
Radiotherapy Is Associated with an Accelerated Risk of Carotid Atherosclerosis in Patients with Nasopharyngeal Carcinoma: A Nine-Year Prospective Follow-Up Study

 ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Selection
2.2. Diagnostic Criteria and Therapeutic Regimens
2.3. Clinical Assessment
2.4. Assessment of Atherosclerosis
2.5. Biochemical Analysis
2.6. Biomarkers for Oxidative Stress and Anti-Oxidative Capacity
2.7. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Study Patients
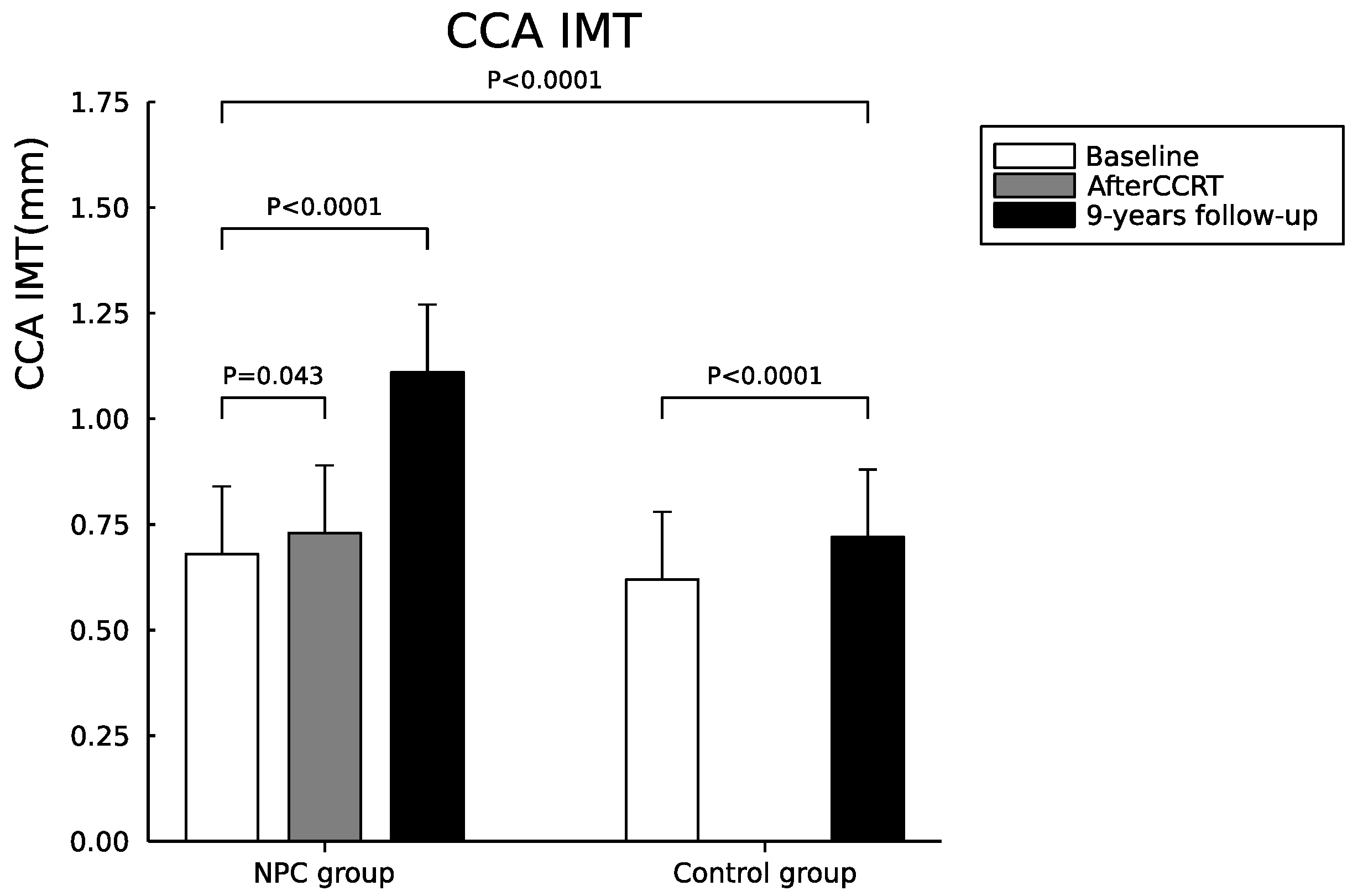
3.2. Serial Changes of Carotid IMT and Plaques between NPC and Control Groups
3.3. Assessment of the Relationship between the Radiation Dose and the CCA IMT Change
3.4. Serial Changes of Biochemical Data, Oxidative Stress, and Platelet Activation Markers between NPC and Control Groups
4. Discussion
4.1. Major Findings of Our Study
4.2. Prevalence and Locations of Radiation-Related Vasculopathy
4.3. The Role of Inflammation, Oxidative Stress and Platelet Activation in Patients with NPC
4.4. Risk of Cerebrovascular Events
4.5. Management of Radiation-Related Extracranial Vasculopathy
4.6. Study Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chang, E.T.; Adami, H.-O. The enigmatic epidemiology of nasopharyngeal carcinoma. Cancer Epidemiol. Prev. Biomark. 2006, 15, 1765–1777. [Google Scholar] [CrossRef] [Green Version]
- Grégoire, V.; Lefebvre, J.-L.; Licitra, L.; Felip, E.; EHNS–ESMO–ESTRO Guidelines Working Group. Squamous cell carcinoma of the head and neck: EHNS–ESMO–ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2010, 21, v184–v186. [Google Scholar] [CrossRef]
- Chen, M.C.; Kuan, F.C.; Huang, S.F.; Lu, C.H.; Chen, P.T.; Huang, C.E.; Wang, T.Y.; Chen, C.C.; Lee, K.D. Accelerated Risk of Premature Ischemic Stroke in 5-Year Survivors of Nasopharyngeal Carcinoma. Oncologist 2019, 24, e891–e897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robbins, M.; Zhao, W. Chronic oxidative stress and radiation-induced late normal tissue injury: A review. Int. J. Radiat. Biol. 2004, 80, 251–259. [Google Scholar] [CrossRef]
- Nakashima, Y.; Raines, E.W.; Plump, A.S.; Breslow, J.L.; Ross, R. Upregulation of VCAM-1 and ICAM-1 at atherosclerosis-prone sites on the endothelium in the ApoE-deficient mouse. Arterioscler. Thromb. Vasc. Biol. 1998, 18, 842–851. [Google Scholar] [CrossRef] [Green Version]
- Okada, Y.; Copeland, B.R.; Mori, E.; Tung, M.M.; Thomas, W.S.; del Zoppo, G.J. P-selectin and intercellular adhesion molecule-1 expression after focal brain ischemia and reperfusion. Stroke A J. Cereb. Circ. 1994, 25, 202–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.C.; Rosenbloom, C.L.; Anderson, D.C.; Manning, A.M. Selective inhibition of E-selectin, vascular cell adhesion molecule-1, and intercellular adhesion molecule-1 expression by inhibitors of I kappa B-alpha phosphorylation. J. Immunol. 1995, 155, 3538–3545. [Google Scholar] [PubMed]
- Minoguchi, K.; Yokoe, T.; Tazaki, T.; Minoguchi, H.; Tanaka, A.; Oda, N.; Okada, S.; Ohta, S.; Naito, H.; Adachi, M. Increased carotid intima-media thickness and serum inflammatory markers in obstructive sleep apnea. Am. J. Respir. Crit. Care Med. 2005, 172, 625–630. [Google Scholar] [CrossRef] [PubMed]
- Ciccone, M.M.; Scicchitano, P.; Zito, A.; Cortese, F.; Boninfante, B.; Falcone, V.A.; Quaranta, V.N.; Ventura, V.A.; Zucano, A.; Di Serio, F.; et al. Correlation between inflammatory markers of atherosclerosis and carotid intima-media thickness in Obstructive Sleep Apnea. Molecules 2014, 19, 1651–1662. [Google Scholar] [CrossRef] [PubMed]
- Crossen, J.R.; Garwood, D.; Glatstein, E.; Neuwelt, E.A. Neurobehavioral sequelae of cranial irradiation in adults: A review of radiation-induced encephalopathy. J. Clin. Oncol. 1994, 12, 627–642. [Google Scholar] [CrossRef]
- Pourcelot, L.; Tranquart, F.; De, J.B.; Philippot, M.; Bonithon, M.; Salez, F. Ultrasound characterization and quantification of carotid atherosclerosis lesions. Minerva Cardioangiol. 1999, 47, 15–24. [Google Scholar] [PubMed]
- Plummer, C.; Henderson, R.D.; O’Sullivan, J.D.; Read, S.J. Ischemic stroke and transient ischemic attack after head and neck radiotherapy: A review. Stroke A J. Cereb. Circ. 2011, 42, 2410–2418. [Google Scholar] [CrossRef] [Green Version]
- Elerding, S.C.; Fernandez, R.N.; Grotta, J.C.; Lindberg, R.D.; Causay, L.C.; McMurtrey, M.J. Carotid artery disease following external cervical irradiation. Ann. Surg. 1981, 194, 609–615. [Google Scholar] [CrossRef] [PubMed]
- Dorresteijn, L.D.; Kappelle, A.C.; Boogerd, W.; Klokman, W.J.; Balm, A.J.; Keus, R.B.; van Leeuwen, F.E.; Bartelink, H. Increased risk of ischemic stroke after radiotherapy on the neck in patients younger than 60 years. J. Clin. Oncol. 2002, 20, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.L.; Hsu, H.C.; Chen, H.C.; Lin, H.C.; Chien, C.Y.; Fang, F.M.; Huang, C.C.; Chang, H.W.; Chang, W.N.; Huang, C.R. Long-term effects on carotid intima-media thickness after radiotherapy in patients with nasopharyngeal carcinoma. Radiat. Oncol. 2013, 8, 261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- So, N.M.; Lam, W.W.; Chook, P.; Woo, K.S.; Liu, K.H.; Leung, S.F.; Wong, K.S.; Metreweli, C. Carotid intima-media thickness in patients with head and neck irradiation for the treatment of nasopharyngeal carcinoma. Clin. Radiol. 2002, 57, 600–603. [Google Scholar] [CrossRef] [PubMed]
- Ye, J.; Rong, X.; Xiang, Y.; Xing, Y.; Tang, Y. A study of radiation-induced cerebral vascular injury in nasopharyngeal carcinoma patients with radiation-induced temporal lobe necrosis. PLoS ONE 2012, 7, e42890. [Google Scholar] [CrossRef] [Green Version]
- Fokkema, M.; den Hartog, A.G.; Bots, M.L.; van der Tweel, I.; Moll, F.L.; de Borst, G.J. Stenting versus surgery in patients with carotid stenosis after previous cervical radiation therapy: Systematic review and meta-analysis. Stroke A J. Cereb. Circ. 2012, 43, 793–801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Leary, D.H.; Polak, J.F.; Kronmal, R.A.; Manolio, T.A.; Burke, G.L.; Wolfson, S.K., Jr. Carotid-artery intima and media thickness as a risk factor for myocardial infarction and stroke in older adults. Cardiovascular Health Study Collaborative Research Group. N. Engl. J. Med. 1999, 340, 14–22. [Google Scholar] [CrossRef]
- O’Leary, D.H.; Polak, J.F. Intima-media thickness: A tool for atherosclerosis imaging and event prediction. Am. J. Cardiol. 2002, 90, 18L–21L. [Google Scholar] [CrossRef]
- Touboul, P.J.; Hennerici, M.G.; Meairs, S.; Adams, H.; Amarenco, P.; Bornstein, N.; Csiba, L.; Desvarieux, M.; Ebrahim, S.; Hernandez Hernandez, R.; et al. Mannheim carotid intima-media thickness and plaque consensus (2004-2006-2011). An update on behalf of the advisory board of the 3rd, 4th and 5th watching the risk symposia, at the 13th, 15th and 20th European Stroke Conferences, Mannheim, Germany, 2004, Brussels, Belgium, 2006, and Hamburg, Germany, 2011. Cereb. Dis. 2012, 34, 290–296. [Google Scholar] [CrossRef] [Green Version]
- Lu, C.-H.; Lin, H.-C.; Huang, C.-C.; Lin, W.-C.; Chen, H.-L.; Chang, H.-W.; Friedman, M.; Chen, C.T.; Tsai, N.-W.; Wang, H.-C. Increased circulating endothelial progenitor cells and anti-oxidant capacity in obstructive sleep apnea after surgical treatment. Clin. Chim. Acta 2015, 448, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, G.; Rothe, G.; Ruf, A.; Barlage, S.; Tschope, D.; Clemetson, K.J.; Goodall, A.H.; Michelson, A.D.; Nurden, A.T.; Shankey, T.V. European Working Group on Clinical Cell Analysis: Consensus protocol for the flow cytometric characterisation of platelet function. Thromb Haemost 1998, 79, 885–896. [Google Scholar] [CrossRef]
- Liao, W.; Zhou, H.; Fan, S.; Zheng, Y.; Zhang, B.; Zhao, Z.; Xiao, S.; Bai, S.; Liu, J. Comparison of significant carotid stenosis for nasopharyngeal carcinoma between intensity-modulated radiotherapy and conventional two-dimensional radiotherapy. Sci. Rep. 2018, 8, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Lam, W.W.m.; Yuen, H.y.; Wong, K.s.; Leung, S.f.; Liu, K.h.; Metreweli, C. Clinically underdetected asymptomatic and symptomatic carotid stenosis as a late complication of radiotherapy in Chinese nasopharyngeal carcinoma patients. Head Neck J. Sci. Spec. Head Neck 2001, 23, 780–784. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Xing, P.; Chen, Y.; Xu, X.; Shen, J.; Lu, X. Carotid and vertebral artery stenosis evaluated by contrast-enhanced MR angiography in nasopharyngeal carcinoma patients after radiotherapy: A prospective cohort study. Br. J. Radiol. 2015, 88, 20150175. [Google Scholar] [CrossRef] [Green Version]
- Eisenberg, R.L.; Hedgcock, M.W.; Wara, W.M.; Jeffrey, R.B. Radiation-induced disease of the carotid artery. West. J. Med. 1978, 129, 500–503. [Google Scholar]
- Lam, W.W.; Leung, S.F.; So, N.M.; Wong, K.S.; Liu, K.H.; Ku, P.K.; Yuen, H.Y.; Metreweli, C. Incidence of carotid stenosis in nasopharyngeal carcinoma patients after radiotherapy. Cancer 2001, 92, 2357–2363. [Google Scholar] [CrossRef]
- Lam, W.W.; Liu, K.H.; Leung, S.F.; Wong, K.S.; So, N.M.; Yuen, H.Y.; Metreweli, C. Sonographic characterisation of radiation-induced carotid artery stenosis. Cereb. Dis. 2002, 13, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Murros, K.E.; Toole, J.F. The effect of radiation on carotid arteries: A review article. Arch. Neurol. 1989, 46, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Huang, M.P.; Fang, H.Y.; Chen, C.Y.; Tan, T.Y.; Kuo, Y.L.; Hsieh, I.C.; Yip, H.K.; Wu, C.J. Long-term outcomes of carotid artery stenting for radiation-associated stenosis. Biomed. J. 2013, 36, 144–149. [Google Scholar] [PubMed]
- Crohns, M.; Liippo, K.; Erhola, M.; Kankaanranta, H.; Moilanen, E.; Alho, H.; Kellokumpu-Lehtinen, P. Concurrent decline of several antioxidants and markers of oxidative stress during combination chemotherapy for small cell lung cancer. Clin. Biochem. 2009, 42, 1236–1245. [Google Scholar] [CrossRef] [PubMed]
- Perillo, B.; Di Donato, M.; Pezone, A.; Di Zazzo, E.; Giovannelli, P.; Galasso, G.; Castoria, G.; Migliaccio, A. ROS in cancer therapy: The bright side of the moon. Exp. Mol. Med. 2020, 52, 192–203. [Google Scholar] [CrossRef] [PubMed]
- Shrivastava, A.; Mishra, S.P.; Pradhan, S.; Choudhary, S.; Singla, S.; Zahra, K.; Aggarwal, L.M. An assessment of serum oxidative stress and antioxidant parameters in patients undergoing treatment for cervical cancer. Free Radic. Biol. Med. 2021, 167, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Greten, F.R.; Grivennikov, S.I. Inflammation and Cancer: Triggers, Mechanisms, and Consequences. Immunity 2019, 51, 27–41. [Google Scholar] [CrossRef] [PubMed]
- Tsai, N.W.; Chang, W.N.; Shaw, C.F.; Jan, C.R.; Chang, H.W.; Huang, C.R.; Chen, S.D.; Chuang, Y.C.; Lee, L.H.; Wang, H.C.; et al. Levels and value of platelet activation markers in different subtypes of acute non-cardio-embolic ischemic stroke. Thromb Res. 2009, 124, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Cha, J.K.; Jeong, M.H.; Jang, J.Y.; Bae, H.R.; Lim, Y.J.; Kim, J.S.; Kim, S.H.; Kim, J.W. Serial measurement of surface expressions of CD63, P-selectin and CD40 ligand on platelets in atherosclerotic ischemic stroke. A possible role of CD40 ligand on platelets in atherosclerotic ischemic stroke. Cereb. Dis. 2003, 16, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Marquardt, L.; Ruf, A.; Mansmann, U.; Winter, R.; Schuler, M.; Buggle, F.; Mayer, H.; Grau, A.J. Course of platelet activation markers after ischemic stroke. Stroke A J. Cereb. Circ. 2002, 33, 2570–2574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, G.L.; Smith, B.D.; Buchholz, T.A.; Giordano, S.H.; Garden, A.S.; Woodward, W.A.; Krumholz, H.M.; Weber, R.S.; Ang, K.-K.; Rosenthal, D.I. Cerebrovascular disease risk in older head and neck cancer patients after radiotherapy. J. Clin. Oncol. 2008, 26, 5119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kernan, W.N.; Ovbiagele, B.; Black, H.R.; Bravata, D.M.; Chimowitz, M.I.; Ezekowitz, M.D.; Fang, M.C.; Fisher, M.; Furie, K.L.; Heck, D.V. Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke A J. Cereb. Circ. 2014, 45, 2160–2236. [Google Scholar] [CrossRef] [PubMed]
- Law, M.R.; Wald, N.J. Environmental tobacco smoke and ischemic heart disease. Prog. Cardiovasc. Dis. 2003, 46, 31–38. [Google Scholar] [CrossRef]
- Poredos, P.; Orehek, M.; Tratnik, E. Smoking is associated with dose-related increase of intima-media thickness and endothelial dysfunction. Angiology 1999, 50, 201–208. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| NPC Patients (n = 36) | Controls (n = 36) | p Value | |
|---|---|---|---|
| Age (years) at enrollment | 55.4 ± 12.3 | 55.3 ± 14.1 | 0.97 |
| Gender (female/male) | 12/24 | 12/24 | 1.0 |
| Body mass index, kg/m2 | 24.8 ± 3.3 | 24.5 ± 2.8 | 0.2 |
| Height (m) | 1.63 ± 0.07 | 1.63 ± 0.09 | 0.82 |
| Body weight (Kg) | 66.2 ± 11.1 | 64.6 ± 11.3 | 0.57 |
| Mean duration between the date of the complete course of radiotherapy and the last follow-up (months) | 105.1 ± 7.0 | - | |
| Systolic blood pressure | 126.9 ± s12.4 | 122.2 ± 17.9 | 0.2 |
| Diastolic blood pressure | 77.1 ± 8.0 | 70.0 ± 9.3 | 0.001 |
| Smoking (%) | 18 | 2 | 0.001 * |
| Staging system of AJCC for NPC | |||
| Stage 1 | 2 | -- | |
| Stage 2 | 8 | -- | |
| Stage 3 | 11 | -- | |
| Stage 4 | 15 | -- |
| Baseline (before and after CCRT) | Nine-Years Follow-Up | ||||
|---|---|---|---|---|---|
| Controls (n = 36) | NPC Patients (n = 36) | Controls γ,Φ (n = 36) | NPC Patients δ (n = 23) α | ||
| Before CCRT | After CCRT β | ||||
| Carotid IMT and plaque score α | |||||
| Right CCA IMT, mm | 0.69 ± 0.20 | 0.65 ± 0.17 | 0.71 ± 0.23 ‡ | 0.81 ± 0.27 #,‖ | 1.05 ± 0.26 ¶ |
| Left CCA IMT, mm | 0.75 ± 0.27 | 0.71 ± 0.21 | 0.74 ± 0.22 ‡ | 0.86 ± 0.27 #,‖ | 1.18 ± 0.27 ¶ |
| Mean CCA IMT, mm | 0.72 ± 0.22 | 0.68 ± 0.16 | 0.73 ± 0.21 ‡ | 0.83 ± 0.25 #,‖ | 1.11 ± 0.23 ¶ |
| Carotid Plaque (%) | 2 (5.5%) | 5 (13.8%) | 5 (13.8%) | 5 (13.8%) | 11 (47.8%) |
| Annual increase mean CCA IMT, mm | - | -- | -- | 0.014 ± 0.013 | 0.053 ± 0.025 § |
| Baseline (before and after CCRT) | Nine-Years Follow-Up | ||||
|---|---|---|---|---|---|
| Controls β (n = 36) | NPC Patients (n = 36) | Controls ζ,Φ (n = 36) | NPC Patients δ (n = 23) α | ||
| Before CCRT | After CCRT γ | ||||
| Biochemical data | |||||
| Cholesterol, mg/dL | |||||
| Total | 184.7 ± 31.5 | 189.3 ± 39.6 | 202.7 ± 32.7 | 180.7 ± 35.3 | 167.4 ± 41.3 |
| HDL-C | 67.9 ± 13.7 * | 51.6 ± 14.2 | 57.5 ± 14.0 | 53.6 ± 11.8 § | 47.3 ± 16.4 |
| LDL-C | 98.9 ± 30.6 | 108.9 ± 29.8 | 121.5 ± 28.8 | 98.5 ± 18.0 | 93.5 ± 34.6 |
| Triglyceride, mg/dL | 89.7 ± 45.9 * | 137.8 ± 70.0 | 120.3 ± 50.0 | 100.4 ± 45.3 | 118.9 ± 42.8 |
| Glucose, mg/dL | 89.7 ± 10.2 * | 117.3 ± 75.6 | 103.0 ± 34.3 | 105.3 ± 17.5 § | 118.9 ± 32.8 |
| HBA1c | 5.6 ± 0.3 * | 6.2 ± 1.2 | 5.7 ± 0.6 # | 5.9 ± 0.7 | 6.3 ± 0.8 |
| hs-CRP, mg/L | 1.1 ± 0.9 * | 4.2 ± 2.5 | 3.0 ± 2.6 | 0.9 ± 0.5 * | 3.9 ± 3.3 |
| WBC counts (×103/mL) | 6.0 ± 1.4 | 6.3 ± 2.0 | 4.1 ± 1.3 # | 6.3 ± 1.9 | 7.0 ± 2.9 |
| RBC counts (×106/mL) | 5.0 ± 0.7 * | 4.6 ± 0.7 | 3.9 ± 0.6 # | 4.5 ± 0.7 | 4.5 ± 0.7 |
| Platelet counts (×103/mL) | 217.6 ± 60.3 | 223.0 ± 67.1 | 221.3 ± 70.8 # | 248.5 ± 131.9 | 235.9 ± 60.4 |
| Biomarkers for oxidative stress | |||||
| TBARS, μmol/L | 12.9 ± 2.4 * | 15.9 ± 8.5 | 13.0 ± 5.3 # | - | 16.2 ± 7.9 |
| Thiols, μmol/L | 1.1 ± 0.2 * | 1.4 ± 0.4 | 1.2 ± 0.3 # | - | 1.1 ± 0.5 ¶ |
| Platelet activation markers | |||||
| CD40 (%) | 0.4 ± 0.2 | 0.5 ± 0.3 | 0.6 ± 0.3 | - | 0.5 ± 0.3 |
| CD63 (%) | 1.7 ± 1.1 * | 2.3 ± 1.1 | 2.1 ± 1.1 | - | 3.5 ± 2.3 |
| CD62P (%) | 1.0 ± 0.7 | 1.5 ± 1.1 | 0.9 ± 0.6 | - | 5.8 ± 4.9 ¶ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, C.-H.; Lai, Y.-R.; Fang, F.-M.; Tan, T.-Y.; Chiu, W.-C.; Hsieh, D.-Y.; Huang, C.-C.; Lien, C.-Y.; Cheng, B.-C.; Chien, C.-Y.; et al. Radiotherapy Is Associated with an Accelerated Risk of Carotid Atherosclerosis in Patients with Nasopharyngeal Carcinoma: A Nine-Year Prospective Follow-Up Study. Cancers 2022, 14, 1234. https://doi.org/10.3390/cancers14051234
Lu C-H, Lai Y-R, Fang F-M, Tan T-Y, Chiu W-C, Hsieh D-Y, Huang C-C, Lien C-Y, Cheng B-C, Chien C-Y, et al. Radiotherapy Is Associated with an Accelerated Risk of Carotid Atherosclerosis in Patients with Nasopharyngeal Carcinoma: A Nine-Year Prospective Follow-Up Study. Cancers. 2022; 14(5):1234. https://doi.org/10.3390/cancers14051234
Chicago/Turabian StyleLu, Cheng-Hsien, Yun-Ru Lai, Fu-Min Fang, Teng-Yeow Tan, Wen-Chan Chiu, Dong-Yi Hsieh, Chih-Cheng Huang, Chia-Yi Lien, Ben-Chung Cheng, Chih-Yen Chien, and et al. 2022. "Radiotherapy Is Associated with an Accelerated Risk of Carotid Atherosclerosis in Patients with Nasopharyngeal Carcinoma: A Nine-Year Prospective Follow-Up Study" Cancers 14, no. 5: 1234. https://doi.org/10.3390/cancers14051234