
Subnormothermic Ex Vivo Lung Perfusion Temperature Improves Graft Preservation in Lung Transplantation



Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
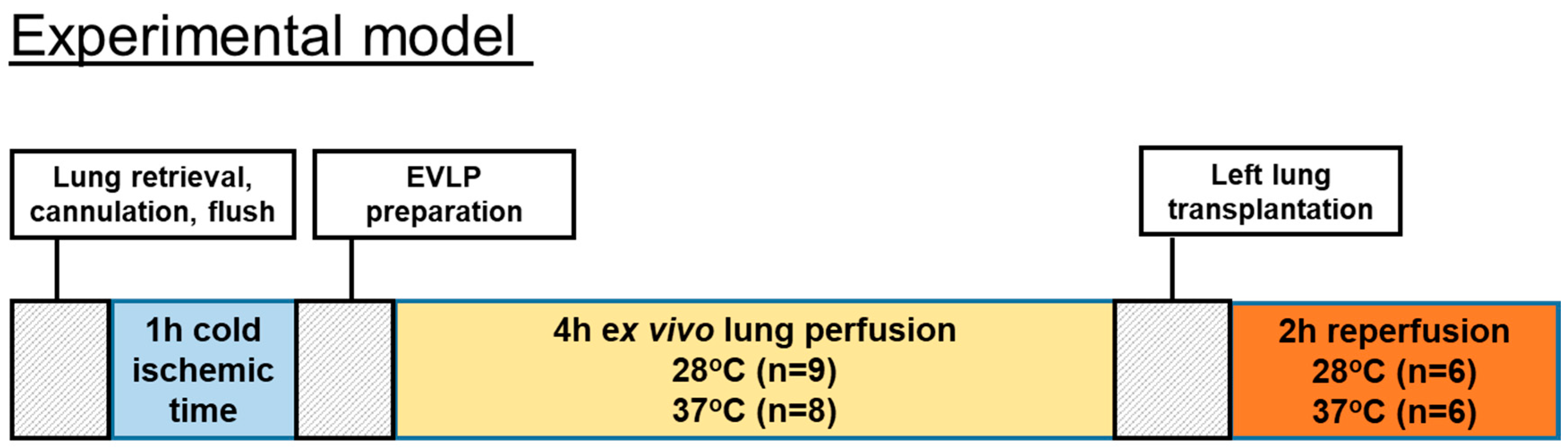
2.2. Surgical Technique and Rat Lung Model for EVLP
2.2.1. Physiological Variables and Clinical Biochemistry Parameters
2.2.2. Normothermic and Subnormothermic EVLP Treatment Groups
2.3. Biochemical Measurements
2.3.1. Rat Lung Transplantation Procedure
2.3.2. Cytokines, Chemokines and Mediators of Tissue Repair
2.3.3. Estimates of ATP Content, Myeloperoxidase Activity and Carbonyl Protein Content in Lung Tissues and Histologic Studies in Lung Sections
2.4. Statistical Method
3. Results
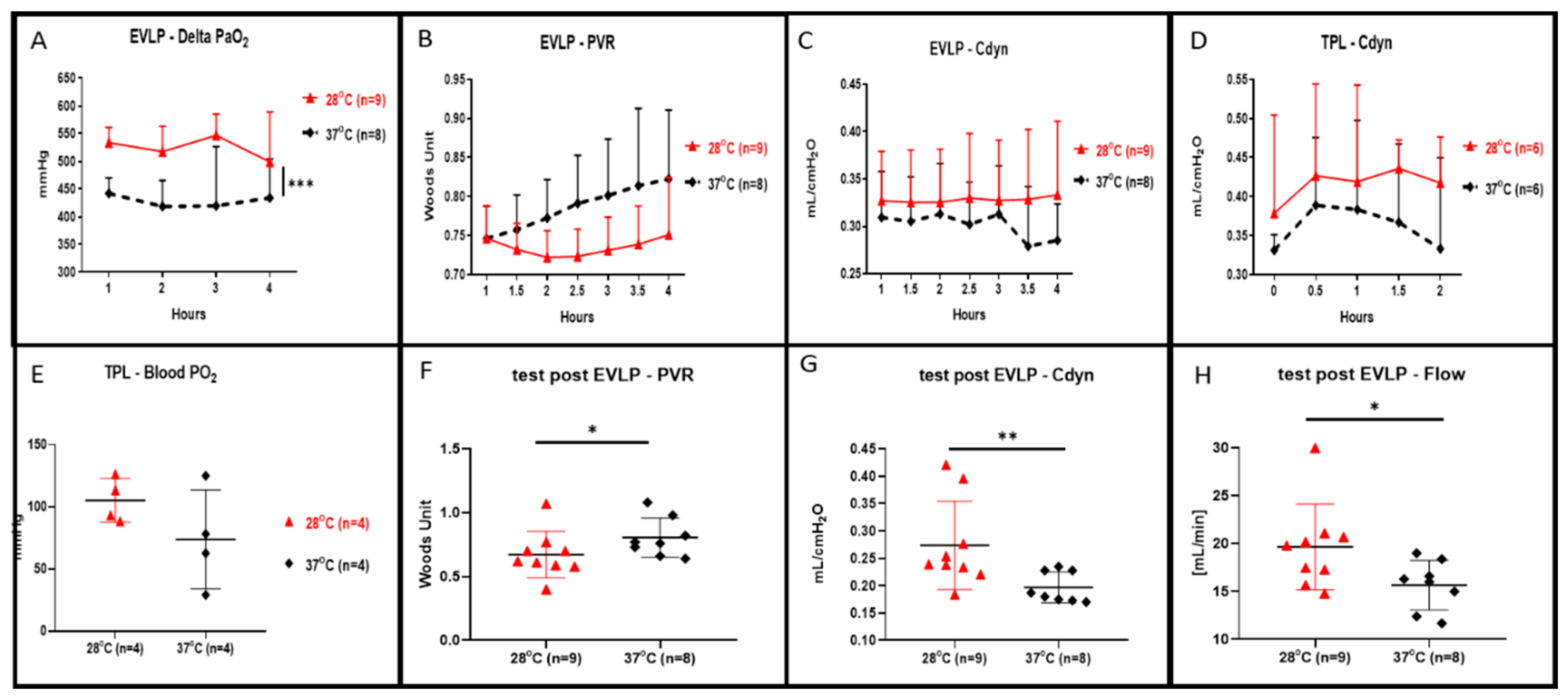
3.1. Lung Physiology during EVLP and Transplantation
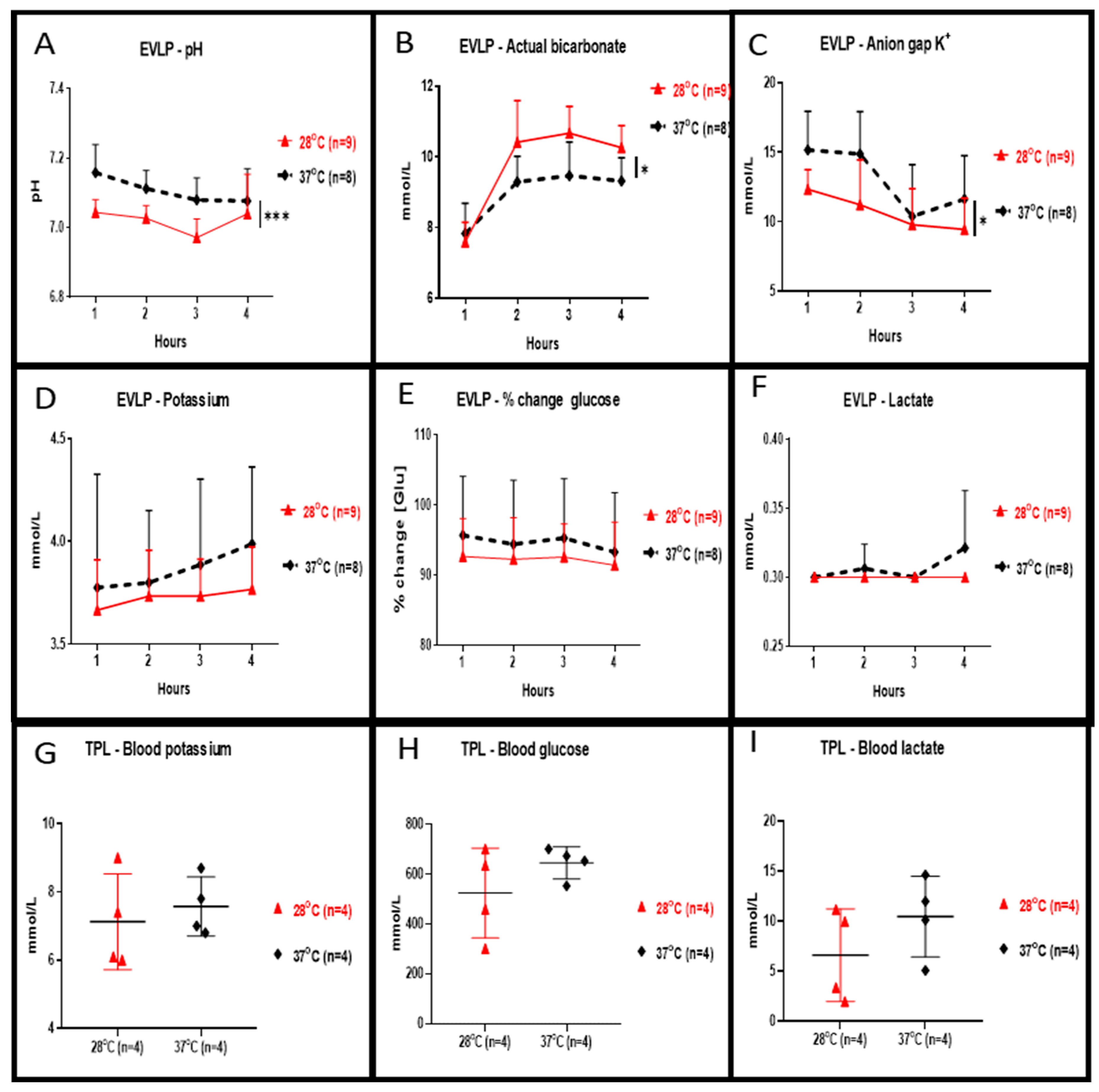
3.2. Clinical Biochemistry in EVLP Perfusate and in Transplanted Recipients
3.3. EVLP Perfusate, Plasma and Tissue Cytokines, Chemokines and Tissue Repair Mediators
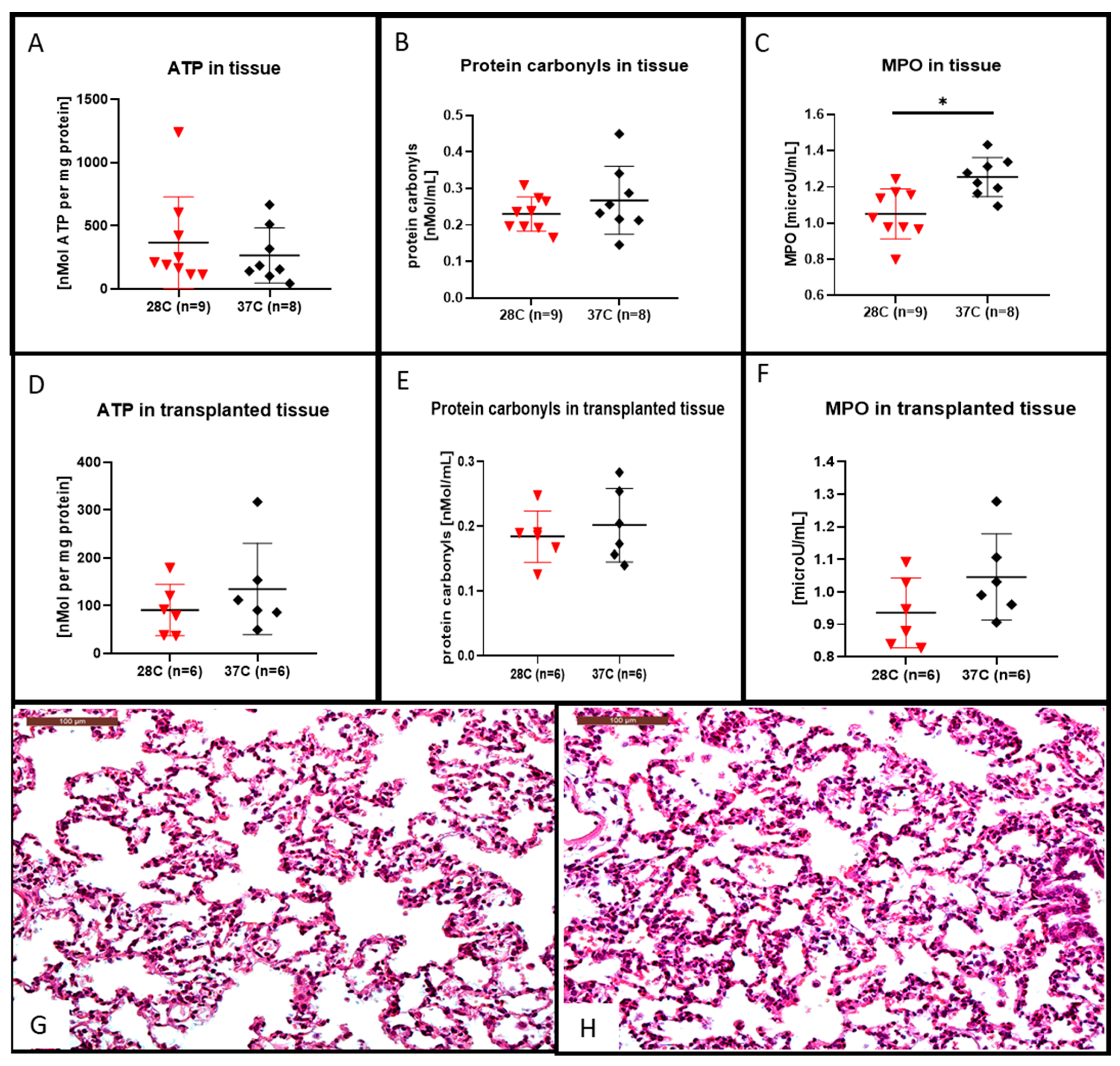
3.4. Lung Tissue Content in MPO, ATP and Carbonyl Proteins, and Histological Studies of Lung Sections
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| Cdyn | dynamic compliance |
| DAMPS | damage-associated molecular patterns |
| EVLP | ex vivo lung perfusion |
| I/R | ischemia-reperfusion |
| MPO | myeloperoxidase |
| PAP | pulmonary arterial pressure |
| PEEP | positive end-expiratory pressure |
| PGD | primary graft dysfunction |
| PVR | pulmonary vascular resistance |
| ROS | reactive oxygen species |
| TPL | transplantation |
References
- Wierup, P.; Haraldsson, A.; Nilsson, F.; Pierre, L.; Schersten, H.; Silverborn, M.; Sjoberg, T.; Westfeldt, U.; Steen, S. Ex vivo evaluation of nonacceptable donor lungs. Ann. Thorac. Surg. 2006, 81, 460–466. [Google Scholar] [CrossRef] [PubMed]
- Jing, L.; Yao, L.; Zhao, M.; Peng, L.P.; Liu, M. Organ preservation: From the past to the future. Acta Pharmacol. Sin. 2018, 39, 845–857. [Google Scholar] [CrossRef] [PubMed]
- Noda, K.; Shigemura, N.; Tanaka, Y.; Bhama, J.K.; D’Cunha, J.; Luketich, J.D.; Bermudez, C.A. Successful prolonged ex vivo lung perfusion for graft preservation in rats. Eur. J. Cardiothorac. Surg. 2014, 45, e54–e60. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Parapanov, R.; Debonneville, A.; Wang, Y.; Abdelnour-Berchtold, E.; Gonzalez, M.; Gronchi, F.; Perentes, J.Y.; Ris, H.B.; Eckert, P.; et al. Treatment with 3-aminobenzamide during ex vivo lung perfusion of damaged rat lungs reduces graft injury and dysfunction after transplantation. Am. J. Transpl. 2020, 20, 967–976. [Google Scholar] [CrossRef]
- Council, N.R. Guide for the Care and Use of Laboratory Animals: Eighth Edition; The National Academies Press: Washington, DC, USA, 2011; p. 246. [Google Scholar] [CrossRef]
- Nelson, K.; Bobba, C.; Eren, E.; Spata, T.; Tadres, M.; Hayes, D., Jr.; Black, S.M.; Ghadiali, S.; Whitson, B.A. Method of isolated ex vivo lung perfusion in a rat model: Lessons learned from developing a rat EVLP program. J. Vis. Exp. 2015. [Google Scholar] [CrossRef] [Green Version]
- Iskender, I.; Arni, S.; Maeyashiki, T.; Citak, N.; Sauer, M.; Rodriguez, J.M.; Frauenfelder, T.; Opitz, I.; Weder, W.; Inci, I. Perfusate adsorption during ex vivo lung perfusion improves early post-transplant lung function. J. Thorac. Cardiovasc. Surg. 2021, 161, e109–e121. [Google Scholar] [CrossRef] [Green Version]
- Fontes, P.; Lopez, R.; van der Plaats, A.; Vodovotz, Y.; Minervini, M.; Scott, V.; Soltys, K.; Shiva, S.; Paranjpe, S.; Sadowsky, D.; et al. Liver preservation with machine perfusion and a newly developed cell-free oxygen carrier solution under subnormothermic conditions. Am. J. Transpl. 2015, 15, 381–394. [Google Scholar] [CrossRef] [PubMed]
- Eshmuminov, D.; Becker, D.; Bautista Borrego, L.; Hefti, M.; Schuler, M.J.; Hagedorn, C.; Muller, X.; Mueller, M.; Onder, C.; Graf, R.; et al. An integrated perfusion machine preserves injured human livers for 1 week. Nat. Biotechnol. 2020, 38, 189–198. [Google Scholar] [CrossRef]
- Obara, H.; Morito, N.; Matsuno, N.; Yoshikawa, R.; Gouchi, M.; Otani, M.; Shonaka, T.; Takahashi, H.; Enosawa, S.; Hirano, T.; et al. Optimum perfusate volume of purified subnormothermic machine perfusion for porcine liver donated after cardiac death. Transpl. Proc. 2018, 50, 2830–2833. [Google Scholar] [CrossRef] [PubMed]
- Vairetti, M.; Ferrigno, A.; Rizzo, V.; Richelmi, P.; Boncompagni, E.; Neri, D.; Freitas, I.; Cillo, U. Subnormothermic machine perfusion protects against rat liver preservation injury: A comparative evaluation with conventional cold storage. Transpl. Proc. 2007, 39, 1765–1767. [Google Scholar] [CrossRef] [PubMed]
- Knaak, J.M.; Spetzler, V.N.; Goldaracena, N.; Louis, K.S.; Selzner, N.; Selzner, M. Technique of subnormothermic ex vivo liver perfusion for the storage, assessment, and repair of marginal liver grafts. J. Vis. Exp. 2014, e51419. [Google Scholar] [CrossRef] [Green Version]
- Bhattacharjee, R.N.; Patel, S.V.B.; Sun, Q.; Jiang, L.; Richard-Mohamed, M.; Ruthirakanthan, A.; Aquil, S.; Al-Ogaili, R.; Juriasingani, S.; Sener, A.; et al. Renal protection against ischemia reperfusion injury: Hemoglobin-based oxygen carrier-201 versus blood as an oxygen carrier in Ex Vivo subnormothermic machine perfusion. Transplantation 2020, 104, 482–489. [Google Scholar] [CrossRef]
- Ward, L.C.; Buttery, P.J. The patho-physiological basis for tests of viability in isolated perfused organs. Biomedicine 1979, 30, 181–186. [Google Scholar] [PubMed]
- Bortner, C.D.; Hughes, F.M., Jr.; Cidlowski, J.A. A primary role for K+ and Na+ efflux in the activation of apoptosis. J. Biol. Chem. 1997, 272, 32436–32442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koike, T.; Yeung, J.C.; Cypel, M.; Rubacha, M.; Matsuda, Y.; Sato, M.; Waddell, T.K.; Liu, M.; Keshavjee, S. Kinetics of lactate metabolism during acellular normothermic ex vivo lung perfusion. J. Heart Lung Transpl. 2011, 30, 1312–1319. [Google Scholar] [CrossRef]
- Couto-Mallon, D.; Gonzalez-Vilchez, F.; Almenar-Bonet, L.; Diaz-Molina, B.; Segovia-Cubero, J.; Gonzalez-Costello, J.; Delgado-Jimenez, J.; Castel-Lavilla, M.A.; Crespo-Leiro, M.G.; Rangel-Sousa, D.; et al. Prognostic value of serum lactate levels in patients undergoing urgent heart transplant: A subanalysis of the ASIS-TC Spanish multicenter study. Rev. Esp. Cardiol. (Engl. Ed.) 2019, 72, 208–214. [Google Scholar] [CrossRef] [Green Version]
- Chouchani, E.T.; Pell, V.R.; James, A.M.; Work, L.M.; Saeb-Parsy, K.; Frezza, C.; Krieg, T.; Murphy, M.P. A unifying mechanism for mitochondrial superoxide production during ischemia-reperfusion injury. Cell Metab. 2016, 23, 254–263. [Google Scholar] [CrossRef] [Green Version]
- Jassem, W.; Fuggle, S.V.; Rela, M.; Koo, D.D.; Heaton, N.D. The role of mitochondria in ischemia/reperfusion injury. Transplantation 2002, 73, 493–499. [Google Scholar] [CrossRef] [Green Version]
- Rauen, U.; de Groot, H. Mammalian cell injury induced by hypothermia- the emerging role for reactive oxygen species. Biol. Chem. 2002, 383, 477–488. [Google Scholar] [CrossRef]
- Luer, B.; Koetting, M.; Efferz, P.; Minor, T. Role of oxygen during hypothermic machine perfusion preservation of the liver. Transpl. Int. 2010, 23, 944–950. [Google Scholar] [CrossRef] [PubMed]
- Muller, X.; Schlegel, A.; Kron, P.; Eshmuminov, D.; Wurdinger, M.; Meierhofer, D.; Clavien, P.A.; Dutkowski, P. Novel real-time prediction of liver graft function during hypothermic oxygenated machine perfusion before liver transplantation. Ann. Surg. 2019, 270, 783–790. [Google Scholar] [CrossRef] [PubMed]
- Noda, K.; Shigemura, N.; Tanaka, Y.; Bhama, J.; D’Cunha, J.; Kobayashi, H.; Luketich, J.D.; Bermudez, C.A. Hydrogen preconditioning during ex vivo lung perfusion improves the quality of lung grafts in rats. Transplantation 2014, 98, 499–506. [Google Scholar] [CrossRef] [PubMed]
- Dalle-Donne, I.; Giustarini, D.; Colombo, R.; Rossi, R.; Milzani, A. Protein carbonylation in human diseases. Trends Mol. Med. 2003, 9, 169–176. [Google Scholar] [CrossRef]
- Dalle-Donne, I.; Aldini, G.; Carini, M.; Colombo, R.; Rossi, R.; Milzani, A. Protein carbonylation, cellular dysfunction, and disease progression. J. Cell Mol. Med. 2006, 10, 389–406. [Google Scholar] [CrossRef]
- Honda, H.M.; Korge, P.; Weiss, J.N. Mitochondria and ischemia/reperfusion injury. Ann. N. Y. Acad. Sci. 2005, 1047, 248–258. [Google Scholar] [CrossRef] [PubMed]
- Machuca, T.N.; Cypel, M.; Yeung, J.C.; Bonato, R.; Zamel, R.; Chen, M.; Azad, S.; Hsin, M.K.; Saito, T.; Guan, Z.; et al. Protein expression profiling predicts graft performance in clinical ex vivo lung perfusion. Ann. Surg. 2015, 261, 591–597. [Google Scholar] [CrossRef]
- Hoffman, S.A.; Wang, L.; Shah, C.V.; Ahya, V.N.; Pochettino, A.; Olthoff, K.; Shaked, A.; Wille, K.; Lama, V.N.; Milstone, A.; et al. Plasma cytokines and chemokines in primary graft dysfunction post-lung transplantation. Am. J. Transpl. 2009, 9, 389–396. [Google Scholar] [CrossRef]
- Allen, J.G.; Lee, M.T.; Weiss, E.S.; Arnaoutakis, G.J.; Shah, A.S.; Detrick, B. Preoperative recipient cytokine levels are associated with early lung allograft dysfunction. Ann. Thorac. Surg. 2012, 93, 1843–1849. [Google Scholar] [CrossRef]
- Gloria, J.N.; Yerxa, J.; Kesseli, S.J.; Davis, R.P.; Samoylova, M.L.; Barbas, A.S.; Hartwig, M.G.; Duke Ex Vivo Organ, L.; Zhang, M.; Parker, W.; et al. Subnormothermic exvivo lung perfusion attenuates graft inflammation in a rat transplant model. J. Thorac. Cardiovasc. Surg. 2021. [Google Scholar] [CrossRef]
- Inci, I.; Erne, B.; Arni, S.; Jungraithmayr, W.; Inci, D.; Hillinger, S.; Vogt, P.; Leskosek, B.; Weder, W. Prevention of primary graft dysfunction in lung transplantation by N-acetylcysteine after prolonged cold ischemia. J. Heart Lung Transpl. 2010, 29, 1293–1301. [Google Scholar] [CrossRef]
- Noda, K.; Tane, S.; Haam, S.J.; D’Cunha, J.; Hayanga, A.J.; Luketich, J.D.; Shigemura, N. Targeting circulating leukocytes and pyroptosis during Ex Vivo lung perfusion improves lung preservation. Transplantation 2017, 101, 2841–2849. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| M (SD) | Perfusate | Perfusate | Plasma | Plasma | Tissue | Tissue |
|---|---|---|---|---|---|---|
| Normo. (N = 8) | Subn. (N = 9) | Normo. (N = 6) | Subno. (N = 6) | Normo. (N = 6) | Subno. (N = 6) | |
| TNF-α | 1589 (1073) *** | 59.65 (69.4) | 1679 (1962) | 633 (451.3) | 140.4 (23.86) * | 105.9 (26.96) |
| VEGF | 0 (0) | 0 (0) | 1271 (1683) | 744.2 (526.2) | ||
| MCP-1 | 109.5 (38.65) *** | 20.29 (9.96) | 2761 (4942) | 838.1 (382.5) | ||
| GM-CSF | 1.23 (0.90) * | 0.50 (0.14) | 562.2 (1062) | 167.5 (113.7) | ||
| RANTES | 12.01 (6.26) * | 6.15 (3.19) | 157.2 (51.79) | 278.3 (153.8) | ||
| MIP3-α | 6.31 (7.64) * | 0.58 (0.02) | 165.3 (69.47) | 139 (89) | ||
| MIP1-α | 3018 (3064) * | 372.9 (201.8) | 713.5 (758.5) | 287.1 (186.1) | ||
| IFN-γ | 0 (0) | 0 (0) | 352.8 (53.03) | 464.7 (363.5) | ||
| M-CSF | 0.67 (0.39) | 0.63 (0.53) | 35.63 (8.41) | 39.43 (29.79) | ||
| G-CSF | 0.18 (0.15) * | 0.042 (0.00) | 13.98 (1.87) | 18.28 (18.67) | ||
| GRO/KC | 4536 (2450) *** | 192.5 (206) | 584.7(397.2) | 407.6 (306.9) | ||
| IL1-α | 0.25 (0.33) | 0.15 (0.14) | 144.8 (50.02) | 171.2 (99.19) | ||
| IL1-β | 9.65 (5.75) | 11.27 (5.72) | 1014 (1508) | 423 (272.8) | 489.5 (194.1) * | 250.8 (165.2) |
| IL-2 | 0 (0) | 0 (0) | 1632 (264.9) | 1810 (935.1) | ||
| IL-4 | 1.20 (0.85) | 0.60 (0.54) | 142.5 (21.3) | 180 (119.3) | ||
| IL-5 | 6.05 (5.33) | 4.92 (3.41) | 159.3 (19.26) | 166.3 (46.47) | ||
| IL-6 | 134.7 (81.87) | 3.032 (0.02) | 826.7 (517.5) | 607 (419.1) | 612.5 (214.7) | 394.1 (169.8) |
| IL-7 | 520.6 (929.7) | 196.4 (138.9) | 0.34 (0.34) | 0.2 (0.002) | ||
| IL-10 | 5.41 (6.11) | 1.89 (3.04) | 3569 (2739) | 5886 (4518) | ||
| IL-12 (p70) | 1.851 (1.30) | 1.036 (1.203) | 191.8 (62.04) | 226.3 (141.4) | ||
| IL-13 | 0 (0) | 0 (0) | 67.67 (11.36) | 94.81 (71.94) | ||
| IL-17A | 0.92 (0.22) | 0.8 (0) | 99.59 (10.04) | 115.6 (61.64) | ||
| IL-18 | 0 (0) | 0 (0) | 890 (222.8) | 1167 (512.3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arni, S.; Maeyashiki, T.; Citak, N.; Opitz, I.; Inci, I. Subnormothermic Ex Vivo Lung Perfusion Temperature Improves Graft Preservation in Lung Transplantation. Cells 2021, 10, 748. https://doi.org/10.3390/cells10040748
Arni S, Maeyashiki T, Citak N, Opitz I, Inci I. Subnormothermic Ex Vivo Lung Perfusion Temperature Improves Graft Preservation in Lung Transplantation. Cells. 2021; 10(4):748. https://doi.org/10.3390/cells10040748
Chicago/Turabian StyleArni, Stephan, Tatsuo Maeyashiki, Necati Citak, Isabelle Opitz, and Ilhan Inci. 2021. "Subnormothermic Ex Vivo Lung Perfusion Temperature Improves Graft Preservation in Lung Transplantation" Cells 10, no. 4: 748. https://doi.org/10.3390/cells10040748