Hemostatic Enhancement via Chitosan Is Independent of Classical Clotting Pathways—A Quantitative Study


Abstract
:
1. Introduction
2. Materials and Methods
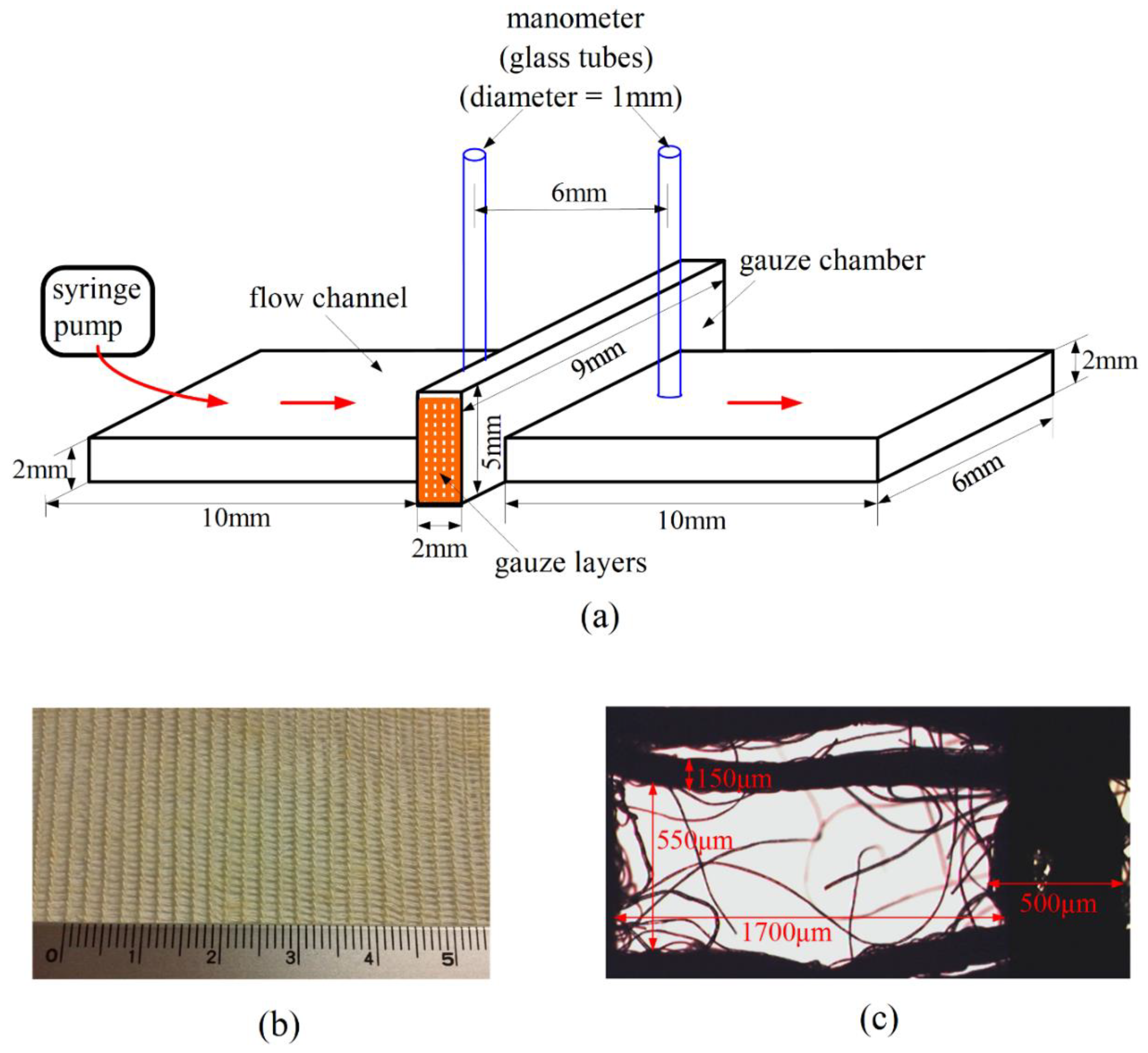
2.1. Flow Device
2.2. Gauzes
2.3. Blood
3. Results
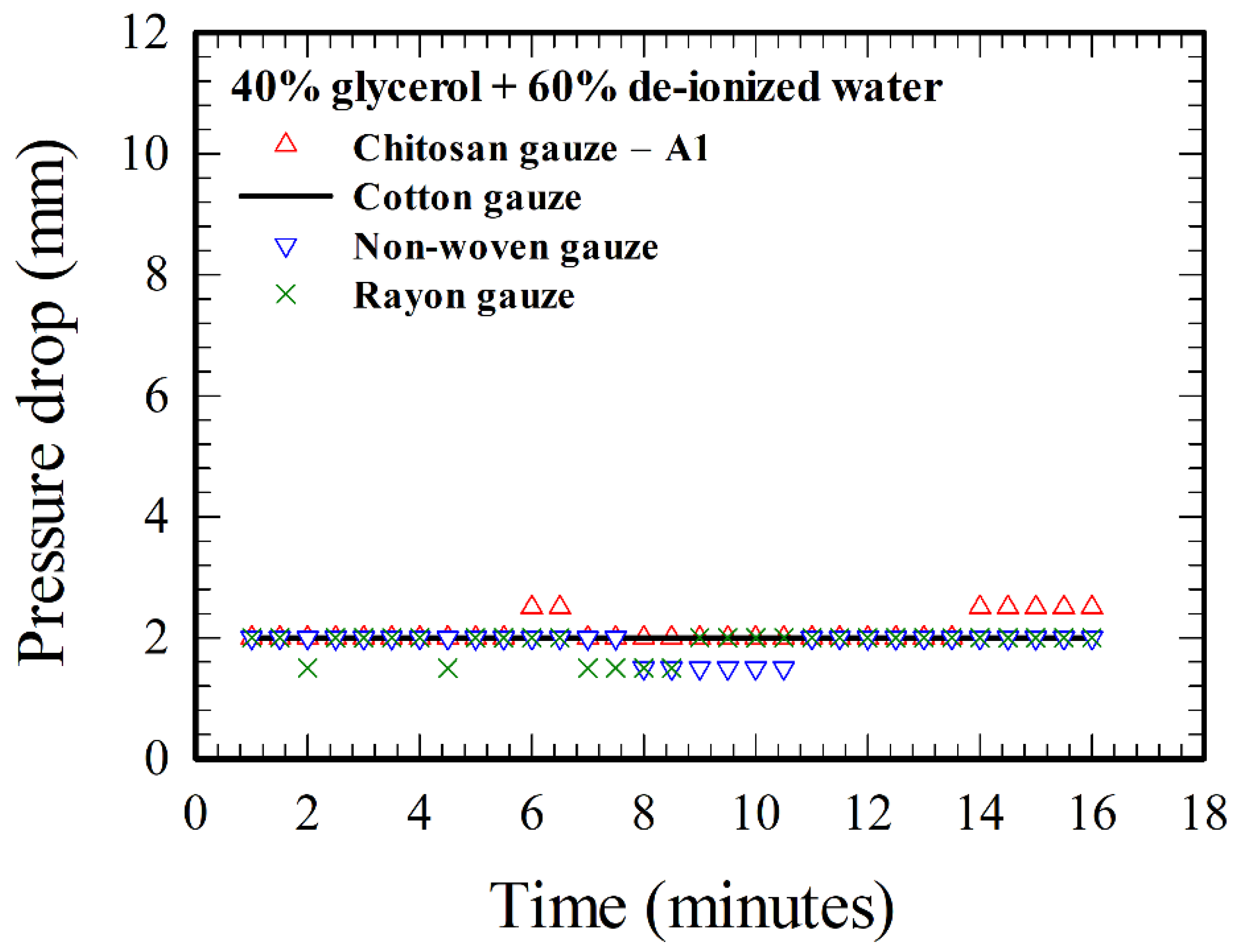
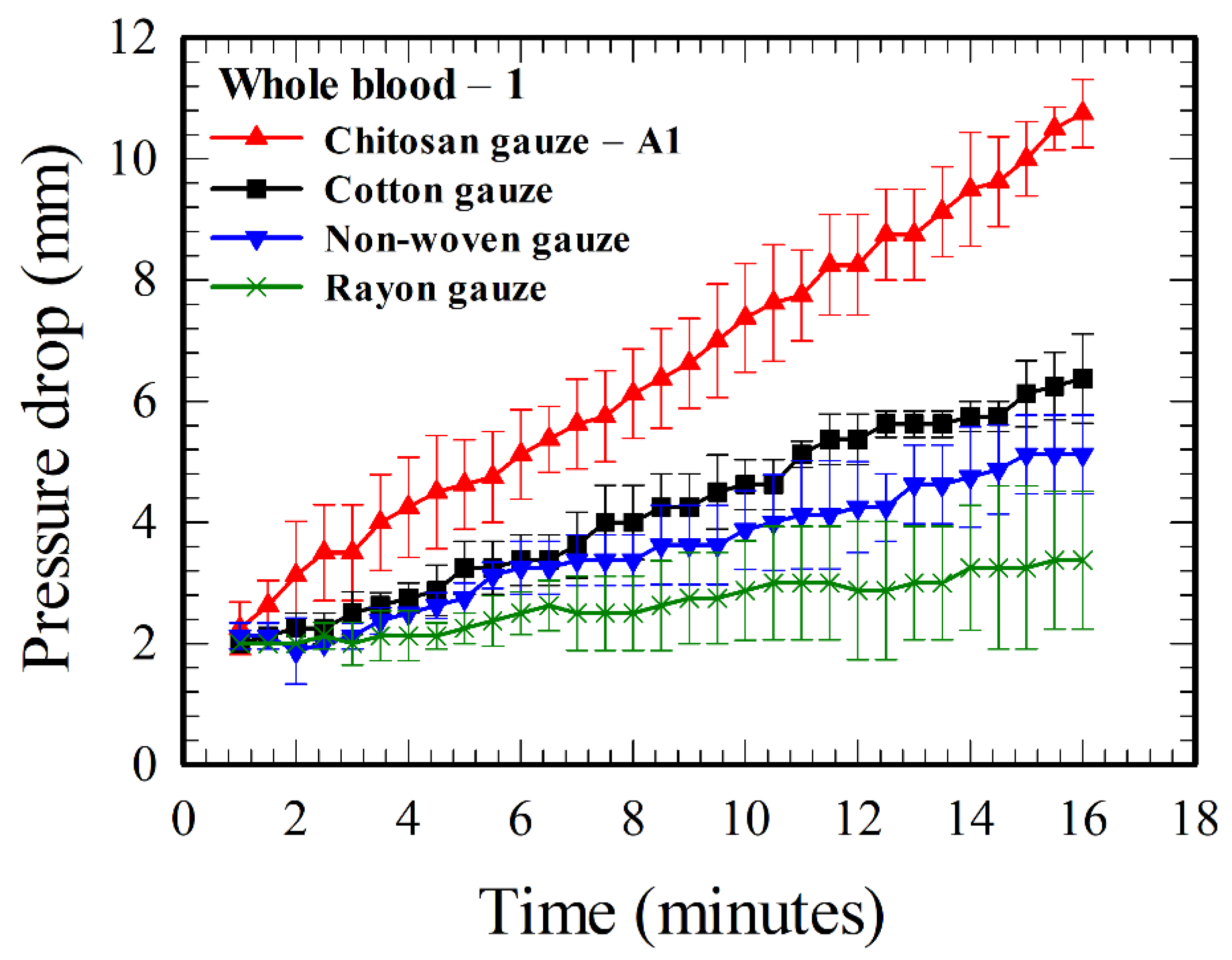
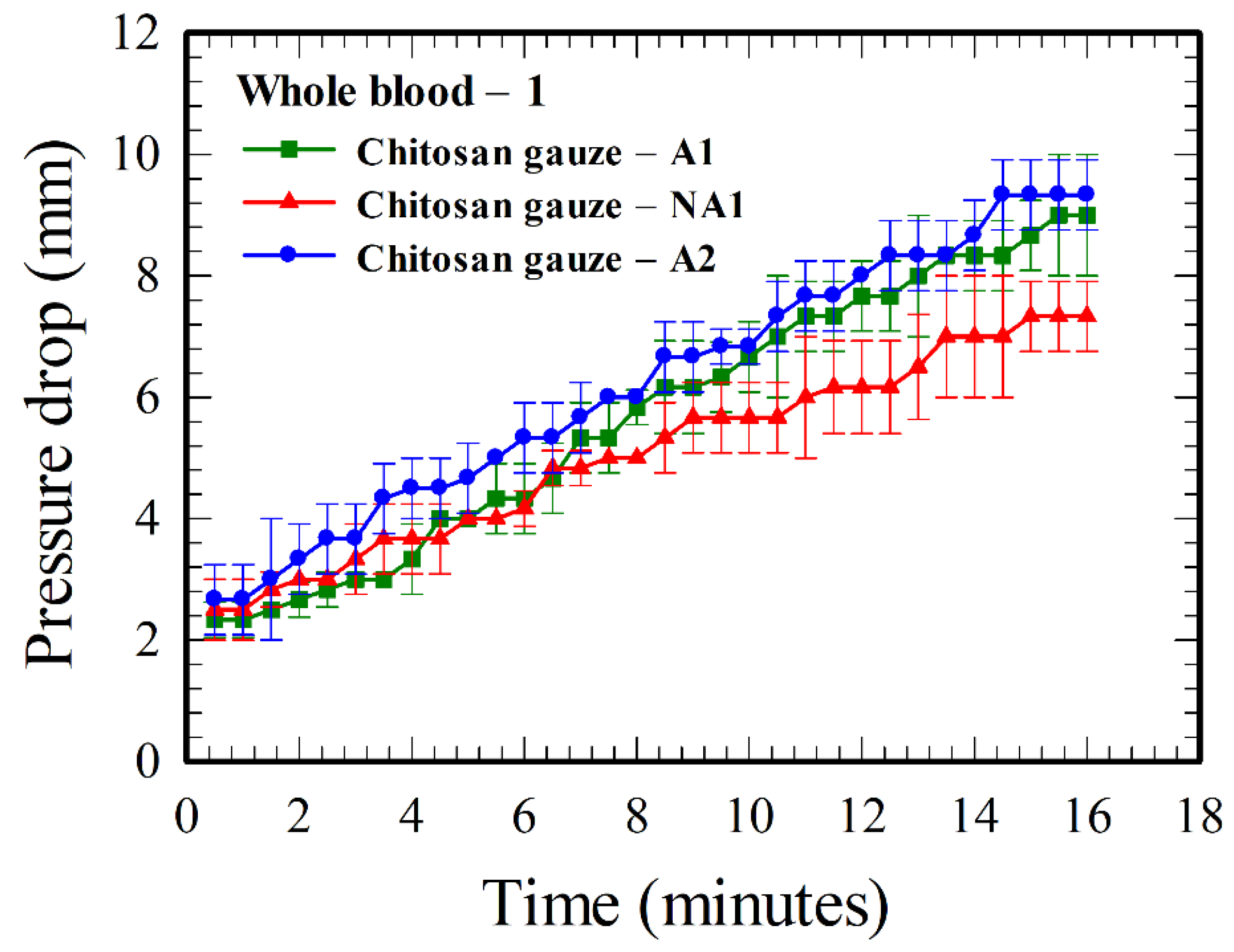
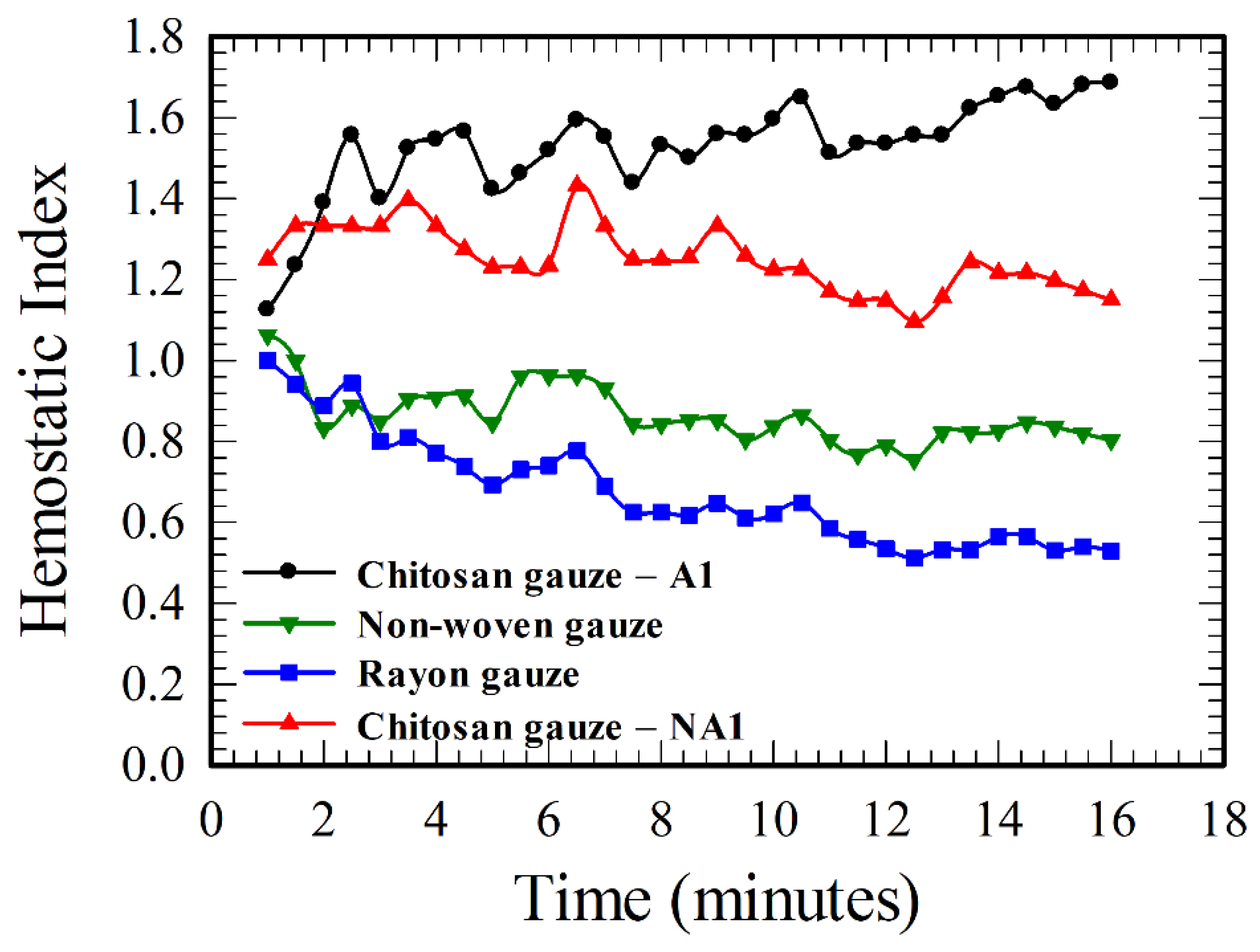
3.1. The Hemostatic Performance of Various Gauzes
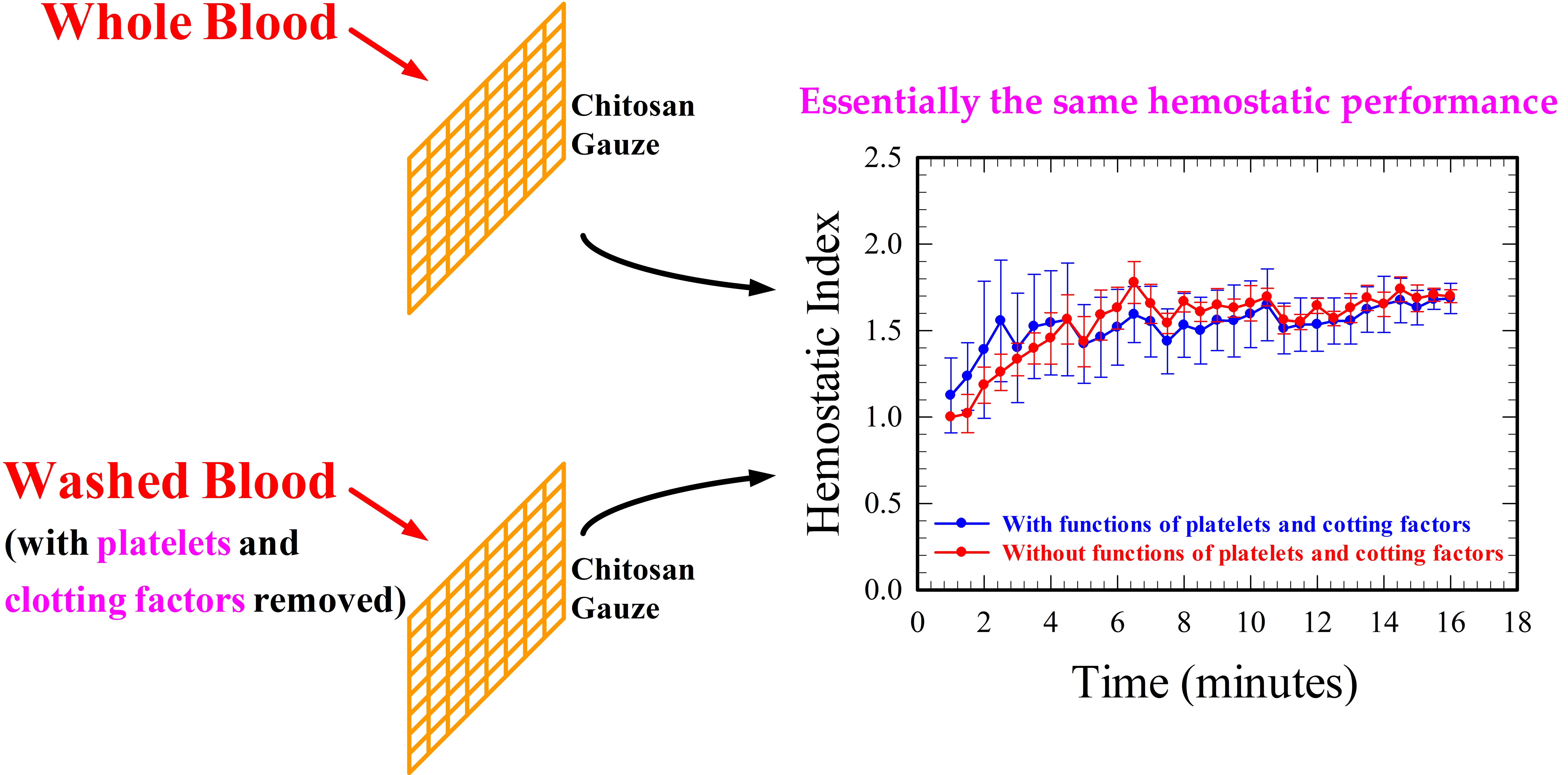
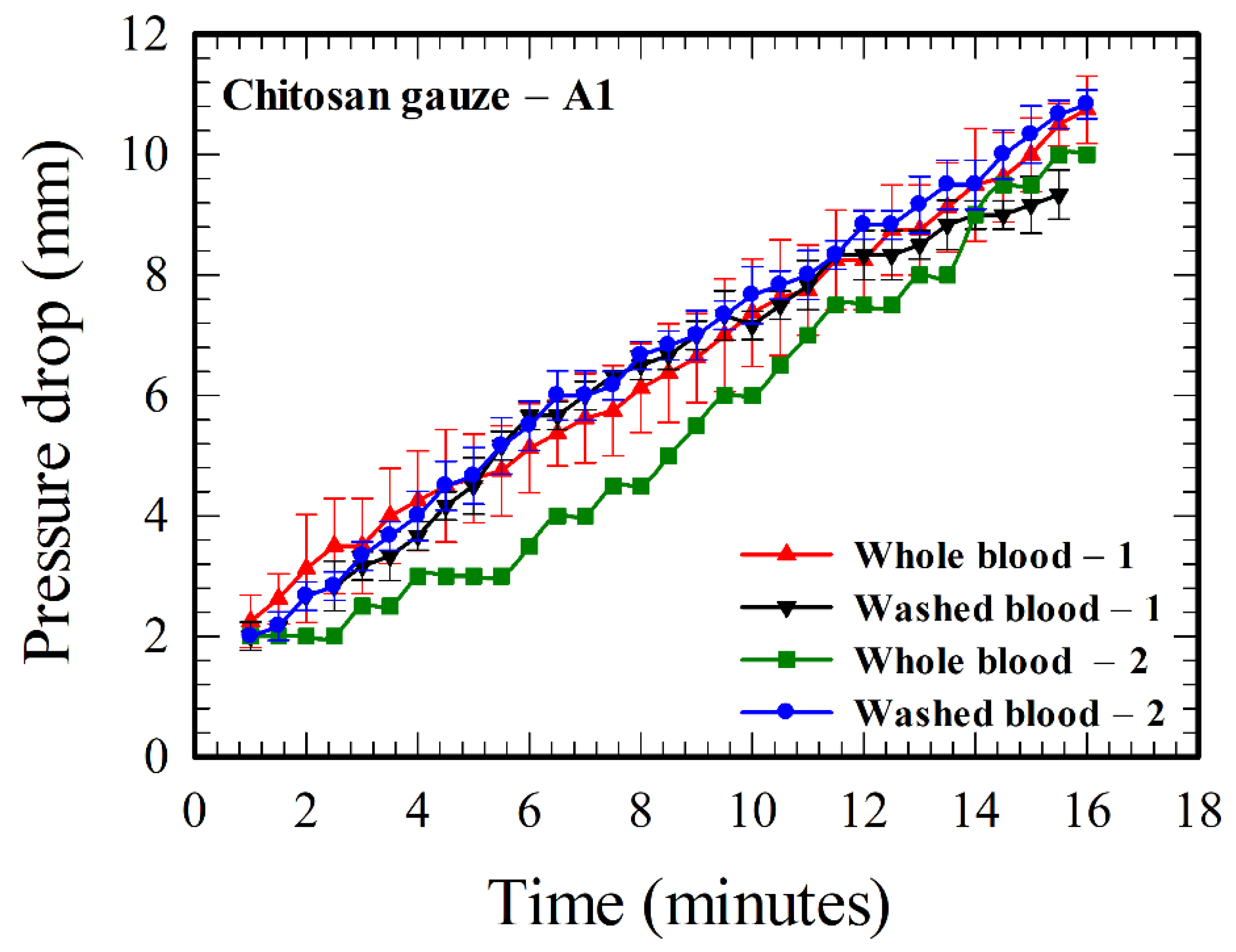
3.2. Tests of the Hemostatic Performance of Chitosan Gauzes Using Whole and Washed Bloods
4. Discussion
4.1. Aspects of the Hemostatic Characteristics of Chitosan Gauzes
4.2. Flow-Through Devices
4.3. Remarks on the Effect of Molecular Weight and Deacetylation Degree of Chitosan
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Measurement Using a Constant Pressure Gradient (CPG) Device


References
- Pillai, C.K.S.; Paul, W.; Sharma, C.P. Chitin and chitosan polymers: Chemistry, solubility and fiber formation. Prog. Polym. Sci. 2009, 34, 641–678. [Google Scholar] [CrossRef]
- Dash, M.; Chiellini, F.; Ottenbrite, R.M.; Vhiellini, F. Chitosan—A versatile semi-synthetic polymer in biomedical applications. Prog. Polym. Sci. 2011, 36, 981–1014. [Google Scholar] [CrossRef]
- Yi, H.; Wu, L.Q.; Bentley, W.E.; Ghodssi, R.; Rubloff, G.W.; Culver, J.N.; Payne, G.F. Biofabrication with chitosan. Biomacromolecules 2005, 6, 2881–2894. [Google Scholar] [CrossRef]
- Dai, T.; Tanaka, M.; Huang, Y.Y.; Hamblin, M.R. Chitosan preparations for wounds and burns: Antimicrobial and wound-healing effects. Expert Rev. Anti Infect. Ther. 2011, 9, 857–879. [Google Scholar] [CrossRef] [PubMed]
- Jayakumar, R.; Prabaharan, M.; Sudheesh Kumar, P.T.; Nair, S.V.; Tamura, H. Biomaterials based on chitin and chitosan in wound dressing applications. Biotechnol. Adv. 2011, 29, 322–337. [Google Scholar] [CrossRef] [PubMed]
- Bennett, B.L.; Littlejohn, L.F.; Kheirabadi, B.S.; Butler, F.K.; Kotwal, R.S.; Dubick, M.A.; Bailey, J.A. Management of external hemorrhage in tactical combat casualty care: Chitosan-based hemostatic gauze dressings. TCCC guidelines—Change 13-05. J. Spec. Oper. Med. 2014, 14, 40–57. [Google Scholar] [PubMed]
- Pusateri, A.E.; Holcomb, J.B.; Kheirabadi, B.S.; Alam, H.B.; Wade, C.E.; Ryan, K.L. Making sense of the preclinical literature on advanced hemostatic products. J. Trauma Injury Infect. Crit. Care 2006, 60, 674–682. [Google Scholar] [CrossRef]
- Gordy, S.D.; Rhee, P.; Schreiber, M.A. Military applications of novel hemostatic devices. Expert Rev. Med. Devices 2011, 8, 41–47. [Google Scholar] [CrossRef]
- Klokkeuold, P.R.; Fukayama, H.; Sung, E.C.; Bertolami, C.N. The effect of chitosan (poly-N-acetylglucosamine) on lingual hemostasis in heparinized rabbits. J. Oral Maxillofac. Surg. 1999, 57, 49–52. [Google Scholar] [CrossRef]
- Millner, R.; Lockhart, A.S.; Marr, R. Chitosan arrests bleeding in major hepatic injuries with clotting dysfunction: An in vivo experimental study in a model of hepatic injury in the presence of moderate systemic heparinisation. Ann. R. Coll. Surg. Engl. 2010, 92, 559–561. [Google Scholar] [CrossRef] [Green Version]
- Brown, M.A.; Daya, M.R.; Worley, J.A. Experience with chitosan dressings in a civilian EMS system. J. Emerg. Med. 2009, 37, 1–7. [Google Scholar] [CrossRef]
- Mlekusch, W.; Dick, P.; Haumer, M.; Sabeti, S.; Minar, E.; Schillinger, M. Arterial puncture site management after percutaneous transluminal procedures using a hemostatic wound dressing (Clo-Sur P.A.D.) versus conventional manual compression: A randomized controlled trial. J. Endovasc. Ther. 2006, 13, 23–31. [Google Scholar] [CrossRef]
- Nguyen, N.; Hasan, S.; Caufield, L.; Ling, F.S.; Narins, C.R. Randomized controlled trial of topical hemostasis pad use for achieving vascular hemostasis following percutaneous coronary intervention. Catheter. Cardiovasc. Interv. 2007, 69, 801–807. [Google Scholar] [CrossRef] [PubMed]
- Ong, S.Y.; Wu, J.; Moochhala, S.M.; Tan, M.H.; Lu, J. Development of a chitosan-based wound dressing with improved hemostatic and antimicrobial properties. Biomaterials 2008, 29, 4323–4332. [Google Scholar] [CrossRef]
- Littlejohn, L.; Bennett, B.L.; Drew, B. Application of current hemorrhage control techniques for backcountry care: Part Two, hemostatic dressings and other adjuncts. Wilderness Environ. Med. 2015, 26, 246–254. [Google Scholar] [CrossRef] [Green Version]
- Chan, L.W.; Kim, C.H.; Wang, X.; Pun, S.H.; White, N.J.; Kim, T.H. PolySTAT-modified chitosan gauzes for improved hemostasis in external hemorrhage. Acta Biomater. 2016, 31, 178–185. [Google Scholar] [CrossRef] [Green Version]
- Chou, T.C.; Fu, E.; Wu, C.J.; Yeh, J.H. Chitosan enhances platelet adhesion and aggregation. Biochem. Biophys. Res. Commun. 2003, 302, 480–483. [Google Scholar] [CrossRef]
- Thatte, H.S.; Zagarins, S.; Khuri, S.F.; Fischer, T.H. Mechanisms of poly-N-acetyl glucosamine polymer-mediated hemostasis: Platelet interactions. J. Trauma Injury Infect. Crit. Care 2004, 57, S13–S21. [Google Scholar] [CrossRef]
- Rao, S.B.; Sharma, C.P. Use of chitosan as a biomaterial: Studies on its safety and hemostatic potential. J. Biomed. Mater. Res. 1997, 34, 21–28. [Google Scholar] [CrossRef]
- Tsao, C.T.; Chang, C.H.; Lin, Y.Y.; Wu, M.F.; Han, J.L.; Hsieh, K.H. Kinetic study of acid depolymerization of chitosan and effects of low molecular weight chitosan on erythrocyte rouleaux formation. Carbohydr. Res. 2011, 346, 94–102. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.Y.; Lin, T.H.; Yang, C.Y.; Kuo, Y.W.; Lei, U. Mechanics for the adhesion and aggregation of red blood cells on chitosan. J. Mech. 2018, 34, 725–732. [Google Scholar] [CrossRef]
- Eylar, E.H.; Madoff, M.A.; Brody, O.V.; Oncley, J.L. The contribution of sialic acid to the surface charge of the erythrocyte. J. Biol. Chem. 1962, 237, 1992–2000. [Google Scholar] [PubMed]
- Kendall, K.; Roberts, A.D. van der Waals forces influencing adhesion of cells. Phil. Trans. R. Soc. B 2015, 370, 20140078. [Google Scholar] [CrossRef] [Green Version]
- Fernandes, H.P.; Cesar, C.L.; Barjas-Castro, M.L. Electrical properties of the red blood cell membrane and immunohematological investigation. Rev. Bras. Hematol. Hemoter. 2011, 33, 297–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, C.; Steffen, P.; Svetina, S. Aggregation of red blood cells: From rouleaux to clot formation. C. R. Phys. 2013, 14, 459–469. [Google Scholar] [CrossRef] [Green Version]
- Israelachvilli, J.N. Intermolecular and Surface Forces, 3rd ed.; Elsevier: London, UK, 2011; ISBN 978-0-12-375182-9. [Google Scholar]
- Yang, J.; Tian, F.; Wang, Z.; Wang, Q.; Zeng, Y.-J.; Chen, S.-Q. Effect of chitosan molecular weight and deacetylation degree on hemostasis. J. Biomed. Mater. Res. Part B Appl. Biomater. 2008, 84B, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Jesty, J.; Wieland, M.; Niemiec, J. Assessment in vitro of the active hemostatic properties of wound dressings. J. Biomed. Mater. Res. Part B Appl. Biomater. 2009, 89B, 536–542. [Google Scholar] [CrossRef]
- Tsao, T. Natural Polymeric Yarn and Its Fabrication Method as well as Application. U.S. Patent US 8776490 B2, July 15, 2014. Available online: https://patents.google.com/patent/US8776490B2/en (accessed on 2 October 2020).
- Tsao, T.; Cherng, J.-H.; Liu, C.-C.; Tang, S.-H. Bandage and Method of Producing the Same. U.S. Patent Application Publication US 2015/0141896 A1, May 21, 2015. Available online: https://patents.google.com/patent/US20150141896 (accessed on 2 October 2020).
- Judd, W.J.; Johnson, S.T.; Storry, J.R. Judd’s Methods in Immunohematology, 3rd ed.; AABB Press: Bethesda, MD, USA, 2008; ISBN 9781563952661. [Google Scholar]
- Segur, J.B.; Oberstar, H.E. Viscosity of glycerol and its aqueous solutions. Ind. Eng. Chem. 1951, 43, 2117–2120. [Google Scholar] [CrossRef]
- Klabunde, R.E. Cardiovascular Physiology Concepts, 2nd ed.; Lippincott Williams & Wilkins: Philadelphia PA, USA, 2012; ISBN 9781451113846. Available online: https://www.cvphysiology.com/Hemodynamics/H011 (accessed on 2 October 2020).
- Correlo, V.M.; Pinho, E.D.; Pashkuleva, I.; Bhattacharya, M.; Nerves, N.M.; Reis, R.L. Water absorption and degradation characteristics of chitosan-based polyesters and hydroxyapatite composites. Macromol. Biosci. 2007, 7, 354–363. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gauze | Average Mesh (μm × μm) | Acidification # |
|---|---|---|
| Chitosan gauze—A1 | 1700 × 550 (85 g/cm2) * | Yes |
| Chitosan gauze—A2 | 350 × 350 (166 g/cm2) * | Yes |
| Chitosan gauze—NA1 | 750 × 600 (130 g/cm2) * | No |
| Cotton gauze | 1200 × 550 | No |
| Non-woven gauze | 1250 × 250 | No |
| Rayon gauze | 2150 × 950 | No |
| Blood Sample | Contents | pH |
|---|---|---|
| Whole blood–1 | Human blood + anticoagulant | 6.60 |
| Whole blood–2 | Human blood + anticoagulant + NaOH | 7.52 |
| Washed blood–1 | Washed RBCs (40%) + Saline (60%) | 7.08 |
| Washed blood–2 | Washed RBCs (50%) + Saline (50%) | 7.55 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, K.-Y.; Chen, Y.-C.; Lin, T.-H.; Yang, C.-Y.; Kuo, Y.-W.; Lei, U. Hemostatic Enhancement via Chitosan Is Independent of Classical Clotting Pathways—A Quantitative Study. Polymers 2020, 12, 2391. https://doi.org/10.3390/polym12102391
Chen K-Y, Chen Y-C, Lin T-H, Yang C-Y, Kuo Y-W, Lei U. Hemostatic Enhancement via Chitosan Is Independent of Classical Clotting Pathways—A Quantitative Study. Polymers. 2020; 12(10):2391. https://doi.org/10.3390/polym12102391
Chicago/Turabian StyleChen, Kuan-Yu, Yen-Cheng Chen, Tzu-Hsin Lin, Cheng-Ying Yang, Ya-Wen Kuo, and U. Lei. 2020. "Hemostatic Enhancement via Chitosan Is Independent of Classical Clotting Pathways—A Quantitative Study" Polymers 12, no. 10: 2391. https://doi.org/10.3390/polym12102391