
Biocompatibility Study of Hydrogel Biopolymer Scaffold with Encapsulated Mesenchymal Stem Cells
 ,
,  ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Rat Mesenchymal Stem Cell (MSC) Culture
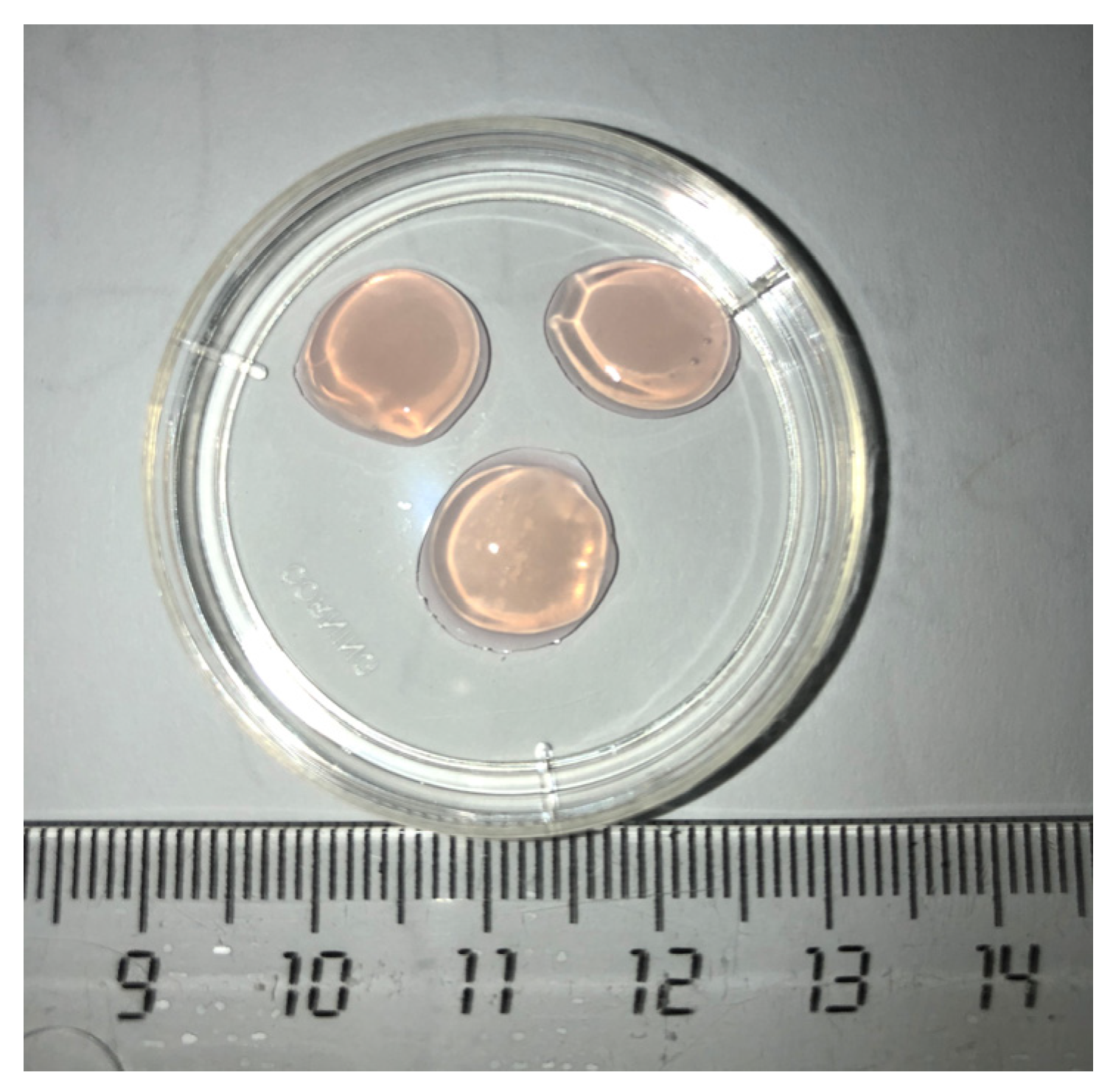
2.2. Scaffold Forming
2.3. Formation of Cell-Containing and Cell-Free Control Implant Specimens
2.4. Evaluation of Scaffold Biocompatibility In Vivo
2.4.1. Animal Experimental Studies
2.4.2. Morphological Analyses of the Biomaterials
2.5. Biotransformation Analysis of Cell-Containing Scaffolds In Vivo
2.5.1. Animal Experimental Study
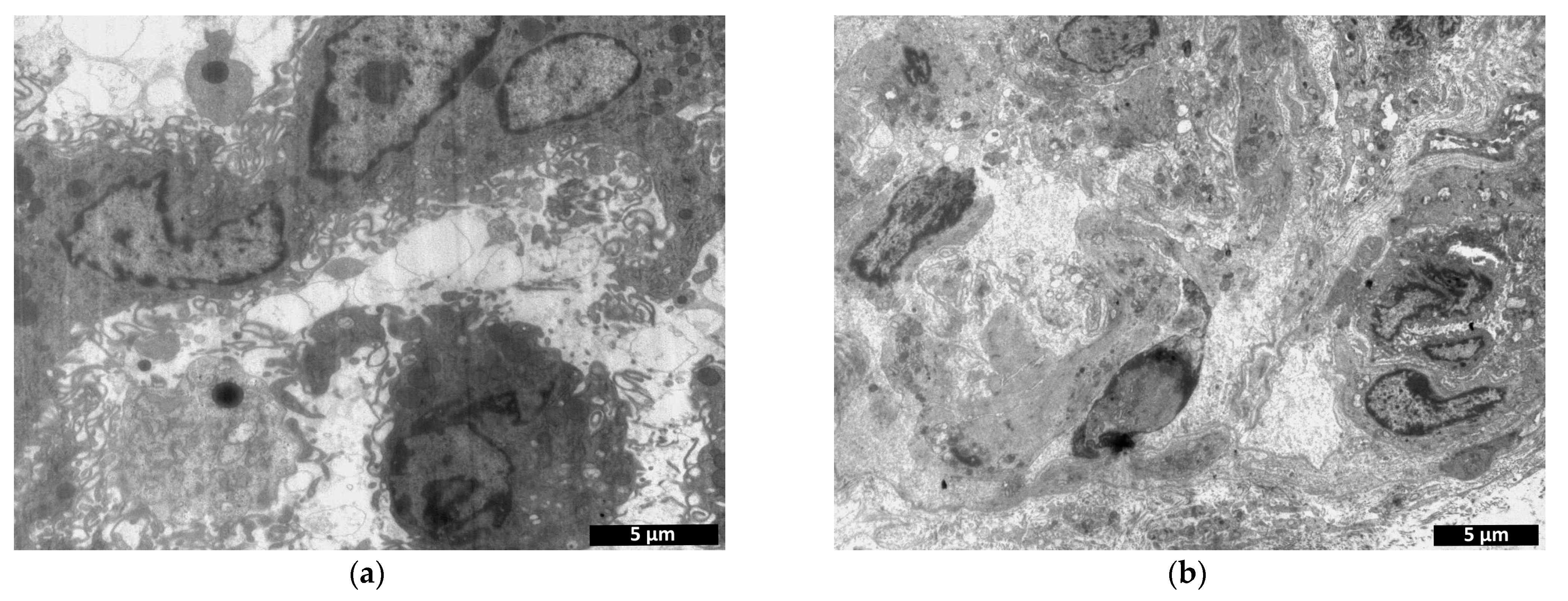
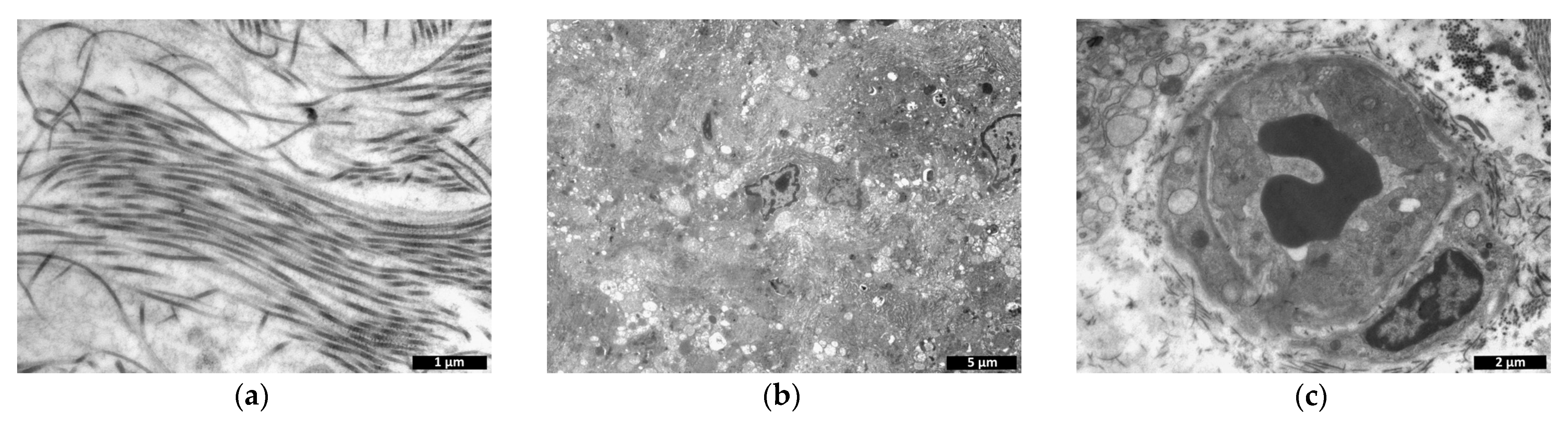
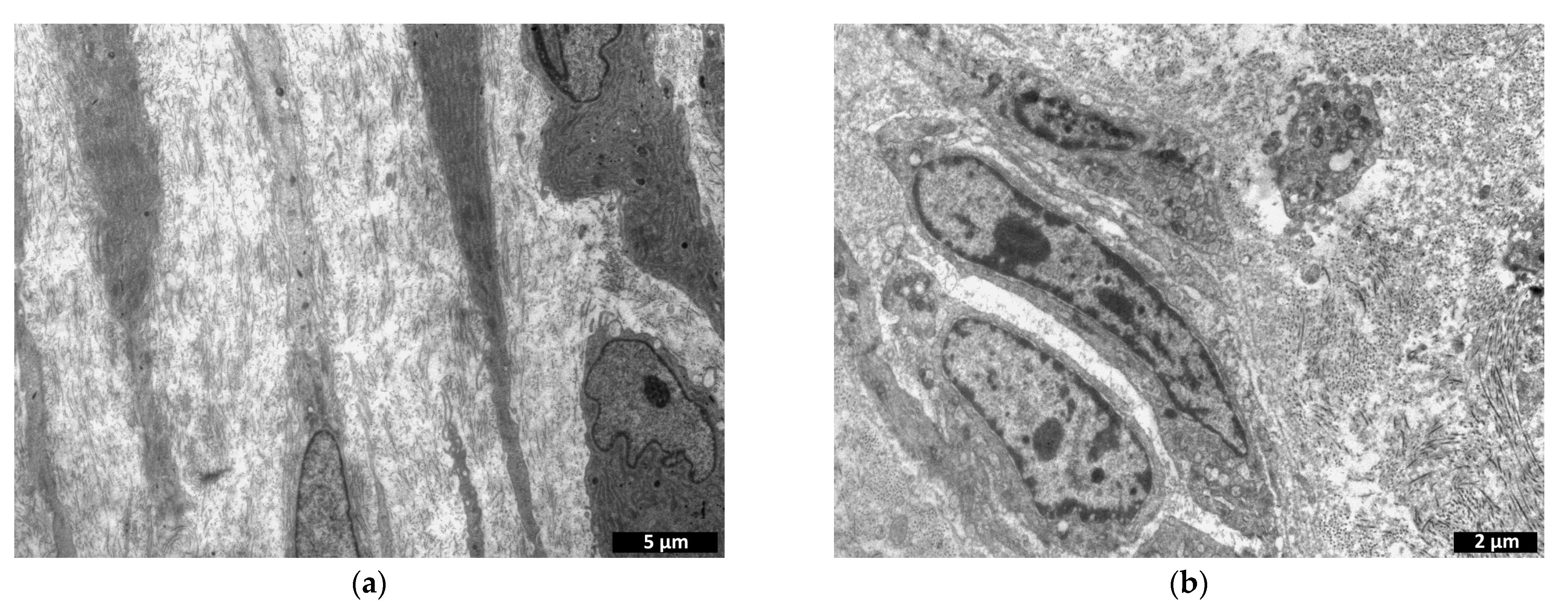
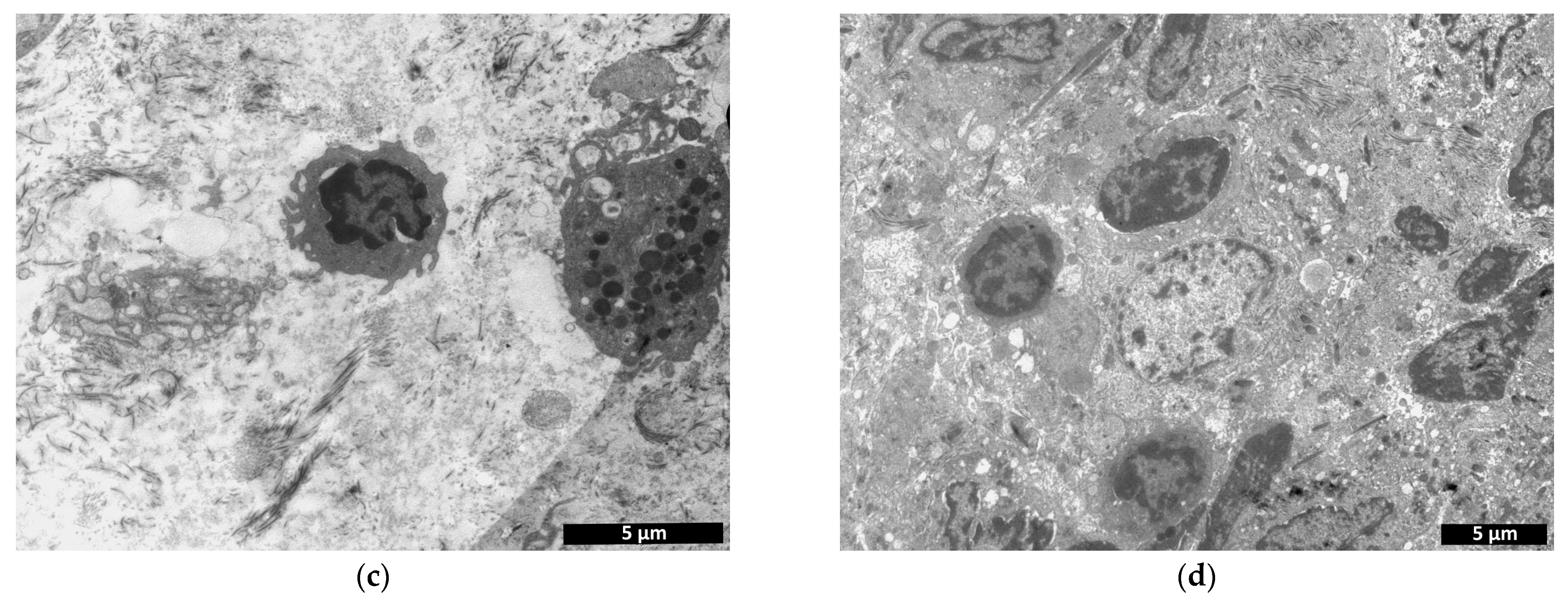
2.5.2. Transmission Electron Microscopy
- -
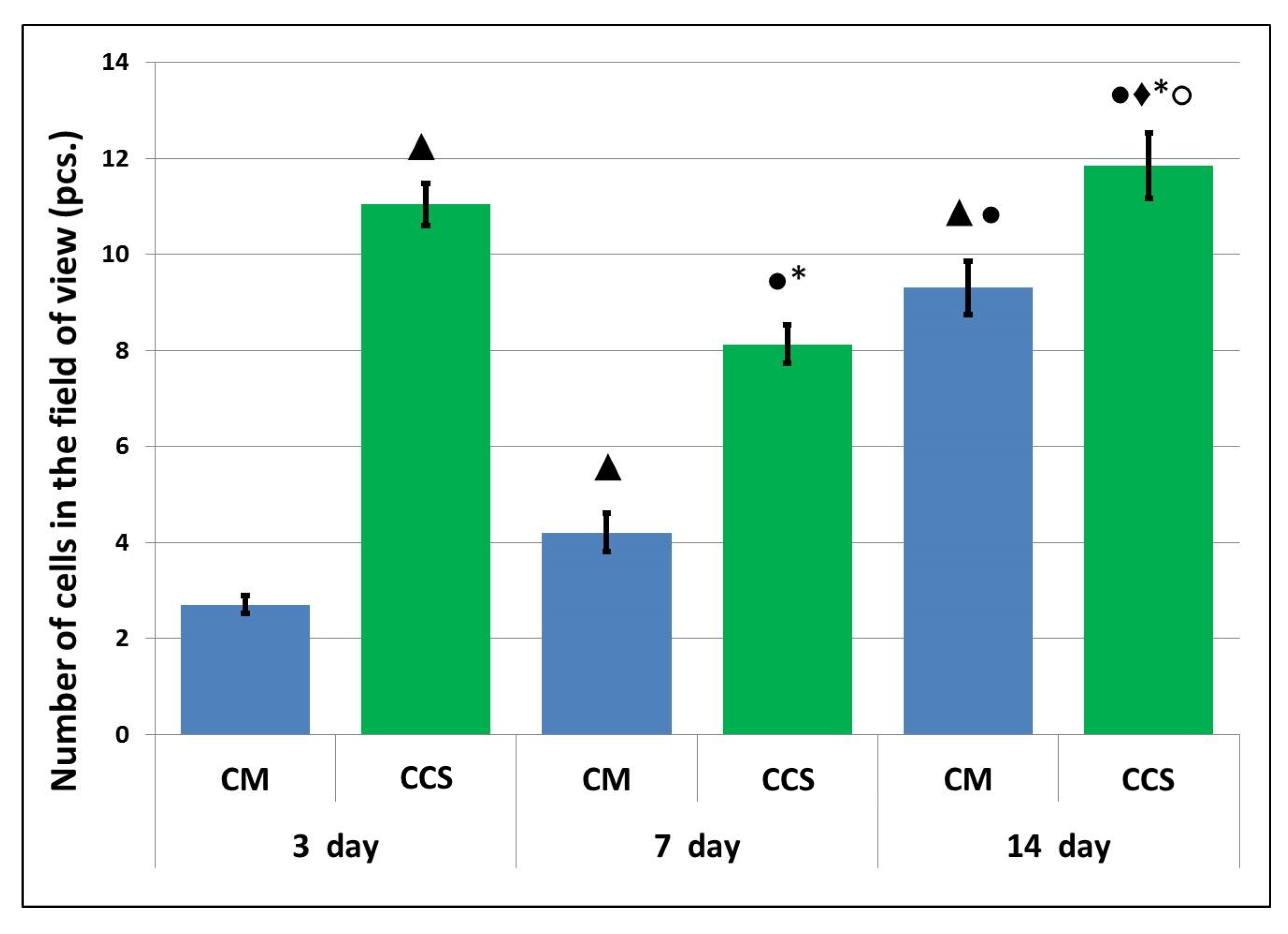
- Counting the number of cells within a 38 × 38 µm field of view of the specimen (n = 25 from each specimen);
- -
- Analysis of structural changes in the implant itself without cells: microphotographs obtained at 14,000× magnification (n = 20 from each specimen) were processed using the ImageJ software package (National Institutes of Health). This software package calculates the percentage ratio of the examined area to the entire image area.
2.6. Statistical Analysis
3. Results and Discussion
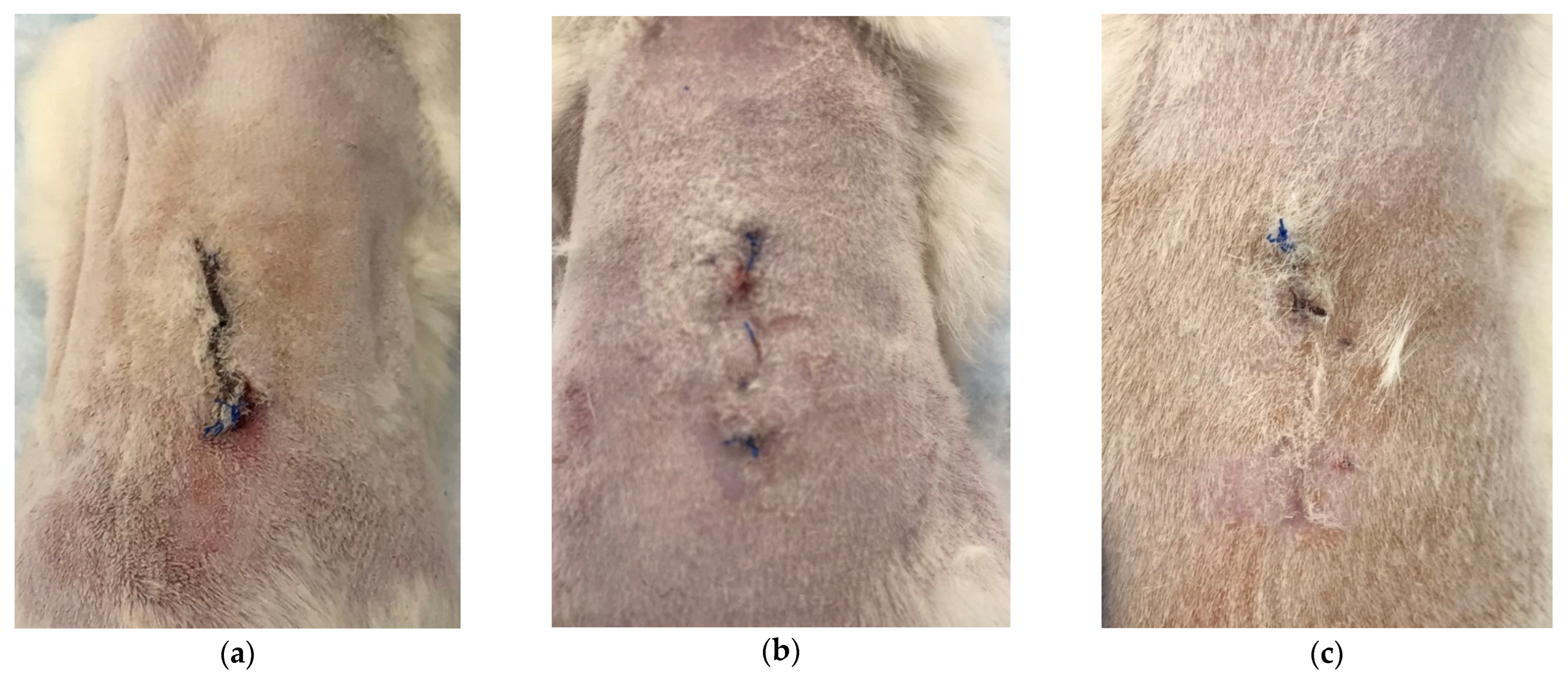
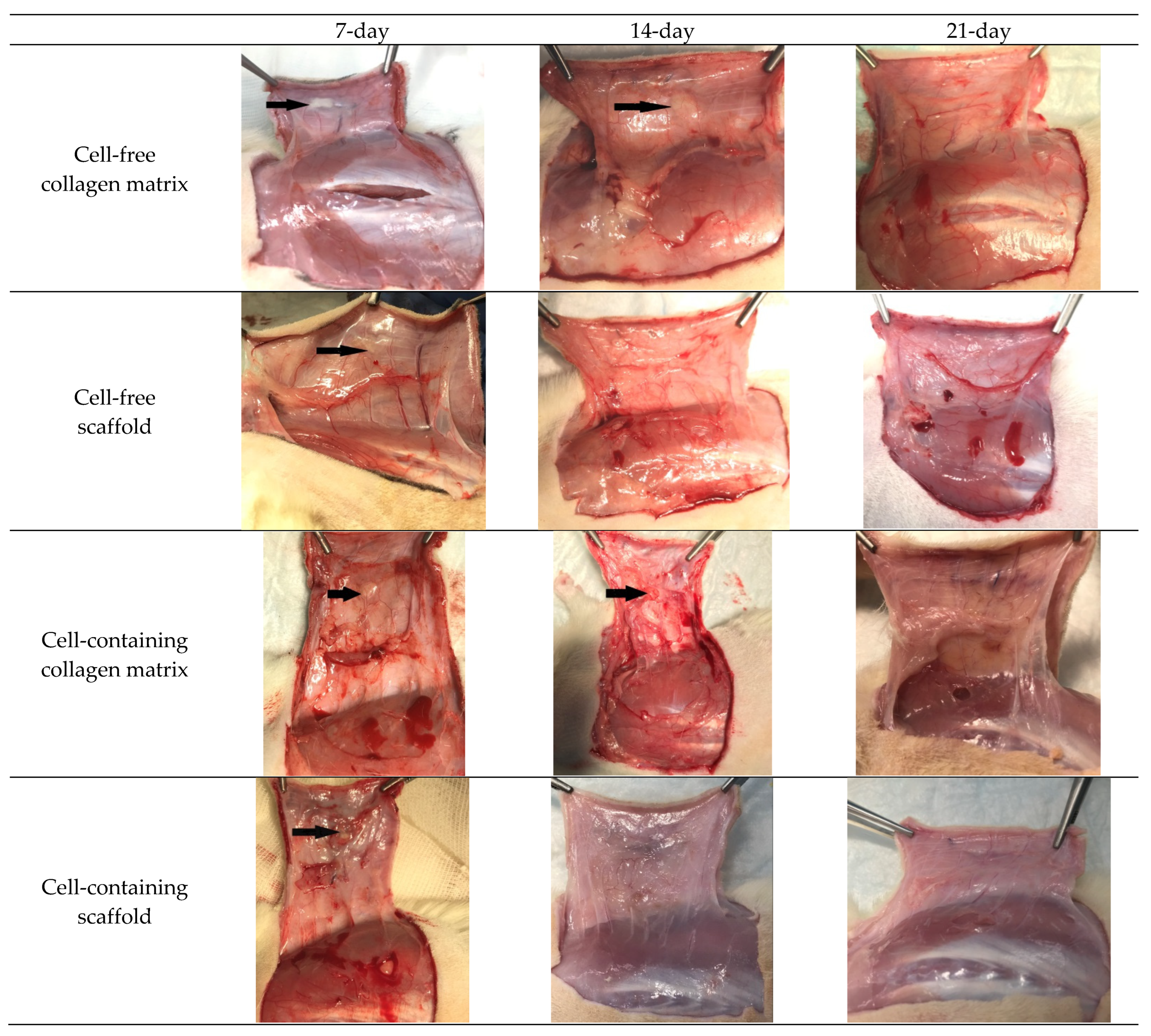
3.1. Macroscopic Observations
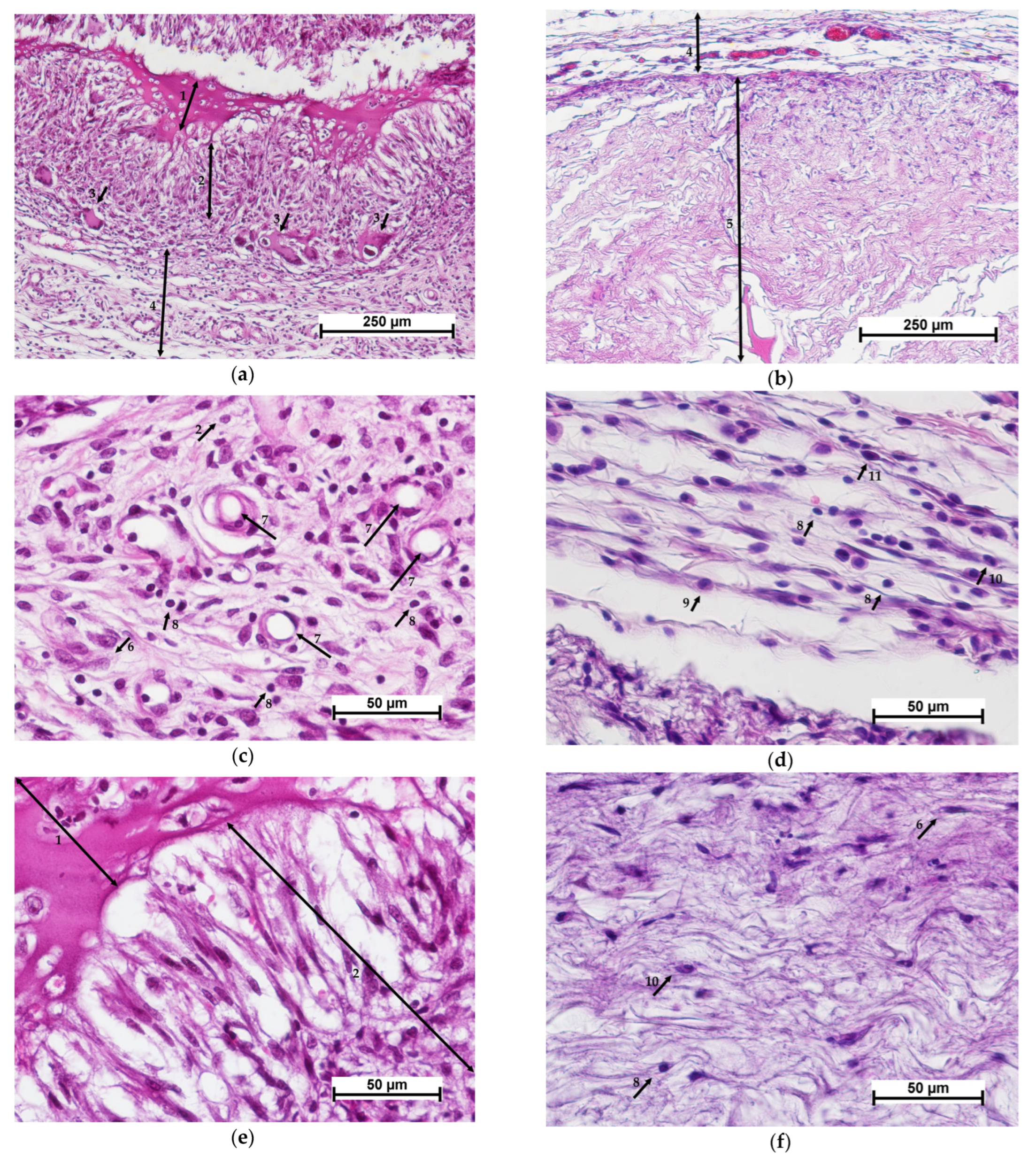
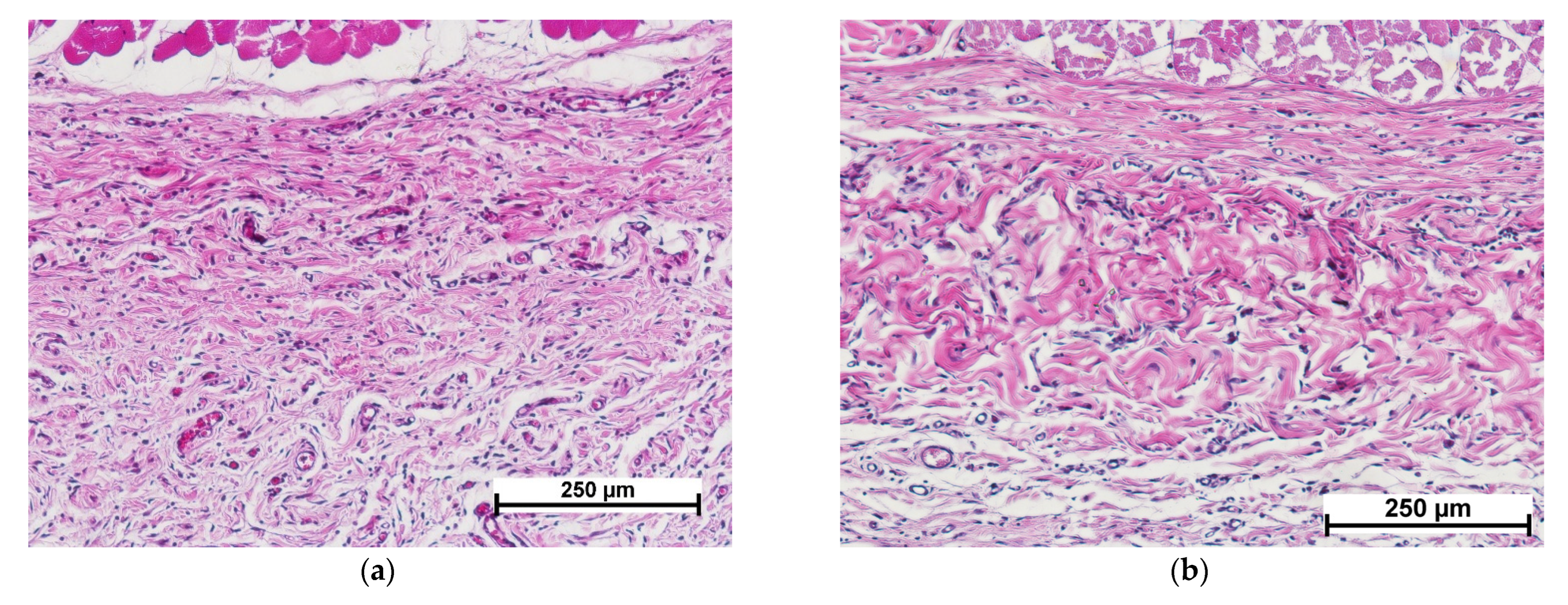
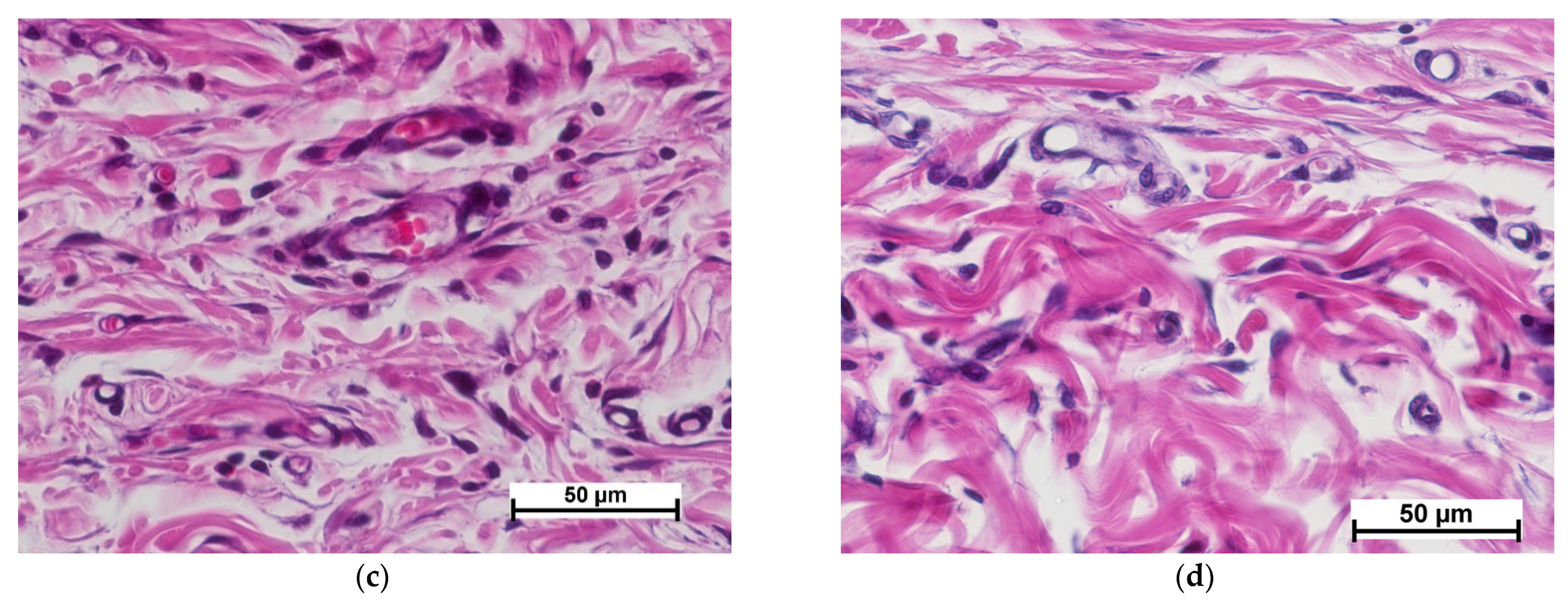
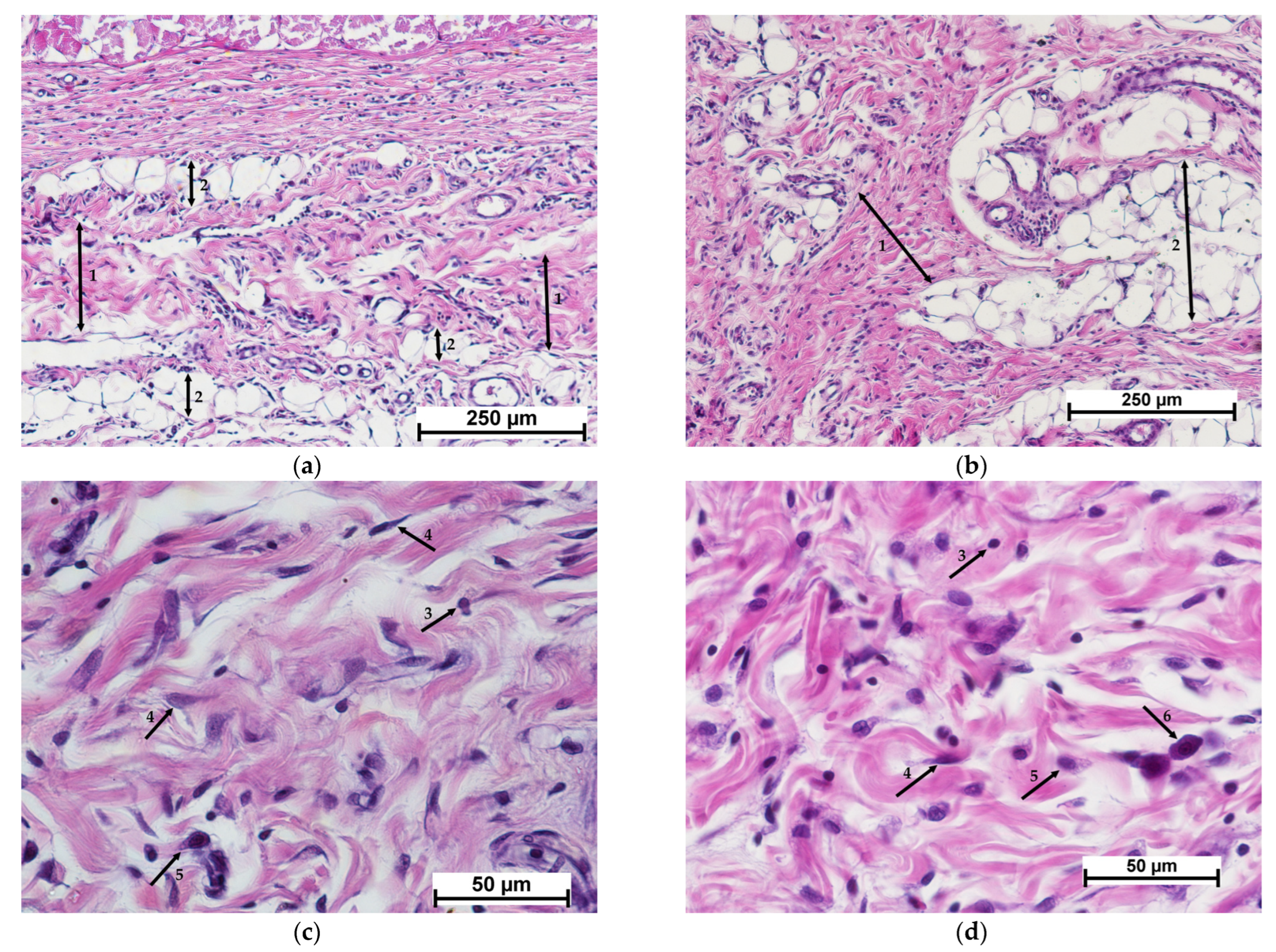
3.2. Results of Morphological Analyses of Cell-Free Implants
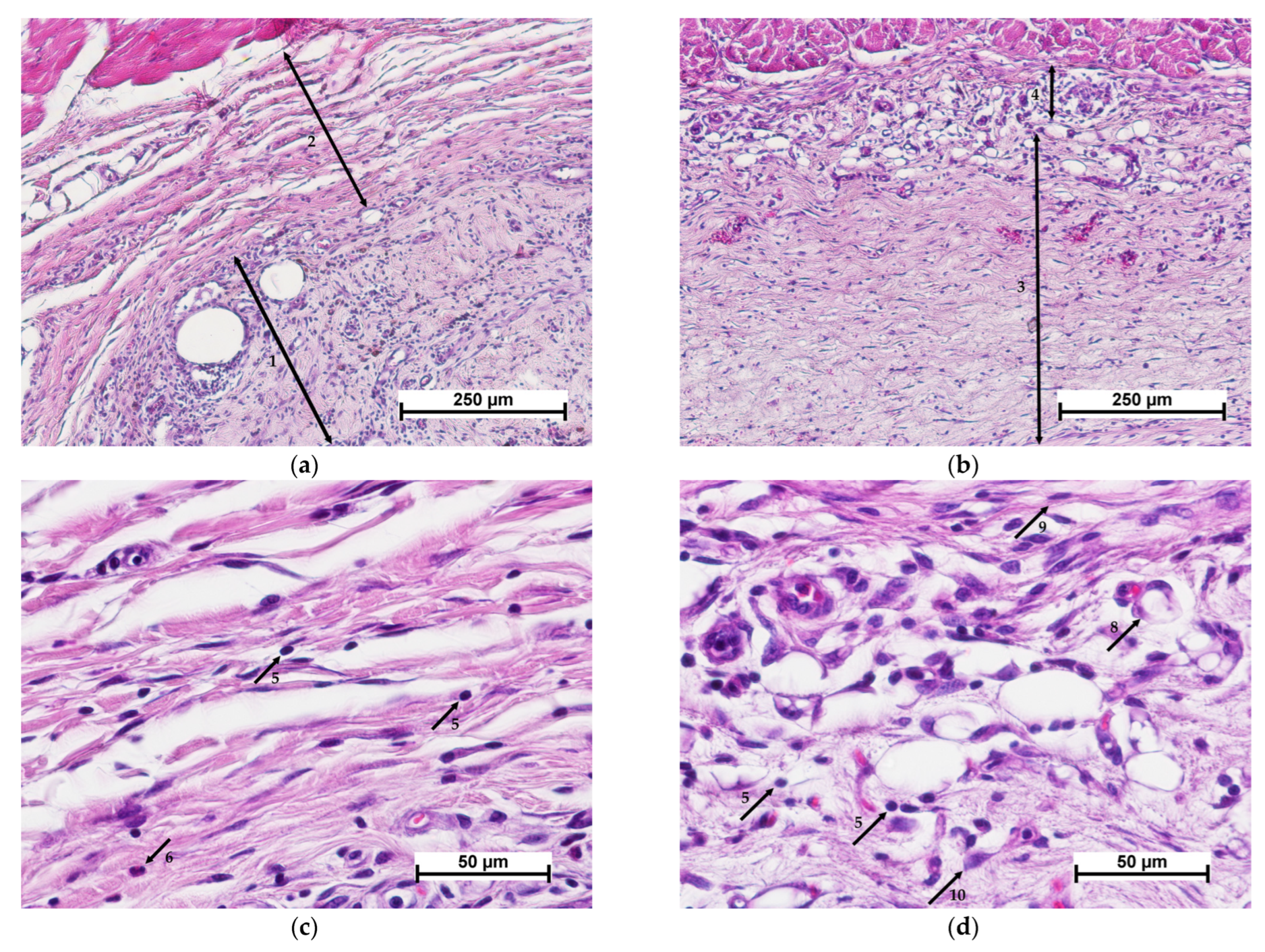
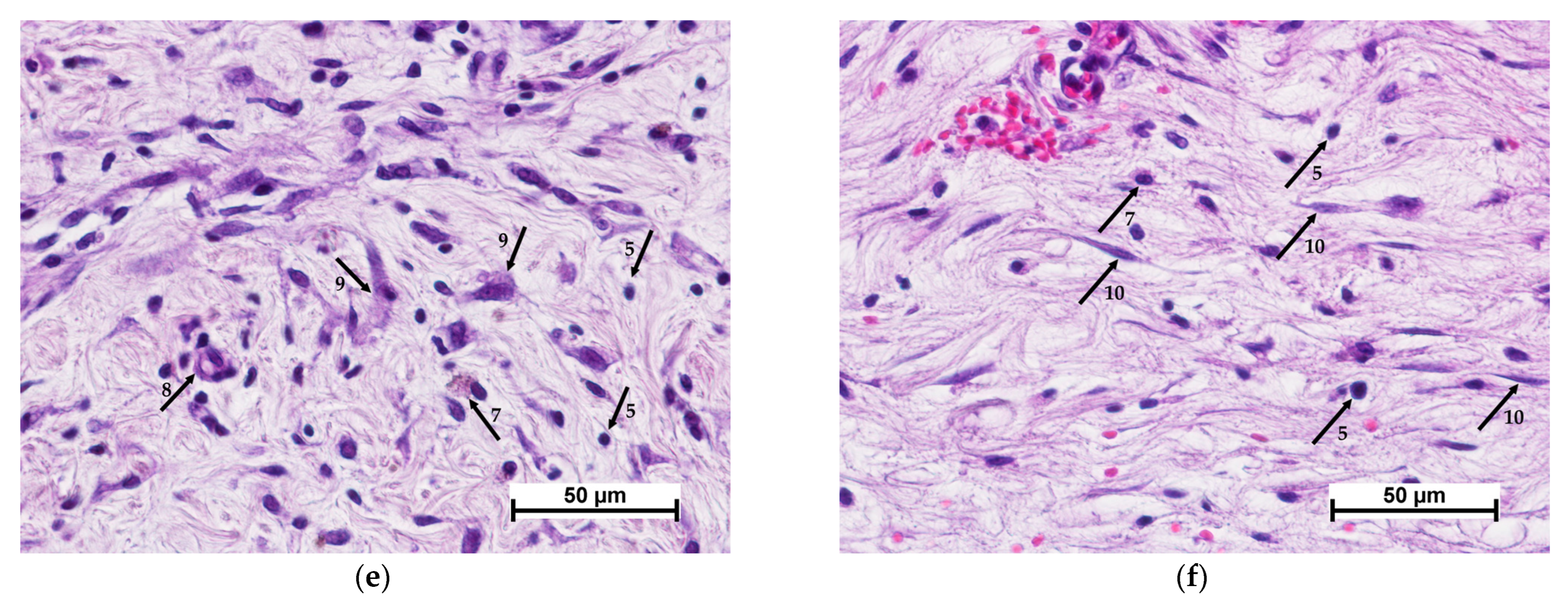
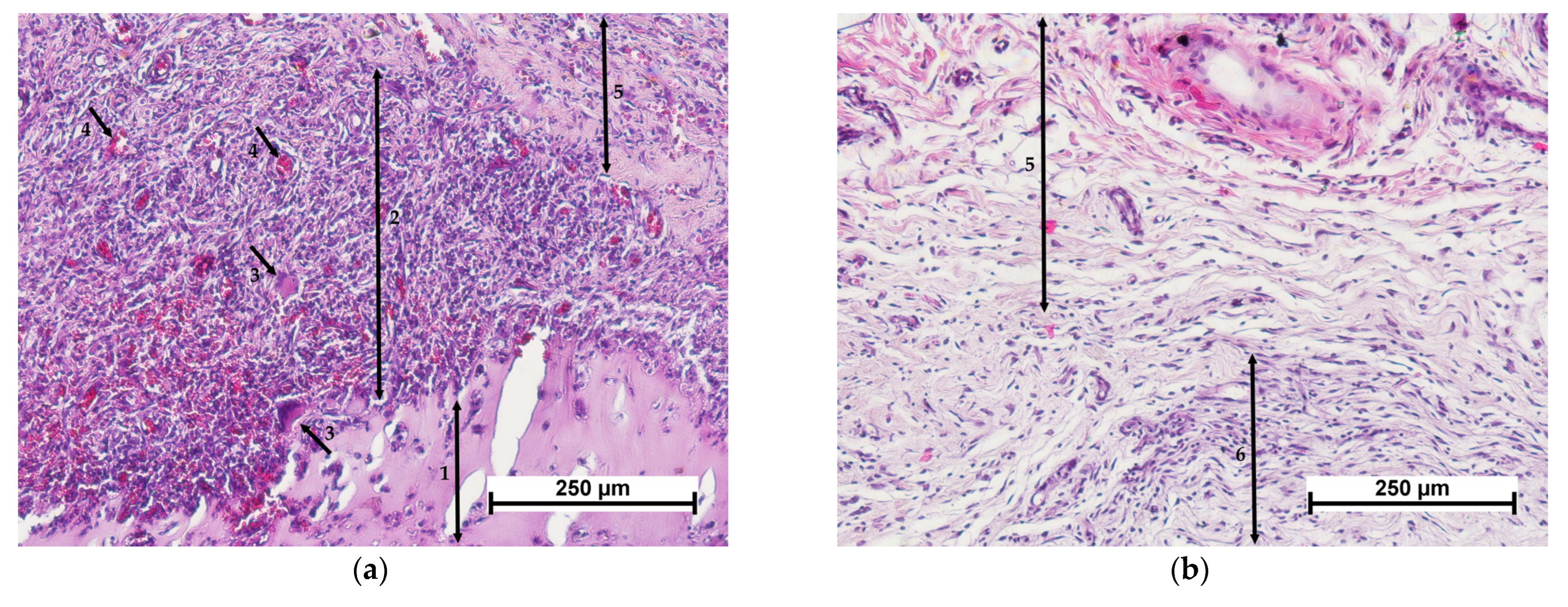
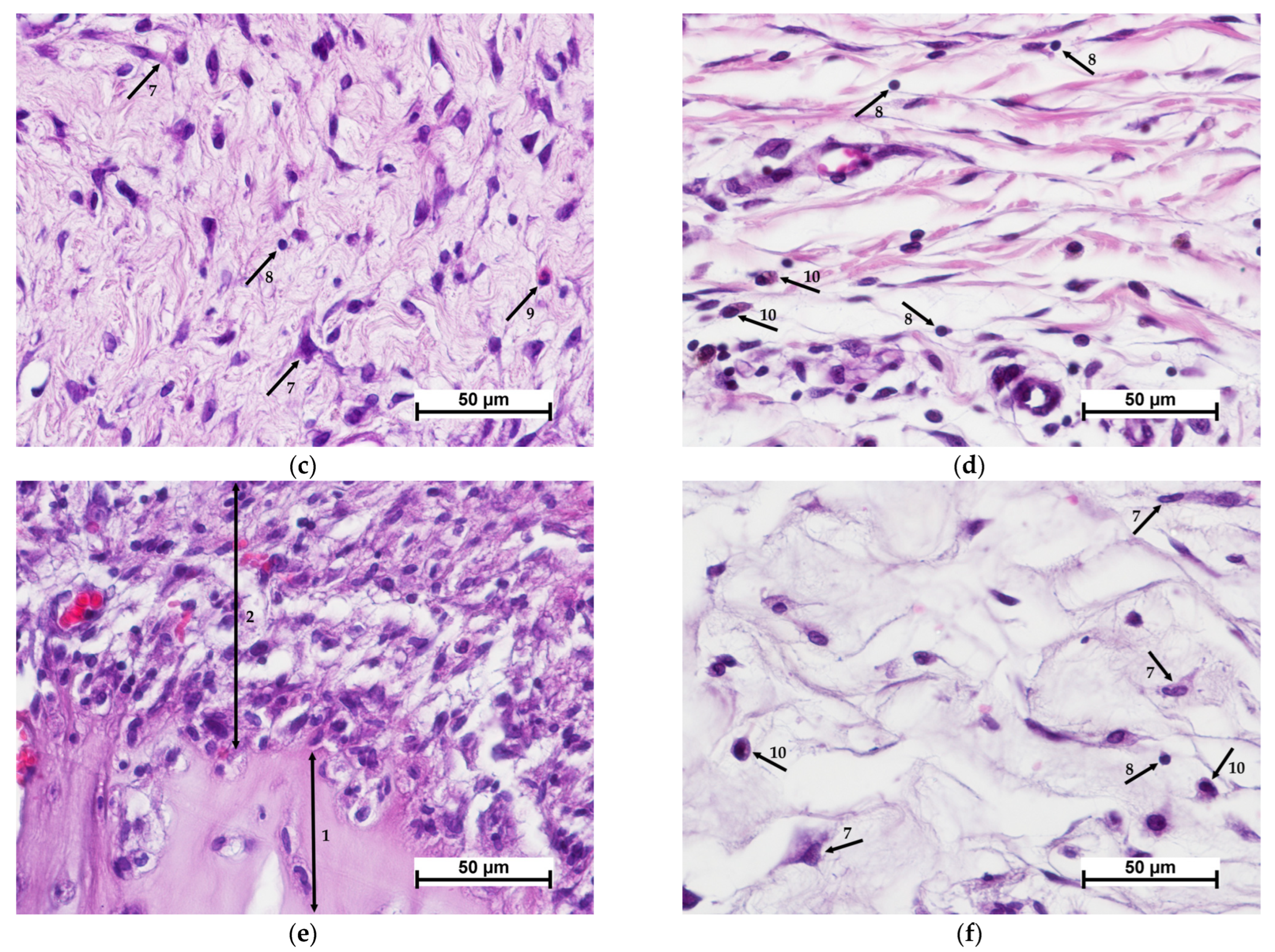
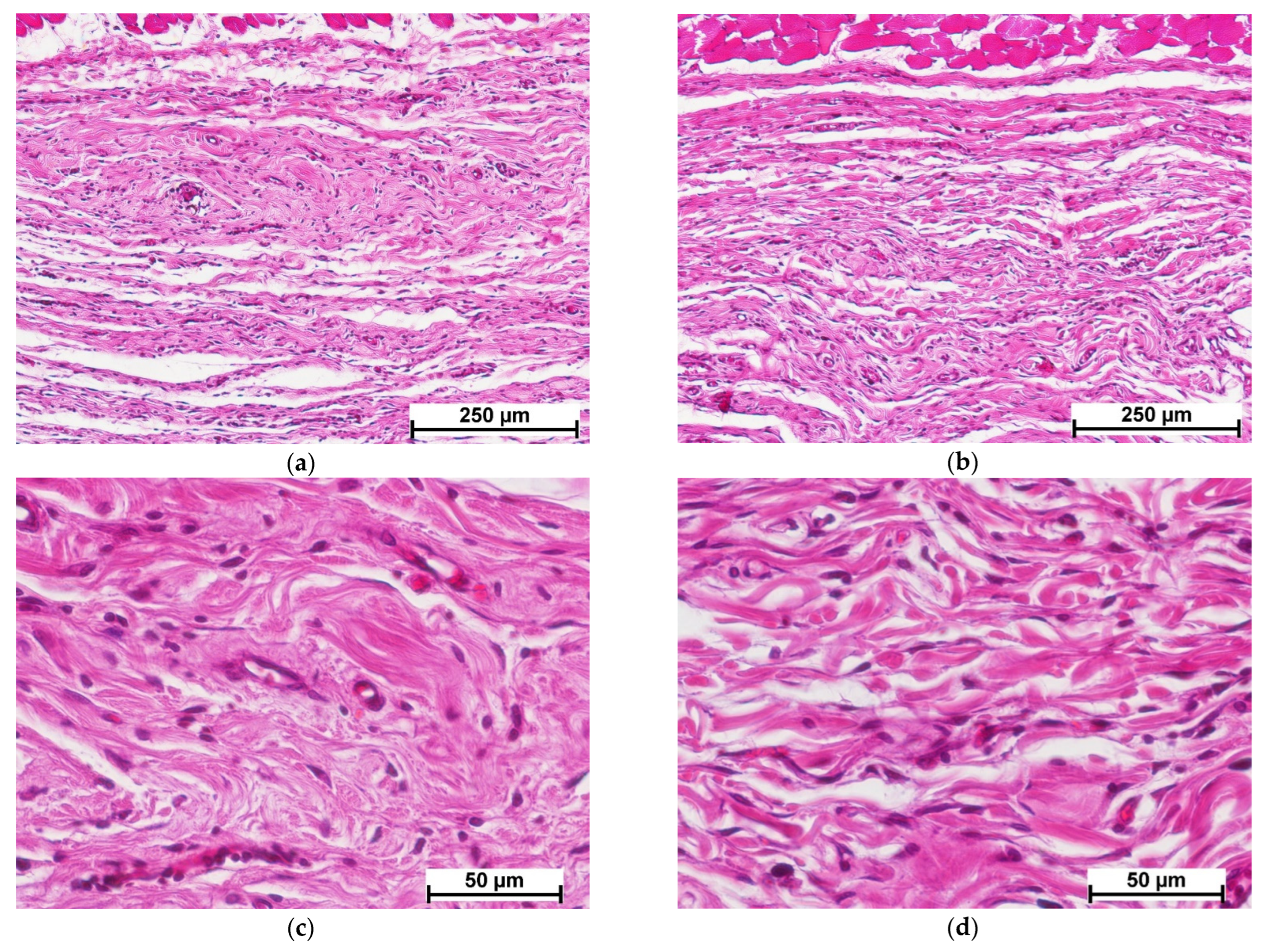
3.3. Morphological Analysis of Results for Implants Containing MSCs
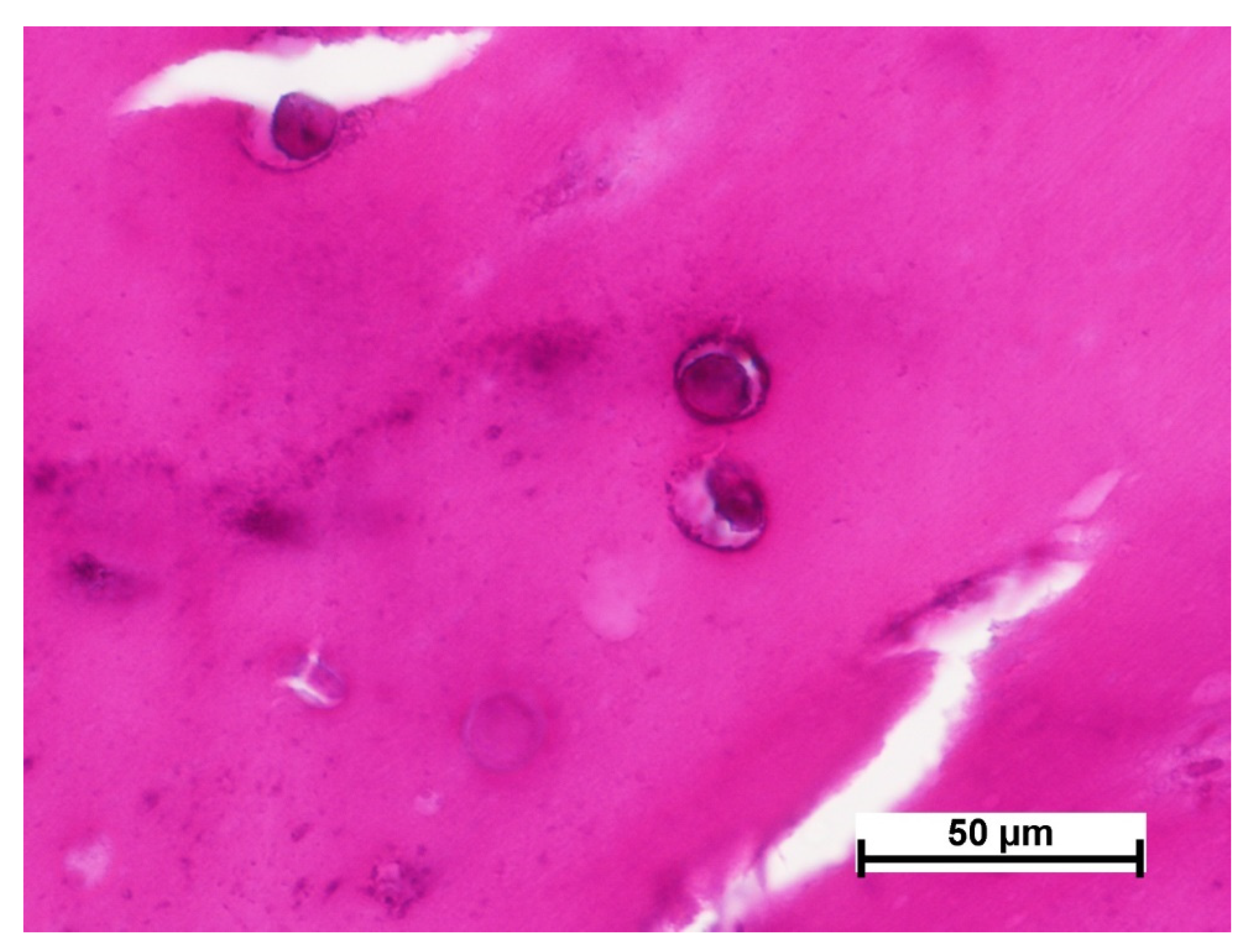
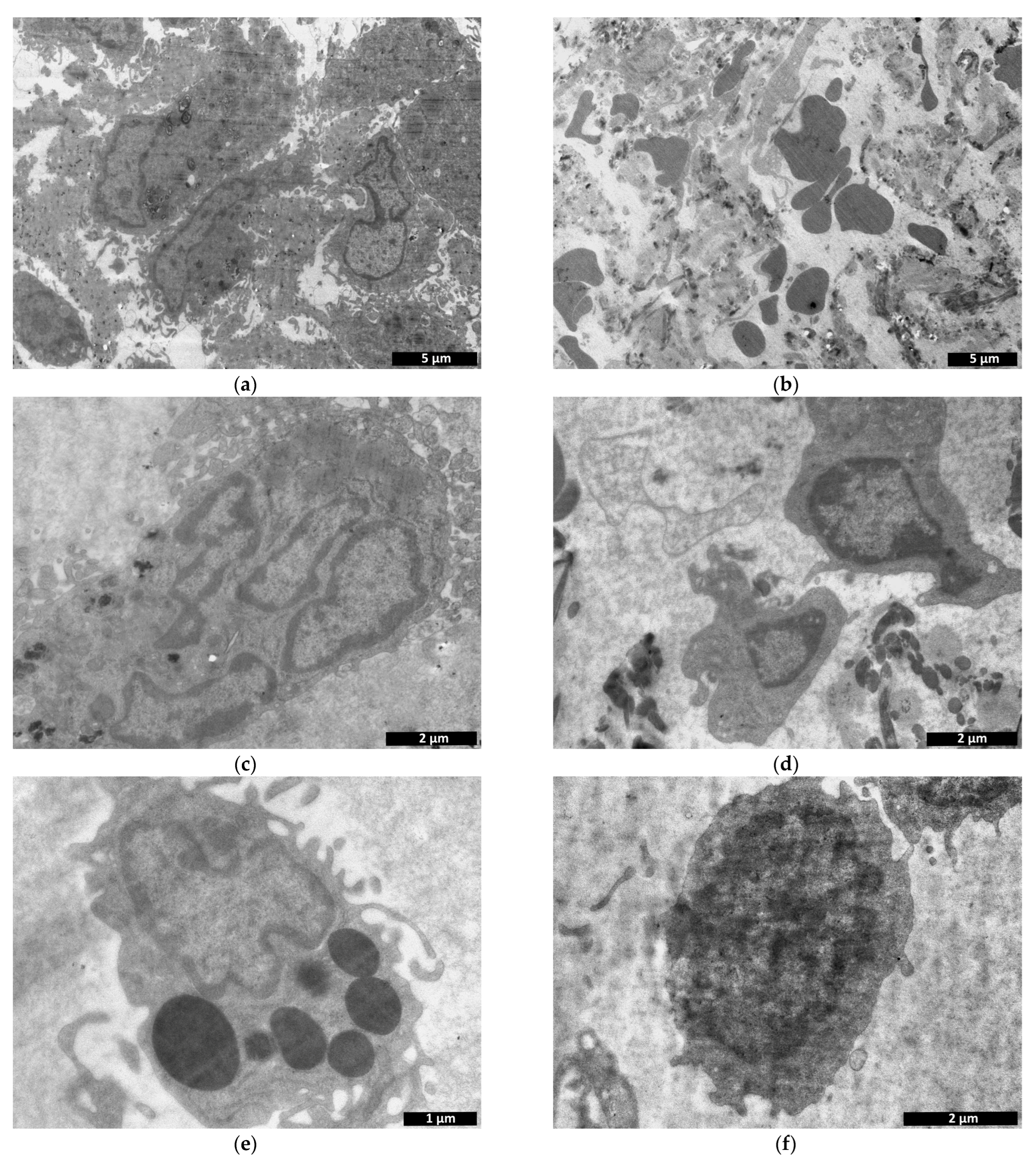
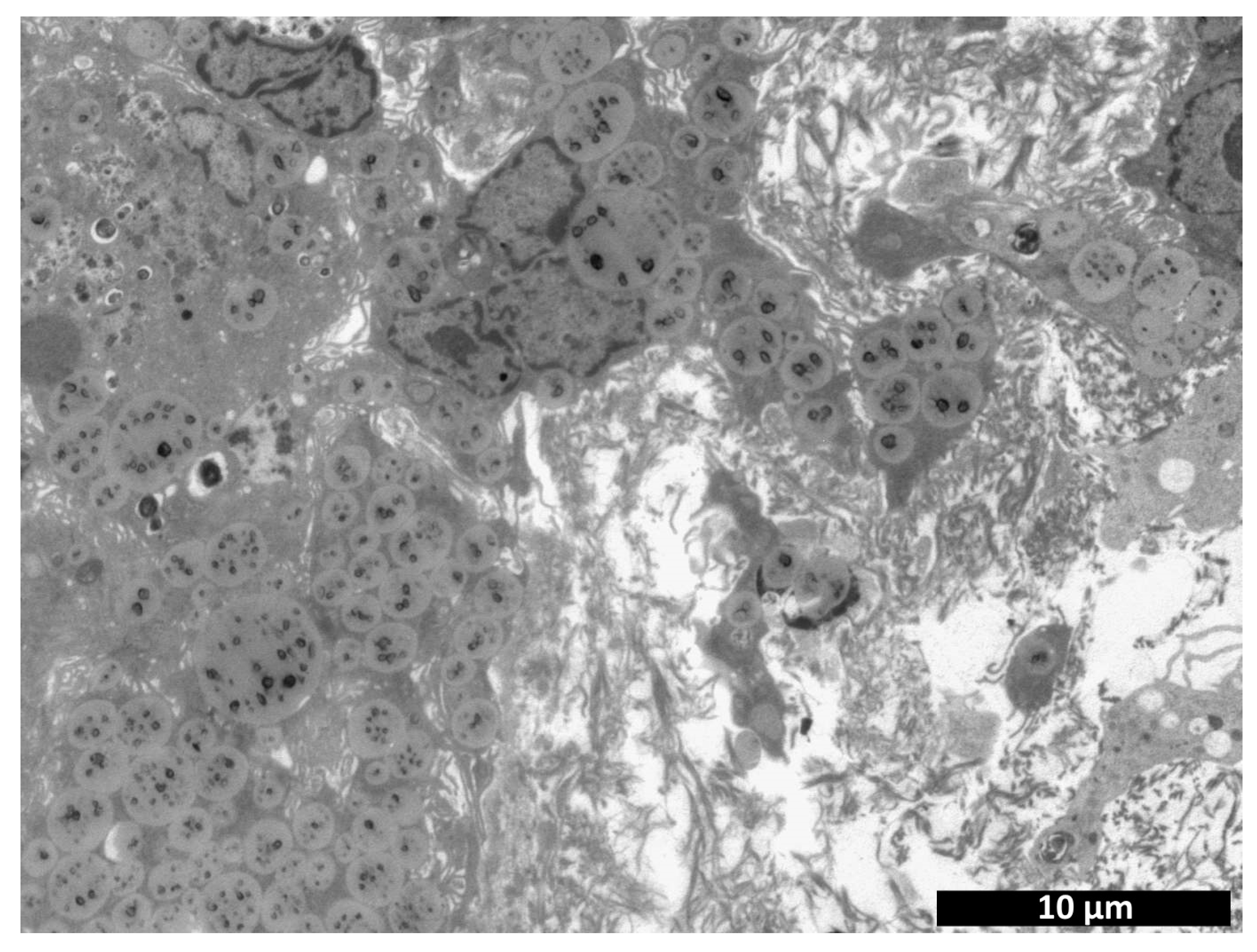
3.4. Biotransformation of Cell-Containing Scaffolds
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sharma, P.; Kumar, P.; Sharma, R.; Bhatt, V.D.; Dhot, P. Tissue Engineering; Current Status & Futuristic Scope. J. Med. Life 2019, 12, 225–229. [Google Scholar] [CrossRef]
- ISO 10993-6-2021 Medical Devices; Biological Evaluation of Medical Devices—Part 6: Tests for Local Effects after Implantation. ISO: Geneva, Switzerland, 2021.
- Tyan, Y.C.; Yang, M.H.; Chang, C.C.; Chung, T.W. Biocompatibility of Materials for Biomedical Engineering. Adv. Exp. Med. Biol. 2020, 1250, 125–140. [Google Scholar] [PubMed]
- Egorikhina, M.N.; Rubtsova, Y.P.; Charykova, I.N.; Bugrova, M.L.; Bronnikova, I.I.; Mukhina, P.A.; Sosnina, L.N.; Aleynik, D.Y. Biopolymer Hydrogel Scaffold as an Artificial Cell Niche for Mesenchymal Stem Cells. Polymers 2020, 12, 2550. [Google Scholar] [CrossRef]
- Sadeghi-Ataabadi, M.; Mostafavi-pour, Z.; Vojdani, Z.; Sani, M.; Latifi, M.; Talaei-Khozani, T. Fabrication and characterization of platelet-rich plasma scaffolds for tissue engineering applications. Mater. Sci. Eng. 2017, 71, 372–380. [Google Scholar] [CrossRef]
- Loh, Q.L.; Choong, C. Three-Dimensional Scaffolds for Tissue Engineering Applications: Role of Porosity and Pore Size. Tissue Eng. 2013, 19, 485–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alonso, J.L.; Goldmann, W.H. Cellular mechanotransduction. AIMS Biophys. 2016, 3, 50–62. [Google Scholar] [CrossRef]
- Egorikhina, M.N.; Aleinik, D.Y.; Rubtsova, Y.P.; Charykova, I.N.; Struchcov, A.A.; Ezhevskaya, A.A.; Zagrekov, V.I.; Sosnina, L.N.; Zagaynova, E.V. Biomedical Cell Product Model for Preclinical Studies Carried out on a Large Laboratory Animal. Vestn. Transpl. I Iskusstv. Organov 2020, 22, 142–156. [Google Scholar] [CrossRef]
- Gottipamula, S.; Sridhar, K.N. Clinical Translation of Tissue Engineered Medicinal Products. J. Stem Cell Regen. Biol. 2016, 2, 38–51. [Google Scholar]
- Niemeyer, P.; Szalay, K.; Luginbühl, R.; Südkamp, N.P.; Kasten, P. Transplantation of human mesenchymal stem cells in a non-autogenous setting for bone regeneration in a rabbit critical-size defect model. Acta Biomater. 2010, 6, 900–908. [Google Scholar] [CrossRef]
- Mair, K.H.; Sedlak, C.; Käser, T.; Pasternak, A.; Levast, B.; Gerner, W. The porcine innate immune system: An update. Dev. Comp. Immunol. 2014, 45, 321–343. [Google Scholar] [CrossRef]
- Summerfield, A.; Meurens, F.; Ricklin, M.E. The immunology of the porcine skin and its value as a model for human skin. Mol. Immunol. 2015, 66, 14–21. [Google Scholar] [CrossRef]
- Crawford, L.; Wyatt, M.; Bryers, J.; Ratner, B. Biocompatibility Evolves: Phenomenology to Toxicology to Regeneration. Adv. Healthc. Mater. 2021, 10, e2002153. [Google Scholar] [CrossRef]
- Ghaemi, R.V.; Siang, L.C.; Yadav, V.G. Improving the Rate of Translation of Tissue Engineering Products. Adv. Healthc. Mater. 2019, 8, e1900538. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Lv, H.; Du, Y.; Zhu, W.; Yang, W.; Wang, X.; Wang, J.; Chen, W. Biologically Modified Implantation as Therapeutic Bioabsorbable Materials for Bone Defect Repair. Regen. Ther. 2022, 19, 9–23. [Google Scholar] [CrossRef]
- Tesfamariam, B. Bioresorbable Vascular Scaffolds: Biodegradation, Drug Delivery and Vascular Remodeling. Pharmacol. Res. 2016, 107, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Saad, B. Qasim In-vitro and in-vivo degradation studies of freeze gelated porous chitosan composite scaffolds for tissue engineering applications. Polym. Degrad. Stab. 2017, 136, 31–38. [Google Scholar]
- Talacua, H.; Söntjens, S.H.M.; Thakkar, S.H.; Brizard, A.M.A.; van Herwerden, L.A.; Vink, A.; van Almen, G.C.; Dankers, P.Y.W.; Carlijn, V.C.; Budde, B.R.P.J.; et al. Imaging the In Vivo Degradation of Tissue Engineering Implants by Use of Supramolecular Radiopaque Biomaterials. Macromol. Biosci. 2020, 20, 2000024. [Google Scholar] [CrossRef]
- De Girolamo, L.; Ragni, E.; Cucchiarini, M.; Van Bergen, C.J.; Hunziker, E.B.; Chubinskaya, S. Cells, soluble factors and matrix harmonically play the concert of allograft integration. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 1717–1725. [Google Scholar] [CrossRef]
- McBane, J.E.; Sharifpoor, S.; Cai, K.; Labow, R.S.; Santerre, J.P. Biodegradation and in vivo biocompatibility of a degradable, polar/hydrophobic/ionic polyurethane for tissue engineering applications. Biomaterials 2011, 32, 6034–6044. [Google Scholar] [CrossRef]
- Chandra, G.; Pandey, A. Biodegradable Bone Implants in Orthopedic Applications: A Review. Biocybern. Biomed. Eng. 2020, 40, 596–610. [Google Scholar] [CrossRef]
- Zhang, F.; King, M.W. Biodegradable Polymers as the Pivotal Player in the Design of Tissue Engineering Scaffolds. Adv. Healthc. Mater. 2020, 9, 1901358. [Google Scholar] [CrossRef] [PubMed]
- Egorikhina, M.N.; Levin, G.Y.; Charykova, I.N.; Alejnik, D.Y.; Sosnina, L.N. Method for Creating a Bioresorbable Cellular Scaffold Based on Fibrin of Blood. Plasma. Patent No. 653434 RU, 8 May 2018. [Google Scholar]
- Semenycheva, L.L.; Astanina, M.V.; Kuznetsova, J.L.; Valetova, N.B.; Geras’kina, E.V.; Tarankova, O.A. Method for Production of Acetic Dispersion of High Molecular Fish. Collagen. Patent 2567171, 10 November 2015. [Google Scholar]
- Tracy, L.E.; Minasian, R.A.; Caterson, E.J. Extracellular Matrix and Dermal Fibroblast Function in the Healing Wound. Adv Wound Care 2016, 5, 119–136. [Google Scholar] [CrossRef] [PubMed]
- Diller, R.B.; Tabor, A.J. The Role of the Extracellular Matrix (ECM) in Wound Healing: A Review. Biomimetics 2022, 7, 87. [Google Scholar] [CrossRef]
- Shafiee, A.; Atala, A. Tissue engineering: Toward a new era of medicine. Annu. Rev. Med. 2016, 68, 29–40. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, V.; Maroufi, N.F.; Saghati, S.; Asadi, N.; Darabi, M.; Ahmad, S.N.S.; Hosseini, H.; Reza, R. Current progress in hepatic tissue regeneration by tissue engineering. J. Transl. Med. BioMed. Cent. 2019, 17, 1–24. [Google Scholar] [CrossRef] [Green Version]
- Gerges, I.; Tamplenizza, M.; Martello, F.; Recordati, C.; Martelli, C.; Ottobrini, L.; Tamplenizza, M.; Scott, A.G.; Tocchio, A.; Lenardi, C. Exploring the potential of polyurethane-based soft foam as cell-free scaffold for soft tissue regeneration. Acta Biomater. 2018, 73, 141–153. [Google Scholar] [CrossRef]
- Daviran, M.; Caram, H.S.; Schultz, K.M. Role of Cell-Mediated Enzymatic Degradation and Cytoskeletal Tension on Dynamic Changes in the Rheology of the Pericellular Region Prior to Human Mesenchymal Stem Cell Motility. ACS Biomater. Sci. Eng. 2018, 4, 468–472. [Google Scholar] [CrossRef] [PubMed]
- Egorikhina, M.N.; Bronnikova, I.I.; Rubtsova, Y.P.; Charykova, I.N.; Bugrova, M.L.; Linkova, D.D.; Aleynik, D.Y. Aspects of In Vitro Biodegradation of Hybrid Fibrin–Collagen Scaffolds. Polymers 2021, 13, 3470. [Google Scholar] [CrossRef]
- Shafiq, M.; Jung, Y.; Kim, S.H. Stem Cell Recruitment, Angiogenesis, and Tissue Regeneration in Substance P-Conjugated Poly (l-Lactide-Co-ε-Caprolactone) Nonwoven Meshes. J. Biomed. Mater. Res. Part A 2015, 103, 2673–2688. [Google Scholar] [CrossRef]
- Wang, F.; Cai, X.; Shen, Y.; Meng, L. Cell–Scaffold Interactions in Tissue Engineering for Oral and Craniofacial Reconstruction. Bioact. Mater. 2023, 23, 16–44. [Google Scholar] [CrossRef]
- Chang, C.; Yan, J.; Yao, Z.; Zhang, C.; Li, X.; Mao, H.Q. Effects of Mesenchymal Stem Cell-Derived Paracrine Signals and Their Delivery Strategies. Adv. Healthc. Mater. 2021, 10, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Kusuma, G.D.; Carthew, J.; Lim, R.; Frith, J.E. Effect of the Microenvironment on Mesenchymal Stem Cell Paracrine Signaling: Opportunities to Engineer the Therapeutic Effect. Stem Cells Dev. 2017, 26, 617–631. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Lee, C.W.; Wang, Y.F.; Huang, S.; Shin, L.Y.; Wang, Y.H.; Wan, Z.; Zhu, X.; Yung, P.S.H.; Lee, O.K.S. The Role of Paracrine Regulation of Mesenchymal Stem Cells in the Crosstalk With Macrophages in Musculoskeletal Diseases: A Systematic Review. Front. Bioeng. Biotechnol. 2020, 8, 587052. [Google Scholar] [CrossRef]
- Askari, A.T.; Unzek, S.; Popovic, Z.B.; Goldman, C.K.; Forudi, F.; Kiedrowski, M.; Rovner, A.; Ellis, S.G.; Thomas, J.D.; DiCorleto, P.E.; et al. Effect of Stromal-Cell-Derived Factor 1 on Stem-Cell Homing and Tissue Regeneration in Ischaemic Cardiomyopathy. Lancet 2003, 362, 697–703. [Google Scholar] [CrossRef] [PubMed]
- Ko, I.K.; Ju, Y.M.; Chen, T.; Atala, A.; Yoo, J.J.; Lee, S.J. Combined Systemic and Local Delivery of Stem Cell Inducing/Recruiting Factors for in Situ Tissue Regeneration. FASEB J. 2012, 26, 158–168. [Google Scholar] [CrossRef] [PubMed]
- Yi, B.; Xu, Q.; Liu, W. An Overview of Substrate Stiffness Guided Cellular Response and Its Applications in Tissue Regeneration. Bioact. Mater. 2021, 15, 82–102. [Google Scholar] [CrossRef]
- Zonderland, J.; Moroni, L. Steering Cell Behavior through Mechanobiology in 3D: A Regenerative Medicine Perspective. Biomaterials 2021, 268, 120572. [Google Scholar] [CrossRef]
- Bandzerewicz, A.; Gadomska-Gajadhur, A. Into the Tissues: Extracellular Matrix and Its Artificial Substitutes: Cell Signalling Mechanisms. Cells 2022, 11, 914. [Google Scholar] [CrossRef]
- Bonnans, C.; Chou, J.; Werb, Z. Remodelling the Extracellular Matrix in Development and Disease. Nat. Rev. Mol. Cell Biol. 2014, 15, 786–801. [Google Scholar] [CrossRef]






















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Day | Percentage of the Implant Structure-Forming Portion to the Total Area of Analyzed Image | |
|---|---|---|
| CM | CCS | |
| day 3 | 69.86 ± 1.41 | 75.73 ± 2.01 ▲ |
| day 7 | 69.52 ± 2.86 | 80.72 ± 2.37 ● * |
| day 14 | 83.46 ± 1.92 ▲ ● | 88.85 ± 1.25 ♦ * ○ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Egorikhina, M.N.; Timofeeva, L.B.; Linkova, D.D.; Rubtsova, Y.P.; Bugrova, M.L.; Charykova, I.N.; Ryabkov, M.G.; Kobyakova, I.I.; Farafontova, E.A.; Aleynik, D.Y. Biocompatibility Study of Hydrogel Biopolymer Scaffold with Encapsulated Mesenchymal Stem Cells. Polymers 2023, 15, 1337. https://doi.org/10.3390/polym15061337
Egorikhina MN, Timofeeva LB, Linkova DD, Rubtsova YP, Bugrova ML, Charykova IN, Ryabkov MG, Kobyakova II, Farafontova EA, Aleynik DY. Biocompatibility Study of Hydrogel Biopolymer Scaffold with Encapsulated Mesenchymal Stem Cells. Polymers. 2023; 15(6):1337. https://doi.org/10.3390/polym15061337
Chicago/Turabian StyleEgorikhina, Marfa N., Lidia B. Timofeeva, Daria D. Linkova, Yulia P. Rubtsova, Marina L. Bugrova, Irina N. Charykova, Maxim G. Ryabkov, Irina I. Kobyakova, Ekaterina A. Farafontova, and Diana Y. Aleynik. 2023. "Biocompatibility Study of Hydrogel Biopolymer Scaffold with Encapsulated Mesenchymal Stem Cells" Polymers 15, no. 6: 1337. https://doi.org/10.3390/polym15061337