
Post-Fatigue Fracture Resistance of Lithium Disilicate and Polymer-Infiltrated Ceramic Network Indirect Restorations over Endodontically-Treated Molars with Different Preparation Designs: An In-Vitro Study
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
- (1)
- Tooth preparation designs at three levels: adhesive crown, overlay, and occlusal veneer, there being one instance where only one bulk-fill composite resin (Voco, Cuxhaven, Germany) was used for the build-up core;
- (2)
- “CAD/CAM blocks” at two levels: after core build-up, two different CAD/CAM restorative materials were tested: a PICN (GrandioBlocks, Voco, Cuxhaven, Germany) and an LS (E-max CAD, HT A2/C14, Ivoclar Vivadent).
2.2. Specimen Selection
2.3. Endodontic Treatment
2.4. Specimen Preparation
- Group 1:
- Occlusal veneer. A cylindrical bur (6836 KR 014, Komet) was used to perform a standardized 1.2 mm occlusal reduction following the occlusal anatomy. A conical bur with a flat point (H15809, Komet) was used to create 1 mm deep mesial and distal interproximal boxes. Finally, a football-shaped bur (8368 L, Komet) was used to bevel the occlusal margins (8368 L, Komet), and an Arkansas tip (661, Komet) and a rubber point (9436 M, Komet) were used to round all corners and finish the preparation.
- Group 2:
- Overlay. A 1.6 mm occlusal reduction was performed using a cylindrical bur (6836 KR 014, Komet). A round shoulder of 1.5 mm depth, placed in the middle third of the clinical crown, and interproximal boxes, placed 1 mm above the CEJ, were then performed in all specimens with a conical bur with a flat point (H15809, Komet). An Arkansas tip (661, Komet) and a rubber point (9436 M, Komet) were used to round all corners.
- Group 3:
- Adhesive crown. A standardized 2 mm occlusal reduction was performed with a chamfer margin 1 ± 0.5 mm above CEJ. Chamfer burs (6881 014, Komet; 8881 014, Komet) were used to perform initial and finishing preparations. Then, an Arkansas tip (661, Komet) and a rubber point (9436 M, Komet) were used to round all corners.
- Subgroup A: PICN (Vita Enamic, Vita), shade 2M1-HT.
- Subgroup B: LS (E-max CAD, Ivoclar), shade A2 HT.
2.5. Luting Procedure
2.6. Cyclical Intermittent Loading
2.7. Fracture Resistance
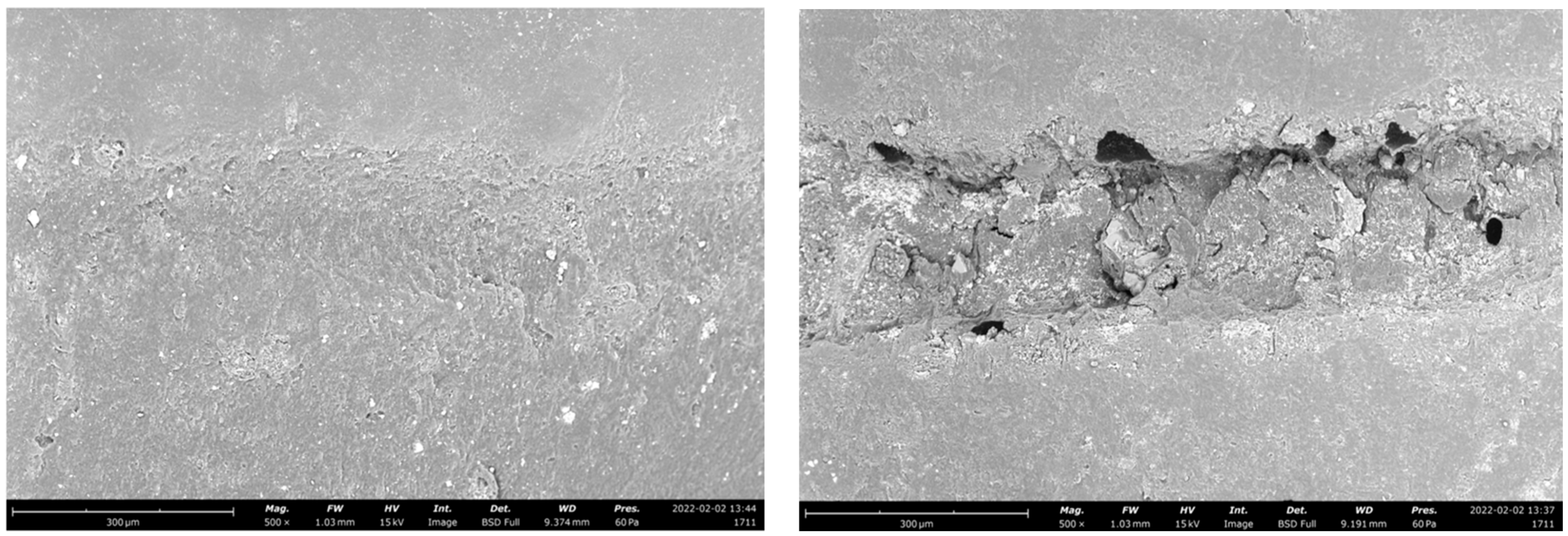
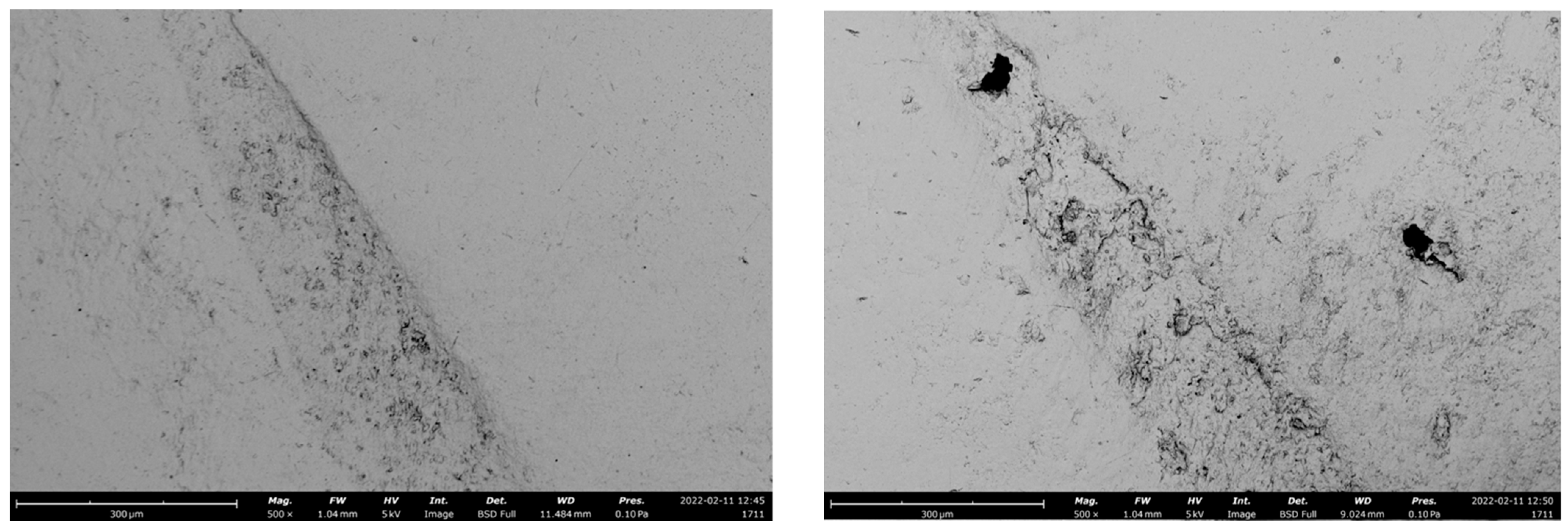
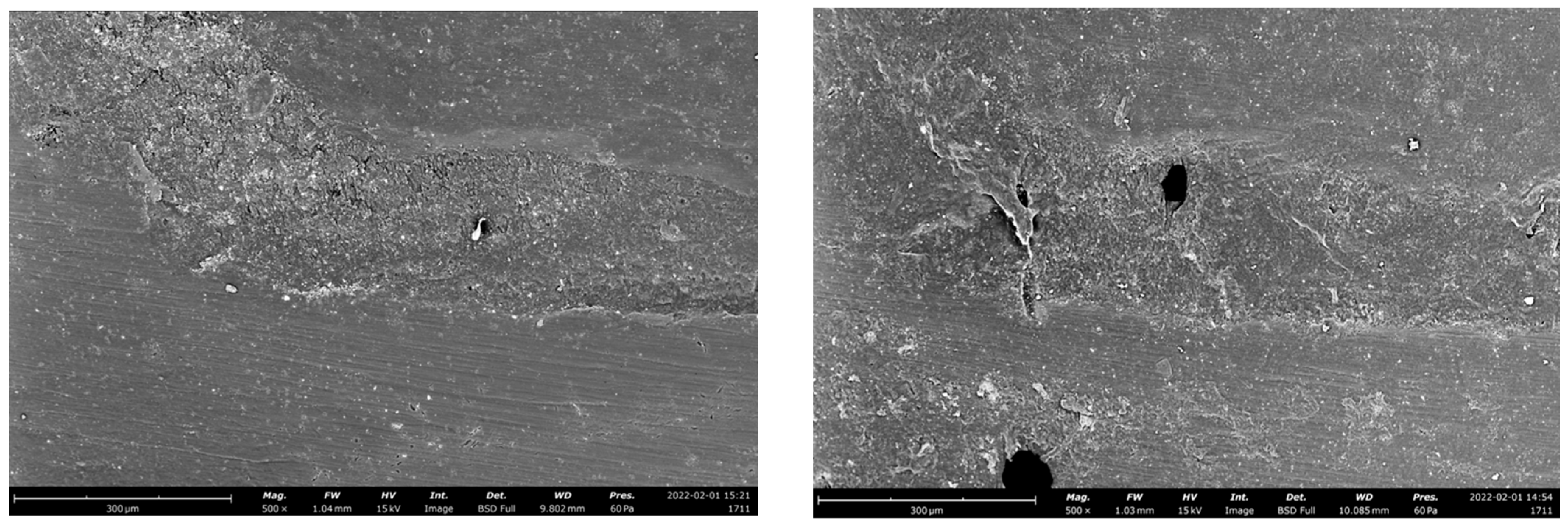
2.8. Scanning Electron Microscopy (SEM) Analysis
2.9. Statistical Analysis Description
3. Results
4. Discussion
5. Conclusions
- −
- Different preparation designs and CAD/CAM materials seem to influence the fatigue resistance of adhesive indirect restorations over ETT;
- −
- Overlay preparation seems to be a valid alternative to the traditional full crown, while occlusal veneers should be avoided in restoring non-vital molars with a high loss of residual tooth structure;
- −
- Both LS and PICN showed an optimal survival rate after a cycling intermittent load test;
- −
- Occlusal veneers and overlay never showed dramatic failures during dynamic loading, showing a high ability to protect the supporting tooth structure;
- −
- Regarding static fracture resistance, LS is more resistant than PICN.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Manhart, J.; Chen, H.; Hamm, G.; Hickel, R. Buonocore Memorial Lecture. Review of the clinical survival of direct and indirect restorations in posterior teeth of the permanent dentition. Oper. Dent. 2004, 29, 481–508. [Google Scholar]
- Van Nieuwenhuysen, J.P.; D’Hoore, W.; Carvalho, J.; Qvist, V. Long-term evaluation of extensive restorations in permanent teeth. J. Dent. 2003, 31, 395–405. [Google Scholar] [CrossRef] [PubMed]
- Colman, H.L. Restoration of endodontically treated teeth. Dent. Clin. N. Am. 1979, 23, 647–662. [Google Scholar] [CrossRef] [PubMed]
- Assif, D.; Gorfil, C. Biomechanical considerations in restoring endodontically treated teeth. J. Prosthet. Dent. 1994, 71, 565–567. [Google Scholar] [CrossRef] [PubMed]
- Seow, L.L.; Toh, C.G.; Wilson, N.H. Strain measurements and fracture resistance of endodontically treated premolars restored with all-ceramic restorations. J. Dent. 2015, 43, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Setzer, F.C.; Kim, S. Comparison of long-term survival of implants and endodontically treated teeth. J. Dent. Res. 2014, 93, 19–26. [Google Scholar] [CrossRef]
- Iqbal, M.K.; Kim, S. A review of factors influencing treatment planning decisions of single-tooth implants versus preserving natural teeth with nonsurgical endodontic therapy. J. Endod. 2008, 34, 519–529. [Google Scholar] [CrossRef]
- Mekhdieva, E.; Del Fabbro, M.; Alovisi, M.; Comba, A.; Scotti, N.; Tumedei, M.; Carossa, M.; Berutti, E.; Pasqualini, D. Postoperative Pain following Root Canal Filling with Bioceramic vs. Traditional Filling Techniques: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2021, 10, 4509. [Google Scholar] [CrossRef]
- Reeh, E.S.; Messer, H.H.; Douglas, W.H. Reduction in tooth stiffness as a result of endodontic and restorative procedures. J. Endod. 1989, 15, 512–516. [Google Scholar] [CrossRef]
- Kishen, A. Mechanisms and Risk Factors for Fracture Predilection in Endodontically Treated Teeth. Endod. Top. 2006, 13, 57–83. [Google Scholar] [CrossRef]
- Lagouvardos, P.; Sourai, P.; Douvitsas, G. Coronal fractures in posterior teeth. Oper. Dent. 1989, 14, 28–32. [Google Scholar] [PubMed]
- Pasqualini, D.; Scotti, N.; Mollo, L.; Berutti, E.; Angelini, E.; Migliaretti, G.; Cuffini, A.; Adlerstein, D. Microbial leakage of Gutta-Percha and Resilon root canal filling material: A comparative study using a new homogeneous assay for sequence detection. J. Biomater. Appl. 2008, 22, 337–352. [Google Scholar] [CrossRef] [Green Version]
- Edelhoff, D.; Sorensen, J.A. Tooth structure removal associated with various preparation designs for anterior teeth. J. Prosthet. Dent. 2002, 87, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Edelhoff, D.; Sorensen, J.A. Tooth structure removal associated with various preparation designs for posterior teeth. Int. J. Periodontics Restor. Dent. 2002, 22, 241–249. [Google Scholar]
- Rocca, G.T.; Krejci, I. Crown and Post-Free Adhesive Restorations for Endodontically Treated Posterior Teeth: From Direct Composite to Endocrowns. Eur. J. Esthet. Dent. 2013, 8, 156–179. [Google Scholar]
- Scotti, N.; Scansetti, M.; Rota, R.; Pera, F.; Pasqualini, D.; Berutti, E. The Effect of the Post Length and Cusp Coverage on the Cycling and Static Load of Endodontically Treated Maxillary Premolars. Clin. Oral Investig. 2011, 15, 923–929. [Google Scholar] [CrossRef]
- Poggio, C.E.; Ercoli, C.; Rispoli, L.; Maiorana, C.; Esposito, M. Metal-free materials for fixed prosthodontic restorations. Cochrane Database Syst. Rev. 2017, 12, CD009606. [Google Scholar] [CrossRef]
- Abdullah, A.; Muhammed, F.; Zheng, B.; Liu, Y. An overview of computer aided design/computer aided manufacturing (CAD/CAM) in restorative dentistry. J. Dent. Mater. Tech. 2018, 7, 1–10. [Google Scholar]
- Zarone, F.; Di Mauro, M.I.; Ausiello, P.; Ruggiero, G.; Sorrentino, R. Current status on lithium disilicate and zirconia: A narrative review. BMC Oral Health. 2019, 19, 134. [Google Scholar] [CrossRef] [Green Version]
- Zarone, F.; Ferrari, M.; Mangano, F.G.; Leone, R.; Sorrentino, R. “Digitally Oriented Materials”: Focus on Lithium Disilicate Ceramics. Int. J. Dent. 2016, 2016, 9840594. [Google Scholar] [CrossRef]
- Luciano, M.; Francesca, Z.; Michela, S.; Tommaso, M.; Massimo, A. Lithium disilicate posterior overlays: Clinical and biomechanical features. Clin. Oral Investig. 2020, 24, 841–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gehrt, M.; Wolfart, S.; Rafai, N.; Reich, S.; Edelhoff, D. Clinical results of lithium-disilicate crowns after up to 9 years of service. Clin. Oral Investig. 2013, 17, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Simeone, P.; Gracis, S. Eleven-Year Retrospective Survival Study of 275 Veneered Lithium Disilicate Single Crowns. Int. J. Periodontics Restor. Dent. 2015, 35, 685–694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Facenda, J.C.; Borba, M.; Corazza, P.H. A literature review on the new polymer-infiltrated ceramic-network material (PICN). J. Esthet. Restor. Dent. 2018, 30, 281–286. [Google Scholar] [CrossRef]
- Gomes de Carvalho, A.B.; de Andrade, G.S.; Mendes Tribst, J.P.; Grassi, E.D.A.; Ausiello, P.; Saavedra, G.S.F.A.; Bressane, A.; Marques de Melo, R.; Borges, A.L.S. Mechanical Behavior of Different Restorative Materials and Onlay Preparation Designs in Endodontically Treated Molars. Materials 2021, 14, 1923. [Google Scholar] [CrossRef]
- Aboushelib, M.N.; Elsafi, M.H. Survival of resin infiltrated ceramics under influence of fatigue. Dent. Mater. 2016, 32, 529–534. [Google Scholar] [CrossRef]
- Swain, M.V.; Coldea, A.; Bilkhair, A.; Guess, P.C. Interpenetrating network ceramic-resin composite dental restorative materials. Dent. Mater. 2016, 32, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Homaei, E.; Farhangdoost, K.; Pow, E.H.N.; Matinlinna, J.P.; Akbari, M.; Tsoi, J.K.H. Fatigue resistance of monolithic CAD/CAM ceramic crowns on human premolars. J. Ceram. Int. 2016, 29, 7–11. [Google Scholar] [CrossRef]
- Homaei, E.; Farhangdoost, K.; Tsoi, J.K.H.; Matinlinna, J.P.; Pow, E.H.N. Static and fatigue mechanical behavior of three dental CAD/CAM ceramics. J. Mech. Behav. Biomed Mater. 2016, 59, 304–313. [Google Scholar] [CrossRef] [PubMed]
- Baldi, A.; Comba, A.; Michelotto Tempesta, R.; Carossa, M.; Pereira, G.K.R.; Valandro, L.F.; Paolone, G.; Vichi, A.; Goracci, C.; Scotti, N. External Marginal Gap Variation and Residual Fracture Resistance of Composite and Lithium-Silicate CAD/CAM Overlays after Cyclic Fatigue over Endodontically-Treated Molars. Polymers 2021, 13, 3002. [Google Scholar] [CrossRef]
- Baldi, A.; Carossa, M.; Comba, A.; Alovisi, M.; Femiano, F.; Pasqualini, D.; Berutti, E.; Scotti, N. Wear Behaviour of Polymer-Infiltrated Network Ceramics, Lithium Disilicate and Cubic Zirconia against Enamel in a Bruxism-Simulated Scenario. Biomedicines 2022, 10, 1682. [Google Scholar] [CrossRef] [PubMed]
- Scotti, N.; Michelotto Tempesta, R.; Pasqualini, D.; Baldi, A.; Vergano, E.A.; Baldissara, P.; Alovisi, M.; Comba, A. 3D Interfacial Gap and Fracture Resistance of Endodontically Treated Premolars Restored with Fiber-reinforced Composites. J. Adhes. Dent. 2020, 22, 215–224. [Google Scholar] [CrossRef] [PubMed]
- Scotti, N.; Bergantin, E.; Alovisi, M.; Pasqualini, D.; Berutti, E. Evaluation of a simplified fiber post removal system. J. Endod. 2013, 39, 1431–1434. [Google Scholar] [CrossRef] [PubMed]
- Maravic, T.; Mazzoni, A.; Comba, A.; Scotti, N.; Checchi, V.; Breschi, L. How stable is dentine as a substrate for bonding? Curr. Oral Health Rep. 2017, 4, 248–257. [Google Scholar] [CrossRef]
- Comba, A.; Scotti, N.; Mazzoni, A.; Maravic, T.; Ribeiro Cunha, S.; Michelotto Tempesta, R.; Carossa, M.; Pashley, D.H.; Tay, F.R.; Breschi, L. Carbodiimide inactivation of matrix metalloproteinases in radicular dentine. J. Dent. 2019, 82, 56–62. [Google Scholar] [CrossRef]
- Dioguardi, M.; Alovisi, M.; Troiano, G.; Caponio, C.V.A.; Baldi, A.; Rocca, G.T.; Comba, A.; Lo Muzio, L.; Scotti, N. Clinical outcome of bonded partial indirect posterior restorations on vital and non-vital teeth: A systematic review and meta-analysis. Clin. Oral Investig. 2021, 25, 6597–6621. [Google Scholar] [CrossRef]
- Scotti, N.; Cavalli, G.; Gagliani, M.; Breschi, L. New adhesives and bonding techniques. Why and when? Int. J. Esthet. Dent. 2017, 12, 524–535. [Google Scholar]
- Spitznagel, F.A.; Boldt, J.; Gierthmuehlen, P.C. CAD/CAM Ceramic Restorative Materials for Natural Teeth. J. Dent. Res. 2018, 97, 1082–1091. [Google Scholar] [CrossRef]
- Scotti, N.; Venturello, A.; Migliaretti, G.; Pera, F.; Pasqualini, D.; Geobaldo, F.; Berutti, E. New-generation curing units and short irradiation time: The degree of conversion of microhybrid composite resin. Quintessence Int. 2011, 42, e89–e95. [Google Scholar]
- Frankenberger, R.; Winter, J.; Dudek, M.C.; Naumann, M.; Amend, S.; Braun, A.; Krämer, N.; Roggendorf, M.J. Post-Fatigue Fracture and Marginal Behavior of Endodontically Treated Teeth: Partial Crown vs. Full Crown vs. Endocrown vs. Fiber-Reinforced Resin Composite. Materials 2021, 14, 7733. [Google Scholar] [CrossRef] [PubMed]
- Frankenberger, R.; Zeilinger, I.; Krech, M.; Mörig, G.; Naumann, M.; Braun, A.; Krämer, N.; Roggendorf, M.J. Stability of endodontically treated teeth with differently invasive restorations: Adhesive vs. non-adhesive cusp stabilization. Dent. Mater. 2015, 31, 1312–1320. [Google Scholar] [CrossRef] [PubMed]
- Skouridou, N.; Pollington, S.; Rosentritt, M.; Tsitrou, E. Fracture strength of minimally prepared all-ceramic CEREC crowns after simulating 5 years of service. Dent. Mater. 2013, 29, e70–e77. [Google Scholar] [CrossRef] [PubMed]
- Vagropoulou, G.I.; Klifopoulou, G.L.; Vlahou, S.G.; Hirayama, H.; Michalakis, K. Complications and survival rates of inlays and onlays vs complete coverage restorations: A systematic review and analysis of studies. J. Oral Rehabil. 2018, 45, 903–920. [Google Scholar] [CrossRef]
- Alberto Jurado, C.; Kaleinikova, Z.; Tsujimoto, A.; Alberto Cortés Treviño, D.; Seghi, R.R.; Lee, D.J. Comparison of Fracture Resistance for Chairside CAD/CAM Lithium Disilicate Crowns and Overlays with Different Designs. J. Prosthodont. 2022, 31, 341–347. [Google Scholar] [CrossRef]
- Schönhoff, L.M.; Lümkemann, N.; Buser, R.; Hampe, R.; Stawarczyk, B. Fatigue resistance of monolithic strength-gradient zirconia materials. J. Mech. Behav. Biomed. Mater. 2021, 119, 104504. [Google Scholar] [CrossRef] [PubMed]
- Baldi, A.; Comba, A.; Ferrero, G.; Italia, E.; Michelotto Tempesta, R.; Paolone, G.; Mazzoni, A.; Breschi, L.; Scotti, N. External gap progression after cyclic fatigue of adhesive overlays and crowns made with high translucency zirconia or lithium silicate. J. Esthet. Restor. Dent. 2022, 34, 557–564. [Google Scholar] [CrossRef]
- Scotti, N.; Baldi, A.; Vergano, E.A.; Tempesta, R.M.; Alovisi, M.; Pasqualini, D.; Carpegna, G.C.; Comba, A. Tridimensional Evaluation of the Interfacial Gap in Deep Cervical Margin Restorations: A Micro-CT Study. Oper. Dent. 2020, 45, E227–E236. [Google Scholar] [CrossRef] [PubMed]
- Dietschi, D.; Duc, O.; Krejci, I.; Sadan, A. Biomechanical considerations for the restoration of endodontically treated teeth: A systematic review of the literature—Part 1. Composition and micro-and macrostructure alterations. Quintessence Int. 2007, 38, 733–743. [Google Scholar] [PubMed]
- de Andrade, G.S.; Pinto, A.B.A.; Tribst, J.P.M.; Chun, E.P.; Borges, A.L.S.; de Siqueira Ferreira Anzaloni Saavedra, G. Does overlay preparation design affect polymerization shrinkage stress distribution? A 3D FEA study. Comput. Methods Biomech. Biomed. Engin. 2021, 24, 1026–1034. [Google Scholar] [CrossRef]
- Tang, W.; Wu, Y.; Smales, R.J. Identifying and reducing risks for potential fractures in endodontically treated teeth. J. Endod. 2010, 36, 609–617. [Google Scholar] [CrossRef]
- El Zhawi, H.; Kaizer, M.R.; Chughtai, A.; Moraes, R.R.; Zhang, Y. Polymer infiltrated ceramic network structures for resistance to fatigue fracture and wear. Dent. Mater. 2016, 32, 1352–1361. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Material | General Description | Manufacturer | Composition |
|---|---|---|---|
| E-max CAD | Lithium disilicate | Ivoclar vivadent, Schaan, Liechtenstein | SiO2 60.0–65.0%, K2 = 15.0–19.0%, Al2 = 3 6.0–10.5%, other oxides and pigments 0.0–8.0% |
| Vita Enamic | Polymer-infiltrated ceramic network | Vita, Bad Säckingen, Germany | Feldspar ceramic enriched with aluminum oxide (75% v/v), (wt 86%), UDMA, TEGDMA (14% wt 25% v/v) |
| Occlusal Veneer | Overlay | Adhesive Crown | ||||
|---|---|---|---|---|---|---|
| LS | PICN | LS | PICN | LS | PICN | |
| Events during cyclical intermittent loading | 1 chipping | 3 chippings | none | 2 chippings | 1 debonding, 1 core fracture | 2 debondings |
| Occlusal Veneer | Adhesive Crown | Overlay | ||||
|---|---|---|---|---|---|---|
| PICN | LS | PICN | LS | PICN | LS | |
| Fracture resistance (N) | 1806.6 ± 270.1 ab | 2029.5 ± 295.3 a | 1555.4 ± 393.9 b | 1859.2 ± 232.0 ab | 1726.9 ± 301.1 ab | 2059.5 ± 308.0 a |
| Fracture Pattern | Occlusal Veneer | Overlay | Adhesive Crown | |||
|---|---|---|---|---|---|---|
| LS | PICN | LS | PICN | LS | PICN | |
| Non-catastrophic | 75% | 71.4% | 71% | 65.5% | 50% | 72.7% |
| Catastrophic | 25% | 28.6% | 28% | 34.5% | 50% | 27.3% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Comba, A.; Baldi, A.; Carossa, M.; Michelotto Tempesta, R.; Garino, E.; Llubani, X.; Rozzi, D.; Mikonis, J.; Paolone, G.; Scotti, N. Post-Fatigue Fracture Resistance of Lithium Disilicate and Polymer-Infiltrated Ceramic Network Indirect Restorations over Endodontically-Treated Molars with Different Preparation Designs: An In-Vitro Study. Polymers 2022, 14, 5084. https://doi.org/10.3390/polym14235084
Comba A, Baldi A, Carossa M, Michelotto Tempesta R, Garino E, Llubani X, Rozzi D, Mikonis J, Paolone G, Scotti N. Post-Fatigue Fracture Resistance of Lithium Disilicate and Polymer-Infiltrated Ceramic Network Indirect Restorations over Endodontically-Treated Molars with Different Preparation Designs: An In-Vitro Study. Polymers. 2022; 14(23):5084. https://doi.org/10.3390/polym14235084
Chicago/Turabian StyleComba, Allegra, Andrea Baldi, Massimo Carossa, Riccardo Michelotto Tempesta, Eric Garino, Xhuliano Llubani, Davide Rozzi, Julius Mikonis, Gaetano Paolone, and Nicola Scotti. 2022. "Post-Fatigue Fracture Resistance of Lithium Disilicate and Polymer-Infiltrated Ceramic Network Indirect Restorations over Endodontically-Treated Molars with Different Preparation Designs: An In-Vitro Study" Polymers 14, no. 23: 5084. https://doi.org/10.3390/polym14235084