

Primary Total Prostate Cryoablation for Localized High-Risk Prostate Cancer: 10-Year Outcomes and Nomograms

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Clinical Information Collection
2.3. Statistical Consideration
3. Results
3.1. Patient Demographics and Tumor Characteristics
3.2. Univariable and Multivariable Analyses Predicting BCR
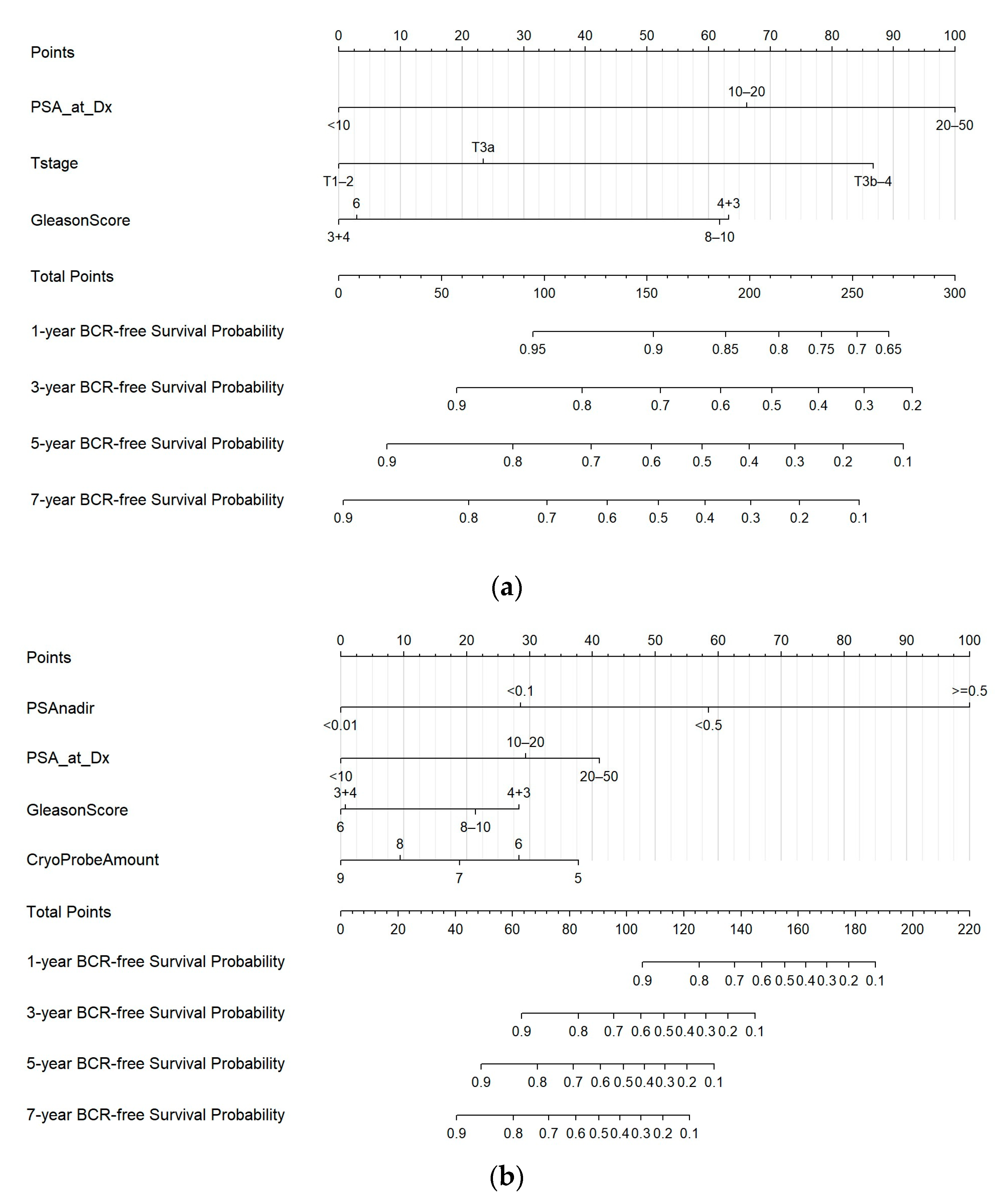
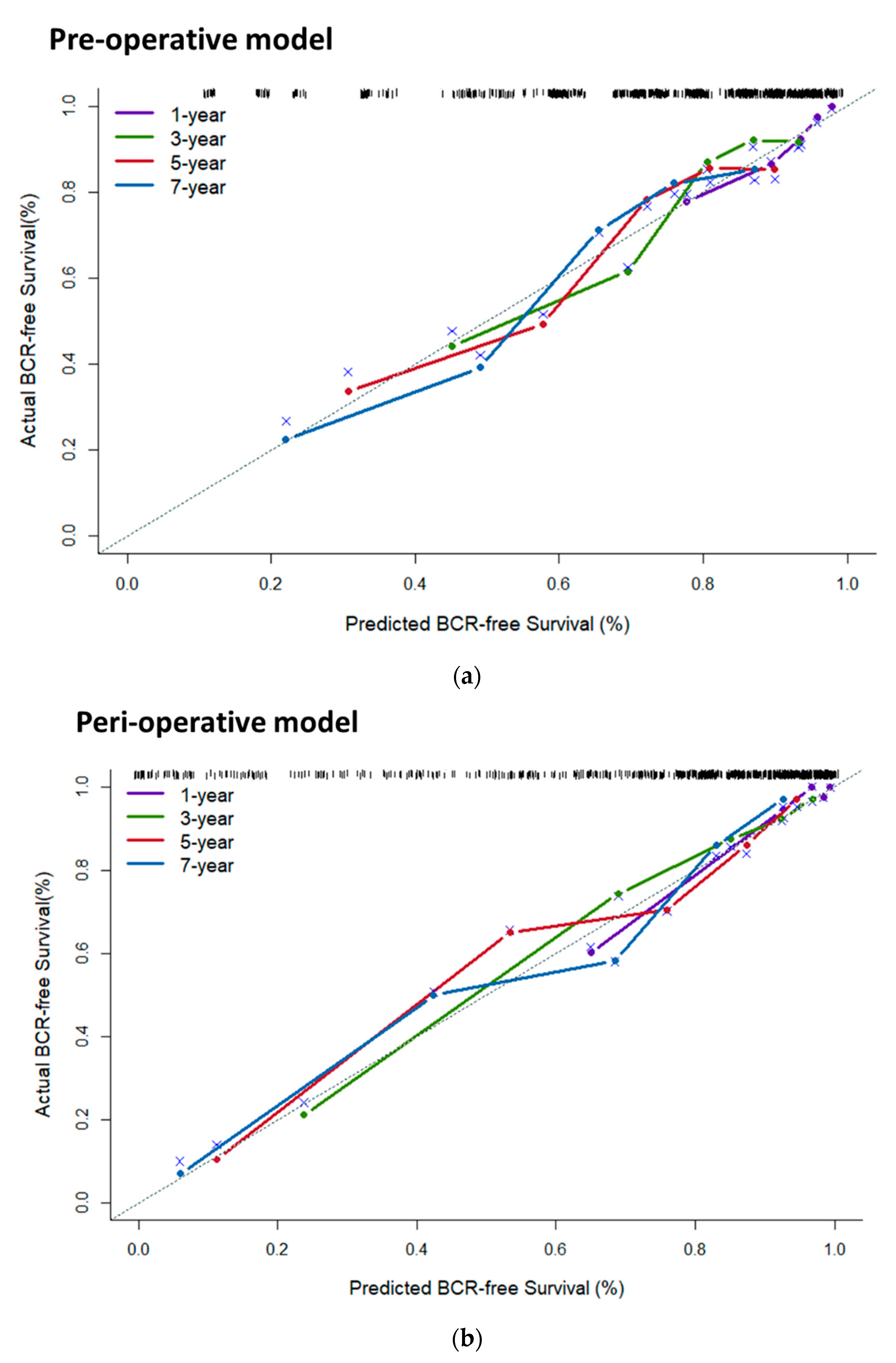
3.3. Predictive Nomograms and Calibration
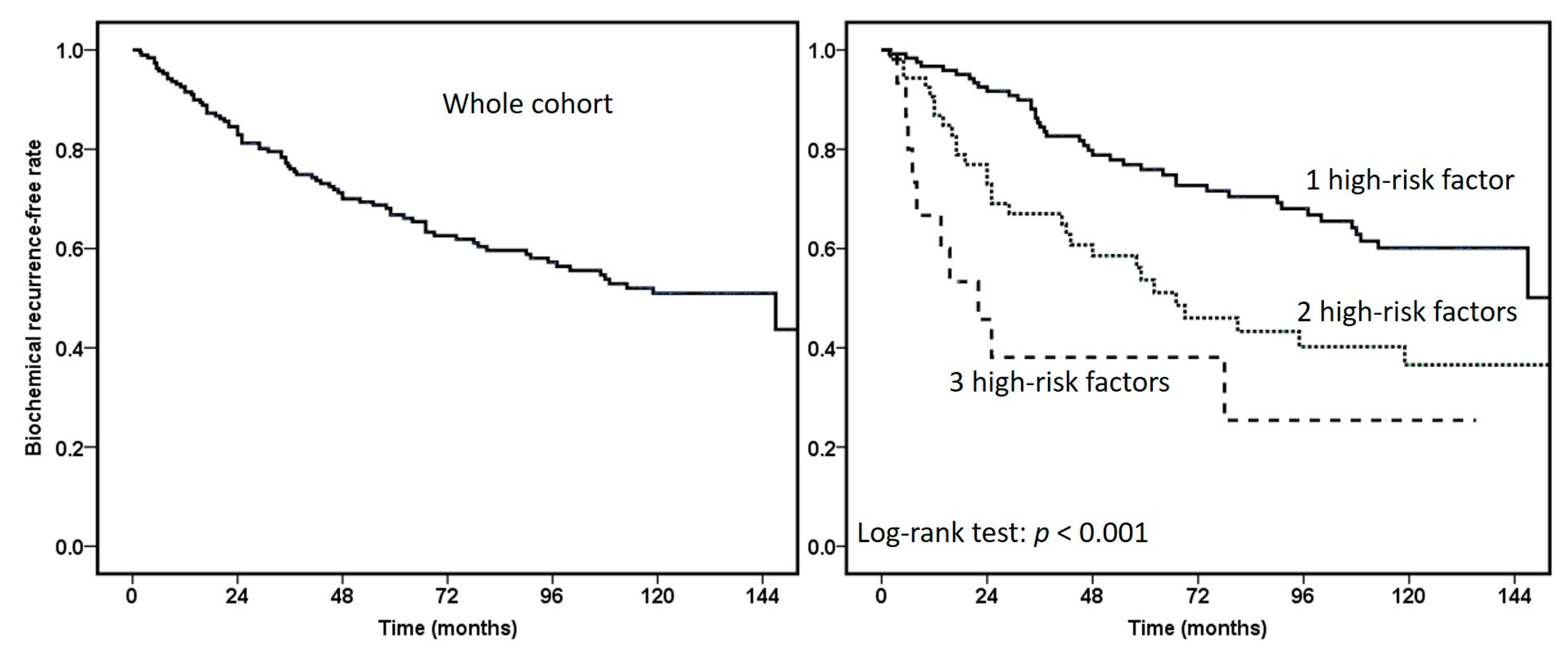
3.4. Pathological and Radiographic Evidence of Recurrence
3.5. Complications
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PC | prostate cancer |
| BCR | biochemical recurrence |
| COLD | Cryo On-Line Database |
| PSA | prostate-specific antigen |
| ADT | androgen deprivation therapy |
| PET | positron emission tomography |
| PTPC | primary total prostate cryoablation |
| MRI | magnetic resonance imaging |
References
- National Comprehensive Cancer Network. Prostate Cancer (Version 2.2022). Available online: https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf (accessed on 1 April 2022).
- EAU. EAU Guidelines. Edn. Presented at the EAU Annual Congress Milan 2023; EAU Guidelines Office: Arnhem, The Netherlands, 2023. [Google Scholar]
- Jones, J.S.; Rewcastle, J.C.; Donnelly, B.J.; Lugnani, F.M.; Pisters, L.L.; Katz, A.E. Whole gland primary prostate cryoablation: Initial results from the cryo on-line data registry. J. Urol. 2008, 180, 554–558. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.H.; Tai, Y.S.; Pu, Y.S. Prognostic value of saturated prostate cryoablation for localized prostate cancer. World J. Urol. 2015, 33, 1487–1494. [Google Scholar] [CrossRef] [PubMed]
- Thompson, I.; Thrasher, J.B.; Aus, G.; Burnett, A.L.; Canby-Hagino, E.D.; Cookson, M.S.; D’Amico, A.V.; Dmochowski, R.R.; Eton, D.T.; Forman, J.D.; et al. Guideline for the management of clinically localized prostate cancer: 2007 update. J. Urol. 2007, 177, 2106–2131. [Google Scholar] [CrossRef] [PubMed]
- Paladini, A.; Cochetti, G.; Colau, A.; Mouton, M.; Ciarletti, S.; Felici, G.; Maiolino, G.; Balzarini, F.; Sebe, P.; Mearini, E. The Challenges of Patient Selection for Prostate Cancer Focal Therapy: A Retrospective Observational Multicentre Study. Curr. Oncol. 2022, 29, 6826–6833. [Google Scholar] [CrossRef]
- Kotamarti, S.; Polascik, T.J. Focal cryotherapy for prostate cancer: A contemporary literature review. Ann. Transl. Med. 2023, 11, 26. [Google Scholar] [CrossRef]
- Aizer, A.A.; Yu, J.B.; Colberg, J.W.; McKeon, A.M.; Decker, R.H.; Peschel, R.E. Radical prostatectomy vs. intensity-modulated radiation therapy in the management of localized prostate adenocarcinoma. Radiother. Oncol. 2009, 93, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Ciezki, J.P.; Weller, M.; Reddy, C.A.; Kittel, J.; Singh, H.; Tendulkar, R.; Stephans, K.L.; Ulchaker, J.; Angermeier, K.; Stephenson, A.; et al. A Comparison Between Low-Dose-Rate Brachytherapy With or Without Androgen Deprivation, External Beam Radiation Therapy With or Without Androgen Deprivation, and Radical Prostatectomy With or Without Adjuvant or Salvage Radiation Therapy for High-Risk Prostate Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2017, 97, 962–975. [Google Scholar] [CrossRef]
- Chen, C.H.; Pu, Y.S. Adjuvant androgen-deprivation therapy following prostate total cryoablation in high-risk localized prostate cancer patients—Open-labeled randomized clinical trial. Cryobiology 2018, 82, 88–92. [Google Scholar] [CrossRef]
- Chen, C.H.; Pu, Y.S. Proactive rectal warming during total-gland prostate cryoablation. Cryobiology 2014, 68, 431–435. [Google Scholar] [CrossRef] [PubMed]
- Roach, M., 3rd; Hanks, G.; Thames, H., Jr.; Schellhammer, P.; Shipley, W.U.; Sokol, G.H.; Sandler, H. Defining biochemical failure following radiotherapy with or without hormonal therapy in men with clinically localized prostate cancer: Recommendations of the RTOG-ASTRO Phoenix Consensus Conference. Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 965–974. [Google Scholar] [CrossRef]
- Van den Broeck, T.; van den Bergh, R.C.N.; Briers, E.; Cornford, P.; Cumberbatch, M.; Tilki, D.; De Santis, M.; Fanti, S.; Fossati, N.; Gillessen, S.; et al. Biochemical Recurrence in Prostate Cancer: The European Association of Urology Prostate Cancer Guidelines Panel Recommendations. Eur. Urol. Focus 2020, 6, 231–234. [Google Scholar] [CrossRef] [PubMed]
- Harrell, F.E., Jr.; Lee, K.L.; Mark, D.B. Multivariable prognostic models: Issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Stat. Med. 1996, 15, 361–387. [Google Scholar] [CrossRef]
- Harrell, F.E., Jr. Rms: Regression Modeling Strategies. R Package Version 6.2-0. Available online: https://cran.r-project.org/web/packages/rms/rms.pdf (accessed on 15 April 2021).
- Harrell, F.E., Jr.; Califf, R.M.; Pryor, D.B.; Lee, K.L.; Rosati, R.A. Evaluating the yield of medical tests. JAMA 1982, 247, 2543–2546. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.H.; Chen, Y.C.; Pu, Y.S. Tumor location on MRI determines outcomes of patients with prostate cancer after total prostate cryoablation. Cryobiology 2021, 98, 39–45. [Google Scholar] [CrossRef]
- Sanda, M.G.; Cadeddu, J.A.; Kirkby, E.; Chen, R.C.; Crispino, T.; Fontanarosa, J.; Freedland, S.J.; Greene, K.; Klotz, L.H.; Makarov, D.V.; et al. Clinically Localized Prostate Cancer: AUA/ASTRO/SUO Guideline. Part I: Risk Stratification, Shared Decision Making, and Care Options. J. Urol. 2018, 199, 683–690. [Google Scholar] [CrossRef]
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer-2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2021, 79, 243–262. [Google Scholar] [CrossRef]
- Pilepich, M.V.; Winter, K.; Lawton, C.A.; Krisch, R.E.; Wolkov, H.B.; Movsas, B.; Hug, E.B.; Asbell, S.O.; Grignon, D. Androgen suppression adjuvant to definitive radiotherapy in prostate carcinoma--long-term results of phase III RTOG 85-31. Int. J. Radiat. Oncol. Biol. Phys. 2005, 61, 1285–1290. [Google Scholar] [CrossRef]
- Bolla, M.; Van Tienhoven, G.; Warde, P.; Dubois, J.B.; Mirimanoff, R.O.; Storme, G.; Bernier, J.; Kuten, A.; Sternberg, C.; Billiet, I.; et al. External irradiation with or without long-term androgen suppression for prostate cancer with high metastatic risk: 10-Year results of an EORTC randomised study. Lancet Oncol. 2010, 11, 1066–1073. [Google Scholar] [CrossRef]
- Tay, K.J.; Polascik, T.J.; Elshafei, A.; Cher, M.L.; Given, R.W.; Mouraviev, V.; Ross, A.E.; Jones, J.S. Primary Cryotherapy for High-Grade Clinically Localized Prostate Cancer: Oncologic and Functional Outcomes from the COLD Registry. J. Endourol. 2016, 30, 43–48. [Google Scholar] [CrossRef]
- Mercader, C.; Musquera, M.; Franco, A.; Alcaraz, A.; Ribal, M.J. Primary cryotherapy for localized prostate cancer treatment. Aging Male 2020, 23, 1460–1466. [Google Scholar] [CrossRef]
- de Vermandois, J.A.R.; Cochetti, G.; Zingaro, M.D.; Santoro, A.; Panciarola, M.; Boni, A.; Marsico, M.; Gaudio, G.; Paladini, A.; Guiggi, P.; et al. Evaluation of Surgical Site Infection in Mini-invasive Urological Surgery. Open Med. 2019, 14, 711–718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ataman, F.; Zurlo, A.; Artignan, X.; van Tienhoven, G.; Blank, L.E.; Warde, P.; Dubois, J.B.; Jeanneret, W.; Keuppens, F.; Bernier, J.; et al. Late toxicity following conventional radiotherapy for prostate cancer: Analysis of the EORTC trial 22863. Eur. J. Cancer 2004, 40, 1674–1681. [Google Scholar] [CrossRef]
- Ficarra, V.; Novara, G.; Rosen, R.C.; Artibani, W.; Carroll, P.R.; Costello, A.; Menon, M.; Montorsi, F.; Patel, V.R.; Stolzenburg, J.U.; et al. Systematic review and meta-analysis of studies reporting urinary continence recovery after robot-assisted radical prostatectomy. Eur. Urol. 2012, 62, 405–417. [Google Scholar] [CrossRef] [PubMed]
- Broggi, G.; Lo Giudice, A.; Di Mauro, M.; Asmundo, M.G.; Pricoco, E.; Piombino, E.; Caltabiano, R.; Morgia, G.; Russo, G.I. SRSF-1 and microvessel density immunohistochemical analysis by semi-automated tissue microarray in prostate cancer patients with diabetes (DIAMOND study). Prostate 2021, 81, 882–892. [Google Scholar] [CrossRef] [PubMed]
- Heni, M.; Hennenlotter, J.; Scharpf, M.; Lutz, S.Z.; Schwentner, C.; Todenhofer, T.; Schilling, D.; Kuhs, U.; Gerber, V.; Machicao, F.; et al. Insulin receptor isoforms A and B as well as insulin receptor substrates-1 and -2 are differentially expressed in prostate cancer. PLoS ONE 2012, 7, e50953. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Groups | All | No BCR | BCR | p Value | |||
|---|---|---|---|---|---|---|---|
| Patient number (n) | 191 | 100.00% | 111 | 58.1% | 80 | 41.90% | |
| Median age (years, range) | 71 (48–88) | 72 (52–88) | 69 (48–87) | 0.014 | |||
| Median PSA at diagnosis (ng/mL, range) | 12.3 (2.0–45.9) | 10.0 (2.0–45.9) | 15.4 (4.5–44) | <0.001 | |||
| PSA at diagnosis (ng/mL) | 0.003 | ||||||
| <10 | 77 | 40.31% | 56 | 50.45% | 21 | 26.25% | |
| 10~20 | 64 | 33.51% | 33 | 29.73% | 31 | 38.75% | |
| >20 | 50 | 26.18% | 22 | 19.82% | 28 | 35.00% | |
| Biopsy Gleason sum | 0.004 | ||||||
| ≤6 | 35 | 18.32% | 26 | 23.42% | 9 | 11.25% | |
| 3 + 4 = 7 | 61 | 31.94% | 42 | 37.84% | 19 | 23.75% | |
| 4 + 3 = 7 | 43 | 22.51% | 21 | 18.92% | 22 | 27.50% | |
| 8~10 | 52 | 27.23% | 22 | 19.82% | 30 | 37.50% | |
| Clinical T stage | 0.006 | ||||||
| T1c | 8 | 4.19% | 5 | 4.50% | 3 | 3.75% | |
| T2a-2c | 41 | 21.47% | 29 | 26.13% | 12 | 15.00% | |
| T3a | 80 | 41.88% | 52 | 46.85% | 28 | 35.00% | |
| T3b | 62 | 32.46% | 25 | 22.52% | 37 | 46.25% | |
| Visible lesions on MRI | 0.084 | ||||||
| No | 32 | 16.75% | 23 | 20.72% | 9 | 11.25% | |
| Yes | 159 | 83.25% | 88 | 79.28% | 71 | 88.75% | |
| Anterior apical tumor | 0.449 | ||||||
| No | 162 | 84.82% | 96 | 86.49% | 66 | 82.50% | |
| Yes | 29 | 15.18% | 15 | 13.51% | 14 | 17.50% | |
| Neoadjuvant hormonal therapy | 0.153 | ||||||
| No | 88 | 46.07% | 56 | 50.45% | 32 | 40.00% | |
| Yes | 103 | 53.93% | 55 | 49.55% | 48 | 60.00% | |
| Adjuvant hormonal therapy | 0.437 | ||||||
| No | 171 | 89.53% | 101 | 90.99% | 70 | 87.50% | |
| Yes | 20 | 10.47% | 10 | 9.01% | 10 | 12.50% | |
| Prostate volume (median in mL, range) | 26.9 (11.9–81.9) | 26.9 (11.9–81.9) | 26.8 (12.6–64.0) | 0.689 | |||
| Cryoprobe number (median, range) | 6 (5–9) | 6 (5–8) | 6 (5–9) | 0.351 | |||
| PSA nadir value (ng/mL) | <0.001 | ||||||
| <0.01 | 87 | 45.55% | 66 | 59.46% | 21 | 26.25% | |
| 0.01~<0.1 | 66 | 34.55% | 35 | 31.53% | 31 | 38.75% | |
| 0.1~<0.5 | 27 | 14.14% | 9 | 8.11% | 18 | 22.50% | |
| 0.5~ | 11 | 5.76% | 1 | 0.90% | 10 | 12.50% | |
| Time to PSA nadir (weeks) | 0.084 | ||||||
| <8 | 71 | 37.17% | 34 | 28.57% | 37 | 51.39% | |
| 8~<12 | 76 | 39.79% | 48 | 40.34% | 28 | 38.89% | |
| 12~ | 44 | 23.04% | 29 | 24.37% | 15 | 20.83% | |
| Univariable Analysis | Multivariable Analysis | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Case No. | Failure Events | Preoperative Model | Peri-Operative Model | ||||||||
| Variables | HR | Range | p Value | HR | Range | p Value | HR | Range | p Value | ||
| Pre-operative | |||||||||||
| Age (year) | 191 | 80 | 0.98 | 0.95–1.01 | 0.145 | ▬ | ▬ | ▬ | ▬ | ▬ | ▬ |
| PSA at diagnosis (ng/mL) | 0.001 * | <0.001 * | |||||||||
| <10 | 77 | 21 | 1 | ▬ | ▬ | 1 | ▬ | ▬ | 1 | ▬ | ▬ |
| 10~<20 | 64 | 31 | 2.01 | 1.15–3.50 | 0.014 | 1.93 | 1.10–3.38 | 0.022 | 2.48 | 1.38–4.46 | 0.002 |
| 20~<50 | 50 | 28 | 3.15 | 1.78–5.57 | <0.001 | 2.75 | 1.54–4.91 | 0.001 | 3.68 | 1.91–7.09 | <0.001 |
| Biopsy Gleason sum | 0.001 * | 0.001 | |||||||||
| ~6 | 35 | 9 | 1 | ▬ | ▬ | 1 | ▬ | ▬ | 1 | ▬ | ▬ |
| 3 + 4 = 7 | 61 | 19 | 1.1 | 0.50–2.43 | 0.817 | 1.11 | 0.50–2.46 | 0.804 | 1.03 | 0.45–2.34 | 0.941 |
| 4 + 3 = 7 | 43 | 22 | 2.26 | 1.04–4.92 | 0.039 | 2.3 | 1.05–5.02 | 0.037 | 2.90 | 1.31–6.37 | 0.009 |
| 8~10 | 52 | 30 | 3.01 | 1.49–6.64 | 0.003 | 2.4 | 1.12–5.13 | 0.024 | 2.44 | 1.13–5.24 | 0.023 |
| Clinical T stage | 0.007 | ||||||||||
| T1c-2c | 49 | 15 | 1 | ▬ | ▬ | 1 | ▬ | ▬ | ▬ | ▬ | ▬ |
| T3a | 80 | 28 | 1.07 | 0.57–2.00 | 0.833 | 1.08 | 0.57–2.04 | 0.809 | ▬ | ▬ | ▬ |
| T3b | 62 | 37 | 2.62 | 1.43–4.78 | 0.002 | 2.18 | 1.18–4.00 | 0.012 | ▬ | ▬ | ▬ |
| Visible lesions on MRI | |||||||||||
| Yes | 159 | 71 | 1 | ▬ | ▬ | ▬ | ▬ | ▬ | ▬ | ▬ | ▬ |
| No | 32 | 9 | 0.52 | 0.56–1.04 | 0.063 | ▬ | ▬ | ▬ | ▬ | ▬ | ▬ |
| Anterior apical tumor | |||||||||||
| No | 162 | 66 | 1 | ▬ | ▬ | ▬ | ▬ | ▬ | ▬ | ▬ | ▬ |
| Yes | 29 | 14 | 1.31 | 0.74–2.33 | 0.361 | ▬ | ▬ | ▬ | ▬ | ▬ | ▬ |
| Neoadjuvant hormonal therapy | |||||||||||
| No | 88 | 32 | 1 | ▬ | ▬ | ▬ | ▬ | ▬ | ▬ | ▬ | ▬ |
| Yes | 103 | 48 | 1.42 | 0.91–2.22 | 0.126 | ▬ | ▬ | ▬ | ▬ | ▬ | ▬ |
| Prostate volume (mL) | 191 | 80 | 1 | 0.98–1.02 | 0.908 | ▬ | ▬ | ▬ | ▬ | ▬ | ▬ |
| Post-operative | |||||||||||
| Cryoprobe number | 191 | 80 | 0.87 | 0.70–1.10 | 0.239 | 0.69 | 0.53–0.92 | 0.002 | |||
| Adjuvant hormonal therapy | |||||||||||
| No | 171 | 70 | 1 | ▬ | ▬ | ▬ | ▬ | ▬ | ▬ | ▬ | ▬ |
| Yes | 20 | 10 | 1.1 | 0.57–2.14 | 0.778 | ▬ | ▬ | ▬ | ▬ | ▬ | ▬ |
| PSA nadir value (ng/mL) | <0.001 * | ||||||||||
| <0.01 | 87 | 21 | 1 | ▬ | ▬ | 1 | ▬ | ▬ | |||
| 0.01~<0.1 | 66 | 31 | 2.37 | 1.36–4.14 | 0.002 | 2.98 | 1.68–5.26 | <0.001 | |||
| 0.1~<0.5 | 27 | 18 | 6.56 | 3.46–12.5 | <0.001 | 6.32 | 3.26–12.3 | <0.001 | |||
| 0.5~ | 11 | 10 | 28.44 | 12.7–63.6 | <0.001 | 37.98 | 15.5–93.1 | <0.001 | |||
| Time to PSA nadir (weeks) | |||||||||||
| <8 | 71 | 37 | 1 | ▬ | ▬ | ▬ | ▬ | ▬ | |||
| 8~<12 | 77 | 28 | 0.52 | 0.32–0.85 | 0.009 | ▬ | ▬ | ▬ | |||
| 12~ | 43 | 15 | 0.48 | 0.27–0.89 | 0.019 | ▬ | ▬ | ▬ | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.-H.; Tsai, C.-Y.; Pu, Y.-S. Primary Total Prostate Cryoablation for Localized High-Risk Prostate Cancer: 10-Year Outcomes and Nomograms. Cancers 2023, 15, 3873. https://doi.org/10.3390/cancers15153873
Chen C-H, Tsai C-Y, Pu Y-S. Primary Total Prostate Cryoablation for Localized High-Risk Prostate Cancer: 10-Year Outcomes and Nomograms. Cancers. 2023; 15(15):3873. https://doi.org/10.3390/cancers15153873
Chicago/Turabian StyleChen, Chung-Hsin, Chung-You Tsai, and Yeong-Shiau Pu. 2023. "Primary Total Prostate Cryoablation for Localized High-Risk Prostate Cancer: 10-Year Outcomes and Nomograms" Cancers 15, no. 15: 3873. https://doi.org/10.3390/cancers15153873