
Efficacity of Deep Inspiration Breath Hold and Intensity-Modulated Radiotherapy in Preventing Perfusion Defect for Left Sided Breast Cancer (EDIPE): A Prospective Cohort Study Protocol
 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Participants
2.3. Practical Conduct of the Study
2.3.1. Screening Procedures and Baseline Evaluation
2.3.2. Treatment Phase—Radiotherapy
2.3.3. Follow-Up Phase
2.4. Practical Implementation of Cardiac SPECT
2.4.1. Cardiac SPECT Settings
2.4.2. Use of Regadenoson (RAPISCAN®)
2.5. Objectives
2.5.1. Primary Endpoint
2.5.2. Secondary Endpoints
- -
- The incidence of left ventricular wall motion disorder and LVEF quantification on follow-up cardiac SPECT scans at 3-, 6-, and 12-months post-irradiation.
- -
- Measurement of the delivered doses to the cardiac volumes and their substructures.
- -
- The influence of cardiac risk factors on postradiation myocardial perfusion.
- -
- Assessment of the influence of chemotherapy/trastuzumab/trastuzumab emtansine exposure on postradiation myocardial perfusion.
- -
- Assessment of tumor-bed boost location on cardiac dose.
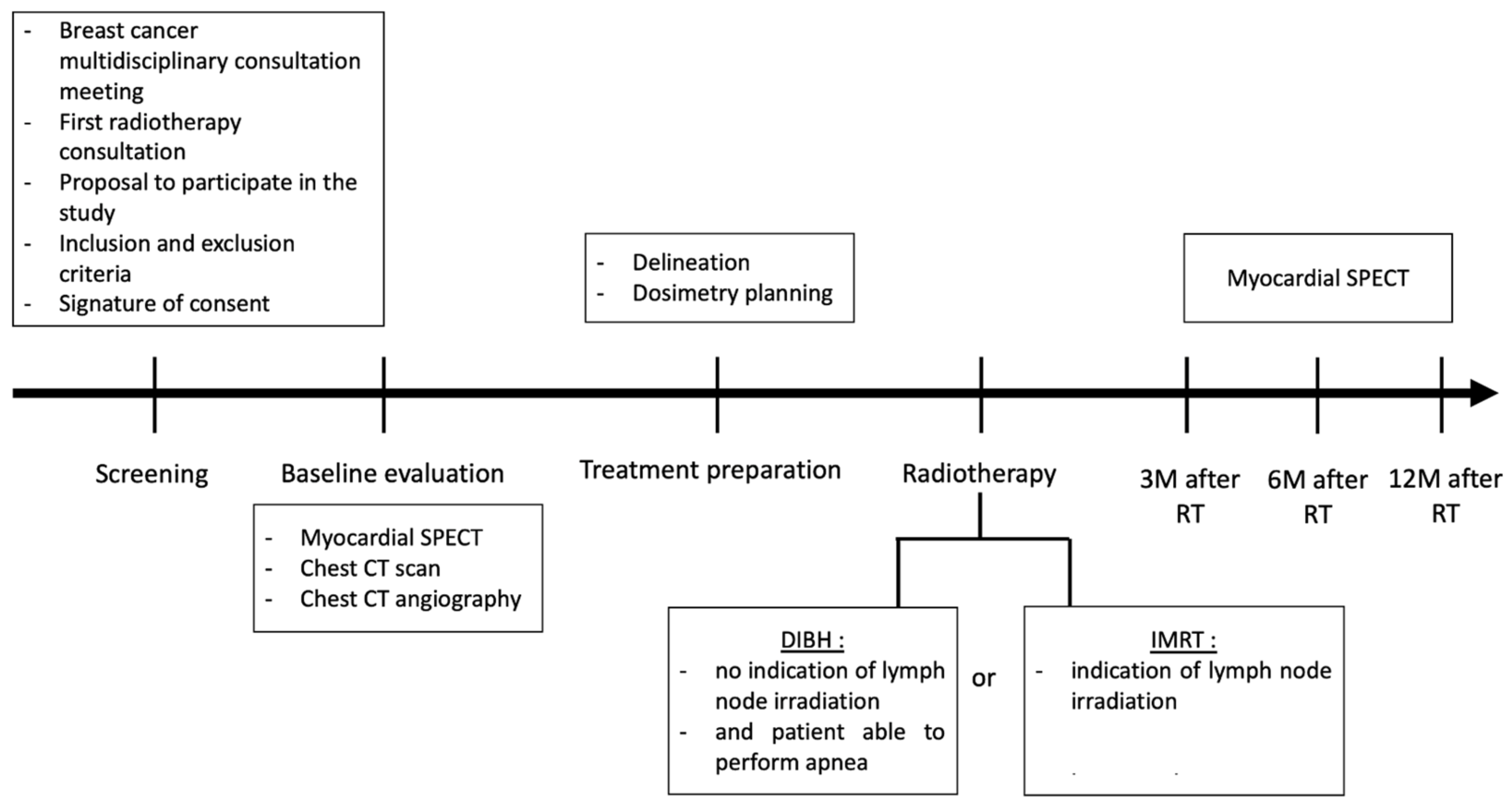
2.6. Participant Timeline
2.7. Data Collection, Management, and Analysis
2.7.1. Assessment of Myocardial Perfusion
2.7.2. Qualitative Scoring of Changes on Cardiac SPECT
2.7.3. Assessment of Ventricular Ejection Function
2.7.4. Assessment of Wall-Thickness Abnormality
2.7.5. Dosimetric Data
2.7.6. Clinical Data
2.7.7. Data Management
2.8. Statistical Analysis
2.8.1. Sample Size
2.8.2. Statistical Methods
2.8.3. Project Duration and Expected Outcomes
3. Discussion
4. Conclusions
5. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Taylor, C.W.; McGale, P.; Darby, S.C. Cardiac risks of breast-cancer radiotherapy: A contemporary view. Clin. Oncol. R. Coll. Radiol. G. B. 2006, 18, 236–246. [Google Scholar] [CrossRef] [PubMed]
- Darby, S.C.; Ewertz, M.; McGale, P.; Bennet, A.M.; Blom-Goldman, U.; Brønnum, D.; Correa, C.; Cutter, D.; Gagliardi, G.; Gigante, B.; et al. Risk of ischemic heart disease in women after radiotherapy for breast cancer. N. Engl. J. Med. 2013, 368, 987–998. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.; Correa, C.; Duane, F.K.; Aznar, M.C.; Anderson, S.J.; Bergh, J.; Dodwell, D.; Ewertz, M.; Gray, R.; Jagsi, R.; et al. Estimating the Risks of Breast Cancer Radiotherapy: Evidence From Modern Radiation Doses to the Lungs and Heart and From Previous Randomized Trials. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2017, 35, 1641–1649. [Google Scholar] [CrossRef]
- Jacobse, J.N.; Duane, F.K.; Boekel, N.B.; Schaapveld, M.; Hauptmann, M.; Hooning, M.J.; Seynaeve, C.M.; Baaijens MH, A.; Gietema, J.A.; Darby, S.C.; et al. Radiation Dose-Response for Risk of Myocardial Infarction in Breast Cancer Survivors. Int. J. Radiat. Oncol. Biol. Phys. 2019, 103, 595–604. [Google Scholar] [CrossRef] [PubMed]
- Marks, L.B.; Yu, X.; Prosnitz, R.G.; Zhou, S.M.; Hardenbergh, P.H.; Blazing, M.; Hollis, D.; Lind, P.; Tisch, A.; Wong, T.Z.; et al. The incidence and functional consequences of RT-associated cardiac perfusion defects. Int. J. Radiat. Oncol. Biol. Phys. 2005, 63, 214–223. [Google Scholar] [CrossRef]
- Heidenreich, P.A.; Hancock, S.L.; Vagelos, R.H.; Lee, B.K.; Schnittger, I. Diastolic dysfunction after mediastinal irradiation. Am. Heart J. 2005, 150, 977–982. [Google Scholar] [CrossRef]
- Yu, X.; Prosnitz, R.R.; Zhou, S.; Hardenberg, P.H.; Tisch, A.; Blazing, M.A.; Borges-Neto, S.; Hollis, D.; Wong, T.; Marks, L.B. Symptomatic cardiac events following radiation therapy for left-sided breast cancer: Possible association with radiation therapy-induced changes in regional perfusion. Clin. Breast Cancer 2003, 4, 193–197. [Google Scholar]
- Eber, J.; Leroy-Freschini, B.; Antoni, D.; Noël, G.; Pflumio, C. Increased cardiac uptake of (18F)-fluorodeoxyglucose incidentally detected on positron emission tomography after left breast irradiation: How to interpret? Cancer Radiother. J. Soc. Fr. Radiother. Oncol. 2022, 26, 724–729. [Google Scholar] [CrossRef]
- Gyenes, G.; Fornander, T.; Carlens, P.; Glas, U.; Rutqvist, L.E. Detection of radiation-induced myocardial damage by technetium-99m sestamibi scintigraphy. Eur. J. Nucl. Med. 1997, 24, 286–292. [Google Scholar]
- Sioka, C.; Exarchopoulos, T.; Tasiou, I.; Tzima, E.; Fotou, N.; Capizzello, A.; Ragos, V.; Tsekeris, P.; Fotopoulos, A. Myocardial perfusion imaging with (99 m)Tc-tetrofosmin SPECT in breast cancer patients that received postoperative radiotherapy: A case-control study. Radiat. Oncol. Lond. Engl. 2011, 6, 151. [Google Scholar] [CrossRef]
- Seddon, B.; Cook, A.; Gothard, L.; Salmon, E.; Latus, K.; Underwood, S.R.; Yarnold, J. Detection of defects in myocardial perfusion imaging in patients with early breast cancer treated with radiotherapy. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2002, 64, 53–63. [Google Scholar] [CrossRef]
- Eftekhari, M.; Anbiaei, R.; Zamani, H.; Fallahi, B.; Beiki, D.; Ameri, A.; Emami-Ardekani, A.; Fard-Esfahani, A.; Gholamrezanezhad, A.; Seid Ratki, K.R.; et al. Radiation-induced myocardial perfusion abnormalities in breast cancer patients following external beam radiation therapy. Asia Ocean. J. Nucl. Med. Biol. 2015, 3, 3–9. [Google Scholar]
- Kaidar-Person, O.; Zagar, T.M.; Oldan, J.D.; Matney, J.; Jones, E.L.; Das, S.; Jensen, B.C.; Zellars, R.C.; Wong, T.Z.; Marks, L.B. Early cardiac perfusion defects after left-sided radiation therapy for breast cancer: Is there a volume response? Breast Cancer Res. Treat. 2017, 164, 253–262. [Google Scholar] [CrossRef]
- Hardenbergh, P.H.; Munley, M.T.; Bentel, G.C.; Kedem, R.; Borges-Neto, S.; Hollis, D.; Prosnitz, L.R.; Marks, L.B. Cardiac perfusion changes in patients treated for breast cancer with radiation therapy and doxorubicin: Preliminary results. Int. J. Radiat. Oncol. Biol. Phys. 2001, 49, 1023–1028. [Google Scholar] [CrossRef]
- Gyenes, G.; Fornander, T.; Carlens, P.; Rutqvist, L.E. Morbidity of ischemic heart disease in early breast cancer 15–20 years after adjuvant radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 1994, 28, 1235–1241. [Google Scholar] [CrossRef]
- Nieder, C.; Schill, S.; Kneschaurek, P.; Molls, M. Influence of different treatment techniques on radiation dose to the LAD coronary artery. Radiat. Oncol. Lond. Engl. 2007, 2, 20. [Google Scholar] [CrossRef]
- Darby, S.C.; Cutter, D.J.; Boerma, M.; Constine, L.S.; Fajardo, L.F.; Kodama, K.; Mabuchi, K.; Marks, L.B.; Mettler, F.A.; Pierce, L.J. Radiation-Related Heart Disease: Current Knowledge and Future Prospects. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, 656–665. [Google Scholar] [CrossRef]
- Gillette, E.L.; McChesney, S.L.; Hoopes, P.J. Isoeffect curves for radiation-induced cardiomyopathy in the dog. Int. J. Radiat. Oncol. Biol. Phys. 1985, 11, 2091–2097. [Google Scholar] [CrossRef]
- Ghita, M.; Gill, E.K.; Walls, G.M.; Edgar, K.S.; McMahon, S.J.; Osorio, E.V.; Bergom, C.; Grieve, D.J.; Watson, C.J.; McWilliam, A.; et al. Cardiac sub-volume targeting demonstrates regional radiosensitivity in the mouse heart. Radiother. Oncol. 2020, 152, 216–221. [Google Scholar] [CrossRef]
- Jacob, S.; Camilleri, J.; Derreumaux, S.; Walker, V.; Lairez, O.; Lapeyre, M.; Bruguière, E.; Pathak, A.; Bernier, M.O.; Laurier, D.; et al. Is mean heart dose a relevant surrogate parameter of left ventricle and coronary arteries exposure during breast cancer radiotherapy: A dosimetric evaluation based on individually-determined radiation dose (BACCARAT study). Radiat. Oncol. Lond. Engl. 2019, 14, 29. [Google Scholar] [CrossRef]
- Eber, J.; Nannini, S.; Chambrelant, I.; Le Fèvre, C.; Noël, G.; Antoni, D. Impact de la radiothérapie thoracique sur les structures cardiaques. Cancer/Radiothérapie 2021, 26, 526–536. [Google Scholar] [CrossRef]
- Feng, M.; Moran, J.M.; Koelling, T.; Chughtai, A.; Chan, J.L.; Freedman, L.; Hayman, J.A.; Jagsi, R.; Jolly, S.; Larouere, J.; et al. Development and validation of a heart atlas to study cardiac exposure to radiation following treatment for breast cancer. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Maffei, N.; Fiorini, L.; Aluisio, G.; D’Angelo, E.; Ferrazza, P.; Vanoni, V.; Lohr, F.; Meduri, B.; Guidi, G. Hierarchical clustering applied to automatic atlas based segmentation of 25 cardiac sub-structures. Phys. Med. 2020, 69, 70–80. [Google Scholar] [CrossRef]
- Loap, P.; Tkatchenko, N.; Goudjil, F.; Ribeiro, M.; Baron, B.; Fourquet, A.; Kirova, Y. Cardiac substructure exposure in breast radiotherapy: A comparison between intensity modulated proton therapy and volumetric modulated arc therapy. Acta Oncol. Stockh. Swed. 2021, 60, 1038–1044. [Google Scholar] [CrossRef] [PubMed]
- Loap, P.; Kirova, Y. Evaluating cardiac substructure radiation exposure in breast rotational intensity modulated radiation therapy: Effects of cancer laterality, fractionation and deep inspiration breath-hold. Cancer Radiother. J. Soc. Fr. Radiother. Oncol. 2021, 25, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Shah, C.; Badiyan, S.; Berry, S.; Khan, A.J.; Goyal, S.; Schulte, K.; Nanavati, A.; Lynch, M.; Vicini, F.A. Cardiac dose sparing and avoidance techniques in breast cancer radiotherapy. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2014, 112, 9–16. [Google Scholar] [CrossRef]
- Loap, P.; Beddok, A.; Cao, K.I.; Goudjil, F.; Fourquet, A.; Dendale, R.; Kirova, Y. Clinical practice of breast cancer protontherapy: A single-centre experience from selection to treatment. Cancer Radiother. J. Soc. Fr. Radiother. Oncol. 2021, 25, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Boda-Heggemann, J.; Knopf, A.C.; Simeonova-Chergou, A.; Wertz, H.; Stieler, F.; Jahnke, A.; Jahnke, L.; Fleckenstein, J.; Vogel, L.; Arns, A.; et al. Deep Inspiration Breath Hold-Based Radiation Therapy: A Clinical Review. Int. J. Radiat. Oncol. Biol. Phys. 2016, 94, 478–492. [Google Scholar] [CrossRef]
- Meattini, I.; Marrazzo, L.; Saieva, C.; Desideri, I.; Scotti, V.; Simontacchi, G.; Bonomo, P.; Greto, D.; Mangoni, M.; Scoccianti, S.; et al. Accelerated Partial-Breast Irradiation Compared With Whole-Breast Irradiation for Early Breast Cancer: Long-Term Results of the Randomized Phase III APBI-IMRT-Florence Trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2020, 38, 4175–4183. [Google Scholar] [CrossRef]
- Ferini, G.; Molino, L.; Tripoli, A.; Valenti, V.; Illari, S.I.; Marchese, V.A.; Cravagno, I.R.; Borzi, G.R. Anatomical Predictors of Dosimetric Advantages for Deep-inspiration-breath-hold 3D-conformal Radiotherapy Among Women With Left Breast Cancer. Anticancer Res. 2021, 41, 1529–1538. [Google Scholar] [CrossRef]
- Ferini, G.; Valenti, V.; Viola, A.; Umana, G.E.; Martorana, E. A Critical Overview of Predictors of Heart Sparing by Deep-Inspiration-Breath-Hold Irradiation in Left-Sided Breast Cancer Patients. Cancers 2022, 14, 3477. [Google Scholar] [CrossRef]
- Ferini, G.; Molino, L. Hypothesis of a decision-making algorithm for adjuvant radiotherapy in left-sided breast cancer patients. Tech. Innov. Patient Support. Radiat. Oncol. 2021, 20, 64–65. [Google Scholar] [CrossRef]
- Zagar, T.M.; Kaidar-Person, O.; Tang, X.; Jones, E.E.; Matney, J.; Das, S.K.; Green, R.L.; Sheikh, A.; Khandani, A.H.; McCartney, W.H.; et al. Utility of Deep Inspiration Breath Hold for Left-Sided Breast Radiation Therapy in Preventing Early Cardiac Perfusion Defects: A Prospective Study. Int. J. Radiat. Oncol. Biol. Phys. 2017, 97, 903–909. [Google Scholar] [CrossRef]
- Chung, E.; Corbett, J.R.; Moran, J.M.; Griffith, K.A.; Marsh, R.B.; Feng, M.; Jagsi, R.; Kessler, M.L.; Ficaro, E.C.; Pierce, L.J. Is there a dose-response relationship for heart disease with low-dose radiation therapy? Int. J. Radiat. Oncol. Biol. Phys. 2013, 85, 959–964. [Google Scholar] [CrossRef]
- Antoni, D.; Natarajan-Ame, S.; Meyer, P.; Niederst, C.; Bourahla, K.; Noel, G. Contribution of three-dimensional conformal intensity-modulated radiation therapy for women affected by bulky stage II supradiaphragmatic Hodgkin disease. Radiat. Oncol. Lond. Engl. 2013, 8, 112. [Google Scholar] [CrossRef]
- Lauche, O.; Kirova, Y.M.; Fenoglietto, P.; Costa, E.; Lemanski, C.; Bourgier, C.; Riou, O.; Tiberi, D.; Campana, F.; Fourquet, A.; et al. Helical tomotherapy and volumetric modulated arc therapy: New therapeutic arms in the breast cancer radiotherapy. World J. Radiol. 2016, 8, 735–742. [Google Scholar] [CrossRef]
- Noël, G.; Antoni, D. Organs at risk radiation dose constraints. Cancer Radiother. J. Soc. Fr. Radiother. Oncol. 2022, 26, 59–75. [Google Scholar] [CrossRef]
- Offersen, B.V.; Boersma, L.J.; Kirkove, C.; Hol, S.; Aznar, M.C.; Biete Sola, A.; Kirova, Y.M.; Pignol, J.P.; Remouchamps, V.; Verhoeven, K.; et al. ESTRO consensus guideline on target volume delineation for elective radiation therapy of early stage breast cancer. Radiother. Oncol. 2015, 114, 3–10. [Google Scholar] [CrossRef]
- Cerqueira, M.D.; Nguyen, P.; Staehr, P.; Underwood, S.R.; Iskandrian, A.E. Effects of Age, Gender, Obesity, and Diabetes on the Efficacy and Safety of the Selective A2A Agonist Regadenoson Versus Adenosine in Myocardial Perfusion Imaging. JACC Cardiovasc. Imaging 2008, 1, 307–316. [Google Scholar] [CrossRef]
- Iskandrian, A.E.; Bateman, T.M.; Belardinelli, L.; Blackburn, B.; Cerqueira, M.D.; Hendel, R.C.; Lieu, H.; Mahmarian, J.J.; Olmsted, A.; Underwood, S.R.; et al. Adenosine versus regadenoson comparative evaluation in myocardial perfusion imaging: Results of the ADVANCE phase 3 multicenter international trial. J. Nucl. Cardiol. Off. Publ. Am. Soc. Nucl. Cardiol. 2007, 14, 645–658. [Google Scholar] [CrossRef]
- Cerqueira, M.D.; Weissman, N.J.; Dilsizian, V.; Jacobs, A.K.; Kaul, S.; Laskey, W.K.; Pennell, D.J.; Rumberger, J.A.; Ryan, T.; Verani, M.S.; et al. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart. A statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association. Circulation 2002, 105, 539–542. [Google Scholar] [PubMed]
- Piroth, M.D.; Baumann, R.; Budach, W.; Dunst, J.; Feyer, P.; Fietkau, R.; Haase, W.; Harms, W.; Hehr, T.; Krug, D.; et al. Heart toxicity from breast cancer radiotherapy. Strahlenther. Onkol. 2019, 195, 1–12. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eber, J.; Blondet, C.; Schmitt, M.; Cox, D.G.; Vit, C.; Le Fèvre, C.; Antoni, D.; Hubele, F.; Noel, G. Efficacity of Deep Inspiration Breath Hold and Intensity-Modulated Radiotherapy in Preventing Perfusion Defect for Left Sided Breast Cancer (EDIPE): A Prospective Cohort Study Protocol. Cancers 2023, 15, 2467. https://doi.org/10.3390/cancers15092467
Eber J, Blondet C, Schmitt M, Cox DG, Vit C, Le Fèvre C, Antoni D, Hubele F, Noel G. Efficacity of Deep Inspiration Breath Hold and Intensity-Modulated Radiotherapy in Preventing Perfusion Defect for Left Sided Breast Cancer (EDIPE): A Prospective Cohort Study Protocol. Cancers. 2023; 15(9):2467. https://doi.org/10.3390/cancers15092467
Chicago/Turabian StyleEber, Jordan, Cyrille Blondet, Martin Schmitt, David G. Cox, Claire Vit, Clara Le Fèvre, Delphine Antoni, Fabrice Hubele, and Georges Noel. 2023. "Efficacity of Deep Inspiration Breath Hold and Intensity-Modulated Radiotherapy in Preventing Perfusion Defect for Left Sided Breast Cancer (EDIPE): A Prospective Cohort Study Protocol" Cancers 15, no. 9: 2467. https://doi.org/10.3390/cancers15092467