

Evaluating the Release of Different Commercial Orally Modified Niacin Formulations In Vitro
 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Methods
2.2.1. In Vitro Dissolution Study
2.2.2. Experimental Methods
2.2.3. UV Spectrophotometer Analysis
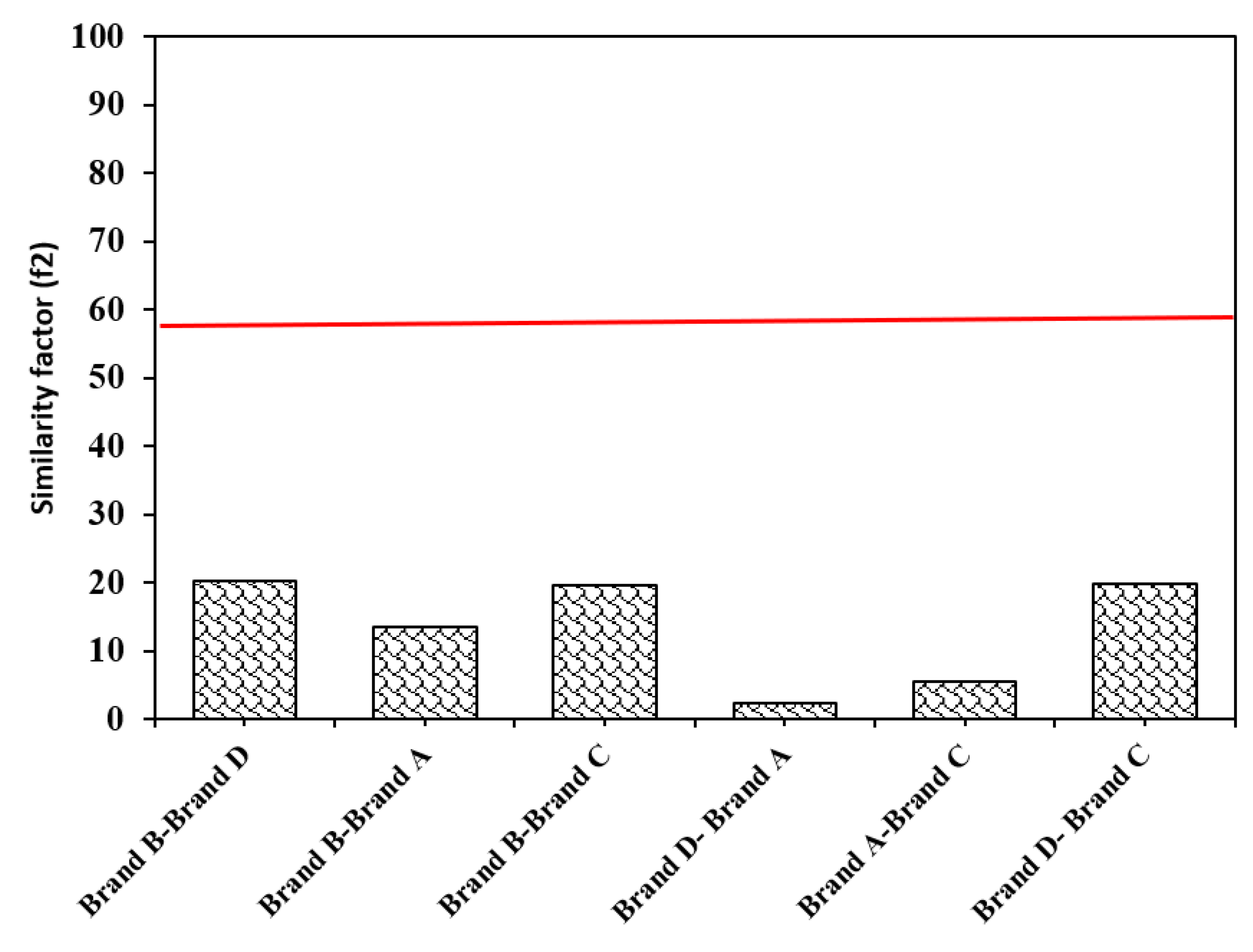
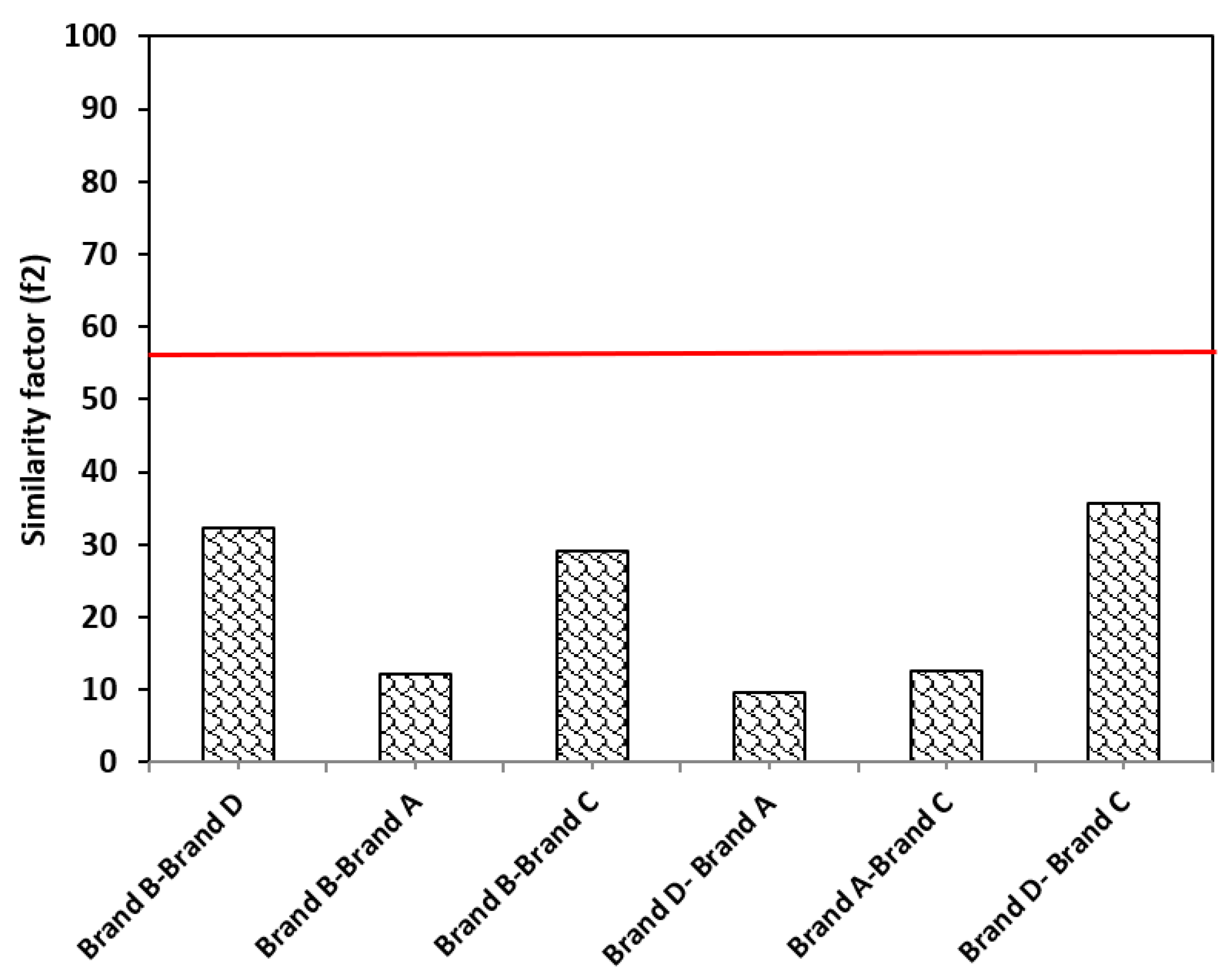
2.2.4. Comparison between Dissolution Profiles Using the f2
3. Results
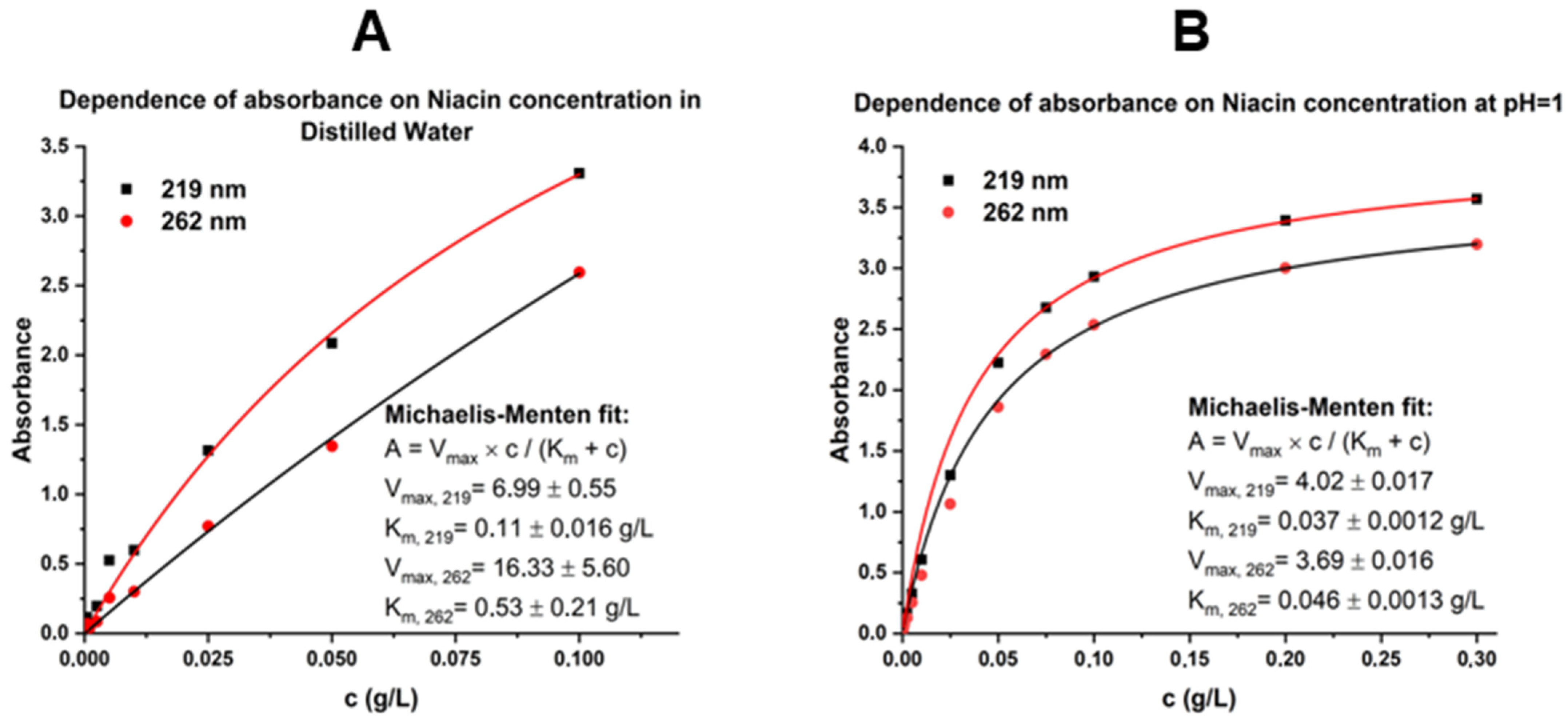
3.1. Determining Niacin Calibration Curves for Concentration Calculation
3.2. Drug Concentration Measurement
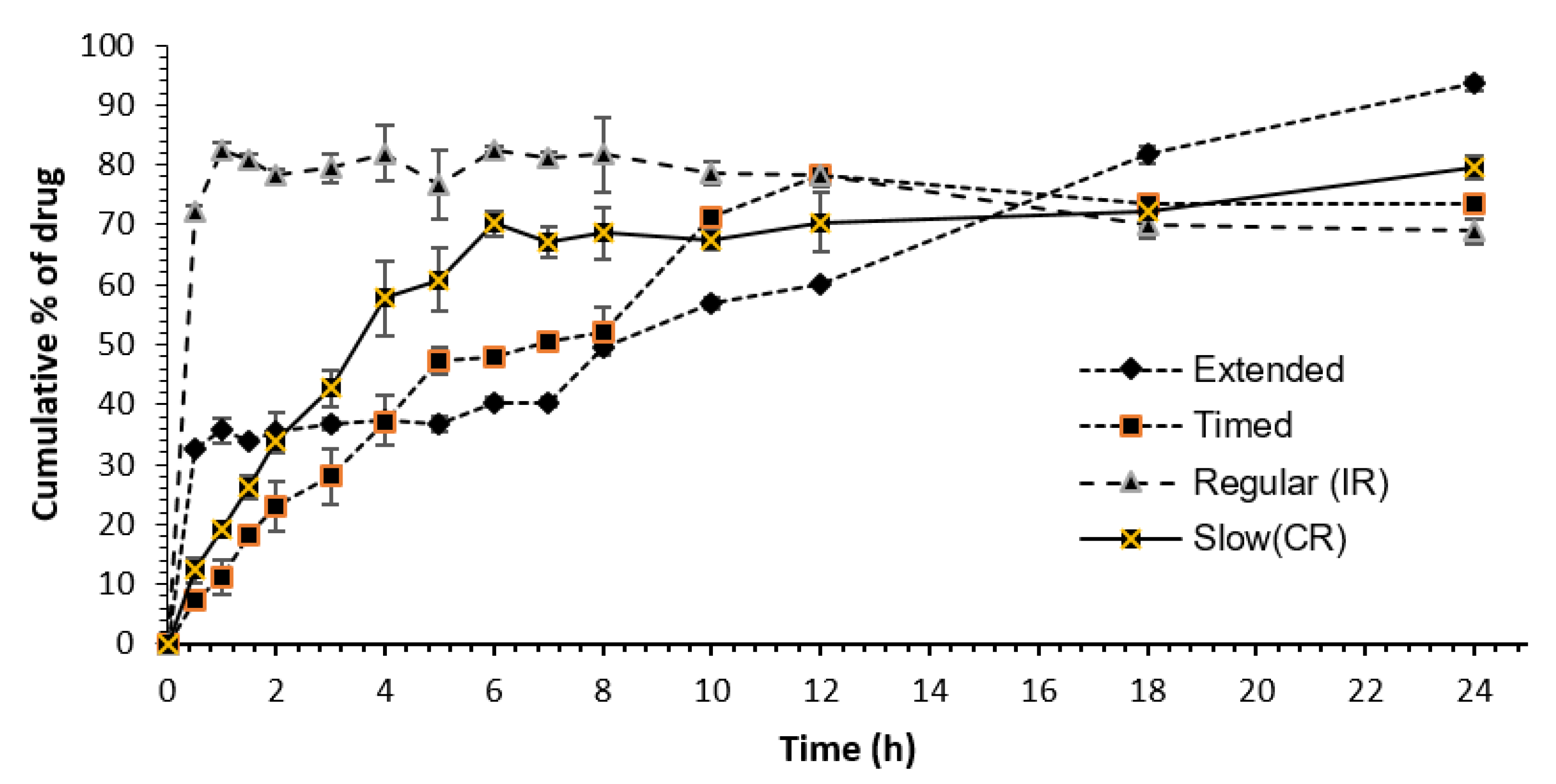
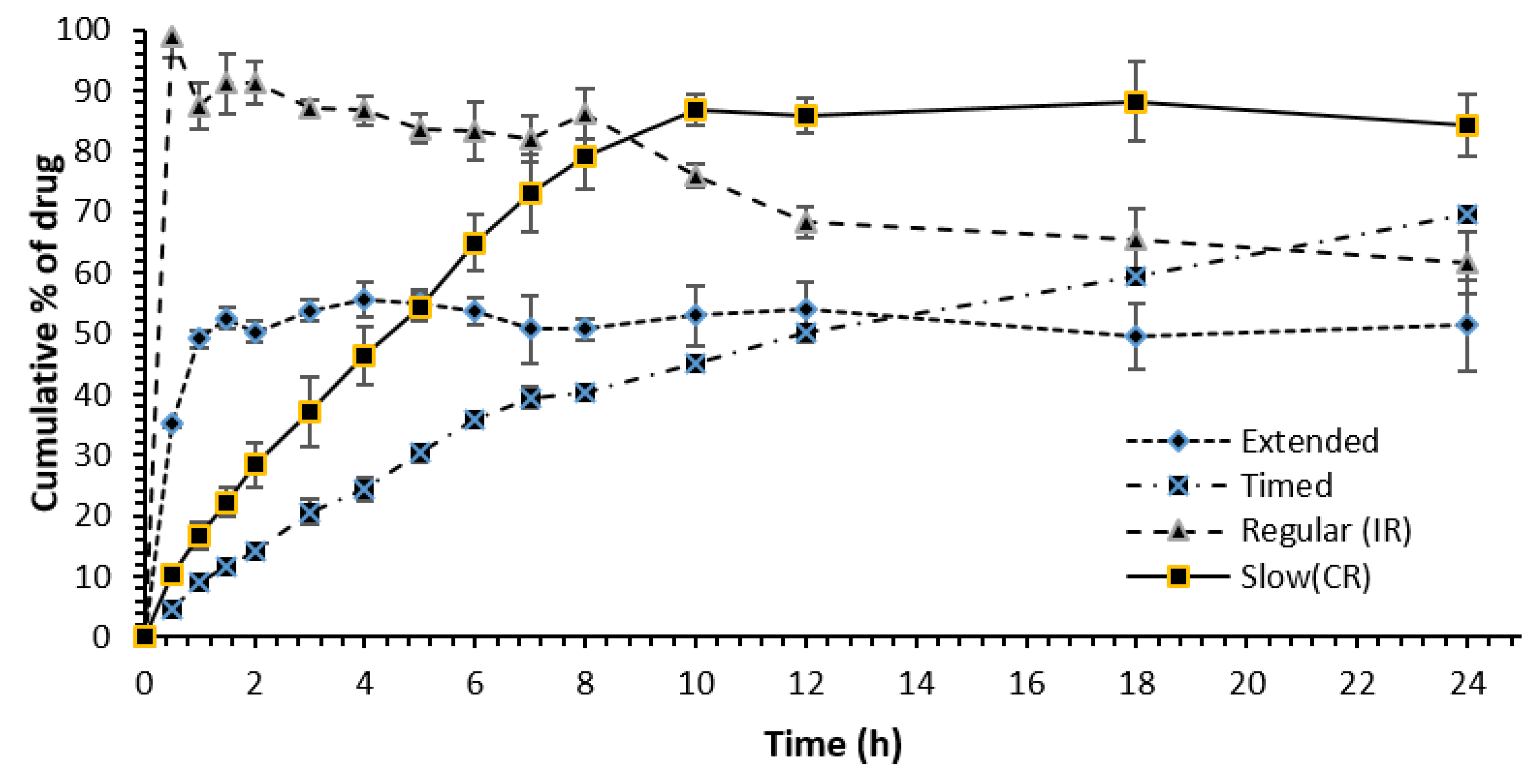
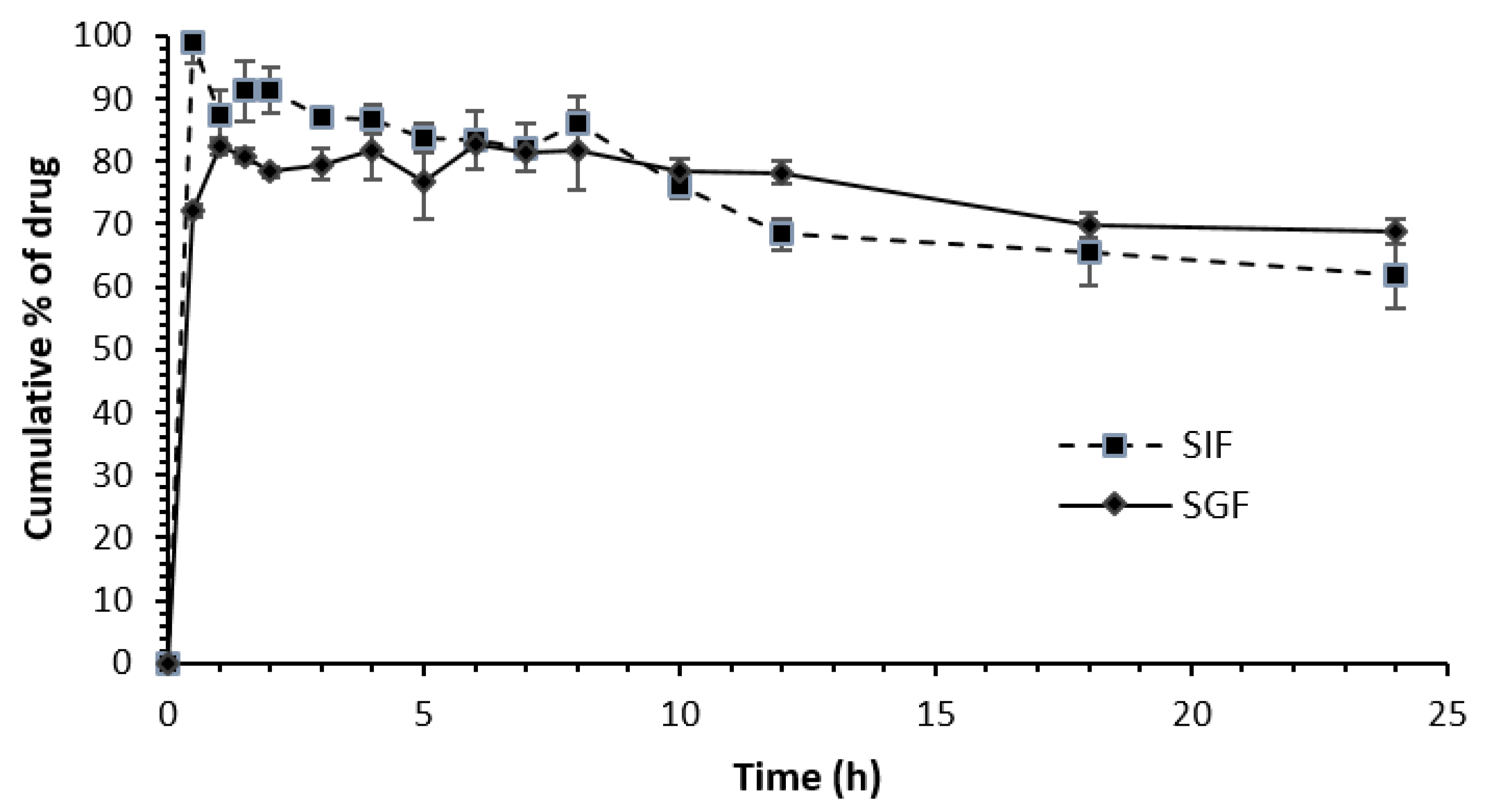
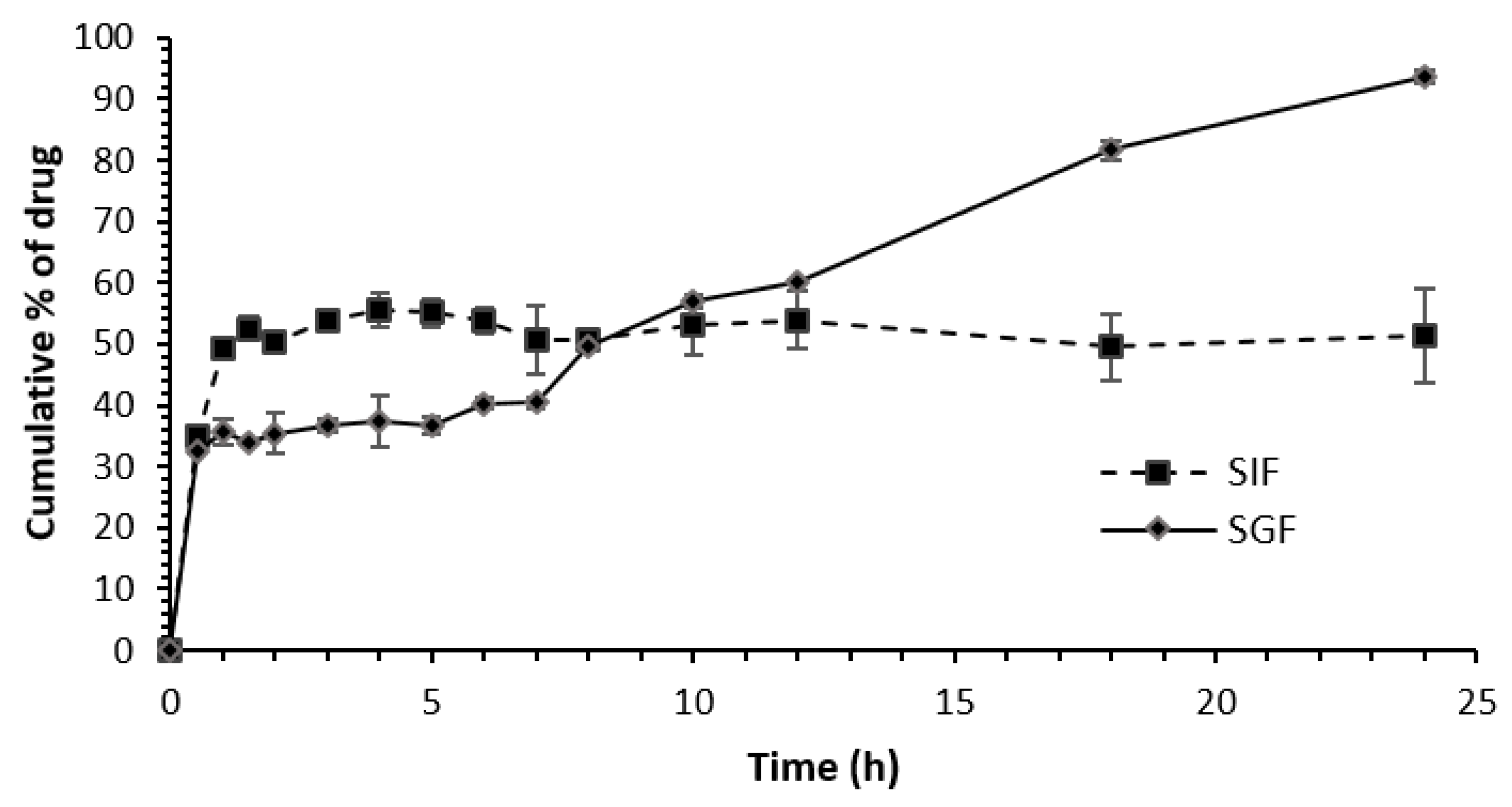
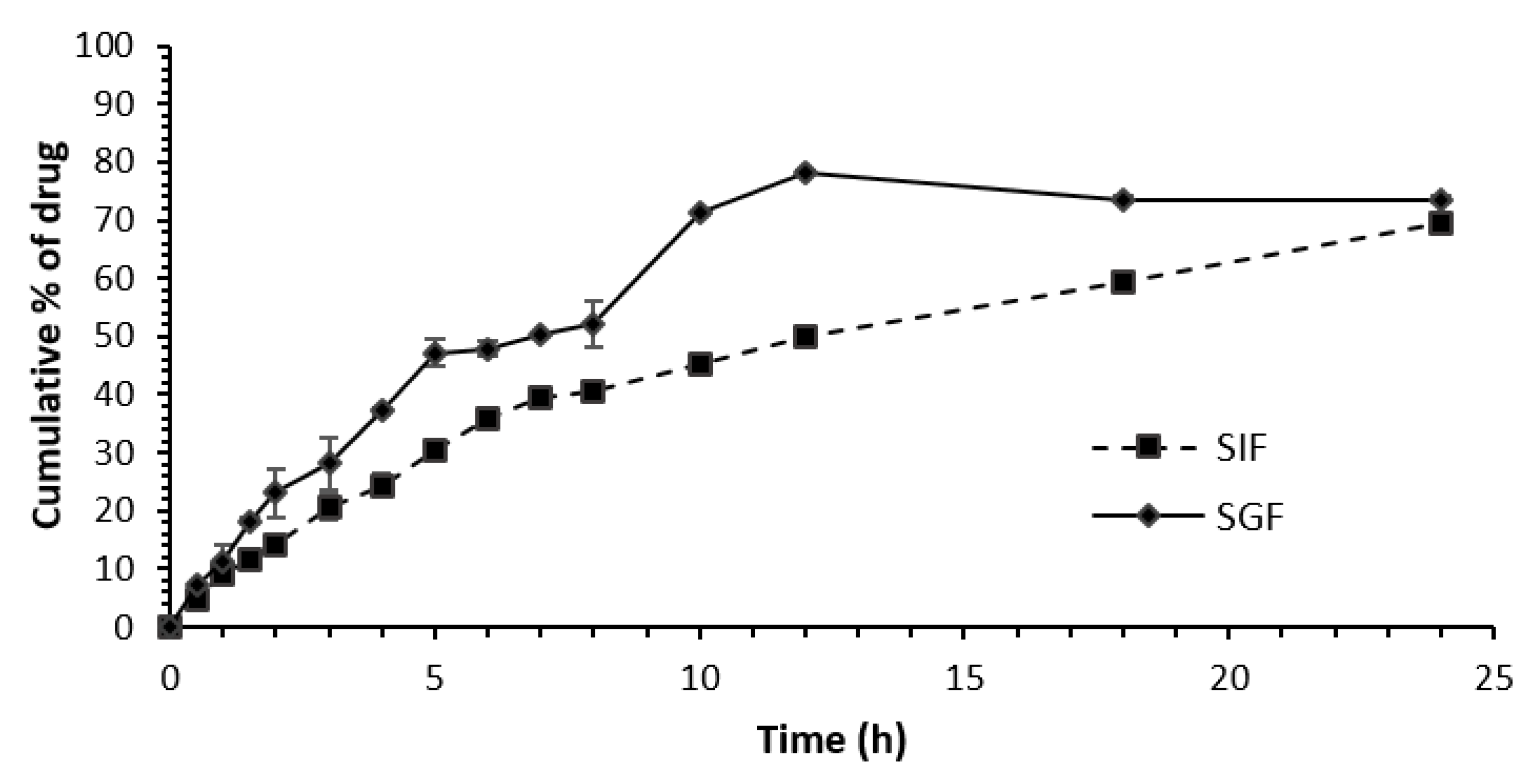
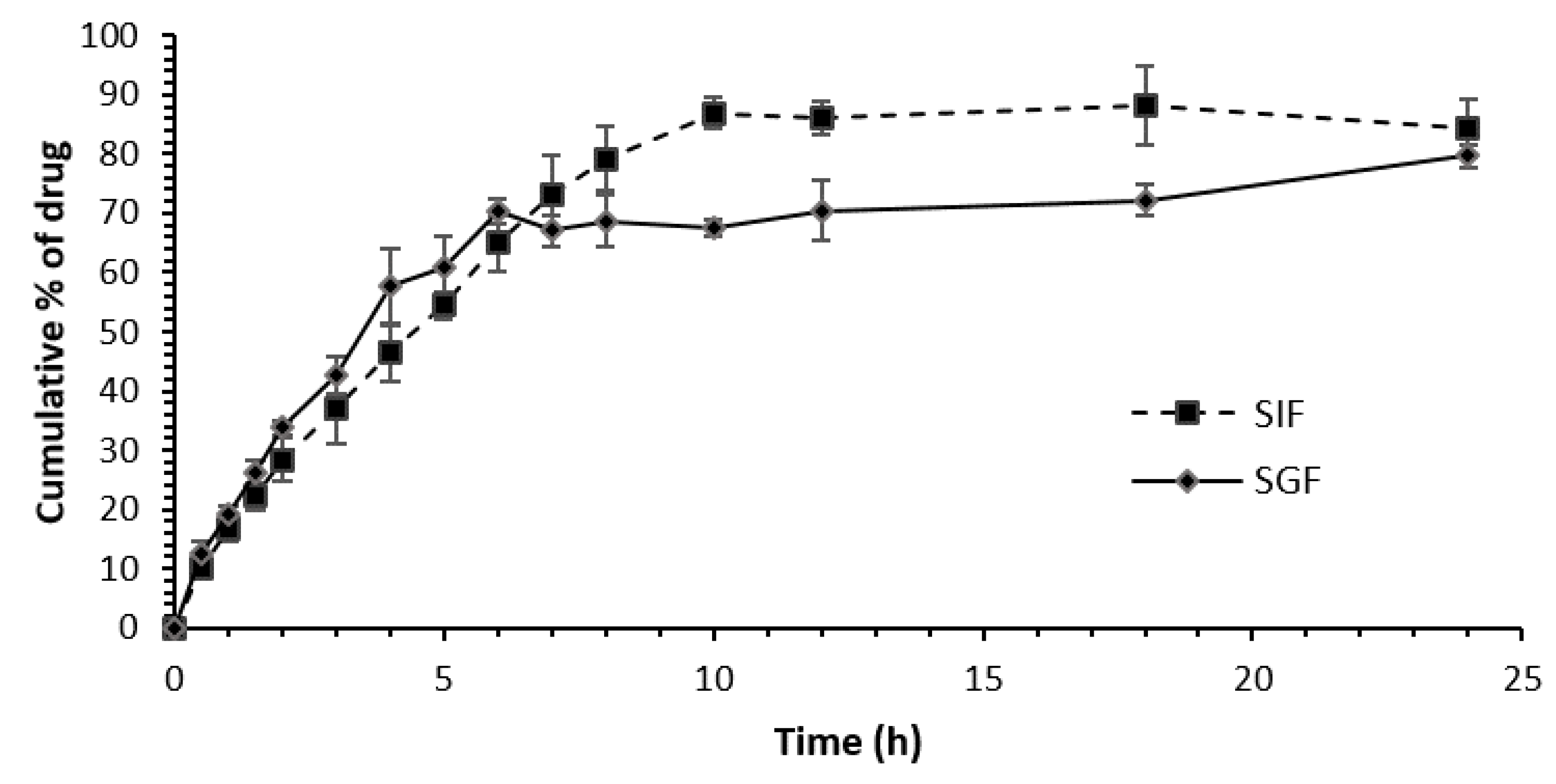
3.3. Release Profiles of Different Niacin Tablet Formulations in SGF and SIF
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jonsson, B.H. Nicotinic Acid Long-Term Effectiveness in a Patient with Bipolar Type II Disorder: A Case of Vitamin Dependency. Nutrients 2018, 10, 134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sledge, C.L.; Morgan, B.W. Encyclopedia of Toxicology, 3rd ed.; Academic Press: Cambridge, MA, USA, 2014. [Google Scholar]
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef] [PubMed]
- Carlson, L.A. Nicotinic acid: The broad-spectrum lipid drug. A 50th anniversary review. J. Intern. Med. 2005, 258, 94–114. [Google Scholar] [CrossRef] [PubMed]
- Piepho, R.W. The pharmacokinetics and pharmacodynamics of agents proven to raise high-density lipoprotein cholesterol. Am. J. Cardiol. 2000, 86, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Niacin-Health Professional Fact Sheet. Available online: https://ods.od.nih.gov/factsheets/Niacin-HealthProfessional/ (accessed on 28 March 2021).
- Li, J.; Kong, D.; Wang, Q.; Wu, W.; Tang, Y.; Bai, T.; Guo, L.; Wei, L.; Zhang, Q.; Yu, Y.; et al. Niacin ameliorates ulcerative colitis via prostaglandin D(2)-mediated D prostanoid receptor 1 activation. EMBO Mol. Med. 2017, 9, 571–588. [Google Scholar] [CrossRef]
- Center for Food Safety and Applied Nutrition (Continued) 2002|FDA. Available online: https://www.fda.gov/inspections-compliance-enforcement-and-criminal-investigations/enforcement-story-archive/center-food-safety-and-applied-nutrition-continued-2002 (accessed on 16 January 2021).
- Boggs, P.T.; Spiegelman, C.H.; Donaldson, J.R.; Schnabel, R.B. A computational examination of orthogonal distance regression. J. Econom. 1988, 38, 169–201. [Google Scholar] [CrossRef] [Green Version]
- Kirchhoefer, R.D.; Hipp, S. Niacin I: Dissolution Profiles of Sustained-Release Niacin Products by Automated and Manual Procedures. J. Aoac Int. 1993, 76, 394–398. [Google Scholar] [CrossRef]
- Kirchhoefer, R.D.; Hamilton, J.F. Effect of USP Apparatus 1 and 2 at Different Rotational Speeds on Dissolution of Niacin Formulations. J. Aoac Int. 1996, 79, 1005–1008. [Google Scholar] [CrossRef] [Green Version]
- Shargel, L.; Wu-Pong, S.; Yu, A.B.C. Applied Biopharmaceutics & Pharmacokinetics; Appleton & Lange Reviews/McGraw-Hill, Medical Pub. Division: Hoboken, NJ, USA, 2005. [Google Scholar]
- Leung, K.; Quezada, M.; Chen, Z.; Kanel, G.; Kaplowitz, N. Niacin-Induced Anicteric Microvesicular Steatotic Acute Liver Failure. Hepatol. Commun. 2018, 2, 1293–1298. [Google Scholar] [CrossRef] [Green Version]
- Wilkin, J.K.; Wilkin, O.; Kapp, R.; Donachie, R.; Chernosky, M.E.; Buckner, J. Aspirin blocks nicotinic acid–induced flushing. Clin. Pharmacol. Ther. 1982, 31, 478–482. [Google Scholar] [CrossRef]
- Pieper, J.A. Overview of niacin formulations: Differences in pharmacokinetics, efficacy, and safety. Am. J. Health-Syst. Pharm. 2003, 60 (Suppl. S2), S9–S14. [Google Scholar] [CrossRef] [PubMed]
- Milanowski, B.; Hejduk, A.; Bawiec, M.A.; Jakubowska, E.; Urbańska, A.; Wiśniewska, A.; Garbacz, G.; Lulek, J. Biorelevant In Vitro Release Testing and In Vivo Study of Extended-Release Niacin Hydrophilic Matrix Tablets. AAPS PharmSciTech 2020, 21, 83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
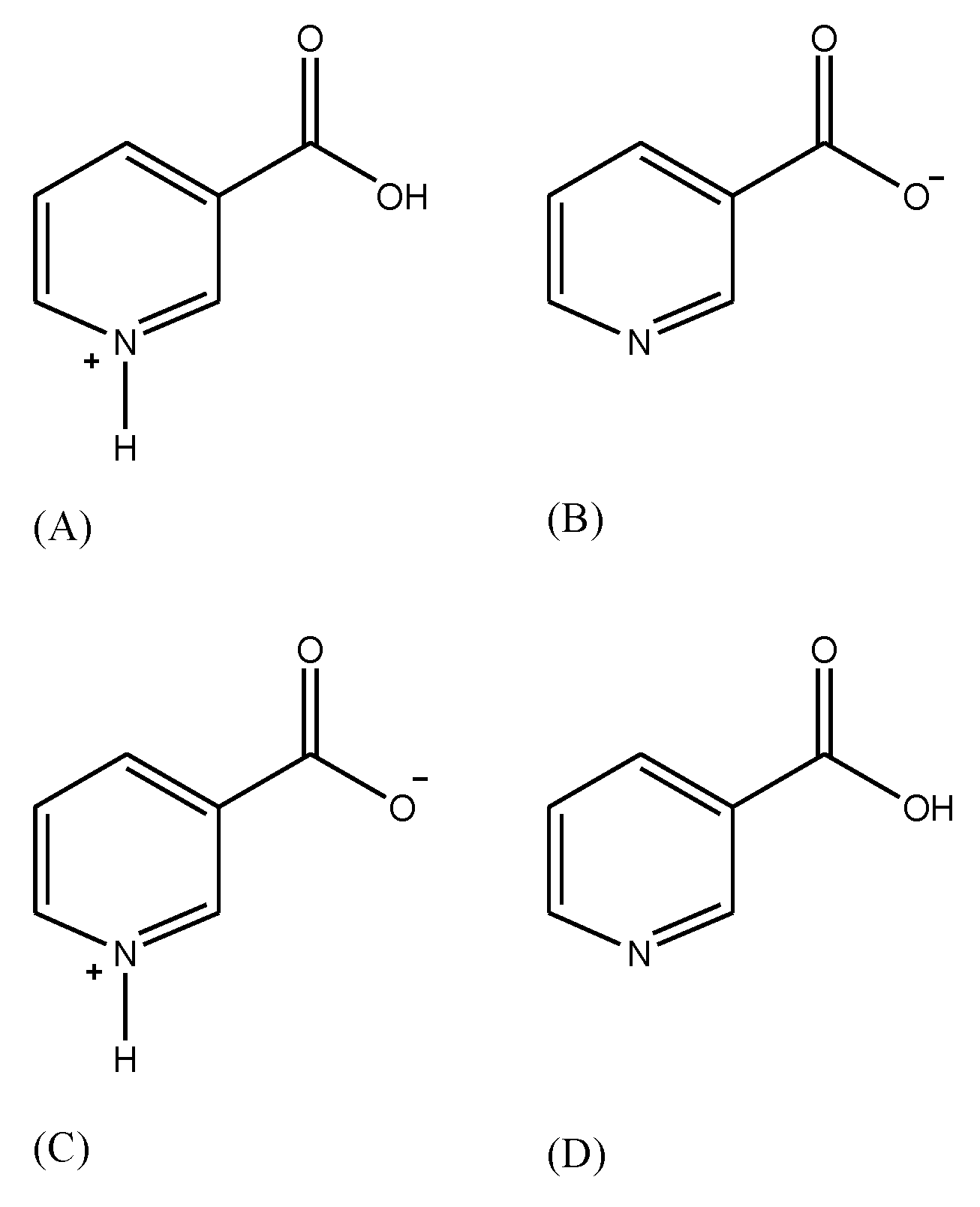
- García, B.; Ibeas, S.; Leal, J.M. Zwitterionic pyridinecarboxylic acids. J. Phys. Org. Chem. 1996, 9, 593–597. [Google Scholar] [CrossRef]
- Moore, J.W.; Flanner, H.H. Mathematical comparison of dissolution profiles. Pharm. Tech. 1996, 20, 64–74. [Google Scholar]
- Poon, I.; Chow, D.S.; Liang, D. Dissolution profiles of nonprescription extended-release niacin and inositor niacinate products. Am. J. Health-Syst. Pharm. 2006, 63, 2128–2134. [Google Scholar] [CrossRef]
- Ikeda, M.; Tsuji, H.; Nakamura, S.; Ichiyama, A.; Nishizuka, Y.; Hayaishi, O. Studies on the biosynthesis of nicotinamide adenine dinu-cleotide: A role of picolinic carboxylase in the biosynthesis of nicotinamideadenine dinucleotide from tryptophan in mammals. J. Biol. Chem. 1965, 240, 1395–1401. [Google Scholar] [CrossRef]
- Meyers, C.D.; Kashyap, M.L. Management of the metabolic syndrome-nicotinic acid. Endocrinol. Metab. Clin. N. Am. 2004, 33, 557–575. [Google Scholar] [CrossRef]
- Meyers, C.D.; Kamanna, V.S.; Kashyap, M.L. Niacin therapy in ath-erosclerosis. Curr. Opin. Lipidol. 2004, 15, 659–665. [Google Scholar] [CrossRef]
- Svetlana, M.; Nabokina, M.L.; Kashyap, L.; Hamid, M.S. Mechanism and regulation of human intestinal niacin uptake. Am. J. Physiol. Cell Physiol. 2005, 289, C97–C103. [Google Scholar]
- Cefali, E.A.; Simmons, P.D.; Stanek, E.J.; Shamp, T.R. Improved control of niacin-induced flushing using an optimized once-daily, extended-release niacin formulation. Int. J. Clin. Pharmacol. Ther. 2006, 44, 633–640. [Google Scholar] [CrossRef] [PubMed]
- Kaur, R.K.S. Role of Polymers in Drug Delivery. J. Drug Deliv. Ther. 2014, 4, 32–36. [Google Scholar] [CrossRef]
- Medronho, B.; Romano, A.; Miguel, M.G.; Stigsson, L.; Lindman, B. Rationalizing cellulose (in)solubility: Reviewing basic physicochemical aspects and role of hydrophobic interactions. Cellulose 2012, 19, 581–587. [Google Scholar] [CrossRef]
- Cooper, D.L.; Murrell, D.E.; Roane, D.S.; Harirforoosh, S. Effects of formulation design on niacin therapeutics: Mechanism of action, metabolism, and drug delivery. Int. J. Pharm. 2015, 490, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Vasvári, G.; Csontos, B.; Sovány, T.; Regdon, G.; Bényei, A.; Váradi, J.; Bácskay, I.; Ujhelyi, Z.; Fehér, P.; Sinka, D.; et al. Development and Characterization of Modified Release Hard Gelatin Capsules, Based on In Situ Lipid Matrix Formation. AAPS PharmSciTech 2018, 19, 3165–3176. [Google Scholar] [CrossRef] [PubMed]
- Nabais, T.; Leclair, G. High-amylose sodium carboxymethyl starch matrices: Development and characterization of tramadol hydrochloride sustained-release tablets for oral administration. ISRN Pharm. 2014, 2014, 391523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riis, T.; Bauer-Brandl, A.; Wagner, T.; Kranz, H. pH-independent drug release of an extremely poorly soluble weakly acidic drug from multiparticulate extended release formulations. Eur. J. Pharm. Biopharm. 2007, 65, 78–84. [Google Scholar] [CrossRef]
- Chung, S.; Kim, J.; Ban, E.; Yun, J.; Park, B.; Kim, A. Solution-Mediated Phase Transformation of Aripiprazole: Negating the Effect of Crystalline Forms on Dissolution and Oral Pharmacokinetics. J. Pharm. Sci. 2020, 109, 3668–3677. [Google Scholar] [CrossRef]
- Lestari, S.D.; Baehaki, A.; Sari, Y. The effect of degradation time in the simulated gastric fluid for bioactive compounds from bekasam. IOP Conf. Ser. Earth Environ. Sci. 2020, 404, 012018. [Google Scholar]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name | Code | Formulation | Niacin Amount per Product | Lot Number # | Expiration Date | Manufacturer | Excipients |
|---|---|---|---|---|---|---|---|
| Niacin | Brand-A | IR tablet | 250 mg | 3245ER2513 | 06/2020 | General Nutrition Corporation (GNC) | Dicalcium phosphate; cellulose; whole brown rice powder (Oryza sativa) |
| ER Niacin | Brand-B | Extended-release tablet | 500 mg | 184548 | 03/2021 | Rugby Laboratories | Gelatin; sugar; talc; pharmaceutical glaze; starch |
| SLO Niacin | Brand-C | CR tablet | 500 mg | 383151 | 04/2022 | Main Pointe Pharmaceuticals, LLC. | Hydromellose; hydrogenated vegetable oil; silicon dioxide; magnesium stearate; glyceryl dibehenate; |
| TR Niacin | Brand-D | Capsule | 1000 mg | 191879 | 04/2021 | Rugby Laboratories | Microcrystalline cellulose; Hypromellose; stearic acid; silica; magnesium stearate; pharmaceutical glaze; magnesium silicate |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chbib, C.; Rashid, M.A.; Shah, S.M.; Kazi, M.; Uddin, M.N. Evaluating the Release of Different Commercial Orally Modified Niacin Formulations In Vitro. Polymers 2023, 15, 3046. https://doi.org/10.3390/polym15143046
Chbib C, Rashid MA, Shah SM, Kazi M, Uddin MN. Evaluating the Release of Different Commercial Orally Modified Niacin Formulations In Vitro. Polymers. 2023; 15(14):3046. https://doi.org/10.3390/polym15143046
Chicago/Turabian StyleChbib, Christiane, Md. Abdur Rashid, Sarthak M. Shah, Mohsin Kazi, and Mohammad N. Uddin. 2023. "Evaluating the Release of Different Commercial Orally Modified Niacin Formulations In Vitro" Polymers 15, no. 14: 3046. https://doi.org/10.3390/polym15143046