
Virtual HDR Boost for Prostate Cancer: Rebooting a Classic Treatment Using Modern Tech
 ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
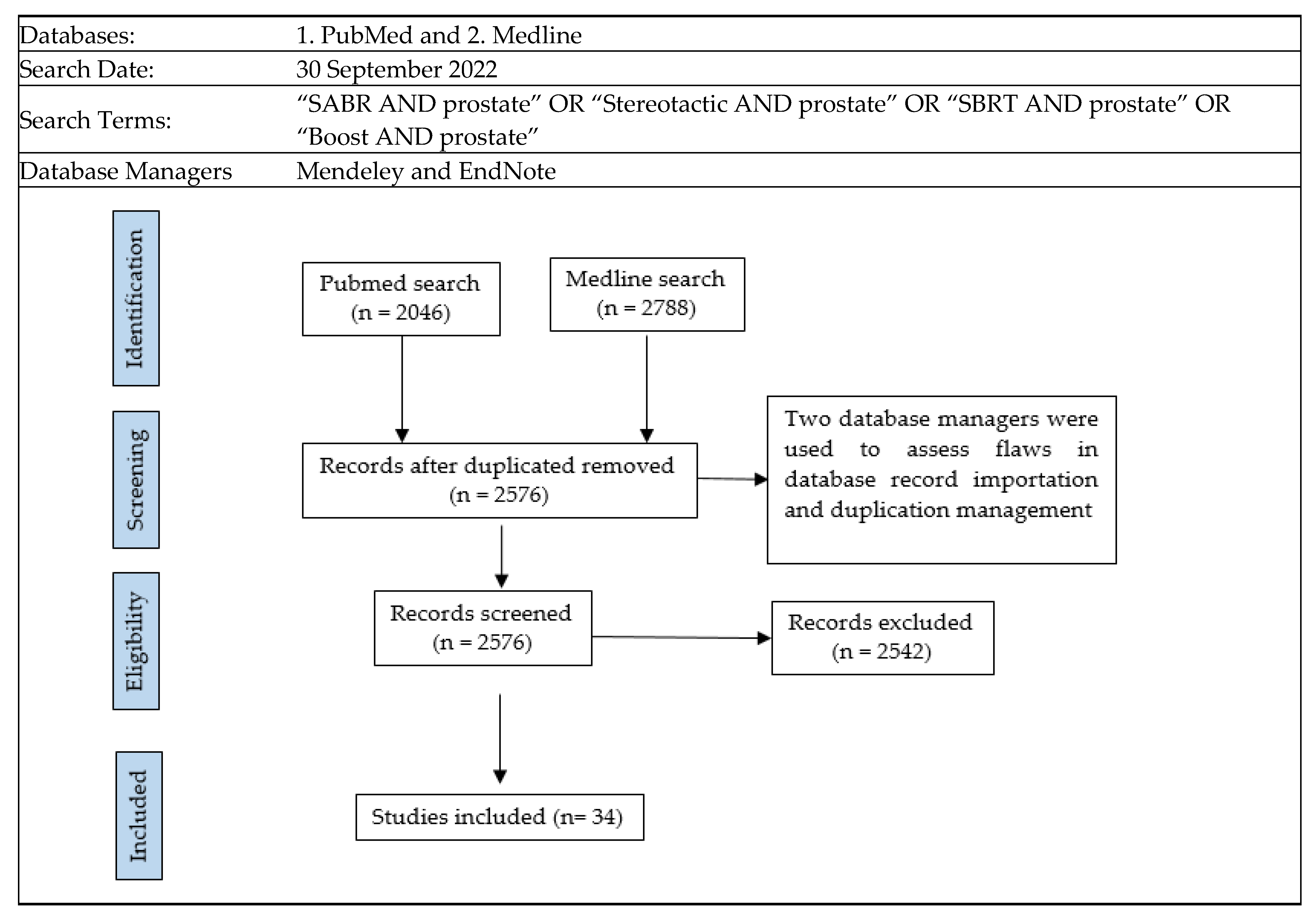
Selection Criteria
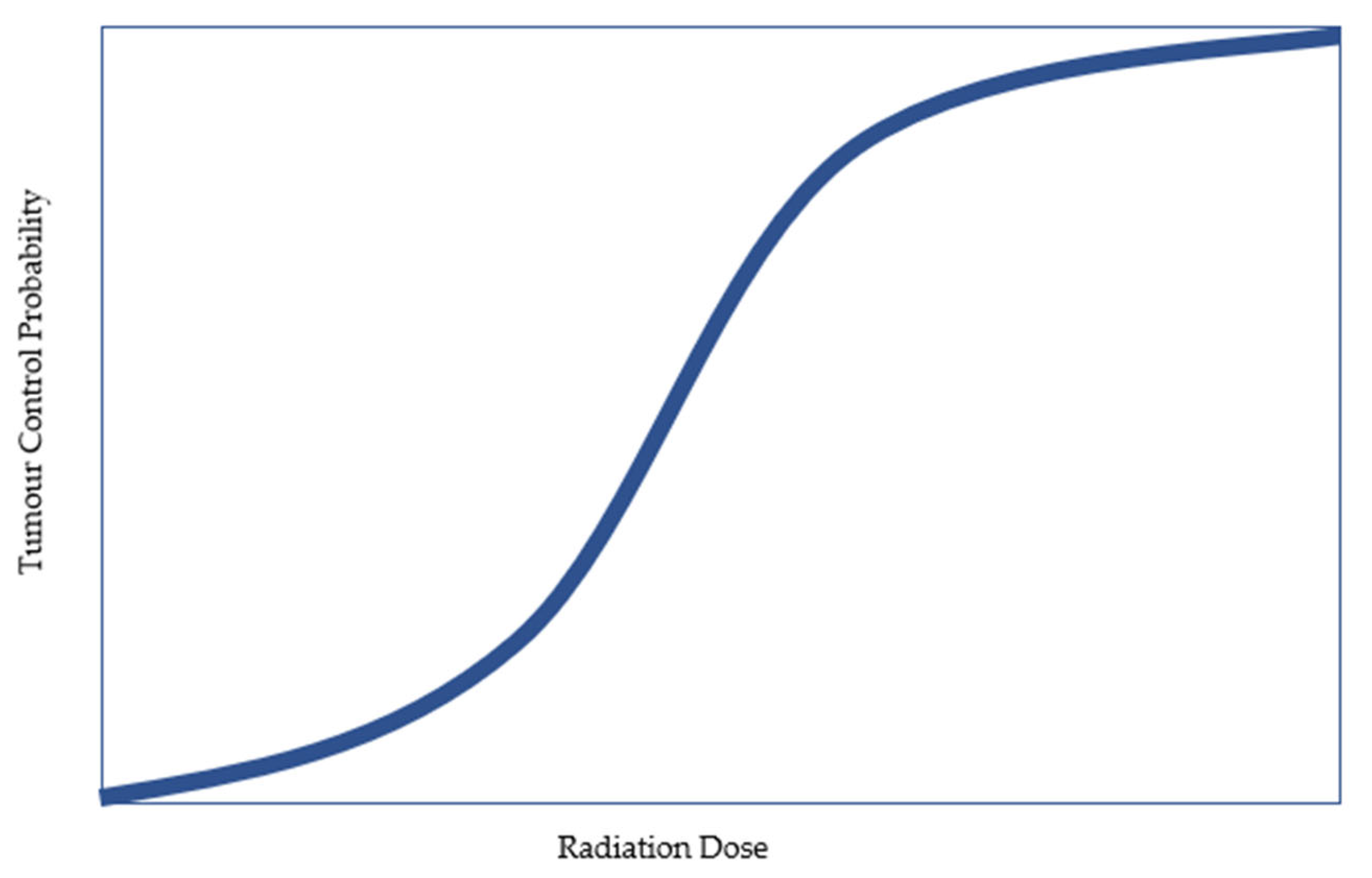
2. Radiation Dose Escalation—Theory and Evidence
3. Brachytherapy as a Dose-Escalation Strategy
4. Diminishing Role of Brachytherapy
5. Emergence of SBRT
5.1. Biochemical Progression-Free Survival
5.2. Toxicities
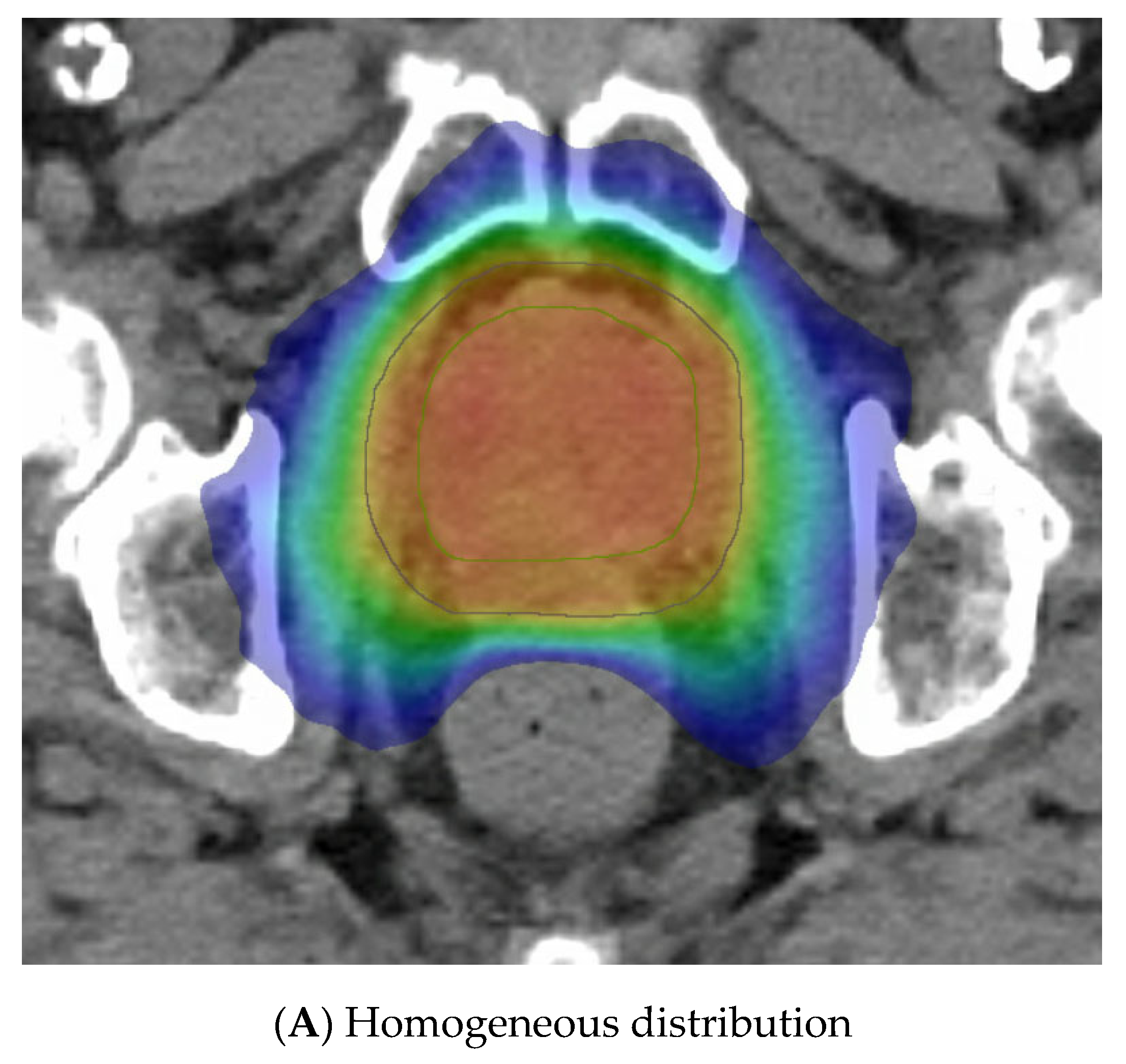
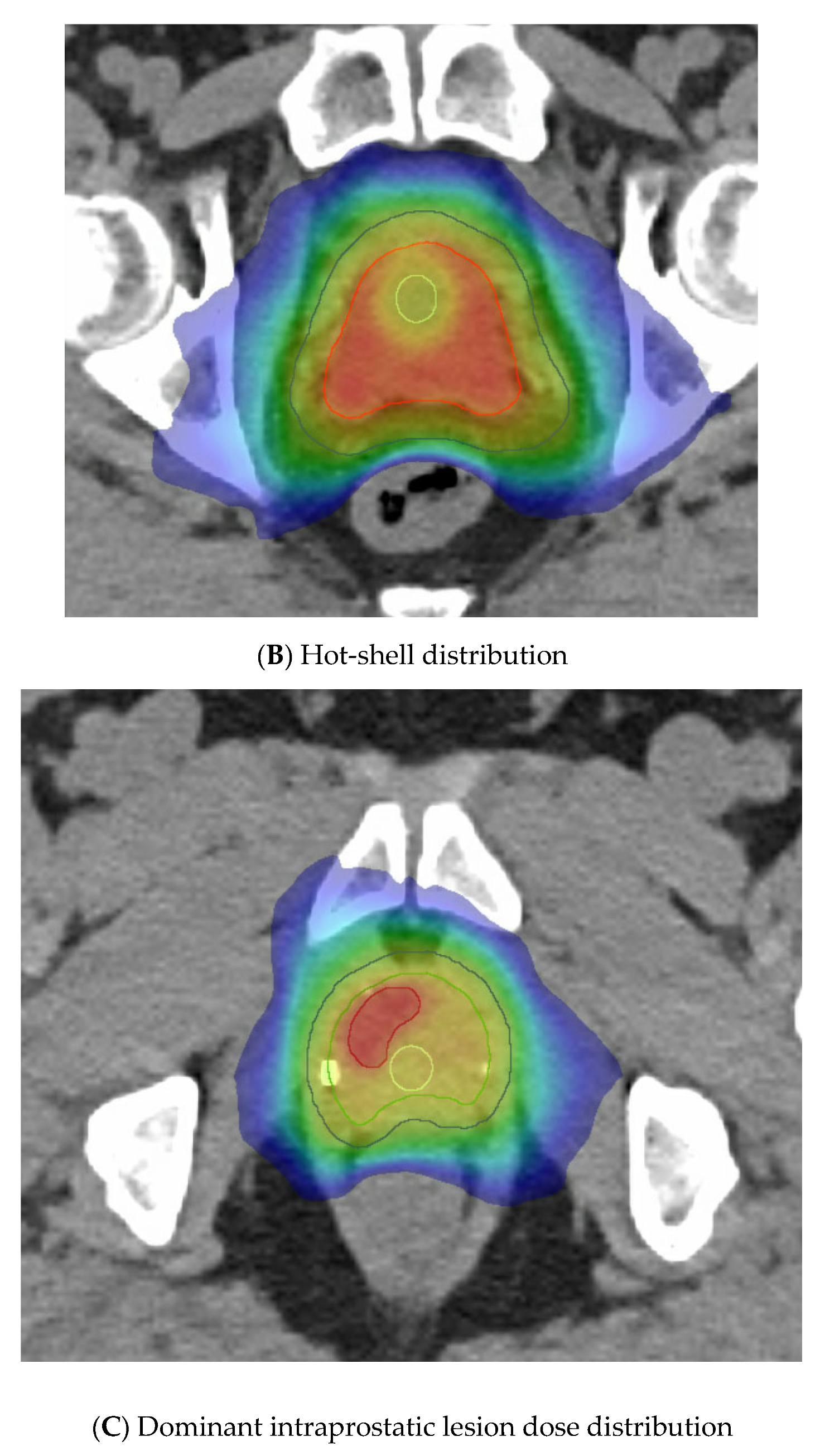
6. SBRT as a Dose-Escalation Strategy—Virtual Boosting
7. Technical Issues with Virtual Boosting
7.1. Simulation Imaging
7.2. Image Guidance
7.3. OAR Stabilization Devices and Hydrogel Spacers
7.4. Radiotherapy Platform
8. Future Directions
9. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hamdy, F.C.; Donovan, J.L.; Lane, J.A.; Mason, M.; Metcalfe, C.; Holding, P.; Davis, M.; Peters, T.J.; Turner, E.L.; Martin, R.M.; et al. 10-Year Outcomes after Monitoring, Surgery, or Radiotherapy for Localized Prostate Cancer. N. Engl. J. Med. 2016, 375, 1415–1424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trada, Y.; Plank, A.; Martin, J. Defining a dose-response relationship for prostate external beam radiotherapy. J. Med. Imaging Radiat. Oncol. 2013, 57, 237–246. [Google Scholar] [CrossRef] [PubMed]
- Matzkin, H.; Chen, J.; Agai, R.; Ziv-Baran, T.; Mabjeesh, N.J. Long-term biochemical progression-free survival following brachytherapy for prostate cancer: Further insight into the role of short-term androgen deprivation and intermediate risk group subclassification. PLoS ONE 2019, 14, e0215582. [Google Scholar] [CrossRef]
- Lazarev, S.; Thompson, M.R.; Stone, N.N.; Stock, R.G. Low-dose-rate brachytherapy for prostate cancer: Outcomes at >10 years of follow-up. BJU Int. 2018, 121, 781–790. [Google Scholar] [CrossRef] [PubMed]
- Dayes, I.S.; Parpia, S.; Gilbert, J.; Julian, J.A.; Davis, I.R.; Levine, M.N.; Sathya, J. Long-Term Results of a Randomized Trial Comparing Iridium Implant Plus External Beam Radiation Therapy with External Beam Radiation Therapy Alone in Node-Negative Locally Advanced Cancer of the Prostate. Int. J. Radiat. Oncol. Biol. Phys. 2017, 99, 90–93. [Google Scholar] [CrossRef] [PubMed]
- Hoskin, P.J.; Rojas, A.M.; Ostler, P.J.; Bryant, L.; Lowe, G.J. Randomised trial of external-beam radiotherapy alone or with high-dose-rate brachytherapy for prostate cancer: Mature 12-year results. Radiother. Oncol. 2021, 154, 214–219. [Google Scholar] [CrossRef]
- Morris, W.J.; Tyldesley, S.; Rodda, S.; Halperin, R.; Pai, H.; McKenzie, M.; Duncan, G.; Morton, G.; Hamm, J.; Murray, N. Androgen Suppression Combined with Elective Nodal and Dose Escalated Radiation Therapy (the ASCENDE-RT Trial): An Analysis of Survival Endpoints for a Randomized Trial Comparing a Low-Dose-Rate Brachytherapy Boost to a Dose-Escalated External Beam Boost for High- and Intermediate-risk Prostate Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2017, 98, 275–285. [Google Scholar] [CrossRef]
- Roberts, M.J.; Papa, N.; Perera, M.; Scott, S.; Teloken, P.E.; Joshi, A.; Vela, I.; Pryor, D.; Martin, J.; Woo, H. A contemporary, nationwide analysis of surgery and radiotherapy treatment for prostate cancer. BJU Int. 2019, 124 (Suppl. S1), 31–36. [Google Scholar] [CrossRef] [Green Version]
- Gomez-Iturriaga, A.; Keyes, M.; Martin, J.; Spratt, D.E. Should brachytherapy be added to external beam radiotherapy for prostate cancer? Lancet Oncol. 2022, 23, 23–25. [Google Scholar] [CrossRef]
- Keall, P.; Nguyen, D.T.; O’Brien, R.; Hewson, E.; Ball, H.; Poulsen, P.; Booth, J.; Greer, P.; Hunter, P.; Wilton, L.; et al. Real-Time Image Guided Ablative Prostate Cancer Radiation Therapy: Results from the TROG 15.01 SPARK Trial. Int. J. Radiat. Oncol. Biol. Phys. 2020, 107, 530–538. [Google Scholar] [CrossRef]
- Widmark, A.; Gunnlaugsson, A.; Beckman, L.; Thellenberg-Karlsson, C.; Hoyer, M.; Lagerlund, M.; Kindblom, J.; Ginman, C.; Johansson, B.; Bjornlinger, K.; et al. Ultra-hypofractionated versus conventionally fractionated radiotherapy for prostate cancer: 5-year outcomes of the HYPO-RT-PC randomised, non-inferiority, phase 3 trial. Lancet 2019, 394, 385–395. [Google Scholar] [CrossRef] [PubMed]
- Tree, A.C.; Ostler, P.; van der Voet, H.; Chu, W.; Loblaw, A.; Ford, D.; Tolan, S.; Jain, S.; Martin, A.; Staffurth, J.; et al. Intensity-modulated radiotherapy versus stereotactic body radiotherapy for prostate cancer (PACE-B): 2-year toxicity results from an open-label, randomised, phase 3, non-inferiority trial. Lancet Oncol. 2022, 23, 1308–1320. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.; Keall, P.; Siva, S.; Greer, P.; Christie, D.; Moore, K.; Dowling, J.; Pryor, D.; Chong, P.; McLeod, N.; et al. TROG 18.01 phase III randomised clinical trial of the Novel Integration of New prostate radiation schedules with adJuvant Androgen deprivation: NINJA study protocol. BMJ Open 2019, 9, e030731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, J.; Sharma, S.; Shumway, R.; Perry, D.; Bydder, S.; Simpson, C.K.; D’Ambrosio, D. Stereotactic Body Radiotherapy for Clinically Localized Prostate Cancer: Toxicity and Biochemical Disease-Free Outcomes from a Multi-Institutional Patient Registry. Cureus 2015, 7, e395. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.J.; Lee, J.S.; Kim, W.C. Long-term outcome of whole pelvis radiotherapy and stereotactic body radiotherapy boost for intermediate and high risk prostate cancer. Int. J. Radiat. Res. 2022, 20, 37–41. [Google Scholar] [CrossRef]
- Kupelian, P.A.; Ciezki, J.; Reddy, C.A.; Klein, E.A.; Mahadevan, A. Effect of increasing radiation doses on local and distant failures in patients with localized prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2008, 71, 16–22. [Google Scholar] [CrossRef]
- Viani, G.A.; Stefano, E.J.; Afonso, S.L. Higher-than-conventional radiation doses in localized prostate cancer treatment: A meta-analysis of randomized, controlled trials. Int. J. Radiat. Oncol. Biol. Phys. 2009, 74, 1405–1418. [Google Scholar] [CrossRef]
- Diez, P.; Vogelius, I.S.; Bentzen, S.M. A new method for synthesizing radiation dose-response data from multiple trials applied to prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2010, 77, 1066–1071. [Google Scholar] [CrossRef] [Green Version]
- Pasalic, D.; Kuban, D.A.; Allen, P.K.; Tang, C.; Mesko, S.M.; Grant, S.R.; Augustyn, A.A.; Frank, S.J.; Choi, S.; Hoffman, K.E.; et al. Dose Escalation for Prostate Adenocarcinoma: A Long-Term Update on the Outcomes of a Phase 3, Single Institution Randomized Clinical Trial. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 790–797. [Google Scholar] [CrossRef]
- Michalski, J.M.; Moughan, J.; Purdy, J.; Bosch, W.; Bruner, D.W.; Bahary, J.P.; Lau, H.; Duclos, M.; Parliament, M.; Morton, G.; et al. Effect of Standard vs Dose-Escalated Radiation Therapy for Patients with Intermediate-Risk Prostate Cancer: The NRG Oncology RTOG 0126 Randomized Clinical Trial. JAMA Oncol. 2018, 4, e180039. [Google Scholar] [CrossRef]
- Hamstra, D.A.; Mariados, N.; Sylvester, J.; Shah, D.; Karsh, L.; Hudes, R.; Beyer, D.; Kurtzman, S.; Bogart, J.; Hsi, R.A.; et al. Continued Benefit to Rectal Separation for Prostate Radiation Therapy: Final Results of a Phase III Trial. Int. J. Radiat. Oncol. Biol. Phys. 2017, 97, 976–985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ratnayake, G.; Martin, J.; Plank, A.; Wong, W. Incremental changes verses a technological quantum leap: The additional value of intensity-modulated radiotherapy beyond image-guided radiotherapy for prostate irradiation. J. Med. Imaging Radiat. Oncol. 2014, 58, 503–510. [Google Scholar] [CrossRef]
- Fowler, J.F. The radiobiology of prostate cancer including new aspects of fractionated radiotherapy. Acta Oncol. 2005, 44, 265–276. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.; Tyldesley, S.; Pai, H.; McKenzie, M.; Halperin, R.; Duncan, G.; Morton, G.; Keyes, M.; Hamm, J.; Morris, W.J. An Updated Analysis of the Survival Endpoints of ASCENDE-RT. Int. J. Radiat. Oncol. Biol. Phys. 2022, 115, 1061–1070. [Google Scholar] [CrossRef] [PubMed]
- Rodda, S.; Tyldesley, S.; Morris, W.J.; Keyes, M.; Halperin, R.; Pai, H.; McKenzie, M.; Duncan, G.; Morton, G.; Hamm, J.; et al. ASCENDE-RT: An Analysis of Treatment-Related Morbidity for a Randomized Trial Comparing a Low-Dose-Rate Brachytherapy Boost with a Dose-Escalated External Beam Boost for High- and Intermediate-Risk Prostate Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2017, 98, 286–295. [Google Scholar] [CrossRef] [Green Version]
- Andring, L.; Yoder, A.; Pezzi, T.; Tang, C.; Kumar, R.; Mahmood, U.; Walker, G.V. PSA: Declining utilization of prostate brachytherapy. Brachytherapy 2022, 21, 6–11. [Google Scholar] [CrossRef]
- Ong, W.L.; Evans, S.M.; Millar, J.L. Under-utilisation of high-dose-rate brachytherapy boost in men with intermediate-high risk prostate cancer treated with external beam radiotherapy. J. Med. Imaging Radiat. Oncol. 2018, 62, 256–261. [Google Scholar] [CrossRef]
- Fuller, D.B.; Naitoh, J.; Lee, C.; Hardy, S.; Jin, H. Virtual HDR CyberKnife treatment for localized prostatic carcinoma: Dosimetry comparison with HDR brachytherapy and preliminary clinical observations. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 1588–1597. [Google Scholar] [CrossRef]
- Miralbell, R.; Moll, M.; Rouzaud, M.; Hidalgo, A.; Toscas, J.I.; Lozano, J.; Sanz, S.; Ares, C.; Jorcano, S.; Linero, D.; et al. Hypofractionated boost to the dominant tumor region with intensity modulated stereotactic radiotherapy for prostate cancer: A sequential dose escalation pilot study. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 50–57. [Google Scholar] [CrossRef]
- Oermann, E.K.; Slack, R.S.; Hanscom, H.N.; Lei, S.; Suy, S.; Park, H.U.; Kim, J.S.; Sherer, B.A.; Collins, B.T.; Satinsky, A.N.; et al. A Pilot Study of Intensity Modulated Radiation Therapy with Hypofractionated Stereotactic Body Radiation Therapy (SBRT) Boost in the Treatment of Intermediate- to High-Risk Prostate Cancer. Technol. Cancer Res. Treat. 2010, 9, 453–462. [Google Scholar] [CrossRef]
- Katz, A.; Kang, J. Stereotactic body radiotherapy with or without external beam radiation as treatment for organ confined high-risk prostate carcinoma: A six year study. Radiat. Oncol. 2014, 9, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katz, A.J.; Santoro, M.; Ashley, R.; Diblasio, F.; Witten, M. Stereotactic Body Radiotherapy as Boost for Organ-confined Prostate Cancer. Technol. Cancer Res. Treat. 2010, 9, 575–582. [Google Scholar] [CrossRef] [PubMed]
- Jabbari, S.; Weinberg, V.K.; Kaprealian, T.; Hsu, I.C.; Ma, L.; Chuang, C.; Descovich, M.; Shiao, S.; Shinohara, K.; Roach, M.; et al. Stereotactic body radiotherapy as monotherapy or post-external beam radiotherapy boost for prostate cancer: Technique, early toxicity, and PSA response. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Anwar, M.; Weinberg, V.; Seymour, Z.; Hsu, I.J.; Roach, M.; Gottschalk, A.R. Outcomes of hypofractionated stereotactic body radiotherapy boost for intermediate and high-risk prostate cancer. Radiat. Oncol. 2016, 11, 8. [Google Scholar] [CrossRef] [Green Version]
- Khmelevsky, E.V.; Kancheli, I.N.; Khoroshkov, V.S.; Kaprin, A.D. Morbidity dynamics in proton–photon or photon radiation therapy for locally advanced prostate cancer. Rep. Pract. Oncol. Radiother. 2018, 23, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Khmelevskiĭ, E.V.; Pan’shin, G.A.; Kancheli, I.N.; Khoroshkov, V.S. Options of hypofractionation of proton boost in locally advanced prostate cancer. Vopr. Onkol. 2012, 58, 787–794. [Google Scholar]
- Lin, Y.W.; Lin, L.C.; Lin, K.L. The early result of whole pelvic radiotherapy and stereotactic body radiotherapy boost for high-risk localized prostate cancer. Front. Oncol. 2014, 4, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Koh, D.-H.; Kim, J.-B.; Kim, H.-W.; Chang, Y.-S.; Kim, H.J. Clinical Outcomes of CyberKnife Radiotherapy in Prostate Cancer Patients: Short-term, Single-Center Experience. Korean J. Urol. 2014, 55, 172–177. [Google Scholar] [CrossRef] [Green Version]
- Freeman, D.; Dickerson, G.; Perman, M. Multi-Institutional Registry for Prostate Cancer Radiosurgery: A Prospective Observational Clinical Trial. Front. Oncol. 2015, 4, 369. [Google Scholar] [CrossRef] [Green Version]
- Mercado, C.; Kress, M.A.; Cyr, R.A.; Chen, L.N.; Yung, T.M.; Bullock, E.G.; Lei, S.; Collins, B.T.; Satinsky, A.N.; Harter, K.W.; et al. Intensity-modulated radiation therapy with stereotactic body radiation therapy boost for unfavorable prostate cancer: The Georgetown University experience. Front. Oncol. 2016, 6, 114. [Google Scholar] [CrossRef] [Green Version]
- Paydar, I.; Pepin, A.; Cyr, R.A.; King, J.; Yung, T.M.; Hartsell, W.F.; Collins, S.P. Intensity-Modulated Radiation Therapy with Stereotactic Body Radiation Therapy Boost for Unfavorable Prostate Cancer: A Report on 3-Year Toxicity. Front. Oncol. 2017, 7, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pontoriero, A.; Iatì, G.; Mondello, S.; Midili, F.; Siragusa, C.; Brogna, A.; Ielo, I.; Anastasi, G.; Magno, C.; Pergolizzi, S.; et al. High-Dose Robotic Stereotactic Body Radiotherapy in the Treatment of Patients With Prostate Cancer: Preliminary Results in 26 Patients. Technol. Cancer Res. Treat. 2016, 15, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Phak, J.H.; Kim, W.C. Prostate-specific antigen kinetics following hypofractionated stereotactic body radiotherapy boost and whole pelvic radiotherapy for intermediate- and high-risk prostate cancer. Asia-Pac. J. Clin. Oncol. 2017, 13, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Phak, J.H.; Kim, W.C. Clinical outcomes of whole pelvis radiotherapy and stereotactic body radiotherapy boost for intermediate- and high-risk prostate cancer. Asia-Pac. J. Clin. Oncol. 2017, 13, e342–e347. [Google Scholar] [CrossRef]
- Phak, J.H.; Kim, H.J.; Kim, W.C. Prostate-specific antigen kinetics following hypofractionated stereotactic body radiotherapy boost as post-external beam radiotherapy versus conventionally fractionated external beam radiotherapy for localized prostate cancer. Prostate Int. 2016, 4, 25–29. [Google Scholar] [CrossRef] [Green Version]
- Pasquier, D.; Nickers, P.; Peiffert, D.; Maingon, P.; Pommier, P.; Lacornerie, T.; Martinage, G.; Tresch, E.; Lartigau, E. Hypofractionated stereotactic boost in intermediate risk prostate carcinoma: Preliminary results of a multicenter phase II trial (CKNO-PRO). PLoS ONE 2017, 12, e0187794. [Google Scholar] [CrossRef] [Green Version]
- Pasquier, D.; Peiffert, D.; Nickers, P.; Maingon, P.; Pommier, P.; Lacornerie, T.; Martinage, G.; Tresch, E.; Lartigau, E. A Multicenter Phase 2 study of Hypofractionated Stereostatic Boost in Intermediate Risk Prostate Carcinoma: A 5-Year Analysis of the CKNO-PRO Trial. Int. J. Radiat. Oncol. Biol. Phys. 2020, 106, 116–123. [Google Scholar] [CrossRef] [Green Version]
- Feng, L.R.; Suy, S.; Collins, S.P.; Lischalk, J.W.; Yuan, B.; Saligan, L.N. Comparison of Late Urinary Symptoms Following SBRT and SBRT with IMRT Supplementation for Prostate Cancer. Curr. Urol. 2018, 11, 218–224. [Google Scholar] [CrossRef]
- Alayed, Y.; Loblaw, A.; Chu, W.; Al-Hanaqta, M.; Chiang, A.; Jain, S.; Chung, H.; Vesprini, D.; Morton, G.; Ravi, A.; et al. Stereotactic Body Radiation Therapy Boost for Intermediate-Risk Prostate Cancer: A Phase 1 Dose-Escalation Study. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 1066–1073. [Google Scholar] [CrossRef]
- Eade, T.; Hruby, G.; Booth, J.; Bromley, R.; Guo, L.; O’Toole, A.; Le, A.; Wu, K.; Whitaker, M.; Rasiah, K.; et al. Results of a Prospective Dose Escalation Study of Linear Accelerator-Based Virtual Brachytherapy (BOOSTER) for Prostate Cancer; Virtual HDR Brachytherapy for Prostate Cancer. Adv. Radiat. Oncol. 2019, 4, 623–630. [Google Scholar] [CrossRef] [Green Version]
- Johansson, S.; Isacsson, U.; Sandin, F.; Turesson, I. High efficacy of hypofractionated proton therapy with 4 fractions of 5 Gy as a boost to 50 Gy photon therapy for localized prostate cancer. Radiother. Oncol. Journal. Eur. Soc. Ther. Radiol. Oncol. 2019, 141, 164–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pryor, D.; Sidhom, M.; Arumugam, S.; Bucci, J.; Gallagher, S.; Smart, J.; Grand, M.; Greer, P.; Keats, S.; Wilton, L.; et al. Phase 2 Multicenter Study of Gantry-Based Stereotactic Radiotherapy Boost for Intermediate and High Risk Prostate Cancer (PROMETHEUS). Front. Oncol. 2019, 9, 217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pollack, A.; Chinea, F.M.; Bossart, E.; Kwon, D.; Abramowitz, M.C.; Lynne, C.; Jorda, M.; Marples, B.; Patel, V.N.; Wu, X.; et al. Phase I Trial of MRI-Guided Prostate Cancer Lattice Extreme Ablative Dose (LEAD) Boost Radiation Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2020, 107, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.-C.; Ting, W.-C.; Chang, Y.-C.; Yang, C.-C.; Lin, L.-C.; Ho, H.-W.; Chu, S.-S.; Lin, Y.-W. Whole Pelvic Radiotherapy with Stereotactic Body Radiotherapy Boost vs. Conventionally Fractionated Radiotherapy for Patients with High or Very High-Risk Prostate Cancer. Front. Oncol. 2020, 10, 814. [Google Scholar] [CrossRef]
- Narang, K.; Kadian, M.; Venkatesan, K.; Mishra, S.; Bisht, S.; Gupta, D.; Banerjee, S.; Kataria, T. Phase I/II Study of Extreme Hypofractionated Stereotactic Body Radiation Therapy Boost to Prostate for Locally Advanced, Node-Positive and Oligometastatic Cancer. Cureus 2020, 12, e11751. [Google Scholar] [CrossRef]
- Kim, Y.J.; Ahn, H.; Kim, C.-S.; Kim, Y.S. Phase I/IIa trial of androgen deprivation therapy, external beam radiotherapy, and stereotactic body radiotherapy boost for high-risk prostate cancer (ADEBAR). Radiat. Oncol. 2020, 15, 234. [Google Scholar] [CrossRef] [PubMed]
- Milecki, P.; Antczak, A.; Milecki, T.; Gluszak, P.; Piotrowski, T.G.; Rucinska, A.; Malicki, J. Ultra-hypofractionated versus Conventionally Fractionated Radiation Therapy Boost for Patients with High-Risk, Localized Prostate Cancer: A 5-Year Results from Randomized HYPO-PROST Trial. Int. J. Radiat. Oncol. Biol. Phys. 2020 108, S62–S63. [CrossRef]
- Turna, M.; Akboru, H.; Ermis, E.; Oskeroglu, S.; Dincer, S.; Altin, S. Stereotactic body radiotherapy as a boost after external beam radiotherapy for high-risk prostate cancer patients. Indian J. Cancer 2021, 58, 518–524. [Google Scholar] [CrossRef]
- Chen, W.C.; Li, Y.; Lazar, A.; Altun, A.; Descovich, M.; Nano, T.; Ziemer, B.; Sudhyadhom, A.; Cunha, A.; Thomas, H.; et al. Stereotactic Body Radiation Therapy and High-Dose-Rate Brachytherapy Boost in Combination with Intensity Modulated Radiation Therapy for Localized Prostate Cancer: A Single-Institution Propensity Score Matched Analysis. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 429–437. [Google Scholar] [CrossRef]
- Phuong, C.; Chan, J.W.; Ni, L.; Wall, P.; Mohamad, O.; Wong, A.C.; Hsu, I.C.; Chang, A.J. Safety of accelerated hypofractionated whole pelvis radiation therapy prior to high dose rate brachytherapy or stereotactic body radiation therapy prostate boost. Radiat. Oncol. 2022, 17, 12. [Google Scholar] [CrossRef]
- Novikov, S.N.; Novikov, R.V.; Merezhko, Y.O.; Gotovchikova, M.Y.; Ilin, N.D.; Melnik, Y.S.; Kanaev, S.V. A comparison between high dose rate brachytherapy and stereotactic body radiotherapy boost after elective pelvic irradiation for high and very high-risk prostate cancer. Radiat. Oncol. J. 2022, 40, 200–207. [Google Scholar] [CrossRef]
- Ferro, M.; de Cobelli, O.; Musi, G.; Del Giudice, F.; Carrieri, G.; Busetto, G.M.; Falagario, U.G.; Sciarra, A.; Maggi, M.; Crocetto, F.; et al. Radiomics in prostate cancer: An up-to-date review. Ther. Adv. Urol. 2022, 14, 17562872221109020. [Google Scholar] [CrossRef]
- Hofman, M.S.; Lawrentschuk, N.; Francis, R.J.; Tang, C.; Vela, I.; Thomas, P.; Rutherford, N.; Martin, J.M.; Frydenberg, M.; Shakher, R.; et al. Prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (proPSMA): A prospective, randomised, multicentre study. Lancet 2020, 395, 1208–1216. [Google Scholar] [CrossRef]
- Koontz, B.F.; Bossi, A.; Cozzarini, C.; Wiegel, T.; D’Amico, A. A systematic review of hypofractionation for primary management of prostate cancer. Eur. Urol. 2015, 68, 683–691. [Google Scholar] [CrossRef] [PubMed]
- Mesci, A.; Isfahanian, N.; Dayes, I.; Lukka, H.; Tsakiridis, T. The Journey of Radiotherapy Dose Escalation in High Risk Prostate Cancer; Conventional Dose Escalation to Stereotactic Body Radiotherapy (SBRT) Boost Treatments. Clin. Genitourin. Cancer 2022, 20, e25–e38. [Google Scholar] [CrossRef] [PubMed]
- Kerkmeijer, L.G.W.; Groen, V.H.; Pos, F.J.; Haustermans, K.; Monninkhof, E.M.; Smeenk, R.J.; Kunze-Busch, M.; de Boer, J.C.J.; van der Voort van Zijp, J.; van Vulpen, M.; et al. Focal Boost to the Intraprostatic Tumor in External Beam Radiotherapy for Patients with Localized Prostate Cancer: Results from the FLAME Randomized Phase III Trial. J. Clin. Oncol. 2021, 39, 787–796. [Google Scholar] [CrossRef]
- Khoo, E.L.; Schick, K.; Plank, A.W.; Poulsen, M.; Wong, W.W.; Middleton, M.; Martin, J.M. Prostate contouring variation: Can it be fixed? Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 1923–1929. [Google Scholar] [CrossRef] [PubMed]
- Keall, P.; Nguyen, D.T.; O’Brien, R.; Booth, J.; Greer, P.; Poulsen, P.; Gebski, V.; Kneebone, A.; Martin, J. Stereotactic prostate adaptive radiotherapy utilising kilovoltage intrafraction monitoring: The TROG 15.01 SPARK trial. BMC Cancer 2017, 17, 180. [Google Scholar] [CrossRef] [Green Version]
- Ng, J.A.; Booth, J.T.; Poulsen, P.R.; Fledelius, W.; Worm, E.S.; Eade, T.; Hegi, F.; Kneebone, A.; Kuncic, Z.; Keall, P.J. Kilovoltage intrafraction monitoring for prostate intensity modulated arc therapy: First clinical results. Int. J. Radiat. Oncol. Biol. Phys. 2012, 84, e655–e661. [Google Scholar] [CrossRef] [Green Version]
- Kishan, A.U.; Ma, T.M.; Lamb, J.M.; Casado, M.; Wilhalme, H.; Low, D.A.; Sheng, K.; Sharma, S.; Nickols, N.G.; Pham, J.; et al. Magnetic Resonance Imaging-Guided vs Computed Tomography-Guided Stereotactic Body Radiotherapy for Prostate Cancer: The MIRAGE Randomized Clinical Trial. JAMA Oncol. 2023, 9, 365–373. [Google Scholar] [CrossRef]
- de Leon, J.; Jameson, M.G.; Rivest-Henault, D.; Keats, S.; Rai, R.; Arumugam, S.; Wilton, L.; Ngo, D.; Liney, G.; Moses, D.; et al. Reduced motion and improved rectal dosimetry through endorectal immobilization for prostate stereotactic body radiotherapy. Br. J. Radiol. 2019, 92, 20190056. [Google Scholar] [CrossRef] [PubMed]
- Wilton, L.; Richardson, M.; Keats, S.; Legge, K.; Hanlon, M.C.; Arumugam, S.; Hunter, P.; Evans, T.J.; Sidhom, M.; Martin, J. Rectal protection in prostate stereotactic radiotherapy: A retrospective exploratory analysis of two rectal displacement devices. J. Med. Radiat. Sci. 2017, 64, 266–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, L.E.; Efstathiou, J.A.; Bhattacharyya, S.K.; Payne, H.A.; Woodward, E.; Pinkawa, M. Association of the Placement of a Perirectal Hydrogel Spacer with the Clinical Outcomes of Men Receiving Radiotherapy for Prostate Cancer: A Systematic Review and Meta-analysis. JAMA Netw. Open 2020, 3, e208221. [Google Scholar] [CrossRef] [PubMed]
- Mariados, N.; Sylvester, J.; Shah, D.; Karsh, L.; Hudes, R.; Beyer, D.; Kurtzman, S.; Bogart, J.; Hsi, R.A.; Kos, M.; et al. Hydrogel Spacer Prospective Multicenter Randomized Controlled Pivotal Trial: Dosimetric and Clinical Effects of Perirectal Spacer Application in Men Undergoing Prostate Image Guided Intensity Modulated Radiation Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2015, 92, 971–977. [Google Scholar] [CrossRef] [Green Version]
- Correa, R.J.M.; Loblaw, A. Stereotactic Body Radiotherapy: Hitting Harder, Faster, and Smarter in High-Risk Prostate Cancer. Front. Oncol. 2022, 12, 889132. [Google Scholar] [CrossRef]
- Dowling, J.A.; Sun, J.; Pichler, P.; Rivest-Henault, D.; Ghose, S.; Richardson, H.; Wratten, C.; Martin, J.; Arm, J.; Best, L.; et al. Automatic Substitute Computed Tomography Generation and Contouring for Magnetic Resonance Imaging (MRI)-Alone External Beam Radiation Therapy from Standard MRI Sequences. Int. J. Radiat. Oncol. Biol. Phys. 2015, 93, 1144–1153. [Google Scholar] [CrossRef] [Green Version]
- Greer, P.; Martin, J.; Sidhom, M.; Hunter, P.; Pichler, P.; Choi, J.H.; Best, L.; Smart, J.; Young, T.; Jameson, M.; et al. A Multi-center Prospective Study for Implementation of an MRI-Only Prostate Treatment Planning Workflow. Front. Oncol. 2019, 9, 826. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Radiotherapy Schedule | Total Dose (Gy) | Dose/Fraction (Gy) | Number of Fractions | Prostate Cancer BED2 (Gy) |
|---|---|---|---|---|
| Conventional (non-dose escalated) | 68 | 2 | 34 | 159 |
| Moderate hypofractionation | 60 | 3 | 20 | 180 |
| Conventional (dose escalated) | 78 | 2 | 39 | 182 |
| Conventional + SBRT boost | 46 19 | 2 9.5 | 23 2 | 107 139 Total: 246 |
| Author/Study | Year | N | Risk | Median Follow-Up (Months) | Conventional Dose | Pelvic Nodal RT | ADT use and Duration | Boost Dose (Target) | Platform (CK, LINAC, Other Particle) | Endpoint | Late Toxicity | Additional Information |
| Miralbel [29] | 2010 | 50 | 5—LR 12—IR 33—HR D’Amico | 72 | 64 Gy/32# | Some 56% | 66% 6 months | 10–16 Gy/2# (DIL) | LINAC | 98% bcDFS | ≥Gr 3 GU 0% GI 10% ≥Gr 2 GU 12% GI 20% RTOG | Pilot study |
| Oermann [30] | 2010 | 24 | 13—IR 11—HR NCCN | 9.3 (month average) | 50.4 Gy/28# | Unknown | 42% Unknown duration | 19.5 Gy/3# (prostate and SVs) | CK | Not reported | No late GI or GU toxicities reported (limited follow-up) CTCAE | Pilot study |
| Katz and Kang [31,32] | 2010 and 2014 | 45 in vHDRB cohort and 52 in SBRT monotherapy cohort | HR NCCN | vHDRB cohort 69 | vHDRB cohort 45 Gy/25# | vHDRB cohort Yes 100%—partial coverage using four-field box | vHDRB cohort 62% Unknown duration | 18–21 Gy/3# (prostate and SVs) | CK | vHDRB cohort 89.5%—IR 77.7%—HR (3 year bFFS) 69% (6 year bcDFS) | vHDRB cohort ≥Gr 3 GU 2.3% GI 0% Gr 2 GU 2.3% GI 13.3% RTOG | Retrospective, 2010 data included larger numbers due to inclusion of intermediate-risk PC |
| SBRT monotherapy cohort 48 | SBRT monotherapy cohort 35–36.25 Gy/5# | SBRT monotherapy cohort No | SBRT monotherapy cohort 50% Unknown duration | SBRT monotherapy cohort 6 year bcDFS—no difference between cohorts (p = 0.86) | SBRT monotherapy cohort ≥Gr 3 GU 3.9% GI 0% Gr 2 GU 7.8% GI 0% RTOG | |||||||
| Jabbari [33] and Anwar [34] | 2012 and 2016 | 48 | 14—IR 34—HR NCCN | 42.7 | 45–50 Gy/25# | Some (if risk >15%, Roach formula) | 88% 6 months | 19–21 Gy/2# (prostate and SVs) | CK | 90% (5 year bNED) | ≥Gr 3 GU 2.1% GI 0% ≥Gr 2 GU 25% GI 0% CTCAE | Pilot study |
| Khmelevsky [35,36] | 2012 and 2018 | 116 in vHDRB cohort and 173 in conventional cohort | LR—HR NCCN | vHDRB cohort 67.8 | vHDRB cohort 44–46 Gy/22–23# | Some (selected IR—HR) | vHDRB cohort 95% 6 months | 28.0–28.8 Gy (radiobiological equivalent of gray)/3–8# | Protons | vHDRB cohort 60% (5 year bcRFS) | vHDRB cohort ≥Gr 3 GU 2.8% GI 0.9% Gr 2 GU 8.3% GI 10.2% RTOG | Randomized |
| Conventional cohort 71.6 | Conventional cohort 68–72 Gy/34–36# | Conventional cohort 95% 6 months | Conventional cohort 61.9% (5 year bcRFS) | Conventional cohort ≥Gr 3 GU 3.8% GI 1.3% Gr 2 GU 9.1% GI 34.8% RTOG | ||||||||
| Lin [37] | 2014 | 41 | 32—HR 9—very HR NCCN | 42 | 45 Gy/25# | Yes 100% | 92.7% 24 months | 21 Gy/3# (prostate and SVs) | CK | 91.9% (4 year bFFS) | ≥Gr 3 GU 0% GI 0% Gr 2 GU 3–11% GI 0% CTCAE | Pilot study |
| Koh [38] | 2014 | 8 in vHDRB cohort and 17 in SBRT monotherapy cohort | vHDRB cohort HR D’Amico | 29.3 (entire cohort) | vHDRB cohort 40 Gy/20# | Unknown | vHDRB cohort 87.5% Unknown duration | 18–24 Gy/3–5# (not reported) | CK | vHDRB cohort 50% bcPFS | vHDRB cohort ≥Gr 3 GU 0% GI 12.5% Gr 2 GU 0% GI 0% RTOG | Retrospective |
| SBRT monotherapy cohort LR—HR D’Amico | SBRT monotherapy cohort 32–37.5 Gy/4–5# | SBRT monotherapy cohort 83.3% for IR 100% for HR Unknown duration | SBRT monotherapy cohort 100% bcPFS for LR-IR 83.3% bcPFS for HR | SBRT monotherapy cohort ≥Gr 3 GU 0% GI 0% Gr 2 GU 0% GI 0% RTOG | ||||||||
| Freeman [39] | 2015 | 160 treated with boost among the total of 2000 in the study | 819—LR 619—IR 172—HR 3—metastatic 130—unspecified NCCN | 24 | 45–50 Gy/25# | Unknown | Unknown | 19.5–21.75 Gy/3# (not reported) | CK | 92%—entire cohort 87%—HR (2 year bcDFS) | ≥Gr 3 GU 0% GI 0.1% Gr 2 not reported Unknown reporting scale | Prospective database, 92% of cohort were SBRT monotherapy patients |
| Mercado [40] and Paydar [41] | 2016 and 2017 | 108 | 4—LR 45—IR 59—HR D’Amico | 53 | 45–50.4 Gy/25–28# | No | 63.6% 6 months | 19.5 Gy/3# (prostate and proximal SVs) | CK | 100%—IR 89.8%—HR (3 year bcPFS) | ≥Gr 3 GU 6% GI 1% Gr 2 GU 40% GI 12% CTCAE | Retrospective |
| Pontoriero [42] | 2016 | 5 in vHDRB cohort and 21 in SBRT monotherapy cohort | vHDRB cohort HR D’Amico | 21.5 (entire cohort) | vHDRB cohort 46 Gy/23# | Yes (100%) | vHDRB cohort 100% 24 months | 19 Gy/2# (not reported) | CK | vHDRB cohort 80% bcPFS | vHDRB cohort ≥Gr 2 GU 0% GI 0% CTCAE | Pilot study |
| SBRT monotherapy cohort LR—IR D’Amico | SBRT monotherapy cohort 38 Gy/4# | SBRT monotherapy cohort 15% 6 months, 46% 24 months | SBRT monotherapy cohort 100% bcPFS | SBRT monotherapy cohort ≥Gr 2 GU 4.8% GI 4.8% CTCAE | ||||||||
| Kim [15,43,44,45] | 2016 (Phak), 2017 (x2), and 2022 | 42 | 31—IR 11—HR NCCN | 84.2 | 45 Gy/25# | Some | No | 21 Gy/3# (prostate and SVs) | CK | 100%—IR 77.8%—HR (8 year bFFS) | ≥Gr 3 GU 0% GI 0% Gr 2 GU 11.9% GI 14.3% RTOG | Phase 1/2a |
| Pasquier/CKNO-PRO) [46,47] | 2017 and 2020 | 76 | IR D’Amico | 62 | 46 Gy/23# | No | No | 18 Gy/3# (prostate) | CK (N = 60) LINAC (N = 16) | 87.4% (5 year bcRFS) | ≥Gr 3 GU 0% GI 3.9% Gr 2 GU 1.4% GI 9.3% CTCAE | Phase 2, multicentre |
| Feng [48] | 2018 | 145 in vHDRB cohort and 200 in SBRT monotherapy cohort | vHDRB cohort 5—LR 51—IR 89—HR D’Amico | vHDRB cohort 24 | vHDRB cohort 45–50.4 Gy/25–28# | Unknown | vHDRB cohort 70.3% Unknown duration | 19.5 Gy/3# (not reported) | CK | vHDRB cohort Not reported | vHDRB cohort 7.60 ± 0.42 AUA symptom score at 1 year 5.5% late urinary flare | Phase 1/2, 1 year AUA symptom scores significantly differed (p = 0.003) |
| SBRT monotherapy cohort 75—LR 104—IR 21—HR D’Amico | SBRT monotherapy cohort 24 | SBRT monotherapy cohort 35–36.25 Gy/5# | SBRT monotherapy cohort 12% Unknown duration | SBRT monotherapy cohort Not reported | SBRT monotherapy cohort 9.53 ± 0.47 AUA symptom score at 1 year 12% late urinary flare | |||||||
| Alayed [49] | 2019 | 30 | IR NCCN | 72 | 37.5 Gy/15# | No | 3.3% <6 months | 10/12.5/15 Gy in single # (prostate and SVs) | LINAC | 92.3% bcPFS | ≥Gr 3 GU 3.3% GI 3.3% ≥Gr 2 GU 43.3% GI 26.6% CTCAE | Phase 1 study |
| Eade/BOOSTER [50] | 2019 | 36 | 13—IR 23—HR D’Amico | 24 | 46 Gy/23# | Some (if HR) | 61% 18 months | 20/22/24 Gy in 2# (prostate) 25/27.5/30 Gy in 2# (to DIL if Identified) | LINAC | 93.3% (3 year bFFS) | ≥Gr 3 GU 0% GI 0% Gr 2 GU 19.3% GI 0% CTCAE | Phase 1 study |
| Johansson [51] | 2019 | 504 | 94—LR 158—IR 135—HR 117—Very HR NCCN | 113 | 50 Gy/25# | Some 16%—HR 60%—very HR | 55% 17% LR 32% IR (5 months) 76% HR (9 months) 91% very HR (24 months) | 20 Gy/4# (prostate and SVs) | Proton | 100%, 94%—LR 94%, 87%—IR 82%, 63%—HR 72%, 55%—very HR (5 and 10 year PSA relapse-free) | ≥Gr 3 GU 2% GI 0% (in pre-treatment symptom-free patients) Gr 2 not reported RTOG at 5 years | Proton boost, retrospective |
| Pryor/PROMETHEUS [52] | 2019 | 135 | 103—IR 32—HR D’Amico | 24 | 46 Gy/23# or 36 Gy/12# | Some (8%) | 54% (36% <6 months and 18% >6 months) | 19–20 Gy/2# (prostate and SVs) | LINAC | 98.6% (2 year bcPFS) | ≥Gr 3 GU 2.2% GI 2% Gr 2 GU 24.9% GI 4.5% CTCAE | Phase 2, multicentre |
| Pollack/LEAD [53] | 2020 | 25 | IR—HR NCCN | 66 | 76 Gy/38# | Some (in HR, 56 Gy/38#) | 56% 6 months | 12–14 Gy/1# (MRI DIL) | Proton | 92% bcPFS | ≥Gr 3 GU 4% GI 0% Gr 2 GU 16% GI 16% CTCAE | Phase 1 using lattice extreme ablative dose technique |
| Wang [54] | 2020 | 121 in vHDRB cohort and 132 in conventional cohort | HR—very HR NCCN | vHDRB cohort 48.5 | vHDRB cohort 45 Gy/25# WPRT | Yes 100% | vHDRB cohort 91.7% Mean: 24.6 months | 21 Gy/3# (prostate and SVs) | CK | vHDRB cohort 93.9% (4 year bFFS) | vHDRB cohort ≥Gr 3 GU 0.8% GI 1.7% Gr 2 GU 19.8% GI 1.7% CTCAE | Retrospective |
| Conventional cohort 41.4 | Conventional cohort 74–79.2 Gy in 1.8–2 Gy/# | Conventional cohort 97.7% Mean: 30.6 months | Conventional cohort 89.1% (4 year bFFS) | Conventional cohort ≥Gr 3 GU 2.3% GI 2.3% Gr 2 GU 15.9% GI 4.5% CTCAE | ||||||||
| Narang [55] | 2020 | 44 | 11—HR 22—very HR 9—node-positive 2—metastatic NCCN | 63.5 | 45 Gy to nodes, 50 Gy to prostate Boost involved nodes (54–56 Gy) All in 25# | Yes 100% | 86.4% 3 months | 18 Gy/3# (prostate) 16 Gy/2# (to bone metastatic lesions) | CK | 91.4% (5 year bcPFS) | ≥Gr 3 GU 4.5% GI 0% Gr 2 not reported CTCAE | Phase 1/2 |
| Kim/ADEBAR [56] | 2020 | 26 | 1—HR 25—very HR NCCN | 35 | 44 Gy/20# | Yes 100% | 100% 25 months | 18—21 Gy/3# (prostate and SVs) | CK | 88.1% (3 year bcRFS) | ≥Gr 3 GU 0% GI 0% Gr 2 GU 4% GI 4% CTCAE | Phase 1/2 |
| Milecki/HYPO-PROST [57] | 2020 | 105 in vHDRB arm and 103 in conventional arm | HR D’Amico | 60.1 | vHDRB arm 46 Gy/23# | Yes | Yes 24 months | 15 Gy/2# (prostate and SVs) | LINAC | vHDRB arm 78.2% (5 year bcRFS) | vHDRB arm ≥Gr 2 GU 5.9% GI 13.9% RTOG | Randomized, abstract only |
| Conventional arm 76 Gy/38# | Conventional arm 82.9% (5 year bcRFS) | Conventional arm ≥Gr 2 GU 5.8% GI 8.6% RTOG | ||||||||||
| Turna [58] | 2021 | 34 | HR D’Amico | 41.2 | 50 Gy/25# WPRT | Yes 100% | 88.2% 36 months | 21 Gy/3# (prostate and proximal SVs) | LINAC | 100% bcPFS | ≥Gr 3 GU 0% GI 0% Gr 2 GU 8% GI 17.6% CTCAE | Retrospective |
| Chen [59] | 2021 | 130 in vHDRB cohort and 101 in HDR brachytherapy boost cohort | 38.2% IR 29% HR 32.8% very HR NCCN | vHDRB cohort 73.4 | 45 Gy/25# | Some | vHDRB cohort 96.2% 6 months | vHDRB cohort 19–21 Gy/2# (prostate and SVs) | CK | vHDRB cohort 88.8%, 85.3% (5 and 10 year BCRF) | vHDRB cohort ≥Gr 3 GU 4.6% GI 1.5% Gr 2 not reported RTOG | Propensity score-matched analysis with HDR brachytherapy boost |
| HDR brachytherapy cohort 186 | HDR brachytherapy cohort 92.1% 6 months | HDR brachytherapy cohort 19 Gy/2# | HDR brachytherapy cohort 91.8%, 74.6% (5 and 10 year BCRF) | HDR brachytherapy cohort ≥Gr 3 GU 3.0% GI 0% Gr 2 not reported RTOG | ||||||||
| Phuong [60] | 2022 | 2 treated with vHDRB boost among the total of 22 in the study | IR—HR NCCN | 32 | 41.25 Gy/15# | Yes 100% | 95% 4 months | 19 Gy/2# (vHDRB) 15 Gy/1# (HDR brachytherapy boost) (prostate and SVs) | CK | 100% (3 year bcPFS) | ≥Gr 3 GU 0% GI 0% Gr 2 GU 14% GI 5% CTCAE | Retrospective, mixed population with SBRT monotherapy |
| Novikov [61] | 2022 | 51 in vHDRB cohort and 98 in HDR brachytherapy cohort | HR, very HR 29.4% of vHDRB cohort were node-positive 32.7% of HDR brachytherapy cohort were node-positive NCCN | vHDRB cohort 55.1 | 45–50.4 Gy/25–28# Some used 3dcrt | Yes 100% | 100% Unknown duration | vHDRB cohort 21 Gy/3# (prostate and proximal SVs) | LINAC | vHDRB cohort 76.5%, 67.7% (3 and 5 year bcRFS) | vHDRB cohort ≥Gr 3 GU 0% GI 5.9% Gr 2 GU 9.8% GI 8.6% CTCAE | Retrospective, no rectal stabilization devices or hydrogel spacers used, significant Gr 3 and 4 toxicity in vHDRB cohort |
| HDR brachytherapy cohort 87.7 | HDR brachytherapy cohort 20 Gy/2# or 15 Gy/1# | HDR brachytherapy cohort 74.6%, 66.8% (3 and 5 year bcRFS) | HDR brachytherapy cohort ≥Gr 3 GU 1.1% GI 0% Gr 2 GU 28.6% GI 8.2% CTCAE |
| Trial Number | Phase | Location | Dose | Accrual Number |
|---|---|---|---|---|
| NINJA/TROG 18.01 | Phase 3 (randomized) | Trans-Tasman Radiation Oncology Group (TROG) | monoSBRT of 40 Gy/5# vs. conventional vHDRB of 36 Gy/12# + boost of 20 Gy/2# | 472 |
| NCT01618851 | Phase 2 | Georgetown University | Conventional treatment of 45 Gy/25# + boost of 19.5 Gy/3# | 70 |
| NCT03564275 | Prospective/matched-pair analysis | University of Cincinnati | Proton boost, no details on dosing | 50 |
| NCT01508390 | Phase 2 | Boston Medical Center | Standard radiotherapy + CK boost of 21 Gy/3# | 35 |
| NCT03380806 | Phase 2 (randomized) | Juravinski Cancer Center | 45 Gy/25# conventional treatment then randomized to either 33–35 Gy/16# or SBRT boost of 19.5–21 Gy/3# | 100 |
| NCT02016248 | Prospective | MemorialCare Health System | 50.4 Gy/28# then CK boost of 27.5 Gy/5# | 167 |
| NCT01839994 | Phase 3 | Maria Sklodowska-Curie National Research Institute of Oncology | Experimental arm: conventional 50 Gy/25# then boost (brachytherapy or SBRT of 20 Gy/2#) | 350 |
| NCT02672449 | Phase 2 | European Institute of Oncology | Conventional 45 Gy/25# + carbon ion boost (16.6 GyE/4#) | 65 |
| NCT03778112 | Prospectiverandomized | Rush University Medical Center | SBRT to whole prostate (36.25 Gy/5#) vs. 45 Gy/25# conventional treatment + 18–21 Gy/3# boost | 58 |
| NCT01985828 | Prospective | Advocate Health Care | 45–50.4 Gy in 25–28# + CK boost of 21 Gy/3# | 72 |
| NCT02307058 | Phase 2 (randomized) | University of Miami | 76 Gy/38# + LEAD (proton boost) of 12–14 Gy/1# vs. 91.2 Gy/39# | 164 |
| NCT02064036 | Not stated | University of California | No details on dose | 29 |
| NCT02339948 | Phase 2 | Genesiscare USA | monoSBRT of 40 Gy/5# vs. 45 Gy/25# conventional treatment + boost of 22 Gy/4# | 279 |
| NCT01352598 | Prospective | Mercy Research | Conventional treatment (dose not specified) + 19–21 Gy/3# boost | 84 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wegener, E.; Samuels, J.; Sidhom, M.; Trada, Y.; Sridharan, S.; Dickson, S.; McLeod, N.; Martin, J.M. Virtual HDR Boost for Prostate Cancer: Rebooting a Classic Treatment Using Modern Tech. Cancers 2023, 15, 2018. https://doi.org/10.3390/cancers15072018
Wegener E, Samuels J, Sidhom M, Trada Y, Sridharan S, Dickson S, McLeod N, Martin JM. Virtual HDR Boost for Prostate Cancer: Rebooting a Classic Treatment Using Modern Tech. Cancers. 2023; 15(7):2018. https://doi.org/10.3390/cancers15072018
Chicago/Turabian StyleWegener, Eric, Justin Samuels, Mark Sidhom, Yuvnik Trada, Swetha Sridharan, Samuel Dickson, Nicholas McLeod, and Jarad M. Martin. 2023. "Virtual HDR Boost for Prostate Cancer: Rebooting a Classic Treatment Using Modern Tech" Cancers 15, no. 7: 2018. https://doi.org/10.3390/cancers15072018