
Local Consolidative Therapy May Have Prominent Clinical Efficacy in Patients with EGFR-Mutant Advanced Lung Adenocarcinoma Treated with First-Line Afatinib

 , , , , , and
, , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
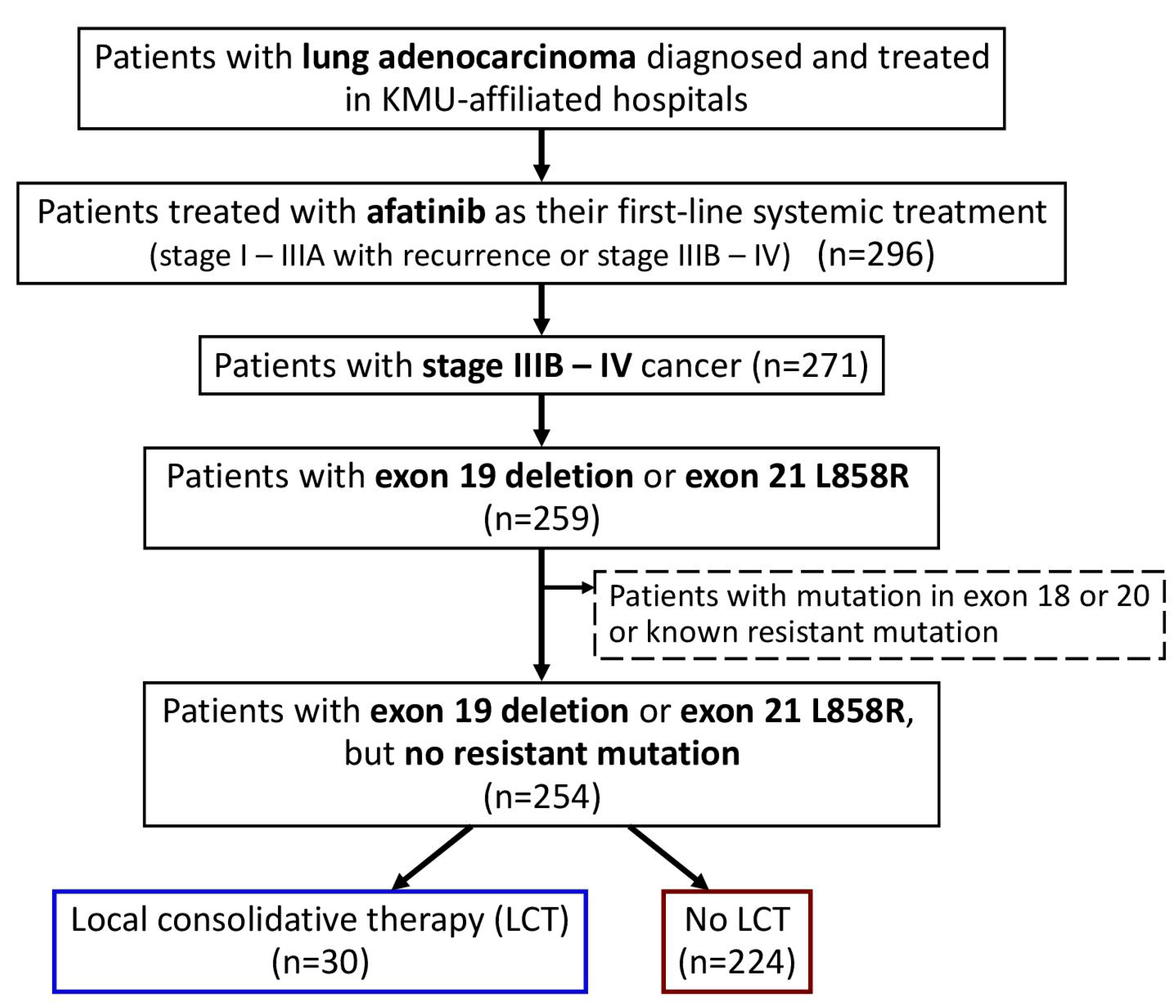
2.1. Patient Identification
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All Patients | LCT | No LCT | p-Value |
|---|---|---|---|---|
| Disease control rate | 249 (98%) | 30 (100%) | 219 (98%) | 0.4085 |
| Response rate | 177 (70%) | 25 (83%) | 152 (68%) | 0.0833 |
| Recurrence | ||||
| No | 85 (33%) | 13 (43%) | 72 (32%) | 0.4514 |
| Single site | 113 (44%) | 12 (40%) | 101 (45%) | |
| Multiple sites | 56 (22%) | 5 (17%) | 51 (23%) | |
| Recurrent site | ||||
| Brain/leptomeningeal | 59 (23%) | 1 (3%) | 58 (26%) | 0.0060 |
| Lung | 91 (36%) | 12 (40%) | 79 (35%) | 0.6117 |
| Pleura/pleural effusion | 39 (15%) | 5 (17%) | 34 (15%) | 0.8319 |
| Bone | 33 (13%) | 2 (7%) | 31 (14%) | 0.2725 |
| Liver | 16 (6%) | 1 (3%) | 15 (7%) | 0.4765 |
| Adrenal gland | 2 (1%) | 0 (0%) | 2 (1%) | 0.6033 |
| Other | 10 (4%) | 1 (3%) | 9 (4%) | 0.8563 |
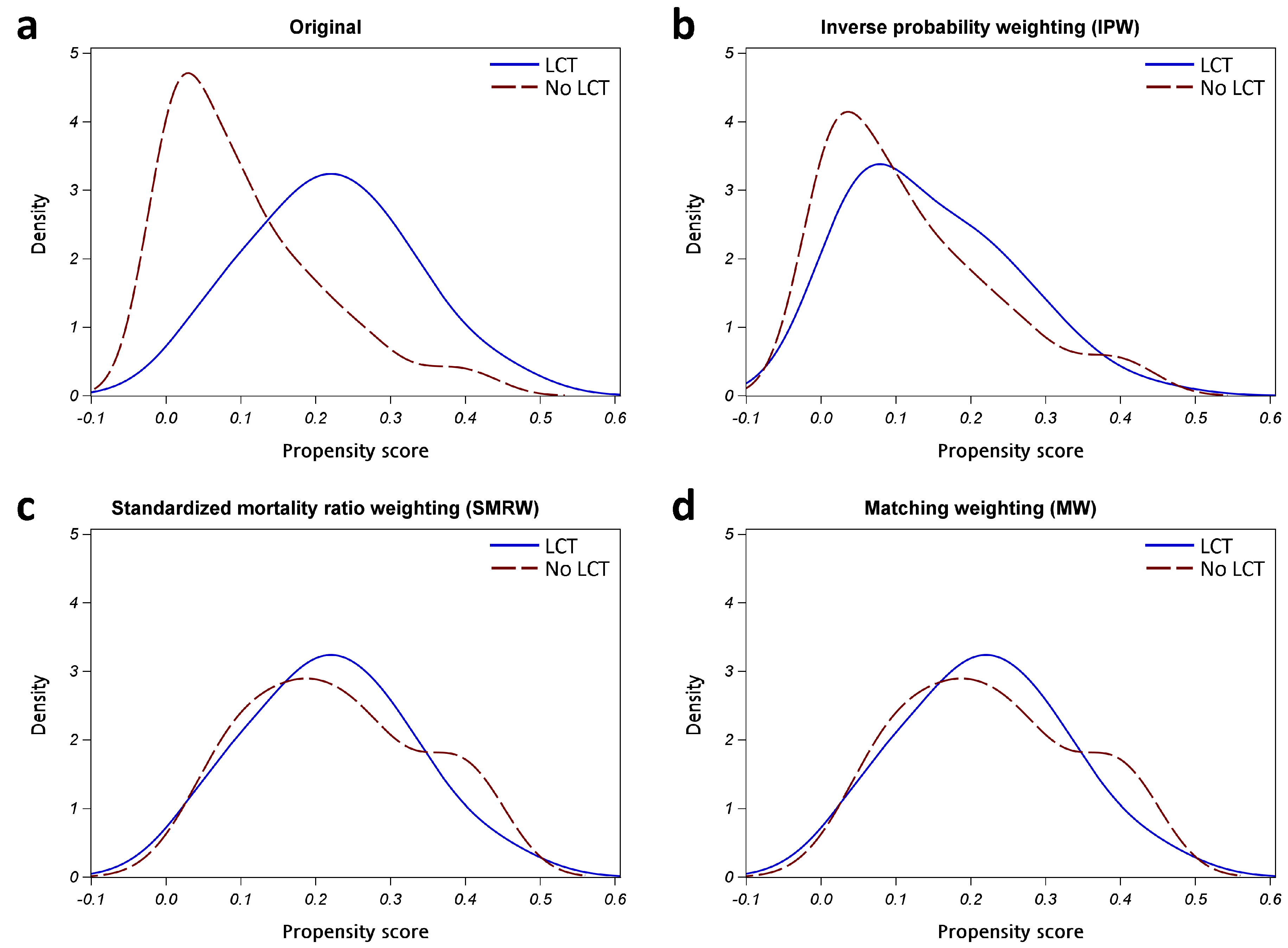
| Variables | No Weighting | Inverse Probability Weighting (IPW) | Standardized Mortality Ratio Weighting (SMRW) | Matching Weighting (MW) |
|---|---|---|---|---|
| Weighted sample size | ||||
| LCT | 30 | 206.0767 | 30 | 30 |
| No LCT | 224 | 254.3010 | 30.3010 | 30.3010 |
| Effective sample size (ESS) | ||||
| LCT | 30 | 14.9843 | 30 | 30 |
| No LCT | 224 | 219.6106 | 93.0320 | 93.0320 |
| Sum | 254 | 234.5949 | 123.032 | 123.032 |
| SMD of covariates | ||||
| Sex | −0.1961 | −0.1812 | 0.0188 | 0.0188 |
| Age | 0.0479 | −0.0113 | 0.0115 | 0.0115 |
| Smoking | −0.2149 | −0.0117 | −0.0143 | −0.0143 |
| ECOG performance status | −0.5878 | −0.5461 | −0.0008 | −0.0008 |
| Exon of EGFR mutation | −0.2534 | −0.0145 | 0.0420 | 0.0420 |
| Brain metastasis | −0.6705 | −0.0348 | −0.0028 | −0.0028 |
| Lung metastasis | −0.2059 | −0.2394 | 0.0318 | 0.0318 |
| Pleural metastasis/effusion | −0.4286 | −0.0410 | 0.0185 | 0.0185 |
| Bone metastasis | −0.1025 | 0.0974 | 0.0132 | 0.0132 |
| Liver metastasis | −0.3818 | −0.2234 | 0.0038 | 0.0038 |
| Adrenal metastasis | −0.2197 | −0.1650 | −0.0028 | −0.0028 |
| Other metastasis | −0.1881 | −0.0543 | −0.0028 | −0.0028 |
| Hazard ratio [95% CI] for PFS | ||||
| LCT (vs. no) | 0.43 [0.26–0.72] ** | 0.40 [0.32–0.51] *** | 0.51 [0.27–0.97] * | 0.51 [0.27–0.97] * |
| Hazard ratio [95% CI] for OS | ||||
| LCT (vs. no) | 0.32 [0.16–0.66] ** | 0.25 [0.17–0.36] *** | 0.41 [0.17–0.97] * | 0.41 [0.17–0.97] * |
| Variables | All Patients | LCT | No LCT | SMD | p-Value |
|---|---|---|---|---|---|
| n | 123.0 | 30 | 93.0 | ||
| Age (year) | 64.7 ± 4.6 | 64.7 ± 9.2 | 64.7 ± 3.5 | 0.0115 | 0.9457 |
| Sex | |||||
| Female | 42.5 (17%) | 21 (70%) | 21.5 (71%) | 0.0188 | 0.9419 |
| Male | 17.8 (7%) | 9 (30%) | 8.8 (29%) | ||
| Smoking | |||||
| Never | 52.1 (21%) | 26 (87%) | 26.1 (86%) | −0.0143 | 0.9559 |
| Ever | 8.2 (3%) | 4 (13%) | 4.2 (14%) | ||
| ECOG performance status | |||||
| 0–1 | 60.3 (24%) | 30 (100%) | 30.3 (100%) | −0.0008 | 0.9974 |
| ≥2 | 0.0 (0%) | 0 (0%) | 0.0 (0%) | ||
| EGFR mutation | |||||
| Exon 19 deletion | 38.8 (15%) | 19 (63%) | 19.8 (65%) | 0.0420 | 0.8706 |
| Exon 21 L858R | 21.5 (8%) | 11 (37%) | 10.5 (35%) | ||
| Metastasis | |||||
| Brain/leptomeningeal metastasis | 4.0 (2%) | 2 (7%) | 2.0 (7%) | −0.0028 | 0.9914 |
| Lung metastasis | 25.7 (10%) | 13 (43%) | 12.7 (42%) | 0.0318 | 0.9019 |
| Pleural metastasis/effusion | 15.8 (6%) | 8 (27%) | 7.8 (26%) | 0.0185 | 0.9427 |
| Bone metastasis | 27.9 (11%) | 14 (47%) | 13.9 (46%) | 0.0132 | 0.9593 |
| Liver metastasis | 2.0 (1%) | 1 (3%) | 1.0 (3%) | 0.0038 | 0.9882 |
| Adrenal metastasis | 2.0 (1%) | 1 (3%) | 1.0 (3%) | −0.0028 | 0.9914 |
| Other metastasis | 2.0 (1%) | 1 (3%) | 1.0 (3%) | −0.0028 | 0.9913 |



References
- Fisher, M.D.; D’Orazio, A. Phase II and III trials: Comparison of four chemotherapy regimens in advanced non small-cell lung cancer (ECOG 1594). Clin. Lung Cancer 2000, 2, 21–22. [Google Scholar] [PubMed]
- Greenhalgh, J.; Boland, A.; Bates, V.; Vecchio, F.; Dundar, Y.; Chaplin, M.; Green, J.A. First-line treatment of advanced epidermal growth factor receptor (EGFR) mutation positive non-squamous non-small cell lung cancer. Cochrane Database Syst. Rev. 2021, 3, CD010383. [Google Scholar] [CrossRef] [PubMed]
- Maemondo, M.; Inoue, A.; Kobayashi, K.; Sugawara, S.; Oizumi, S.; Isobe, H.; Gemma, A.; Harada, M.; Yoshizawa, H.; Kinoshita, I.; et al. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N. Engl. J. Med. 2010, 362, 2380–2388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mok, T.S.; Wu, Y.L.; Thongprasert, S.; Yang, C.H.; Chu, D.T.; Saijo, N.; Sunpaweravong, P.; Han, B.; Margono, B.; Ichinose, Y.; et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N. Engl. J. Med. 2009, 361, 947–957. [Google Scholar] [CrossRef] [PubMed]
- Takeda, M.; Okamoto, I.; Nakagawa, K. Pooled safety analysis of EGFR-TKI treatment for EGFR mutation-positive non-small cell lung cancer. Lung Cancer 2015, 88, 74–79. [Google Scholar] [CrossRef]
- Park, K.; Tan, E.H.; O’Byrne, K.; Zhang, L.; Boyer, M.; Mok, T.; Hirsh, V.; Yang, J.C.; Lee, K.H.; Lu, S.; et al. Afatinib versus gefitinib as first-line treatment of patients with EGFR mutation-positive non-small-cell lung cancer (LUX-Lung 7): A phase 2B, open-label, randomised controlled trial. Lancet Oncol. 2016, 17, 577–589. [Google Scholar] [CrossRef]
- Yang, J.C.; Wu, Y.L.; Schuler, M.; Sebastian, M.; Popat, S.; Yamamoto, N.; Zhou, C.; Hu, C.P.; O’Byrne, K.; Feng, J.; et al. Afatinib versus cisplatin-based chemotherapy for EGFR mutation-positive lung adenocarcinoma (LUX-Lung 3 and LUX-Lung 6): Analysis of overall survival data from two randomised, phase 3 trials. Lancet Oncol. 2015, 16, 141–151. [Google Scholar] [CrossRef] [Green Version]
- Liang, S.K.; Lee, M.R.; Liao, W.Y.; Ho, C.C.; Ko, J.C.; Shih, J.Y. Prognostic factors of afatinib as a first-line therapy for advanced EGFR mutation-positive lung adenocarcinoma: A real-world, large cohort study. Oncotarget 2018, 9, 23749–23760. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Tan, E.H.; O’Byrne, K.; Zhang, L.; Hirsh, V.; Boyer, M.; Yang, J.C.; Mok, T.; Lee, K.H.; Lu, S.; et al. Afatinib versus gefitinib in patients with EGFR mutation-positive advanced non-small-cell lung cancer: Overall survival data from the phase IIb LUX-Lung 7 trial. Ann. Oncol. 2017, 28, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Tamura, K.; Nukiwa, T.; Gemma, A.; Yamamoto, N.; Mizushima, M.; Ochai, K.; Ikeda, R.; Azuma, H.; Nakanishi, Y. Real-world treatment of over 1600 Japanese patients with EGFR mutation-positive non-small cell lung cancer with daily afatinib. Int. J. Clin. Oncol. 2019, 24, 917–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, H.; Taima, K.; Itoga, M.; Ishioka, Y.; Baba, K.; Shiratori, T.; Sakamoto, H.; Tsuchiya, J.; Nakagawa, H.; Hasegawa, Y.; et al. Real-world study of afatinib in first-line or re-challenge settings for patients with EGFR mutant non-small cell lung cancer. Med. Oncol. 2019, 36, 57. [Google Scholar] [CrossRef] [Green Version]
- Yokoyama, T.; Yoshioka, H.; Fujimoto, D.; Demura, Y.; Hirano, K.; Kawai, T.; Kagami, R.; Washio, Y.; Ishida, T.; Kogo, M.; et al. A phase II study of low starting dose of afatinib as first-line treatment in patients with EGFR mutation-positive non-small-cell lung cancer (KTORG1402). Lung Cancer 2019, 135, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Huang, M.Y.; Hsieh, K.P.; Huang, R.Y.; Hung, J.Y.; Chen, L.T.; Tsai, M.J.; Yang, Y.H. Comparing survival and subsequent treatment of first-line tyrosine kinase inhibitors in patients of advanced lung adenocarcinoma with epidermal growth factor receptor mutation. J. Formos. Med. Assoc. 2022, 121, 170–180. [Google Scholar] [CrossRef]
- Chen, Y.C.; Tsai, M.J.; Lee, M.H.; Kuo, C.Y.; Shen, M.C.; Tsai, Y.M.; Chen, H.C.; Hung, J.Y.; Huang, M.S.; Chong, I.W.; et al. Lower starting dose of afatinib for the treatment of metastatic lung adenocarcinoma harboring exon 21 and exon 19 mutations. Bmc Cancer 2021, 21, 495. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.J.; Tsai, M.J.; Hung, J.Y.; Lee, M.H.; Tsai, Y.M.; Tsai, Y.C.; Hsu, J.F.; Liu, T.C.; Huang, M.S.; Chong, I.W. The clinical efficacy of Afatinib 30 mg daily as starting dose may not be inferior to Afatinib 40 mg daily in patients with stage IV lung Adenocarcinoma harboring exon 19 or exon 21 mutations. Bmc Pharm. Toxicol. 2017, 18, 82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.H.; Chang, J.W.; Chang, C.F.; Huang, C.Y.; Yang, C.T.; Kuo, C.S.; Fang, Y.F.; Hsu, P.C.; Wu, C.E. Real-world Afatinib Outcomes in Advanced Non-small Cell Lung Cancer Harboring EGFR Mutations. Anticancer Res. 2022, 42, 2145–2157. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.H.; Ju, J.S.; Chiu, T.H.; Huang, A.C.; Tung, P.H.; Wang, C.C.; Liu, C.Y.; Chung, F.T.; Fang, Y.F.; Guo, Y.K.; et al. Afatinib treatment in a large real-world cohort of nonsmall cell lung cancer patients with common and uncommon epidermal growth factor receptor mutation. Int. J. Cancer 2022, 150, 626–635. [Google Scholar] [CrossRef] [PubMed]
- Liang, S.K.; Hsieh, M.S.; Lee, M.R.; Keng, L.T.; Ko, J.C.; Shih, J.Y. Real-world experience of afatinib as a first-line therapy for advanced EGFR mutation-positive lung adenocarcinoma. Oncotarget 2017, 8, 90430–90443. [Google Scholar] [CrossRef] [Green Version]
- Elamin, Y.Y.; Gomez, D.R.; Antonoff, M.B.; Robichaux, J.P.; Tran, H.; Shorter, M.K.; Bohac, J.M.; Negrao, M.V.; Le, X.; Rinsurogkawong, W.; et al. Local Consolidation Therapy (LCT) After First Line Tyrosine Kinase Inhibitor (TKI) for Patients With EGFR Mutant Metastatic Non-small-cell Lung Cancer (NSCLC). Clin. Lung Cancer 2019, 20, 43–47. [Google Scholar] [CrossRef]
- Gomez, D.R.; Tang, C.; Zhang, J.; Blumenschein, G.R., Jr.; Hernandez, M.; Lee, J.J.; Ye, R.; Palma, D.A.; Louie, A.V.; Camidge, D.R.; et al. Local Consolidative Therapy Vs. Maintenance Therapy or Observation for Patients With Oligometastatic Non-Small-Cell Lung Cancer: Long-Term Results of a Multi-Institutional, Phase II, Randomized Study. J. Clin. Oncol. 2019, 37, 1558–1565. [Google Scholar] [CrossRef]
- Liu, K.; Zheng, D.; Xu, G.; Du, Z.; Wu, S. Local thoracic therapy improve prognosis for stage IV non-small cell lung cancer patients combined with chemotherapy: A Surveillance, Epidemiology, and End Results database analysis. PLoS ONE 2017, 12, e0187350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tseng, J.S.; Hsu, K.H.; Zheng, Z.R.; Yang, T.Y.; Chen, K.C.; Huang, Y.H.; Su, K.Y.; Yu, S.L.; Chang, G.C. Primary Tumor Resection Is Associated with a Better Outcome among Advanced EGFR-Mutant Lung Adenocarcinoma Patients Receiving EGFR-TKI Treatment. Oncology 2021, 99, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Verma, V.; Liang, F.; Lin, Q.; Zhou, Z.; Wang, Z.; Wang, Y.; Wang, J.; Chang, J.Y. Local Consolidative Therapy Versus Systemic Therapy Alone for Metastatic Non-Small Cell Lung Cancer: A Systematic Review and Meta-Analysis. Int. J. Radiat. Oncol. Biol. Phys. 2022. [Google Scholar] [CrossRef]
- Gomez, D.R.; Blumenschein, G.R., Jr.; Lee, J.J.; Hernandez, M.; Ye, R.; Camidge, D.R.; Doebele, R.C.; Skoulidis, F.; Gaspar, L.E.; Gibbons, D.L.; et al. Local consolidative therapy versus maintenance therapy or observation for patients with oligometastatic non-small-cell lung cancer without progression after first-line systemic therapy: A multicentre, randomised, controlled, phase 2 study. Lancet Oncol. 2016, 17, 1672–1682. [Google Scholar] [CrossRef] [Green Version]
- Iyengar, P.; Wardak, Z.; Gerber, D.E.; Tumati, V.; Ahn, C.; Hughes, R.S.; Dowell, J.E.; Cheedella, N.; Nedzi, L.; Westover, K.D.; et al. Consolidative Radiotherapy for Limited Metastatic Non-Small-Cell Lung Cancer: A Phase 2 Randomized Clinical Trial. JAMA Oncol. 2018, 4, e173501. [Google Scholar] [CrossRef] [PubMed]
- Palma, D.A.; Olson, R.; Harrow, S.; Gaede, S.; Louie, A.V.; Haasbeek, C.; Mulroy, L.; Lock, M.; Rodrigues, G.B.; Yaremko, B.P.; et al. Stereotactic Ablative Radiotherapy for the Comprehensive Treatment of Oligometastatic Cancers: Long-Term Results of the SABR-COMET Phase II Randomized Trial. J. Clin. Oncol. 2020, 38, 2830–2838. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.Y.; Yen, Y.T.; Lai, W.W.; Huang, W.L.; Chang, C.C.; Tseng, Y.L. Outcomes of salvage lung resections in advanced EGFR-mutant lung adenocarcinomas under EGFR TKIs. Thorac. Cancer 2021, 12, 2655–2665. [Google Scholar] [CrossRef]
- Kuo, S.W.; Chen, P.H.; Lu, T.P.; Chen, K.C.; Liao, H.C.; Tsou, K.C.; Tsai, T.M.; Lin, M.W.; Hsu, H.H.; Chen, J.S. Primary Tumor Resection for Stage IV Non-small-cell Lung Cancer Without Progression After First-Line Epidermal Growth Factor Receptor-Tyrosine Kinase Inhibitor Treatment: A Retrospective Case-Control Study. Ann. Surg. Oncol. 2022, 29, 4873–4884. [Google Scholar] [CrossRef]
- Galetta, D.; De Marinis, F.; Spaggiari, L. Rescue Surgery after Immunotherapy/Tyrosine Kinase Inhibitors for Initially Unresectable Lung Cancer. Cancers 2022, 14, 2661. [Google Scholar] [CrossRef]
- Yang, C.J.; Hung, J.Y.; Tsai, M.J.; Wu, K.L.; Liu, T.C.; Chou, S.H.; Lee, J.Y.; Hsu, J.S.; Huang, M.S.; Chong, I.W. The salvage therapy in lung adenocarcinoma initially harbored susceptible EGFR mutation and acquired resistance occurred to the first-line gefitinib and second-line cytotoxic chemotherapy. Bmc Pharm. Toxicol. 2017, 18, 21. [Google Scholar] [CrossRef] [Green Version]
- Yang, C.J.; Tsai, M.J.; Hung, J.Y.; Liu, T.C.; Chou, S.H.; Lee, J.Y.; Hsu, J.S.; Tsai, Y.M.; Huang, M.S.; Chong, I.W. Pemetrexed had significantly better clinical efficacy in patients with stage IV lung adenocarcinoma with susceptible EGFR mutations receiving platinum-based chemotherapy after developing resistance to the first-line gefitinib treatment. Oncotargets Ther. 2016, 9, 1579–1587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, C.J.; Tsai, M.J.; Hung, J.Y.; Tsai, Y.M.; Lee, J.Y.; Chou, S.H.; Liu, T.C.; Shen, M.C.; Huang, M.S.; Chong, I.W. Poorer prognosis in Taiwanese female ever smokers with stage IV lung adenocarcinoma who were readministered a tyrosine kinase inhibitor. Oncotargets Ther. 2016, 9, 1511–1518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, F.; Li, F. Propensity score weighting for causal inference with multiple treatments. Ann. Appl. Stat. 2019, 13, 2389–2415. [Google Scholar] [CrossRef] [Green Version]
- Chuang, C.H.; Hsu, J.F.; Shen, Y.T.; Yang, C.J. Regression of a metastatic lung mass after receiving whole brain irradiation: Can the abscopal effect cross the blood-brain barrier? Asia Pac. J. Clin. Oncol. 2018, 14, e548–e550. [Google Scholar] [CrossRef]
- Li, X.; Wang, J.; Chang, X.; Gao, Z.; Teng, F.; Meng, X.; Yu, J. Optimal Initial Time Point of Local Radiotherapy for Unresectable Lung Adenocarcinoma: A Retrospective Analysis on Overall Arrangement of Local Radiotherapy in Advanced Lung Adenocarcinoma. Front. Oncol. 2022, 12, 793190. [Google Scholar] [CrossRef]
- Lim, J.U.; Kang, H.S.; Shin, A.Y.; Yeo, C.D.; Park, C.K.; Lee, S.H.; Kim, S.J.; Korean Association for Lung Cancer, K.C.C.R. Association between clinical outcomes and local treatment in stage IV non-small cell lung cancer patients with single extrathoracic metastasis. Thorac. Cancer 2022, 13, 1349–1360. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Cao, X.; Ai, B.; Xiao, H.; Huang, Q.; Zhang, Z.; Chu, Q.; Zhang, L.; Dai, X.; Liao, Y. Salvage surgery following downstaging of advanced non-small cell lung cancer by targeted therapy. Thorac. Cancer 2021, 12, 2161–2169. [Google Scholar] [CrossRef]


| Variables | All Patients | LCT | No LCT | p-Value |
|---|---|---|---|---|
| n | 254 | 30 | 224 | |
| LCT | ||||
| No | 224 (88%) | 0 (0%) | 224 (100%) | <0.0001 |
| Radiotherapy | 15 (6%) | 15 (50%) | 0 (0%) | |
| Operation | 15 (6%) | 15 (50%) | 0 (0%) | |
| Age(year) | 64.3 ± 10.1 | 64.7 ± 9.2 | 64.3 ± 10.2 | 0.8129 |
| <65 | 128 (50%) | 12 (40%) | 116 (52%) | 0.2253 |
| ≥65 | 126 (50%) | 18 (60%) | 108 (48%) | |
| Sex | ||||
| Female | 157 (62%) | 21 (70%) | 136 (61%) | 0.3256 |
| Male | 97 (38%) | 9 (30%) | 88 (39%) | |
| Smoking | ||||
| Never | 202 (80%) | 26 (87%) | 176 (79%) | 0.3021 |
| Ever | 52 (20%) | 4 (13%) | 48 (21%) | |
| Familyhistory | ||||
| No | 237 (93%) | 27 (90%) | 210 (94%) | 0.4402 |
| Yes | 17 (7%) | 3 (10%) | 14 (6%) | |
| ECOG performance status | ||||
| 0–1 | 221 (87%) | 30 (100%) | 191 (85%) | 0.0242 |
| ≥2 | 33 (13%) | 0 (0%) | 33 (15%) | |
| EGFR mutation | ||||
| Exon 19 deletion | 135 (53%) | 19 (63%) | 116 (52%) | 0.2339 |
| Exon 21 L858R | 121 (48%) | 11 (37%) | 110 (49%) | 0.2001 |
| Stage | ||||
| IIIB–IIIC | 11 (4%) | 3 (10%) | 8 (4%) | 0.1043 |
| IV | 243 (96%) | 27 (90%) | 216 (96%) | |
| Metastatic sites | ||||
| 0–1 | 94 (37%) | 19 (63%) | 75 (33%) | 0.0015 |
| ≥2 | 160 (63%) | 11 (37%) | 149 (67%) | |
| Metastasis | ||||
| Brain metastasis | 73 (29%) | 2 (7%) | 71 (32%) | 0.0044 |
| Lung metastasis | 133 (52%) | 13 (43%) | 120 (54%) | 0.2917 |
| Pleural metastasis/effusion | 113 (44%) | 8 (27%) | 105 (47%) | 0.0365 |
| Bone metastasis | 130 (51%) | 14 (47%) | 116 (52%) | 0.5984 |
| Liver metastasis | 32 (13%) | 1 (3%) | 31 (14%) | 0.1034 |
| Adrenal metastasis | 20 (8%) | 1 (3%) | 19 (8%) | 0.3255 |
| Other metastasis | 18 (7%) | 1 (3%) | 17 (8%) | 0.3936 |
| Variables | Univariate | Multivariable Model 1 | Multivariable Model 1R | Multivariable Model 2 | Multivariable Model 2R |
|---|---|---|---|---|---|
| Local consolidative therapy (vs. no) | 0.43 [0.26-0.72] ** | 0.46 [0.27–0.76] ** | 0.45 [0.27–0.75] ** | 0.44 [0.26–0.74] ** | 0.44 [0.26–0.73] ** |
| Male (vs. female) | 1.23 [0.92–1.63] | 1.26 [0.90–1.77] | 1.29 [0.92–1.81] | ||
| Age (≥65 vs. <65) | 0.83 [0.63–1.10] | 0.85 [0.64–1.13] | 0.89 [0.67–1.19] | ||
| Smoking (ever vs. never) | 1.10 [0.78–1.55] | 1.01 [0.67–1.52] | 0.86 [0.57–1.30] | ||
| ECOG performance status (≥2 vs. ≤1) | 1.55 [1.04–2.30] * | 1.35 [0.90–2.03] | 1.39 [0.94–2.07] | 1.27 [0.84–1.93] | 1.35 [0.90–2.01] |
| L858R vs. exon 19 del | 1.04 [0.78–1.38] | 0.97 [0.73–1.30] | 1.02 [0.76–1.37] | ||
| Stage IV (vs. stage IIIB-IIIC) | 2.19 [0.81–5.90] | 2.10 [0.77–5.72] | |||
| Brain metastasis (vs. no) | 1.38 [1.02–1.87] * | 1.09 [0.79–1.50] | |||
| Lung metastasis (vs. no) | 0.91 [0.69–1.21] | 1.00 [0.75–1.33] | |||
| Pleural metastasis/effusion (vs. no) | 1.50 [1.13–1.99] ** | 1.50 [1.12–2.02] ** | 1.49 [1.12–1.99] ** | ||
| Bone metastasis (vs. no) | 1.92 [1.45–2.56] *** | 2.00 [1.46–2.74] *** | 2.03 [1.50–2.73] *** | ||
| Liver metastasis (vs. no) | 1.74 [1.18–2.56] ** | 1.43 [0.94–2.16] | 1.34 [0.90–2.01] | ||
| Adrenal metastasis (vs. no) | 1.31 [0.80–2.16] | 0.96 [0.57–1.64] | |||
| Other metastasis (vs. no) | 0.87 [0.49–1.53] | 0.81 [0.45–1.47] |
| Variables | Univariate | Multivariable Model 3 | Multivariable Model 3R | Multivariable Model 4 | Multivariable Model 4R |
|---|---|---|---|---|---|
| Local consolidative therapy (vs. no) | 0.32 [0.16–0.66] ** | 0.33 [0.16–0.70] ** | 0.35 [0.17–0.72] ** | 0.26 [0.12–0.56] ** | 0.26 [0.12–0.54] ** |
| Male (vs. female) | 1.67 [1.19–2.35] ** | 1.32 [0.88–2.00] | 1.38 [0.92–2.06] | 1.36 [0.92–2.03] | |
| Age (≥65 vs. <65) | 1.35 [0.97–1.89] | 1.39 [0.99–1.95] | 1.40 [1.00–1.96] | 1.49 [1.06–2.11] * | 1.45 [1.04–2.04] * |
| Smoking (ever vs. never) | 1.72 [1.17–2.52] ** | 1.76 [1.10–2.83] * | 2.03 [1.37–3.00] ** | 1.51 [0.96–2.37] | 1.51 [0.96–2.37] |
| ECOG performance status (≥2 vs. ≤1) | 2.69 [1.75–4.12] *** | 2.53 [1.61–3.97] *** | 2.70 [1.74–4.21] *** | 2.49 [1.56–3.99] *** | 2.62 [1.67–4.12] *** |
| L858R vs. exon 19 del | 1.16 [0.83–1.62] | 0.99 [0.70–1.40] | 0.93 [0.65–1.33] | ||
| Stage IV (vs. stage IIIB-IIIC) | 1.31 [0.49–3.55] | 1.55 [0.56–4.30] | |||
| Brain metastasis (vs. no) | 1.63 [1.14–2.33] ** | 1.21 [0.82–1.77] | |||
| Lung metastasis (vs. no) | 0.79 [0.56–1.10] | 0.91 [0.64–1.29] | |||
| Pleural metastasis/effusion (vs. no) | 1.43 [1.02–2.00] * | 1.42 [1.00–2.01] * | 1.41 [1.00–1.98] * | ||
| Bone metastasis (vs. no) | 2.21 [1.56–3.13] *** | 2.62 [1.78–3.84] *** | 2.74 [1.89–3.95] *** | ||
| Liver metastasis (vs. no) | 1.43 [0.88–2.33] | 1.23 [0.73–2.06] | |||
| Adrenal metastasis (vs. no) | 0.87 [0.46–1.66] | 0.52 [0.26–1.03] | 0.54 [0.27–1.05] | ||
| Other metastasis (vs. no) | 0.98 [0.48–2.02] | 1.16 [0.55–2.46] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, M.-J.; Hung, J.-Y.; Ma, J.-Y.; Tsai, Y.-C.; Wu, K.-L.; Lee, M.-H.; Kuo, C.-Y.; Chuang, C.-H.; Lee, T.-H.; Lee, Y.-L.; et al. Local Consolidative Therapy May Have Prominent Clinical Efficacy in Patients with EGFR-Mutant Advanced Lung Adenocarcinoma Treated with First-Line Afatinib. Cancers 2023, 15, 2019. https://doi.org/10.3390/cancers15072019
Tsai M-J, Hung J-Y, Ma J-Y, Tsai Y-C, Wu K-L, Lee M-H, Kuo C-Y, Chuang C-H, Lee T-H, Lee Y-L, et al. Local Consolidative Therapy May Have Prominent Clinical Efficacy in Patients with EGFR-Mutant Advanced Lung Adenocarcinoma Treated with First-Line Afatinib. Cancers. 2023; 15(7):2019. https://doi.org/10.3390/cancers15072019
Chicago/Turabian StyleTsai, Ming-Ju, Jen-Yu Hung, Juei-Yang Ma, Yu-Chen Tsai, Kuan-Li Wu, Mei-Hsuan Lee, Chia-Yu Kuo, Cheng-Hao Chuang, Tai-Huang Lee, Yen-Lung Lee, and et al. 2023. "Local Consolidative Therapy May Have Prominent Clinical Efficacy in Patients with EGFR-Mutant Advanced Lung Adenocarcinoma Treated with First-Line Afatinib" Cancers 15, no. 7: 2019. https://doi.org/10.3390/cancers15072019