
Phase II Trial of CDX-3379 and Cetuximab in Recurrent/Metastatic, HPV-Negative, Cetuximab-Resistant Head and Neck Cancer

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Study Design
2.3. Treatment Plan
2.4. Biomarker Analyses
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Protocol Treatment
3.2.1. CDX-3379 Exposure
3.2.2. Cetuximab Exposure
3.3. Safety
3.4. Efficacy
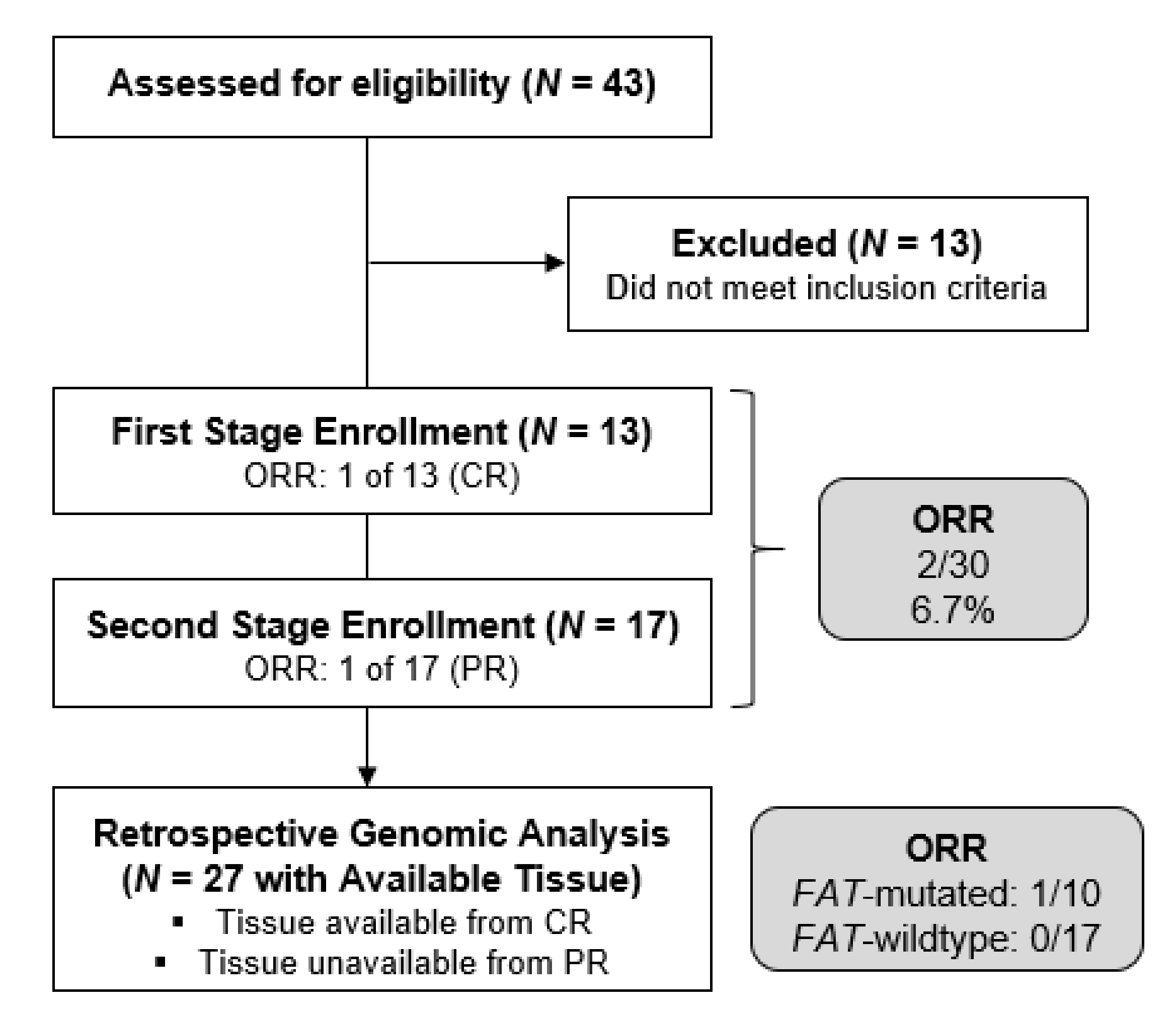
3.4.1. ORR, Genomic All-Comers (N = 30)
3.4.2. ORR, FAT1 Mutation-Positive Cohort (N = 10)
3.4.3. Secondary Efficacy Endpoints
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Sacco, A.G.; Cohen, E.E. Current Treatment Options for Recurrent or Metastatic Head and Neck Squamous Cell Carcinoma. J. Clin. Oncol. 2015, 33, 3305–3313. [Google Scholar] [CrossRef] [PubMed]
- Grandis, J.R.; Melhem, M.F.; Gooding, W.E.; Day, R.; Holst, V.A.; Wagener, M.M.; Drenning, S.D.; Tweardy, D.J. Levels of TGF-alpha and EGFR protein in head and neck squamous cell carcinoma and patient survival. J. Natl. Cancer Inst. 1998, 90, 824–832. [Google Scholar] [CrossRef] [Green Version]
- Ang, K.K.; Berkey, B.A.; Tu, X.; Zhang, H.Z.; Katz, R.; Hammond, E.H.; Fu, K.K.; Milas, L. Impact of epidermal growth factor receptor expression on survival and pattern of relapse in patients with advanced head and neck carcinoma. Cancer Res. 2002, 62, 7350–7356. [Google Scholar]
- Bonner, J.A.; Harari, P.M.; Giralt, J.; Azarnia, N.; Shin, D.M.; Cohen, R.B.; Jones, C.U.; Sur, R.; Raben, D.; Jassem, J.; et al. Radiotherapy plus cetuximab for squamous-cell carcinoma of the head and neck. N. Engl. J. Med. 2006, 354, 567–578. [Google Scholar] [CrossRef] [Green Version]
- Vermorken, J.B.; Mesia, R.; Rivera, F.; Remenar, E.; Kawecki, A.; Rottey, S.; Erfan, J.; Zabolotnyy, D.; Kienzer, H.R.; Cupissol, D.; et al. Platinum-based chemotherapy plus cetuximab in head and neck cancer. N. Engl. J. Med. 2008, 359, 1116–1127. [Google Scholar] [CrossRef] [Green Version]
- Vermorken, J.B.; Trigo, J.; Hitt, R.; Koralewski, P.; Diaz-Rubio, E.; Rolland, F.; Knecht, R.; Amellal, N.; Schueler, A.; Baselga, J. Open-label, uncontrolled, multicenter phase II study to evaluate the efficacy and toxicity of cetuximab as a single agent in patients with recurrent and/or metastatic squamous cell carcinoma of the head and neck who failed to respond to platinum-based therapy. J. Clin. Oncol. 2007, 25, 2171–2177. [Google Scholar] [CrossRef]
- Burtness, B.; Harrington, K.J.; Greil, R.; Soulieres, D.; Tahara, M.; de Castro, G., Jr.; Psyrri, A.; Baste, N.; Neupane, P.; Bratland, A.; et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): A randomised, open-label, phase 3 study. Lancet 2019, 394, 1915–1928. [Google Scholar] [CrossRef]
- Burtness, B.; Bauman, J.E.; Galloway, T. Novel targets in HPV-negative head and neck cancer: Overcoming resistance to EGFR inhibition. Lancet Oncol. 2013, 14, e302–e309. [Google Scholar] [CrossRef]
- Alvarado, D.; Ligon, G.F.; Lillquist, J.S.; Seibel, S.B.; Wallweber, G.; Neumeister, V.M.; Rimm, D.L.; McMahon, G.; LaVallee, T.M. ErbB activation signatures as potential biomarkers for anti-ErbB3 treatment in HNSCC. PLoS ONE 2017, 12, e0181356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baro, M.; Lopez Sambrooks, C.; Burtness, B.A.; Lemmon, M.A.; Contessa, J.N. Neuregulin Signaling Is a Mechanism of Therapeutic Resistance in Head and Neck Squamous Cell Carcinoma. Mol. Cancer Ther. 2019, 18, 2124–2134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, D.; Qian, G.; Zhang, H.; Magliocca, K.R.; Nannapaneni, S.; Amin, A.R.; Rossi, M.; Patel, M.; El-Deiry, M.; Wadsworth, J.T.; et al. HER3 Targeting Sensitizes HNSCC to Cetuximab by Reducing HER3 Activity and HER2/HER3 Dimerization: Evidence from Cell Line and Patient-Derived Xenograft Models. Clin. Cancer Res. 2017, 23, 677–686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, N.; Wang, D.; Hu, Z.; Shin, H.J.; Qian, G.; Rahman, M.A.; Zhang, H.; Amin, A.R.; Nannapaneni, S.; Wang, X.; et al. Combination of anti-HER3 antibody MM-121/SAR256212 and cetuximab inhibits tumor growth in preclinical models of head and neck squamous cell carcinoma. Mol. Cancer Ther. 2014, 13, 1826–1836. [Google Scholar] [CrossRef] [Green Version]
- Civenni, G.; Holbro, T.; Hynes, N.E. Wnt1 and Wnt5a induce cyclin D1 expression through ErbB1 transactivation in HC11 mammary epithelial cells. EMBO Rep. 2003, 4, 166–171. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Goto, Y.; Allevato, M.M.; Wu, V.H.; Saddawi-Konefka, R.; Gilardi, M.; Alvarado, D.; Yung, B.S.; O’Farrell, A.; Molinolo, A.A.; et al. Disruption of the HER3-PI3K-mTOR oncogenic signaling axis and PD-1 blockade as a multimodal precision immunotherapy in head and neck cancer. Nat. Commun. 2021, 12, 2383. [Google Scholar] [CrossRef]
- Li, Z.; Razavi, P.; Li, Q.; Toy, W.; Liu, B.; Ping, C.; Hsieh, W.; Sanchez-Vega, F.; Brown, D.N.; Da Cruz Paula, A.F.; et al. Loss of the FAT1 Tumor Suppressor Promotes Resistance to CDK4/6 Inhibitors via the Hippo Pathway. Cancer Cell 2018, 34, 893–905.e898. [Google Scholar] [CrossRef] [Green Version]
- Chen, Z.; Zhang, C.; Chen, J.; Wang, D.; Tu, J.; Van Waes, C.; Saba, N.F.; Chen, Z.G.; Chen, Z. The Proteomic Landscape of Growth Factor Signaling Networks Associated with FAT1 Mutations in Head and Neck Cancers. Cancer Res. 2021, 81, 4402–4416. [Google Scholar] [CrossRef]
- Duvvuri, U.; George, J.; Kim, S.; Alvarado, D.; Neumeister, V.M.; Chenna, A.; Gedrich, R.; Hawthorne, T.; LaVallee, T.; Grandis, J.R.; et al. Molecular and Clinical Activity of CDX-3379, an Anti-ErbB3 Monoclonal Antibody, in Head and Neck Squamous Cell Carcinoma Patients. Clin. Cancer Res. 2019, 25, 5752–5758. [Google Scholar] [CrossRef] [Green Version]
- Faden, D.L.; Gomez-Casal, R.; Alvarado, D.; Duvvuri, U. Genomic Correlates of Exceptional Response to ErbB3 Inhibition in Head and Neck Squamous Cell Carcinoma. JCO Precis. Oncol. 2019, 3, 1–5. [Google Scholar] [CrossRef]
- Falchook, G.S.; Bauer, T.M.; LoRusso, P.; McLaughlin, J.F.; LaVallee, T.; Peck, R.A.; Eder, J.P. Safety, pharmacokinetics, pharmacodynamics, and antitumor activity in a phase 1b study evaluating anti-ErbB3 antibody KTN3379 in adults with advanced tumors alone and with targeted therapies. J. Clin. Oncol. 2016, 34, 2501. [Google Scholar] [CrossRef]
- Schwartz, L.H.; Litiere, S.; de Vries, E.; Ford, R.; Gwyther, S.; Mandrekar, S.; Shankar, L.; Bogaerts, J.; Chen, A.; Dancey, J.; et al. RECIST 1.1-Update and clarification: From the RECIST committee. Eur. J. Cancer 2016, 62, 132–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauman, J.E.; Saba, N.F.; Wise-Draper, T.; Adkins, D.; O’Brien, P.; Heath-Chiozzi, M.; Alvarado, D.; Drescher, J.; Gedrich, R.; Golden, P.; et al. CDX3379-04: Phase 2 evaluation of CDX-3379 in combination with cetuximab in patients with advanced treatment-refractory head and neck squamous cell carcinoma. J Clin. Oncol. 2019, 37, 6025. [Google Scholar] [CrossRef]
- Lin, S.C.; Lin, L.H.; Yu, S.Y.; Kao, S.Y.; Chang, K.W.; Cheng, H.W.; Liu, C.J. FAT1 somatic mutations in head and neck carcinoma are associated with tumor progression and survival. Carcinogenesis 2018, 39, 1320–1330. [Google Scholar] [CrossRef]
- Cancer Genome Atlas, N. Comprehensive genomic characterization of head and neck squamous cell carcinomas. Nature 2015, 517, 576–582. [Google Scholar] [CrossRef] [Green Version]
- Fayette, J.; Wirth, L.; Oprean, C.; Udrea, A.; Jimeno, A.; Rischin, D.; Nutting, C.; Harari, P.M.; Csoszi, T.; Cernea, D.; et al. Randomized Phase II Study of Duligotuzumab (MEHD7945A) vs. Cetuximab in Squamous Cell Carcinoma of the Head and Neck (MEHGAN Study). Front. Oncol. 2016, 6, 232. [Google Scholar] [CrossRef] [Green Version]
- Saba, N.F. Commentary: Randomized Phase II Study of Duligotuzumab (MEHD7945A) vs. Cetuximab in Squamous Cell Carcinoma of the Head and Neck (MEHGAN Study). Front. Oncol. 2017, 7, 31. [Google Scholar] [CrossRef] [Green Version]
- Muraro, E.; Fanetti, G.; Lupato, V.; Giacomarra, V.; Steffan, A.; Gobitti, C.; Vaccher, E.; Franchin, G. Cetuximab in locally advanced head and neck squamous cell carcinoma: Biological mechanisms involved in efficacy, toxicity and resistance. Crit. Rev. Oncol. Hematol. 2021, 164, 103424. [Google Scholar] [CrossRef]
- Kansy, B.A.; Shayan, G.; Jie, H.B.; Gibson, S.P.; Lei, Y.L.; Brandau, S.; Lang, S.; Schmitt, N.C.; Ding, F.; Lin, Y.; et al. T cell receptor richness in peripheral blood increases after cetuximab therapy and correlates with therapeutic response. Oncoimmunology 2018, 7, e1494112. [Google Scholar] [CrossRef] [Green Version]
- Jie, H.B.; Srivastava, R.M.; Argiris, A.; Bauman, J.E.; Kane, L.P.; Ferris, R.L. Increased PD-1(+) and TIM-3(+) TILs during Cetuximab Therapy Inversely Correlate with Response in Head and Neck Cancer Patients. Cancer Immunol. Res. 2017, 5, 408–416. [Google Scholar] [CrossRef] [Green Version]
- Trivedi, S.; Srivastava, R.M.; Concha-Benavente, F.; Ferrone, S.; Garcia-Bates, T.M.; Li, J.; Ferris, R.L. Anti-EGFR Targeted Monoclonal Antibody Isotype Influences Antitumor Cellular Immunity in Head and Neck Cancer Patients. Clin. Cancer Res. 2016, 22, 5229–5237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, L.G.; Kaufman, A.M.; Gong, Y.; Ramaswami, D.; Walsh, L.A.; Turcan, S.; Eng, S.; Kannan, K.; Zou, Y.; Peng, L.; et al. Recurrent somatic mutation of FAT1 in multiple human cancers leads to aberrant Wnt activation. Nat. Genet. 2013, 45, 253–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drilon, A.; Somwar, R.; Mangatt, B.P.; Edgren, H.; Desmeules, P.; Ruusulehto, A.; Smith, R.S.; Delasos, L.; Vojnic, M.; Plodkowski, A.J.; et al. Response to ERBB3-Directed Targeted Therapy in NRG1-Rearranged Cancers. Cancer Discov. 2018, 8, 686–695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azharuddin, M.; Roberg, K.; Dhara, A.K.; Jain, M.V.; Darcy, P.; Hinkula, J.; Slater, N.K.H.; Patra, H.K. Dissecting multi drug resistance in head and neck cancer cells using multicellular tumor spheroids. Sci. Rep. 2019, 9, 20066. [Google Scholar] [CrossRef] [PubMed]
- Kanno, Y.; Chen, C.Y.; Lee, H.L.; Chiou, J.F.; Chen, Y.J. Molecular Mechanisms of Chemotherapy Resistance in Head and Neck Cancers. Front. Oncol. 2021, 11, 640392. [Google Scholar] [CrossRef] [PubMed]
- Kogawa, T.; Yonemori, K.; Masuda, N.; Takahashi, S.; Takahashi, M.; Iwase, H.; Nakayama, T.; Saeki, T.; Toyama, T.; Takano, T.; et al. Single agent activity of U3-1402, a HER3-targeting antibody-drug conjugate, in breast cancer patients: Phase 1 dose escalation study. J. Clin. Oncol. 2018, 36 (Suppl. S 15), 2512. [Google Scholar] [CrossRef]
- Janne, P.A.; Yu, H.A.; Johnson, M.L.; Steuer, C.E.; Vigliotti, M.; Iacobucci, C.; Chen, S.; Yu, C.; Sellami, D.B. Safety and preliminary antitumor activity of U3-1402: A HER3-targeted antibody drug conjugate in EGFR TKI-resistant, EGFRm NSCLC. J. Clin. Oncol. 2019, 37 (Suppl. S15), 9010. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | N = 30 |
|---|---|
| Age, years | |
| Mean (SD) | 62.0 (8.5) |
| Range (min, max) | 46, 79 |
| Sex, N (%) | |
| Male | 26 (87) |
| Female | 4 (13) |
| Race, N (%) | |
| White | 25 (83) |
| Black or African American | 3 (10) |
| Asian | 1 (3) |
| Other | 1 (3) |
| Ethnicity, N (%) | |
| Not Hispanic or Latino | 26 (87) |
| Hispanic or Latino | 4 (13) |
| Primary Tumor Site, N (%) | |
| Oral cavity | 11 (37) |
| Oropharynx (HPV-negative) | 8 (27) |
| Larynx | 4 (13) |
| Hypopharynx | 3 (10) |
| Nasopharynx (EBV-negative) | 1 (3) |
| Other | 3 (10) |
| ECOG Performance Status, N (%) | |
| 0 | 4 (13) |
| 1 | 26 (87) |
| Smoking status, N (%) | |
| Former | 16 (53) |
| Current | 7 (23) |
| Never | 7 (23) |
| Subjects with any prior radiotherapy, N (%) | 26 (87) |
| Subjects with any prior surgery, N (%) | 30 (100) |
| Number of prior systemic therapy regimens in the recurrent/metastatic setting, N (%) | |
| 1 | 0 |
| 2 | 1 (3) |
| 3 | 4 (13) |
| 4 | 6 (20) |
| ≥5 | 17 (57) |
| Unknown | 2 (17) |
| Prior systemic therapy, N (%) | |
| Cetuximab | 29 (97) |
| Pembrolizumab | 22 (73) |
| Carboplatin | 21 (70) |
| Cisplatin | 18 (60) |
| MedDRA System Organ Class/ High Level Term/ Preferred Term | N = 30 | |||||
|---|---|---|---|---|---|---|
| Grade 1 | Grade 2 | Grade 3 | Grade 4 | Grade 5 | Total | |
| N (%) | N (%) | N (%) | N (%) | N (%) | N (%) | |
| Any AE related to CDX-3379 | 3 (10) | 7 (23) | 16 (53) | 1 (3) | 0 | 27 (90) |
| Gastrointestinal disorders | 10 (33) | 9 (30) | 7 (23) | 0 | 0 | 26 (87) |
| Diarrhea | 12 (40) | 7 (23) | 6 (20) | 0 | 0 | 25 (83) |
| Nausea and vomiting symptoms | 5 (17) | 1 (3) | 0 | 0 | 0 | 6 (20) |
| Stomatitis | 2 (7) | 1 (3) | 1 (3) | 0 | 0 | 4 (13) |
| Oral dryness and saliva altered | 2 (7) | 0 | 0 | 0 | 0 | 2 (7) |
| Abdominal pain | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| Duodenal ulcer | 0 | 0 | 1 (3) | 0 | 0 | 1 (3) |
| Flatulence | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| Gastrointestinal disorder | 0 | 1 (3) | 0 | 0 | 0 | 1 (3) |
| Small intestinal hemorrhage | 0 | 0 | 1 (3) | 0 | 0 | 1 (3) |
| Metabolism and nutrition disorders | 3 (10) | 4 (13) | 6 (20) | 1 (3) | 0 | 14 (47) |
| Hypomagnesemia | 2 (7) | 3 (10) | 3 (10) | 1 (3) | 0 | 9 (30) |
| Hypokalemia | 4 (13) | 0 | 3 (10) | 0 | 0 | 7 (23) |
| Decreased appetite | 0 | 1 (3) | 1 (3) | 0 | 0 | 2 (7) |
| Dehydration | 0 | 2 (7) | 0 | 0 | 0 | 2 (7) |
| Hypophosphatemia | 0 | 2 (7) | 0 | 0 | 0 | 2 (7) |
| Hypoalbuminemia | 0 | 1 (3) | 0 | 0 | 0 | 1 (3) |
| Hypocalcemia | 0 | 1 (3) | 0 | 0 | 0 | 1 (3) |
| Skin and subcutaneous tissue disorders | 2 (7) | 4 (13) | 7 (23) | 0 | 0 | 13 (43) |
| Dermal and epidermal conditions NEC | 4 (13) | 1 (3) | 1 (3) | 0 | 0 | 6 (20) |
| Dermatitis acneiform | 0 | 0 | 6 (20) | 0 | 0 | 6 (20) |
| Rashes, eruptions and exanthems NEC | 3 (10) | 2 (7) | 1 (3) | 0 | 0 | 6 (20) |
| Pruritus | 0 | 2 (7) | 0 | 0 | 0 | 2 (7) |
| Alopecia | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| Onychoclasis | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| Palmar-plantar erythrodysesthesia syndrome | 0 | 1 (3) | 0 | 0 | 0 | 1 (3) |
| General disorders and administration site conditions | 2 (7) | 6 (20) | 2 (7) | 0 | 0 | 10 (33) |
| Asthenic conditions | 2 (7) | 5 (17) | 0 | 0 | 0 | 7 (23) |
| Mucosal inflammation | 0 | 0 | 2 (7) | 0 | 0 | 2 (7) |
| Chills | 0 | 1 (3) | 0 | 0 | 0 | 1 (3) |
| Pain | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| Investigations | 3 (10) | 3 (10) | 2 (7) | 0 | 0 | 8 (27) |
| Electrocardiogram QT prolonged | 1 (3) | 1 (3) | 1 (3) | 0 | 0 | 3 (10) |
| Weight decreased | 2 (7) | 1 (3) | 0 | 0 | 0 | 3 (10) |
| Digestive enzymes | 0 | 2 (7) | 0 | 0 | 0 | 2 (7) |
| Alanine aminotransferase increased | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| Blood creatinine increased | 0 | 1 (3) | 0 | 0 | 0 | 1 (3) |
| Lymphocyte count decreased | 0 | 0 | 1 (3) | 0 | 0 | 1 (3) |
| Eye disorders | 2 (7) | 1 (3) | 0 | 0 | 0 | 3 (10) |
| Conjunctival hyperemia | 0 | 1 (3) | 0 | 0 | 0 | 1 (3) |
| Eye pruritus | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| Ocular discomfort | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| Vision blurred | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| Nervous system disorders | 2 (7) | 0 | 1 (3) | 0 | 0 | 3 (10) |
| Dysgeusia | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| Encephalopathy | 0 | 0 | 1 (3) | 0 | 0 | 1 (3) |
| Headache | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| Peripheral sensory neuropathy | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| Injury | 1 (3) | 1 (3) | 0 | 0 | 0 | 2 (7) |
| Radiation skin injury | 0 | 1 (3) | 0 | 0 | 0 | 1 (3) |
| Skin laceration | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| Infections and infestations | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| Fungal skin infection | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| Renal and urinary disorders | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| Proteinuria | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| Reproductive system and breast disorders | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| Perineal rash | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| Any AE related to cetuximab | 5 (17) | 8 (27) | 13 (43) | 2 (7) | 0 | 28 (93) |
| Skin and subcutaneous tissue disorders | 7 (23) | 7 (23) | 9 (30) | 0 | 0 | 23 (77) |
| Dermatitis acneiform | 5 (17) | 3 (10) | 8 (27) | 0 | 0 | 16 (53) |
| Dermal and epidermal conditions NEC | 6 (20) | 1 (3) | 1 (3) | 0 | 0 | 8 (27) |
| Rashes, eruptions and exanthems NEC | 3 (10) | 2 (7) | 1 (3) | 0 | 0 | 6 (20) |
| Pruritus | 1 (3) | 2 (7) | 0 | 0 | 0 | 3 (10) |
| Palmar-plantar erythrodysesthesia syndrome | 2 (7) | 0 | 0 | 0 | 0 | 2 (7) |
| Urticaria | 2 (7) | 0 | 0 | 0 | 0 | 2 (7) |
| Dermal cyst | 0 | 1 (3) | 0 | 0 | 0 | 1 (3) |
| Erythema | 0 | 1 (3) | 0 | 0 | 0 | 1 (3) |
| Onychoclasis | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| Metabolism and nutrition disorders | 3 (10) | 3 (10) | 9 (30) | 2 (7) | 0 | 17 (57) |
| Magnesium metabolism disorders | 4 (13) | 4 (13) | 5 (17) | 2 (7) | 0 | 15 (50) |
| Hypokalaemia | 5 (17) | 0 | 3 (10) | 0 | 0 | 8 (27) |
| Hypophosphatemia | 0 | 3 (10) | 0 | 0 | 0 | 3 (10) |
| Dehydration | 0 | 1 (3) | 1 (3) | 0 | 0 | 2 (7) |
| Hypocalcemia | 1 (3) | 1 (3) | 0 | 0 | 0 | 2 (7) |
| Decreased appetite | 0 | 1 (3) | 0 | 0 | 0 | 1 (3) |
| Hypoalbuminemia | 0 | 1 (3) | 0 | 0 | 0 | 1 (3) |
| Gastrointestinal disorders | 5 (17) | 7 (23) | 3 (10) | 0 | 0 | 15 (50) |
| Diarrhea | 5 (17) | 7 (23) | 1 (3) | 0 | 0 | 13 (43) |
| Nausea and vomiting symptoms | 4 (13) | 1 (3) | 0 | 0 | 0 | 5 (17) |
| Abdominal pain | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| Dysphagia | 0 | 0 | 1 (3) | 0 | 0 | 1 (3) |
| Lip dry | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| Small intestinal hemorrhage | 0 | 0 | 1 (3) | 0 | 0 | 1 (3) |
| Stomatitis | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| General disorders and administration site conditions | 2 (7) | 6 (20) | 2 (7) | 0 | 0 | 10 (33) |
| Asthenic conditions | 2 (7) | 5 (17) | 0 | 0 | 0 | 7 (23) |
| Chills | 1 (3) | 1 (3) | 0 | 0 | 0 | 2 (7) |
| Mucosal inflammation | 0 | 0 | 2 (7) | 0 | 0 | 2 (7) |
| Pain | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| Infections and infestations | 4 (13) | 4 (13) | 0 | 0 | 0 | 8 (27) |
| Skin structures and soft tissue infections | 2 (7) | 4 (13) | 0 | 0 | 0 | 6 (20) |
| Fungal infections NEC | 3 (10) | 1 (3) | 0 | 0 | 0 | 4 (13) |
| Groin infection | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| Lip infection | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| Investigations | 2 (7) | 3 (10) | 1 (3) | 0 | 0 | 6 (20) |
| Digestive enzymes | 0 | 2 (7) | 0 | 0 | 0 | 2 (7) |
| Weight decreased | 1 (3) | 1 (3) | 0 | 0 | 0 | 2 (7) |
| Alanine aminotransferase increased | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| Blood creatinine increased | 0 | 1 (3) | 0 | 0 | 0 | 1 (3) |
| Electrocardiogram QT prolonged | 0 | 1 (3) | 0 | 0 | 0 | 1 (3) |
| Lymphocyte count decreased | 0 | 0 | 1 (3) | 0 | 0 | 1 (3) |
| Eye disorders | 1 (3) | 1 (3) | 1 (3) | 0 | 0 | 3 (10) |
| Blepharitis | 0 | 0 | 1 (3) | 0 | 0 | 1 (3) |
| Conjunctival hyperemia | 0 | 1 (3) | 0 | 0 | 0 | 1 (3) |
| Ocular discomfort | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| Vision blurred | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| Nervous system disorders | 3 (10) | 0 | 0 | 0 | 0 | 3 (10) |
| Headache | 2 (7) | 0 | 0 | 0 | 0 | 2 (7) |
| Peripheral sensory neuropathy | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| Injury | 1 (3) | 1 (3) | 0 | 0 | 0 | 2 (7) |
| Radiation skin injury | 0 | 1 (3) | 0 | 0 | 0 | 1 (3) |
| Skin laceration | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| Reproductive system and breast disorders | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
| Perineal rash | 1 (3) | 0 | 0 | 0 | 0 | 1 (3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bauman, J.E.; Julian, R.; Saba, N.F.; Wise-Draper, T.M.; Adkins, D.R.; O’Brien, P.; Fidler, M.J.; Gibson, M.K.; Duvvuri, U.; Heath-Chiozzi, M.; et al. Phase II Trial of CDX-3379 and Cetuximab in Recurrent/Metastatic, HPV-Negative, Cetuximab-Resistant Head and Neck Cancer. Cancers 2022, 14, 2355. https://doi.org/10.3390/cancers14102355
Bauman JE, Julian R, Saba NF, Wise-Draper TM, Adkins DR, O’Brien P, Fidler MJ, Gibson MK, Duvvuri U, Heath-Chiozzi M, et al. Phase II Trial of CDX-3379 and Cetuximab in Recurrent/Metastatic, HPV-Negative, Cetuximab-Resistant Head and Neck Cancer. Cancers. 2022; 14(10):2355. https://doi.org/10.3390/cancers14102355
Chicago/Turabian StyleBauman, Julie E., Ricklie Julian, Nabil F. Saba, Trisha M. Wise-Draper, Douglas R. Adkins, Paul O’Brien, Mary Jo Fidler, Michael K. Gibson, Umamaheswar Duvvuri, Margo Heath-Chiozzi, and et al. 2022. "Phase II Trial of CDX-3379 and Cetuximab in Recurrent/Metastatic, HPV-Negative, Cetuximab-Resistant Head and Neck Cancer" Cancers 14, no. 10: 2355. https://doi.org/10.3390/cancers14102355