi, T.; Chout, R.; Etienne-Julan, M.; Hue, O.; Meiselman, H.J.; et al. Red blood cell aggregation, aggregate strength and oxygen transport potential of blood are abnormal in both homozygous sickle cell anemia and sickle-hemoglobin C disease. Haematologica 2009, 94, 1060–1065. [Google Scholar] [CrossRef]
- Cita, K.C.; Brureau, L.; Lemonne, N.; Billaud, M.; Connes, P.; Ferdinand, S.; Tressieres, B.; Tarer, V.; Etienne-Julan, M.; Blanchet, P.; et al. Men with Sickle Cell Anemia and Priapism Exhibit Increased Hemolytic Rate, Decreased Red Blood Cell Deformability and Increased Red Blood Cell Aggregate Strength. PLoS ONE 2016, 11, e0154866. [Google Scholar] [CrossRef] [Green Version]
- Connes, P.; Lamarre, Y.; Hardy-Dessources, M.D.; Lemonne, N.; Waltz, X.; Mougenel, D.; Mukisi-Mukaza, M.; Lalanne-Mistrih, M.L.; Tarer, V.; Tressieres, B.; et al. Decreased hematocrit-to-viscosity ratio and increased lactate dehydrogenase level in patients with sickle cell anemia and recurrent leg ulcers. PLoS ONE 2013, 8, e79680. [Google Scholar] [CrossRef]
- Lamarre, Y.; Romana, M.; Lemonne, N.; Hardy-Dessources, M.D.; Tarer, V.; Mougenel, D.; Waltz, X.; Tressieres, B.; Lalanne-Mistrih, M.L.; Etienne-Julan, M.; et al. Alpha thalassemia protects sickle cell anemia patients from macro-albuminuria through its effects on red blood cell rheological properties. Clin. Hemorheol. Microcirc. 2014, 57, 63–72. [Google Scholar] [CrossRef]
- Lemaire, C.; Lamarre, Y.; Lemonne, N.; Waltz, X.; Chahed, S.; Cabot, F.; Botez, I.; Tressieres, B.; Lalanne-Mistrih, M.L.; Etienne-Julan, M.; et al. Severe proliferative retinopathy is associated with blood hyperviscosity in sickle cell hemoglobin-C disease but not in sickle cell anemia. Clin. Hemorheol. Microcirc. 2013, 55, 205–212. [Google Scholar] [CrossRef]
- Ballas, S.K.; Larner, J.; Smith, E.D.; Surrey, S.; Schwartz, E.; Rappaport, E.F. Rheologic predictors of the severity of the painful sickle cell crisis. Blood 1988, 72, 1216–1223. [Google Scholar] [CrossRef] [Green Version]
- Lapoumeroulie, C.; Connes, P.; El Hoss, S.; Hierso, R.; Charlot, K.; Lemonne, N.; Elion, J.; Le Van Kim, C.; Romana, M.; Hardy-Dessources, M.D. New insights into red cell rheology and adhesion in patients with sickle cell anaemia during vaso-occlusive crises. Br. J. Haematol. 2019, 185, 991–994. [Google Scholar] [CrossRef] [Green Version]
- Rab, M.A.E.; Kanne, C.K.; Bos, J.; van Oirschot, B.A.; Boisson, C.; Houwing, M.E.; Gerritsma, J.; Teske, E.; Renoux, C.; Riedl, J.; et al. Oxygen gradient ektacytometry derived-biomarkers are associated with vaso-occlusive crises and correlate with treatment response in sickle cell disease. Am. J. Hematol. 2020, 96, E29–E32. [Google Scholar] [CrossRef]
- Rab, M.A.E.; van Oirschot, B.A.; Bos, J.; Merkx, T.H.; van Wesel, A.C.W.; Abdulmalik, O.; Safo, M.K.; Versluijs, B.A.; Houwing, M.E.; Cnossen, M.H.; et al. Rapid and reproducible characterization of sickling during automated deoxygenation in sickle cell disease patients. Am. J. Hematol. 2019, 94, 575–584. [Google Scholar] [CrossRef]
- Boisson, C.; Rab, M.A.E.; Nader, E.; Renoux, C.; van Oirschot, B.A.; Joly, P.; Fort, R.; Stauffer, E.; van Beers, E.J.; Sheehan, V.A.; et al. Methodological aspects of oxygen gradient ektacytometry in sickle cell disease: Effects of sample storage on outcome parameters in distinct patient subgroups. Clin. Hemorheol. Microcirc. 2020, 1–4. [Google Scholar] [CrossRef]
- Aguilar-Martinez, P.; Badens, C.; Bonello-Palot, N.; Cadet, E.; Couque, N.; Ducrocq, R.; Elion, J.; Francina, A.; Joly, P.; Pissard, S.; et al. Flowcharts for the diagnosis and the molecular characterization of hemoglobinopathies. Ann. Biol. Clin. Paris 2010, 68, 455–464. [Google Scholar] [CrossRef]
- Tarer, V.; Etienne-Julan, M.; Diara, J.P.; Belloy, M.S.; Mukizi-Mukaza, M.; Elion, J.; Romana, M. Sickle cell anemia in Guadeloupean children: Pattern and prevalence of acute clinical events. Eur. J. Haematol. 2006, 76, 193–199. [Google Scholar] [CrossRef]
- Rab, M.A.E.; Kanne, C.K.; Bos, J.; Boisson, C.; van Oirschot, B.A.; Nader, E.; Renoux, C.; Joly, P.; Fort, R.; van Beers, E.J.; et al. Methodological aspects of the oxygenscan in sickle cell disease: A need for standardization. Am. J. Hematol. 2020, 95, E5–E8. [Google Scholar] [CrossRef]
- Rab, M.A.E.; van Oirschot, B.A.; Bos, J.; Kanne, C.K.; Sheehan, V.A.; van Beers, E.J.; van Wijk, R. Characterization of Sickling During Controlled Automated Deoxygenation with Oxygen Gradient Ektacytometry. J. Vis. Exp. 2019. [Google Scholar] [CrossRef] [PubMed]
- Baskurt, O.K.; Boynard, M.; Cokelet, G.C.; Connes, P.; Cooke, B.M.; Forconi, S.; Liao, F.; Hardeman, M.R.; Jung, F.; Meiselman, H.J.; et al. New guidelines for hemorheological laboratory techniques. Clin. Hemorheol. Microcirc. 2009, 42, 75–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ballas, S.K.; Dover, G.J.; Charache, S. Effect of hydroxyurea on the rheological properties of sickle erythrocytes in vivo. Am. J. Hematol. 1989, 32, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Lemonne, N.; Charlot, K.; Waltz, X.; Ballas, S.K.; Lamarre, Y.; Lee, K.; Hierso, R.; Connes, C.; Etienne-Julan, M.; Romana, M.; et al. Hydroxyurea treatment does not increase blood viscosity and improves red blood cell rheology in sickle cell anemia. Haematologica 2015, 100, e383–e386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemonne, N.; Mockesch, B.; Charlot, K.; Garnier, Y.; Waltz, X.; Lamarre, Y.; Antoine-Jonville, S.; Etienne-Julan, M.; Hardy-Dessources, M.D.; Romana, M.; et al. Effects of hydroxyurea on blood rheology in sickle cell anemia: A two-years follow-up study. Clin. Hemorheol. Microcirc. 2017, 67, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Akinsheye, I.; Alsultan, A.; Solovieff, N.; Ngo, D.; Baldwin, C.T.; Sebastiani, P.; Chui, D.H.; Steinberg, M.H. Fetal hemoglobin in sickle cell anemia. Blood 2011, 118, 19–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charache, S.; Terrin, M.L.; Moore, R.D.; Dover, G.J.; Barton, F.B.; Eckert, S.V.; McMahon, R.P.; Bonds, D.R. Effect of hydroxyurea on the frequency of painful crises in sickle cell anemia. Investigators of the Multicenter Study of Hydroxyurea in Sickle Cell Anemia. N. Engl. J. Med. 1995, 332, 1317–1322. [Google Scholar] [CrossRef]
- Pittman, R.N.; Golub, A.S.; Carvalho, H. Measurement of oxygen in the microcirculation using phosphorescence quenching microscopy. Adv. Exp. Med. Biol. 2010, 662, 157–162. [Google Scholar] [CrossRef]
- Sakadzic, S.; Mandeville, E.T.; Gagnon, L.; Musacchia, J.J.; Yaseen, M.A.; Yucel, M.A.; Lefebvre, J.; Lesage, F.; Dale, A.M.; Eikermann-Haerter, K.; et al. Large arteriolar component of oxygen delivery implies a safe margin of oxygen supply to cerebral tissue. Nat. Commun. 2014, 5, 5734. [Google Scholar] [CrossRef]
- Nash, G.B.; Johnson, C.S.; Meiselman, H.J. Influence of oxygen tension on the viscoelastic behavior of red blood cells in sickle cell disease. Blood 1986, 67, 110–118. [Google Scholar] [CrossRef]
- Lu, X.; Wood, D.K.; Higgins, J.M. Deoxygenation Reduces Sickle Cell Blood Flow at Arterial Oxygen Tension. Biophys. J. 2016, 110, 2751–2758. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| SS (N = 29) | SS < 5 Years Old (N = 11) | SS with HU (N = 45) | SS Transfused (N = 54) | SC (N = 22) | Sb+ (N = 6) | |
|---|---|---|---|---|---|---|
| Age (yrs) | 24.1 ± 14.0 | 3.6 ± 1.2 *** | 27.1 ± 13.0 +++ | 23.4 ± 12.7 +++ | 29.5 ± 17.2 +++ | 21.2 ± 12.1 ++ |
| HbF (%) | 11.1 ± 12.4 | 15.7 ± 11.4 | 18.3 ± 8.5 *** | 3.6 ± 3.7 ***+++xxx | 4.6 ± 6.7 **+++xxx | 6.8 ± 6.8 +xx |
| HbC (%) | / | / | / | / | 39.5 ± 11.2 | / |
| HbA (%) | / | / | / | 49.3 ± 16.2 | / | 14.3 ± 17.2 |
| Hb (g/L) | 84.7 ± 14.2 | 80.6 ± 14.7 | 90.4 ± 12.7 + | 96.1 ± 17.9 **++x | 110.5 ± 13.9 ***+++xxx### | 97.2 ± 24.3 *+$ |
| MCV (fl) | 78 ± 12 | 83 ± 11 | 95 ± 14 ***++ | 85 ± 10 **xx | 74 ± 10 +x### | 62 ± 9 **+++xxx###$ |
| MCHC (g/dL) | 34.2 ± 1.7 | 34.1 ± 1.4 | 35.1 ± 1.3 | 32.9 ± 4.5 *xxx | 35.6 ± 1.1 *### | 31.2 ± 2.7 *+xx$$ |
| LDH (IU/L) | 380 ± 207 | 451 ± 240 | 334 ± 218 | 122 ± 210 ***+++xxx | 224 ± 176 **++x | 236 ± 209 *+# |
| Retic (%) | 8.8 ± 3.7 | 10.4 ± 5.5 | 8.0 ± 4.2 | 10.1 ± 6.1 x | 4.1 ± 4.5 **++xx### | 2.6 ± 1.9 **++x## |
| RBC aggregation (%) | 60 ± 10 | 65 ± 9 | 64 ± 11 | 59 ± 11 x | 54 ± 10 *++xxx# | 63 ± 5 $ |
| RBC aggregates strenght (s−1) | 442 ± 246 | 550 ± 203 | 509 ± 272 | 424 ± 300 | 369 ± 236 | 445 ± 282 |
| SS (N = 29) | SC (N = 22) | |
|---|---|---|
| VOC or ACS (%) | 63.3 | 37.9 * |
| Osteonecrosis (%) | 16.7 | 20.7 |
| Retinopathy (%) | 0 | 47.0 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boisson, C.; Rab, M.A.E.; Nader, E.; Renoux, C.; Kanne, C.; Bos, J.; van Oirschot, B.A.; Joly, P.; Fort, R.; Gauthier, A.; et al. Effects of Genotypes and Treatment on Oxygenscan Parameters in Sickle Cell Disease. Cells 2021, 10, 811. https://doi.org/10.3390/cells10040811
Boisson C, Rab MAE, Nader E, Renoux C, Kanne C, Bos J, van Oirschot BA, Joly P, Fort R, Gauthier A, et al. Effects of Genotypes and Treatment on Oxygenscan Parameters in Sickle Cell Disease. Cells. 2021; 10(4):811. https://doi.org/10.3390/cells10040811
Chicago/Turabian StyleBoisson, Camille, Minke A. E. Rab, Elie Nader, Céline Renoux, Celeste Kanne, Jennifer Bos, Brigitte A. van Oirschot, Philippe Joly, Romain Fort, Alexandra Gauthier, and et al. 2021. "Effects of Genotypes and Treatment on Oxygenscan Parameters in Sickle Cell Disease" Cells 10, no. 4: 811. https://doi.org/10.3390/cells10040811