
Dislodgment Resistance, Adhesive Pattern, and Dentinal Tubule Penetration of a Novel Experimental Algin Biopolymer-Incorporated Bioceramic-Based Root Canal Sealer

 , ,
, ,
Abstract
:1. Introduction
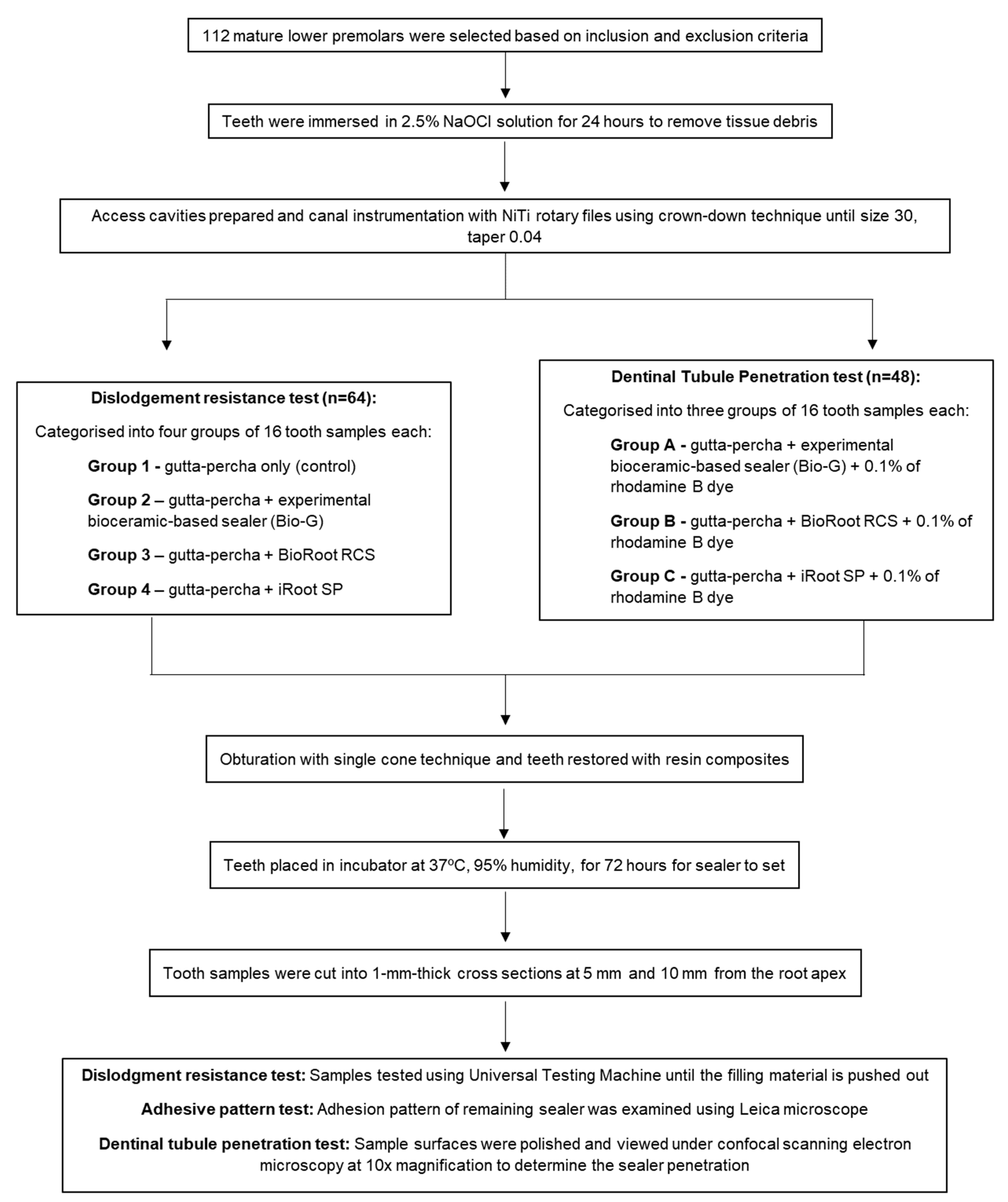
2. Materials and Methods
2.1. Sample Size Calculation
2.2. Sample Preparation
2.3. Dislodgment Resistance Test
2.4. Adhesive Pattern Test
2.5. Dentinal Tubule Penetration Test
2.6. Statistical Analysis
3. Results
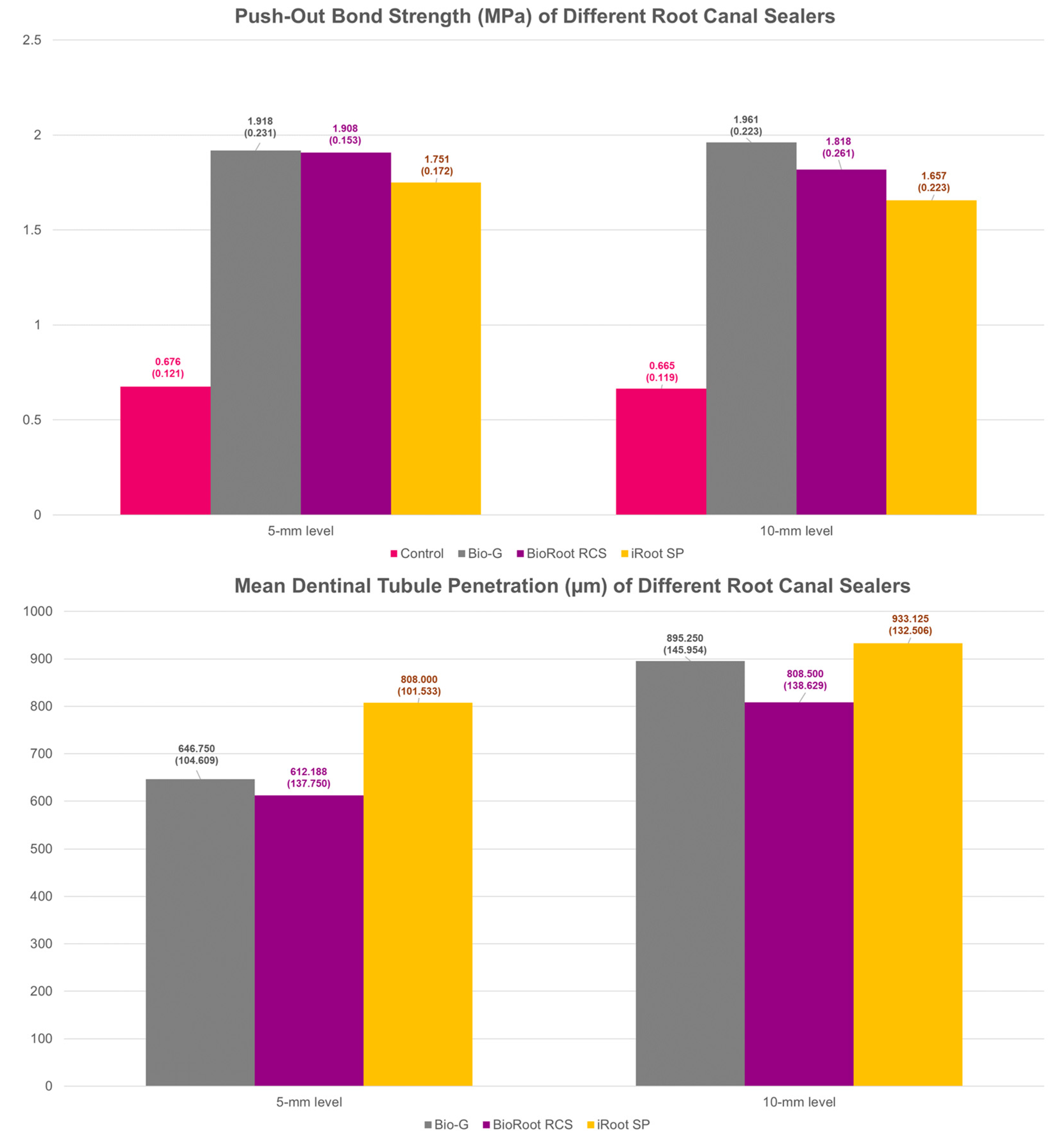
3.1. Dislodgment Resistance
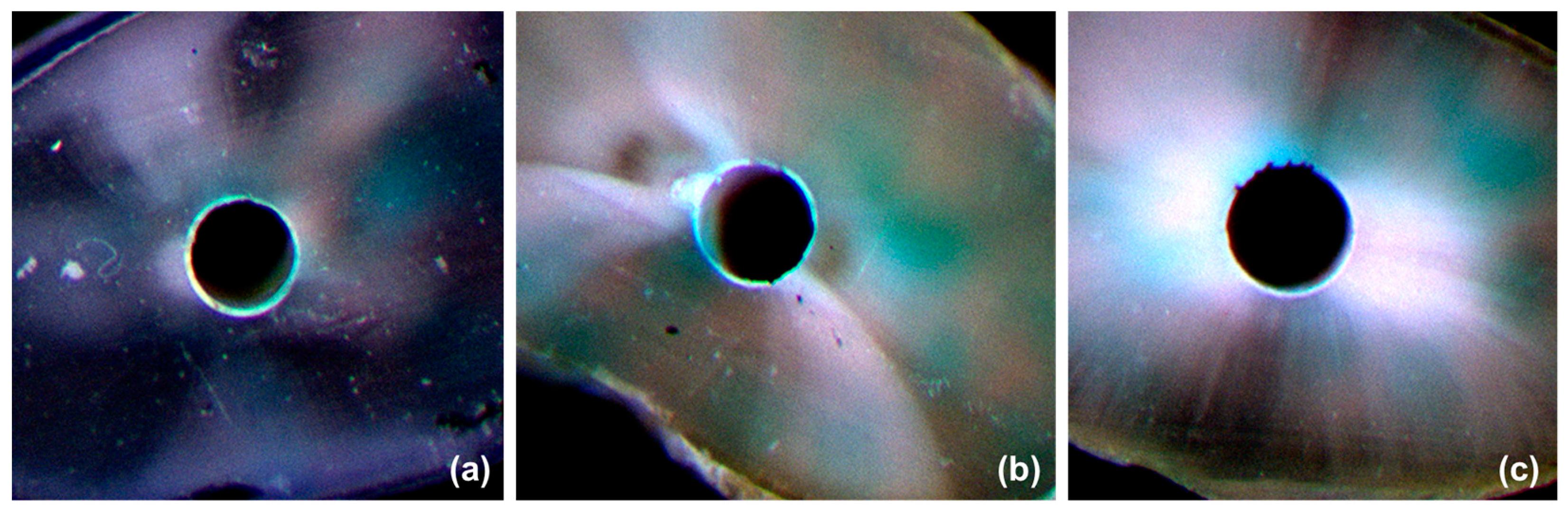
3.2. Adhesive Pattern
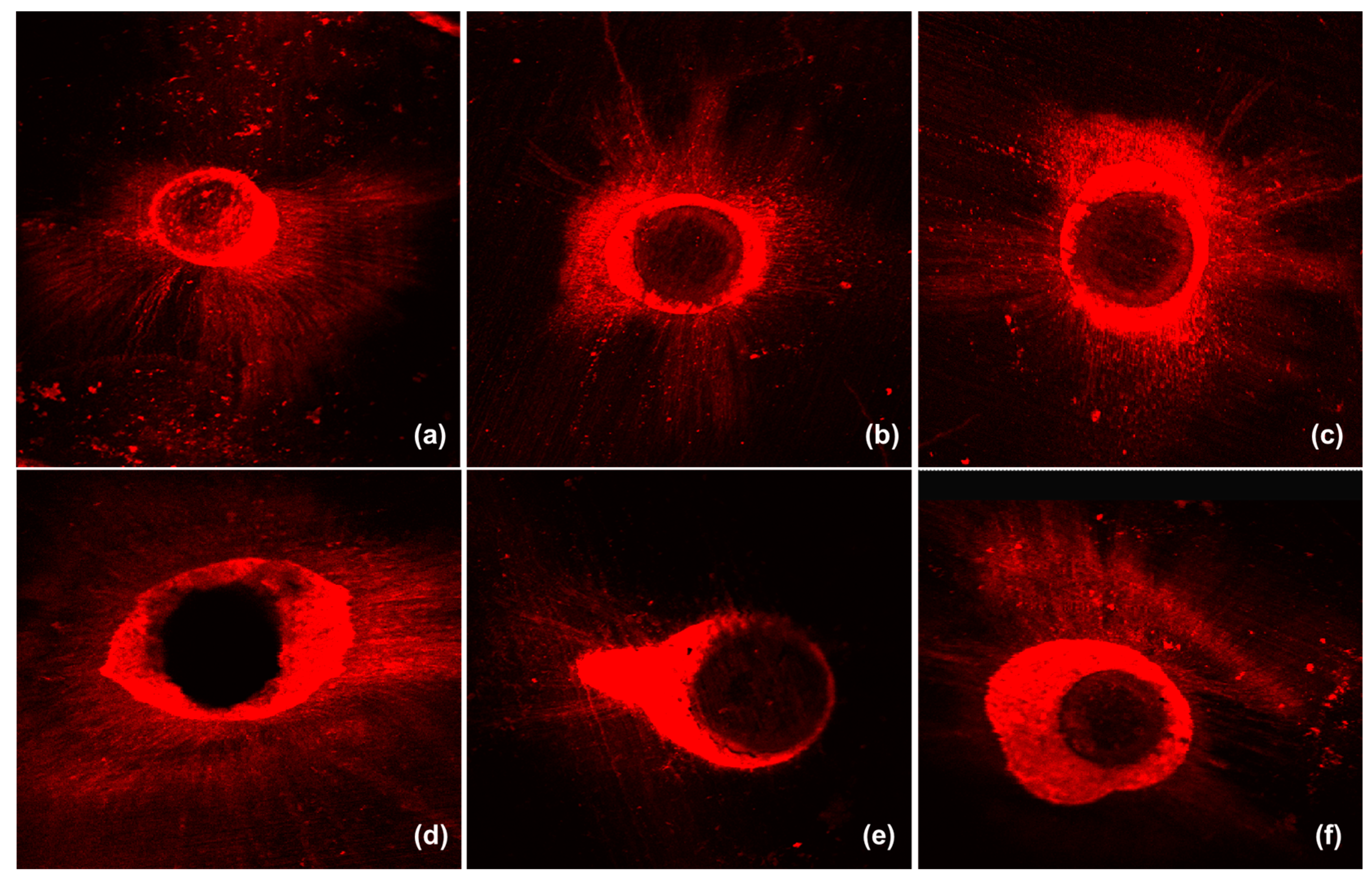
3.3. Dentinal Tubule Penetration
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lin, G.S.S.; Ghani, N.; Noorani, T.Y.; Ismail, N.H.; Mamat, N. Dislodgement resistance and adhesive pattern of different endodontic sealers to dentine wall after artificial ageing: An in-vitro study. Odontology 2021, 109, 149–156. [Google Scholar] [CrossRef] [PubMed]
- El Hachem, R.; Khalil, I.; Le Brun, G.; Pellen, F.; Le Jeune, B.; Daou, M.; El Osta, N.; Naaman, A.; Abboud, M. Dentinal tubule penetration of AH Plus, BC Sealer and a novel tricalcium silicate sealer: A confocal laser scanning microscopy study. Clin. Oral Investig. 2019, 23, 1871–1876. [Google Scholar] [CrossRef] [PubMed]
- Donnermeyer, D.; Dornseifer, P.; Schafer, E.; Dammaschke, T. The push-out bond strength of calcium silicate-based endodontic sealers. Head Face Med. 2018, 14, 13. [Google Scholar] [CrossRef]
- Jeong, J.W.; DeGraft-Johnson, A.; Dorn, S.O.; Di Fiore, P.M. Dentinal Tubule Penetration of a Calcium Silicate-based Root Canal Sealer with Different Obturation Methods. J. Endod. 2017, 43, 633–637. [Google Scholar] [CrossRef] [PubMed]
- Tomson, R.M.; Polycarpou, N.; Tomson, P.L. Contemporary obturation of the root canal system. Br. Dent. J. 2014, 216, 315–322. [Google Scholar] [CrossRef] [Green Version]
- Mekhdieva, E.; Del Fabbro, M.; Alovisi, M.; Comba, A.; Scotti, N.; Tumedei, M.; Carossa, M.; Berutti, E.; Pasqualini, D. Postoperative Pain following Root Canal Filling with Bioceramic vs. Traditional Filling Techniques: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2021, 10, 4509. [Google Scholar] [CrossRef]
- Kim, Y.; Kim, B.S.; Kim, Y.M.; Lee, D.; Kim, S.Y. The Penetration Ability of Calcium Silicate Root Canal Sealers into Dentinal Tubules Compared to Conventional Resin-Based Sealer: A Confocal Laser Scanning Microscopy Study. Materials 2019, 12, 531. [Google Scholar] [CrossRef] [Green Version]
- Parirokh, M.; Torabinejad, M. Mineral trioxide aggregate: A comprehensive literature review—Part III: Clinical applications, drawbacks, and mechanism of action. J. Endod. 2010, 36, 400–413. [Google Scholar] [CrossRef]
- Oliveira, D.S.; Cardoso, M.L.; Queiroz, T.F.; Silva, E.J.; Souza, E.M.; De-Deus, G. Suboptimal push-out bond strengths of calcium silicate-based sealers. Int. Endod. J. 2016, 49, 796–801. [Google Scholar] [CrossRef]
- Ersahan, S.; Aydin, C. Dislocation resistance of iRoot SP, a calcium silicate-based sealer, from radicular dentine. J. Endod. 2010, 36, 2000–2002. [Google Scholar] [CrossRef]
- Siboni, F.; Taddei, P.; Zamparini, F.; Prati, C.; Gandolfi, M.G. Properties of BioRoot RCS, a tricalcium silicate endodontic sealer modified with povidone and polycarboxylate. Int. Endod. J. 2017, 50 (Suppl. S2), e120–e136. [Google Scholar] [CrossRef] [Green Version]
- Lim, M.; Jung, C.; Shin, D.H.; Cho, Y.B.; Song, M. Calcium silicate-based root canal sealers: A literature review. Restor. Dent. Endod. 2020, 45, e35. [Google Scholar] [CrossRef]
- Lin, G.S.S.; Sim, D.H.H.; Luddin, N.; Lai, J.C.H.; Ghani, H.A.; Noorani, T.Y. Fabrication and characterisation of novel algin incorporated bioactive-glass 58S calcium-silicate-based root canal sealer. J. Dent. Sci. 2022, in press. [Google Scholar] [CrossRef]
- Ching, S.H.; Bansal, N.; Bhandari, B. Alginate gel particles—A review of production techniques and physical properties. Crit. Rev. Food Sci. Nutr. 2017, 57, 1133–1152. [Google Scholar] [CrossRef] [PubMed]
- Lin, G.S.S.; Cher, C.Y.; Goh, Y.H.; Chan, D.Z.K.; Karobari, M.I.; Lai, J.C.H.; Noorani, T.Y. An Insight into the Role of Marine Biopolymer Alginate in Endodontics: A Review. Mar. Drugs 2022, 20, 539. [Google Scholar] [CrossRef] [PubMed]
- Yadav, P.; Yadav, H.; Shah, V.G.; Shah, G.; Dhaka, G. Biomedical Biopolymers, their Origin and Evolution in Biomedical Sciences: A Systematic Review. J. Clin. Diagn. Res. 2015, 9, ZE21–ZE25. [Google Scholar] [CrossRef]
- Lee, K.Y.; Mooney, D.J. Alginate: Properties and biomedical applications. Prog. Polym. Sci. 2012, 37, 106–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ungor, M.; Onay, E.O.; Orucoglu, H. Push-out bond strengths: The Epiphany-Resilon endodontic obturation system compared with different pairings of Epiphany, Resilon, AH Plus and gutta-percha. Int. Endod. J. 2006, 39, 643–647. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Shen, Y.; Haapasalo, M. Dentin extends the antibacterial effect of endodontic sealers against Enterococcus faecalis biofilms. J. Endod. 2014, 40, 505–508. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Lin, G.S.S.; Ghani, N.; Noorani, T.Y. The existence of butterfly effect and its impact on the dentinal microhardness and crack formation after root canal instrumentation. Odontology 2021, 109, 672–678. [Google Scholar] [CrossRef] [PubMed]
- Shokouhinejad, N.; Gorjestani, H.; Nasseh, A.A.; Hoseini, A.; Mohammadi, M.; Shamshiri, A.R. Push-out bond strength of gutta-percha with a new bioceramic sealer in the presence or absence of smear layer. Aust. Endod. J. 2013, 39, 102–106. [Google Scholar] [CrossRef]
- Coronas, V.S.; Villa, N.; Nascimento, A.L.D.; Duarte, P.H.M.; Rosa, R.A.D.; So, M.V.R. Dentinal Tubule Penetration of a Calcium Silicate-Based Root Canal Sealer Using a Specific Calcium Fluorophore. Braz. Dent. J. 2020, 31, 109–115. [Google Scholar] [CrossRef]
- Tuncel, B.; Nagas, E.; Cehreli, Z.; Uyanik, O.; Vallittu, P.; Lassila, L. Effect of endodontic chelating solutions on the bond strength of endodontic sealers. Braz. Oral Res. 2015, 29, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Al-Haddad, A.; Che Ab Aziz, Z.A. Bioceramic-Based Root Canal Sealers: A Review. Int. J. Biomater. 2016, 2016, 9753210. [Google Scholar] [CrossRef] [Green Version]
- Jainaen, A.; Palamara, J.E.; Messer, H.H. Push-out bond strengths of the dentine-sealer interface with and without a main cone. Int. Endod. J. 2007, 40, 882–890. [Google Scholar] [CrossRef]
- Pane, E.S.; Palamara, J.E.; Messer, H.H. Critical evaluation of the push-out test for root canal filling materials. J. Endod. 2013, 39, 669–673. [Google Scholar] [CrossRef] [PubMed]
- Lin, G.S.S.; Leong, J.Z.; Toh, E.Y.J.; Leow, Y.S.; Pillai, M.P.M.; Teoh, H.S.; Luddin, N.; Noorani, T.Y. Do different irrigating solutions affect the dislodgement resistance of bioceramic-based root canal sealers? A systematic review and meta-analysis. J. Adhes. Sci. Technol. 2022, in press. [Google Scholar] [CrossRef]
- Daemi, H.; Barikani, M. Synthesis and characterization of calcium alginate nanoparticles, sodium homopolymannuronate salt and its calcium nanoparticles. Sci. Iran. 2012, 19, 2023–2028. [Google Scholar] [CrossRef] [Green Version]
- Craig, R.G.; Ward, M.L. Restorative Dental Materials; Mosby: Maryland Heights, MO, USA, 1997. [Google Scholar]
- Kenneth, J.; Anusavice, D.; Shen, C.; Rawls, H.R. Phillips’ Science of Dental Materials; Elsevier Health Sciences: Amsterdam, The Netherlands, 2012. [Google Scholar]
- Khalil, I.; Naaman, A.; Camilleri, J. Properties of Tricalcium Silicate Sealers. J. Endod. 2016, 42, 1529–1535. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Liu, S.; Dong, Y. In vitro study of dentinal tubule penetration and filling quality of bioceramic sealer. PLoS ONE 2018, 13, e0192248. [Google Scholar] [CrossRef] [PubMed]
- Akcay, M.; Arslan, H.; Durmus, N.; Mese, M.; Capar, I.D. Dentinal tubule penetration of AH Plus, iRoot SP, MTA fillapex, and guttaflow bioseal root canal sealers after different final irrigation procedures: A confocal microscopic study. Lasers Surg. Med. 2016, 48, 70–76. [Google Scholar] [CrossRef]
- Aktemur Turker, S.; Uzunoglu, E.; Purali, N. Evaluation of dentinal tubule penetration depth and push-out bond strength of AH 26, BioRoot RCS, and MTA Plus root canal sealers in presence or absence of smear layer. J. Dent. Res. Dent. Clin. Dent. Prospect. 2018, 12, 294–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.; Zhao, X.; Qiu, Y.; Xu, D.; Cui, L.; Wu, B. The Tubular Penetration Depth and Adaption of Four Sealers: A Scanning Electron Microscopic Study. BioMed Res. Int. 2017, 2017, 2946524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arikatla, S.K.; Chalasani, U.; Mandava, J.; Yelisela, R.K. Interfacial adaptation and penetration depth of bioceramic endodontic sealers. J. Conserv. Dent. 2018, 21, 373–377. [Google Scholar]
- Lin, G.S.S.; Chan, D.Z.K.; Leong, J.Z.; Kan, Z.; Xuan, W.M.; Tee, V. Dentinal tubule penetration of bioceramic-based versus epoxy resin-based root canal sealers: A systematic review and meta-analysis. G. Ital. Endod. 2021, 36, 11–21. [Google Scholar]
- Chandra, S.S.; Shankar, P.; Indira, R. Depth of penetration of four resin sealers into radicular dentinal tubules: A confocal microscopic study. J. Endod. 2012, 38, 1412–1416. [Google Scholar] [CrossRef]
- Song, D.; Yang, S.-E. Comparison of Dentinal Tubule Penetration between a Calcium Silicate-Based Sealer with Ultrasonic Activation and an Epoxy Resin-Based Sealer: A Study Using Confocal Laser Scanning Microscopy. Eur. J. Dent. 2022, 16, 195–201. [Google Scholar] [CrossRef]
- Mandras, N.; Alovisi, M.; Roana, J.; Crosasso, P.; Luganini, A.; Pasqualini, D.; Genta, E.; Arpicco, S.; Banche, G.; Cuffini, A.; et al. Evaluation of the Bactericidal Activity of a Hyaluronic Acid-Vehicled Clarithromycin Antibiotic Mixture by Confocal Laser Scanning Microscopy. Appl. Sci. 2020, 10, 761. [Google Scholar] [CrossRef]
- Alovisi, M.; Carossa, M.; Mandras, N.; Roana, J.; Costalonga, M.; Cavallo, L.; Pira, E.; Putzu, M.G.; Bosio, D.; Roato, I.; et al. Disinfection and Biocompatibility of Titanium Surfaces Treated with Glycine Powder Airflow and Triple Antibiotic Mixture: An In Vitro Study. Materials 2022, 15, 4850. [Google Scholar] [CrossRef]
- Alovisi, M.; Pasqualini, D.; Mandras, N.; Roana, J.; Costamagna, P.; Comba, A.; Cavalli, R.; Luganini, A.; Iandolo, A.; Cavallo, L.; et al. Confocal Laser Scanner Evaluation of Bactericidal Effect of Chitosan Nanodroplets Loaded with Benzalkonium Chloride. J. Clin. Med. 2022, 11, 1650. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Level | Type of Sealer | p-Values | |||
|---|---|---|---|---|---|
| Control | Bio-G | BioRoot RCS | iRoot SP | ||
| 5 mm | 0.676 ± 0.121 | 1.918 ± 0.231 ○ | 1.908 ± 0.153 ○● | 1.751 ± 0.172 ● | 0.001 * |
| 10 mm | 0.665 ± 0.119 | 1.961 ± 0.223 ◊ | 1.818 ± 0.261 ◊ ♦ | 1.657 ± 0.223 ♦ | 0.001 * |
| Type of Sealer | Type of Adhesive Pattern (n = 16) | p-Value | ||||
|---|---|---|---|---|---|---|
| Non-Adhesive | Adhesive | |||||
| 1 | 2 | 3 | 4 | |||
| 5 mm level | ||||||
| Bio-G | - | - | - | 10 | 6 | 0.001 * |
| BioRoot RCS | - | - | 2 | 9 | 5 | |
| iRoot SP | - | 2 | 11 | 3 | - | |
| 10 mm level | ||||||
| Bio-G | - | - | 1 | 9 | 6 | 0.001 * |
| BioRoot RCS | - | - | 3 | 9 | 4 | |
| iRoot SP | - | 4 | 6 | 4 | 2 | |
| Level | Bio-G | BioRoot RCS | iRoot SP | p-Values |
|---|---|---|---|---|
| Maximum Depths | ||||
| 5 mm | 969.688 ± 78.787 | 906.375 ± 107.248 Ɵ | 1004.500 ± 106.609 Ɵ | 0.023 * |
| 10 mm | 1439.063 ± 97.380 ○ | 1281.625 ± 187.490 | 1484.188 ± 141.990 ○ | 0.001 * |
| Mean Depths | ||||
| 5 mm | 646.750 ± 104.609 ● | 612.188 ± 137.750 ● | 808.000 ± 101.553 | 0.001 * |
| 10 mm | 895.250 ± 145.954 | 808.500 ± 138.629 ╫ | 933.125 ± 132.506 ╫ | 0.043 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, G.S.S.; Luddin, N.; Ghani, H.A.; Lai, J.C.H.; Noorani, T.Y. Dislodgment Resistance, Adhesive Pattern, and Dentinal Tubule Penetration of a Novel Experimental Algin Biopolymer-Incorporated Bioceramic-Based Root Canal Sealer. Polymers 2023, 15, 1317. https://doi.org/10.3390/polym15051317
Lin GSS, Luddin N, Ghani HA, Lai JCH, Noorani TY. Dislodgment Resistance, Adhesive Pattern, and Dentinal Tubule Penetration of a Novel Experimental Algin Biopolymer-Incorporated Bioceramic-Based Root Canal Sealer. Polymers. 2023; 15(5):1317. https://doi.org/10.3390/polym15051317
Chicago/Turabian StyleLin, Galvin Sim Siang, Norhayati Luddin, Huwaina Abd Ghani, Josephine Chang Hui Lai, and Tahir Yusuf Noorani. 2023. "Dislodgment Resistance, Adhesive Pattern, and Dentinal Tubule Penetration of a Novel Experimental Algin Biopolymer-Incorporated Bioceramic-Based Root Canal Sealer" Polymers 15, no. 5: 1317. https://doi.org/10.3390/polym15051317