

Diagnosis of Depth of Submucosal Invasion in Colorectal Cancer with AI Using Deep Learning
 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
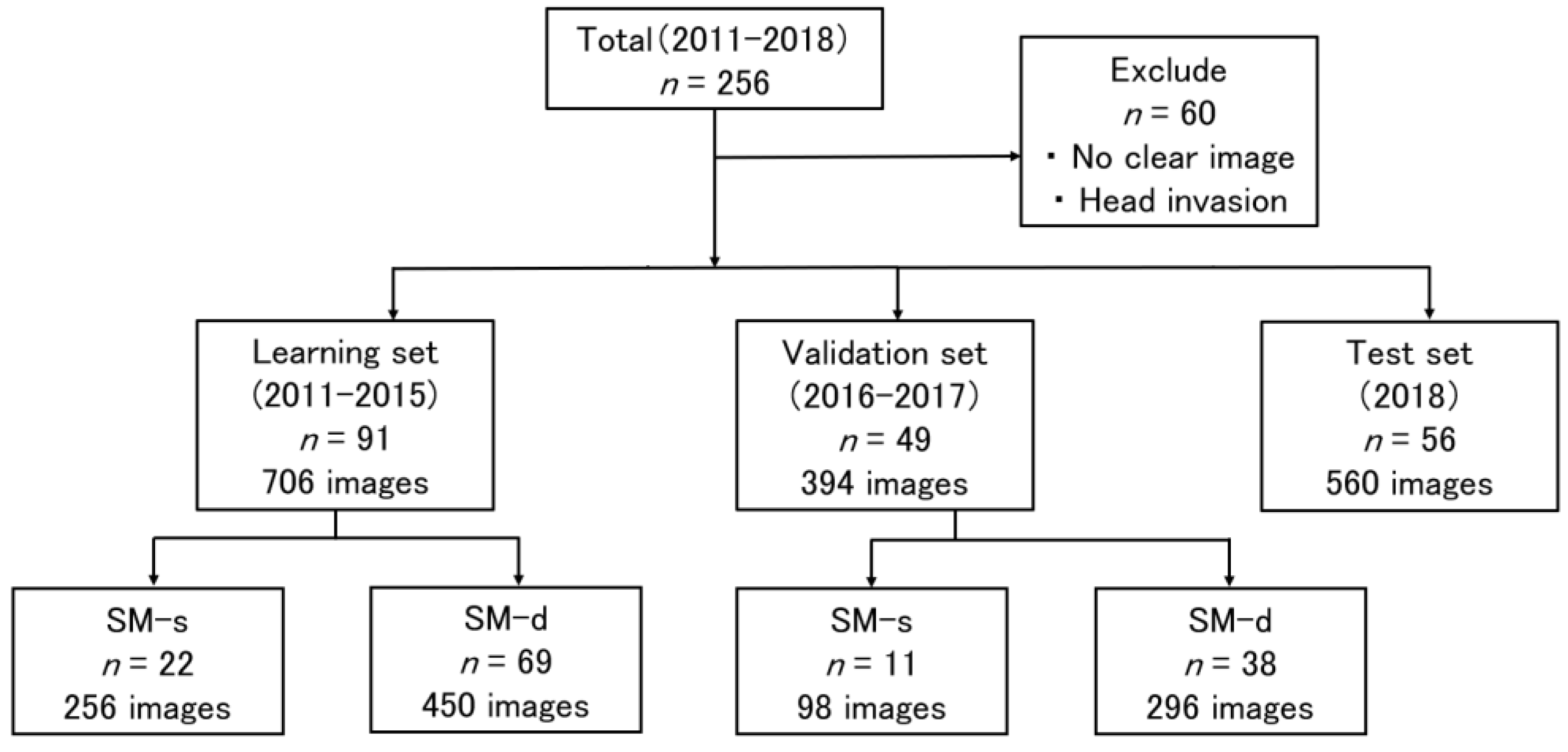
2.1. Patients and Datasets
2.2. Colonoscopy and Endoscopic Images
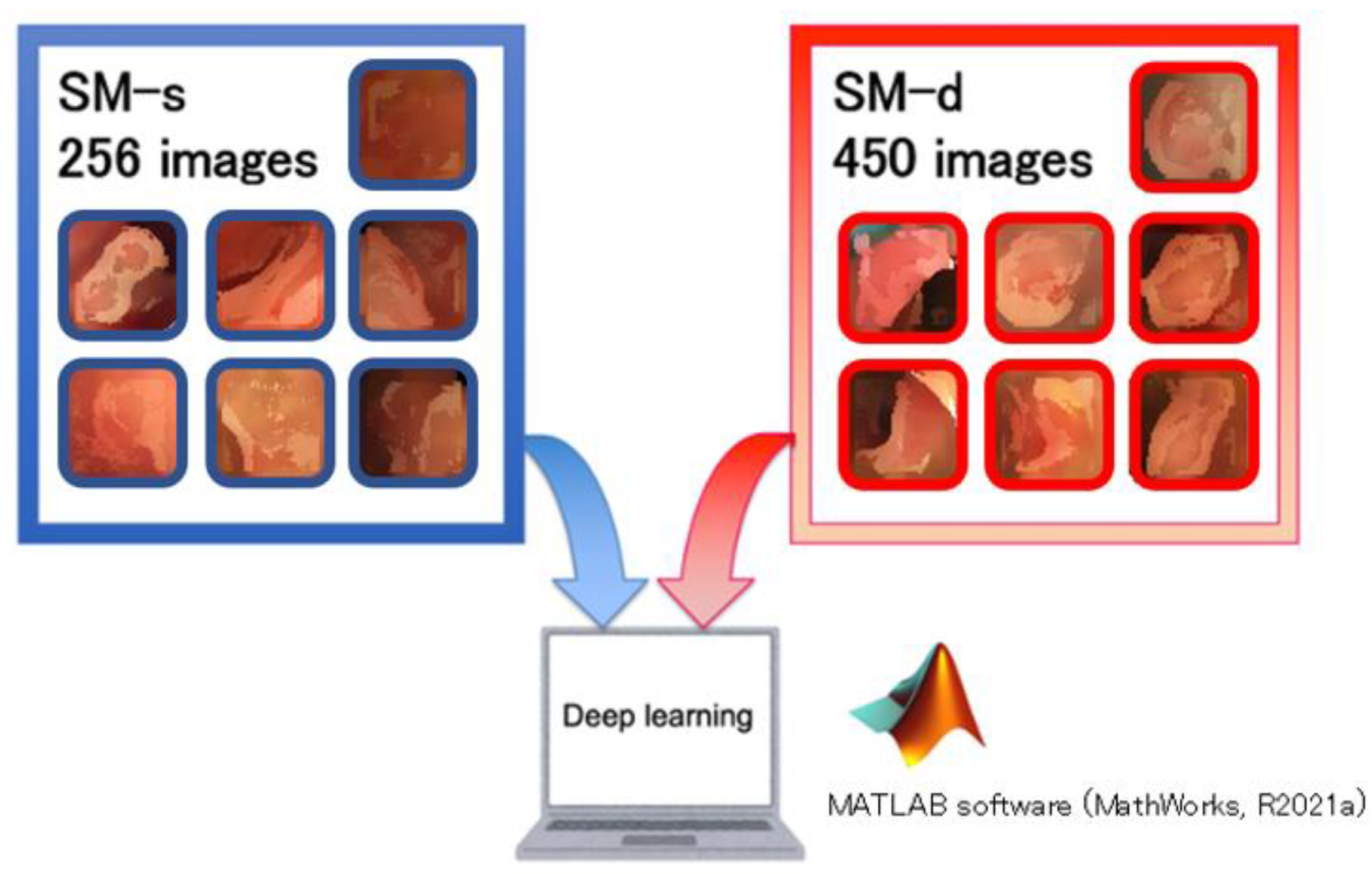
2.3. Analysis
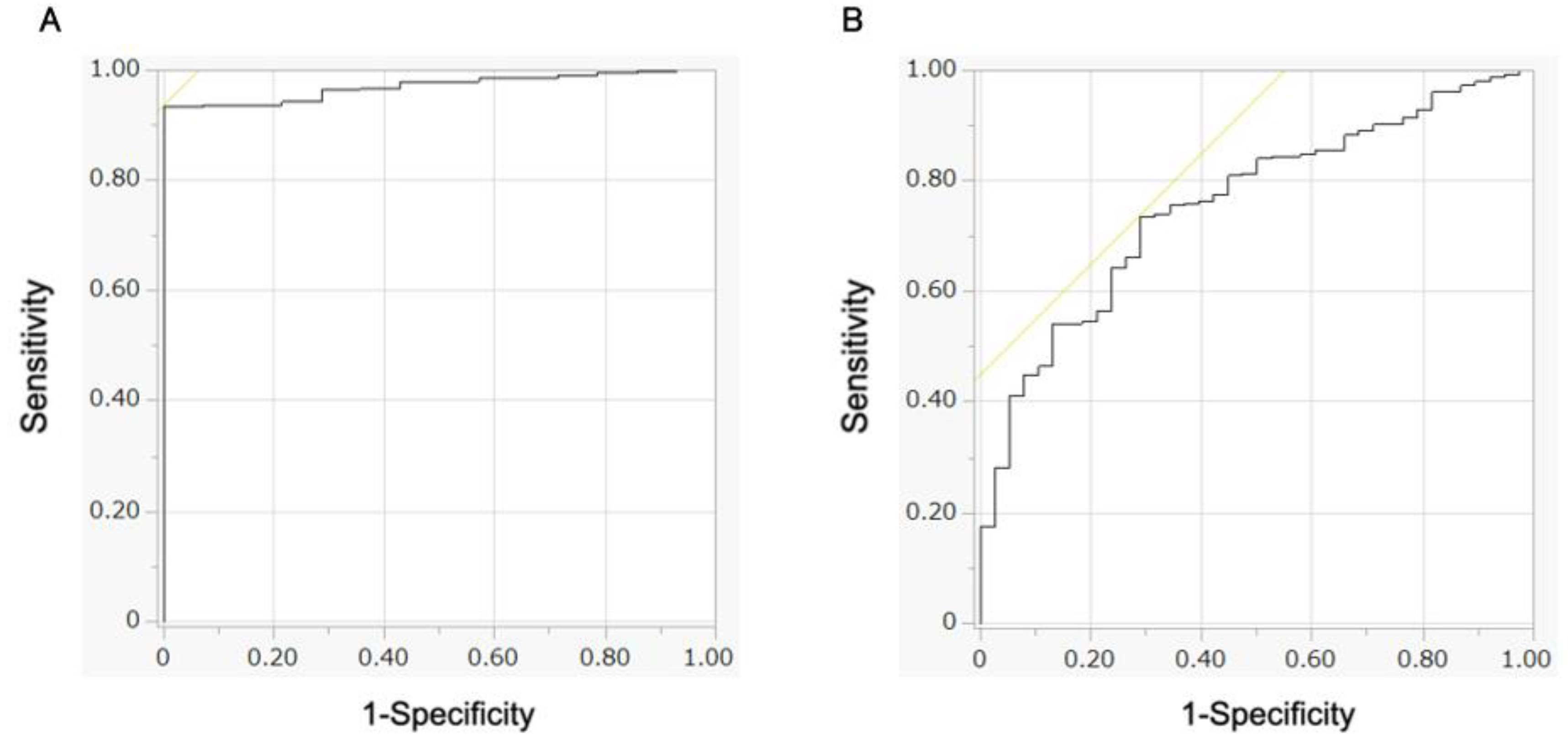
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Van Cutsem, E.; Cervantes, A.; Nordlinger, B.; Arnold, D. Metastatic colorectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2014, 25, iii1–iii9. [Google Scholar] [CrossRef] [PubMed]
- El-Shami, K.; Oeffinger, K.C.; Erb, N.L.; Willis, A.; Bretsch, J.K.; Pratt-Chapman, M.L.; Cannady, R.S.; Wong, S.L.; Rose, J.; Barbour, A.L.; et al. American Cancer Society Colorectal Cancer Survivorship Care Guidelines. CA Cancer J. Clin. 2015, 65, 428–455. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Muro, K.; Ajioka, Y.; Hashiguchi, Y.; Ito, Y.; Saito, Y.; Hamaguchi, T.; Ishida, H.; Ishiguro, M.; Ishihara, S.; et al. Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2016 for the treatment of colorectal cancer. Int. J. Clin. Oncol. 2018, 23, 1–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakamoto, T.; Saito, Y.; Nakajima, T.; Matsuda, T. Comparison of magnifying chromoendoscopy and narrow-band imaging in estimation of early colorectal cancer invasion depth: A pilot study. Dig. Endosc. 2011, 23, 118–123. [Google Scholar] [CrossRef]
- Backes, Y.; Moss, A.; Reitsma, J.B.; Siersema, P.D.; Moons, L.M. Narrow Band Imaging, Magnifying Chromoendoscopy, and Gross Morphological Features for the Optical Diagnosis of T1 Colorectal Cancer and Deep Submucosal Invasion: A Systematic Review and Meta-Analysis. Am. J. Gastroenterol. 2017, 112, 54–64. [Google Scholar] [CrossRef]
- Sano, Y.; Tanaka, S.; Kudo, S.E.; Saito, S.; Matsuda, T.; Wada, Y.; Fujii, T.; Ikematsu, H.; Uraoka, T.; Kobayashi, N.; et al. Narrow-band imaging (NBI) magnifying endoscopic classification of colorectal tumors proposed by the Japan NBI Expert Team. Dig. Endosc. 2016, 28, 526–533. [Google Scholar] [CrossRef]
- Komeda, Y.; Kashida, H.; Sakurai, T.; Asakuma, Y.; Tribonias, G.; Nagai, T.; Kono, M.; Minaga, K.; Takenaka, M.; Arizumi, T.; et al. Magnifying Narrow Band Imaging (NBI) for the Diagnosis of Localized Colorectal Lesions Using the Japan NBI Expert Team (JNET) Classification. Oncology 2017, 93, 49–54. [Google Scholar] [CrossRef]
- Fu, K.I.; Kato, S.; Sano, Y.; Onuma, E.K.; Saito, Y.; Matsuda, T.; Koba, I.; Yoshida, S.; Fujii, T. Staging of early colorectal cancers: Magnifying colonoscopy versus endoscopic ultrasonography for estimation of depth of invasion. Dig. Dis. Sci. 2008, 53, 1886–1892. [Google Scholar] [CrossRef]
- Yanai, S.; Nakamura, S.; Matsumoto, T. Role of magnifying colonoscopy for diagnosis of colorectal neoplasms: From the perspective of Japanese colonoscopists. Dig. Endosc. 2016, 28, 274–280. [Google Scholar] [CrossRef]
- Su, M.Y.; Hsu, C.M.; Ho, Y.P.; Chen, P.C.; Lin, C.J.; Chiu, C.T. Comparative study of conventional colonoscopy, chromoendoscopy, and narrow-band imaging systems in differential diagnosis of neoplastic and nonneoplastic colonic polyps. Am. J. Gastroenterol. 2006, 101, 2711–2716. [Google Scholar] [CrossRef] [PubMed]
- Kawaguti, F.S.; Franco, M.C.; Martins, B.C.; Segateli, V.; Marques, C.F.S.; Nahas, C.S.R.; Pinto, R.A.; Safatle-Ribeiro, A.V.; Ribeiro-Junior, U.; Nahas, S.C.; et al. Role of Magnification Chromoendoscopy in the Management of Colorectal Neoplastic Lesions Suspicious for Submucosal Invasion. Dis. Colon. Rectum. 2019, 62, 422–428. [Google Scholar] [CrossRef] [PubMed]
- Pinto, N.; Cox, D.D.; DiCarlo, J.J. Why is real-world visual object recognition hard? PLoS Comput. Biol. 2008, 4, e27. [Google Scholar] [CrossRef] [PubMed]
- Bibault, J.E.; Giraud, P.; Burgun, A. Big Data and machine learning in radiation oncology: State of the art and future prospects. Cancer Lett. 2016, 382, 110–117. [Google Scholar] [CrossRef]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. Imagenet classification with deep convolutional neural networks. Commun. ACM 2017, 60, 84–90. [Google Scholar] [CrossRef] [Green Version]
- Fukushima, K.; Miyake, S. Neocognitron: A new algorithm for pattern recognition tolerant of deformations and shifts in position. Pattern Recognit. 1982, 15, 455–469. [Google Scholar] [CrossRef]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef]
- Gulshan, V.; Peng, L.; Coram, M.; Stumpe, M.C.; Wu, D.; Narayanaswamy, A.; Venugopalan, S.; Widner, K.; Madams, T.; Cuadros, J.; et al. Development and Validation of a Deep Learning Algorithm for Detection of Diabetic Retinopathy in Retinal Fundus Photographs. JAMA 2016, 316, 2402–2410. [Google Scholar] [CrossRef]
- Hirasawa, T.; Aoyama, K.; Tanimoto, T.; Ishihara, S.; Shichijo, S.; Ozawa, T.; Ohnishi, T.; Fujishiro, M.; Matsuo, K.; Fujisaki, J.; et al. Application of artificial intelligence using a convolutional neural network for detecting gastric cancer in endoscopic images. Gastric Cancer 2018, 21, 653–660. [Google Scholar] [CrossRef] [Green Version]
- Miyoshi, N. AI application for surgery. J. Jpn. Soc. Precis. Eng. 2022, 88, 9–11. [Google Scholar] [CrossRef]
- Zeiler, M.D.; Fergus, R. Visualizing and Understanding Convolutional Networks. In Proceedings of the European Conference on Computer Vision, Zurich, Switzerland, 6–12 September 2014; Springer: Berlin/Heidelberg, Germany, 2014; pp. 818–833. [Google Scholar]
- Machida, H.; Sano, Y.; Hamamoto, Y.; Muto, M.; Kozu, T.; Tajiri, H.; Yoshida, S. Narrow-band imaging in the diagnosis of colorectal mucosal lesions: A pilot study. Endoscopy 2004, 36, 1094–1098. [Google Scholar] [CrossRef] [PubMed]
- Apel, D.; Jakobs, R.; Schilling, D.; Weickert, U.; Teichmann, J.; Bohrer, M.H.; Riemann, J.F. Accuracy of high-resolution chromoendoscopy in prediction of histologic findings in diminutive lesions of the rectosigmoid. Gastrointest. Endosc. 2006, 63, 824–828. [Google Scholar] [CrossRef] [PubMed]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef]
- Xu, Y.; Jia, Z.; Wang, L.B.; Ai, Y.; Zhang, F.; Lai, M.; Chang, E.I. Large scale tissue histopathology image classification, segmentation, and visualization via deep convolutional activation features. BMC Bioinform. 2017, 18, 281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hattori, S.; Iwatate, M.; Sano, W.; Hasuike, N.; Kosaka, H.; Ikumoto, T.; Kotaka, M.; Ichiyanagi, A.; Ebisutani, C.; Hisano, Y.; et al. Narrow-band imaging observation of colorectal lesions using NICE classification to avoid discarding significant lesions. World J. Gastrointest. Endosc. 2014, 6, 600–605. [Google Scholar] [CrossRef]
- Kaltenbach, T.; Sano, Y.; Friedland, S.; Soetikno, R. American Gastroenterological Association (AGA) Institute technology assessment on image-enhanced endoscopy. Gastroenterology 2008, 134, 327–340. [Google Scholar] [CrossRef]
- Kudo, S.; Tamura, S.; Nakajima, T.; Yamano, H.; Kusaka, H.; Watanabe, H. Diagnosis of colorectal tumorous lesions by magnifying endoscopy. Gastrointest. Endosc. 1996, 44, 8–14. [Google Scholar] [CrossRef]
- Kanao, H.; Tanaka, S.; Oka, S.; Kaneko, I.; Yoshida, S.; Arihiro, K.; Yoshihara, M.; Chayama, K. Clinical significance of type V(I) pit pattern subclassification in determining the depth of invasion of colorectal neoplasms. World J. Gastroenterol. 2008, 14, 211–217. [Google Scholar] [CrossRef]
- Sikka, S.; Ringold, D.A.; Jonnalagadda, S.; Banerjee, B. Comparison of white light and narrow band high definition images in predicting colon polyp histology, using standard colonoscopes without optical magnification. Endoscopy 2008, 40, 818–822. [Google Scholar] [CrossRef]
- Sakamoto, T.; Nakajima, T.; Matsuda, T.; Murakami, Y.; Ishikawa, H.; Yao, K.; Saito, Y. Comparison of the diagnostic performance between magnifying chromoendoscopy and magnifying narrow-band imaging for superficial colorectal neoplasms: An online survey. Gastrointest. Endosc. 2018, 87, 1318–1323. [Google Scholar] [CrossRef]
- İncetan, K.; Celik, I.O.; Obeid, A.; Gokceler, G.I.; Ozyoruk, K.B.; Almalioglu, Y.; Chen, R.J.; Mahmood, F.; Gilbert, H.; Durr, N.J.; et al. VR-Caps: A Virtual Environment for Capsule Endoscopy. Med. Image Anal. 2021, 70, 101990. [Google Scholar] [CrossRef] [PubMed]
- Mathew, S.; Nadeem, S.; Kaufman, A. CLTS-GAN: Color-Lighting-Texture-Specular Reflection Augmentation for Colonoscopy. In International Conference on Medical Image Computing and Computer-Assisted Intervention; Springer: Cham, Germany, 2022; pp. 519–529. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Variables | Learning Set (2011–2015) | Validation Set (2016–2017) |
|---|---|---|
| n = 91 | n = 49 | |
| Age, median (years) * | 66 (41–86) | 66 (35–84) |
| Sex (male/female) | 59/32 | 28/21 |
| Location (colon/rectum) | 54/37 | 32/17 |
| Greatest diameter, median (mm) | 20 (0–50) | 20 (6–66) |
| Preoperative CEA (≥5/5</NA) (ng/mL) | 12/78/1 | 11/36/2 |
| Preoperative CA19-9 (≥38/38</NA) (ng/mL) | 5/85/1 | 3/44/2 |
| Degree of differentiation (tub1/tub2/others) | 57/30/4 | 29/19/1 |
| Depth of invasion, median (µm) * | 2000 (0–9000) | 2200 (91–12,000) |
| Lymph node metastasis (+/−) | 7/84 | 7/42 |
| Lymphatic invasion (+/−) | 24/67 | 16/33 |
| Vascular invasion (+/−) | 12/79 | 7/42 |
| Budding grade (1/2, 3/NA) | 54/16/21 | 37/8/4 |
| Variables | SM-s (n = 22) | SM-d (n = 69) | p-Value |
|---|---|---|---|
| Age, median (years) * | 66 (41–86) | 66 (35–84) | 0.846 |
| Sex (male/female) | 15/7 | 44/25 | 0.706 |
| Location (C/A/T/D/S/R) a | 1/2/1/0/7/11 | 7/14/7/5/10/26 | NA |
| Degree of differentiation (tub1, 2/others) | 22/0 | 65/4 | 0.248 |
| Lymphatic invasion (+/−) | 4/18 | 20/49 | 0.317 |
| Vascular invasion (+/−) | 2/20 | 10/59 | 0.514 |
| Budding grade (1/2, 3) ** | 13/2 | 41/14 | 0.322 |
| AI Diagnosis | |||
|---|---|---|---|
| SM-s | SM-d | ||
| Pathological classification | SM-s n = 11 98 images | 35 images | 63 images |
| SM-d n = 38 296 images | 38 images | 258 images | |
| (A) | |||||
| n = 56 560 images | |||||
| Age, median (years) * | 63.8 (38–82) | ||||
| Sex (male/female) | 30/26 | ||||
| Location (C/A/T/D/S/R) a | 5/7/9/5/8/22 | ||||
| Degree of differentiation (tub1/tub2/others) | 37/17/2 | ||||
| Lymphatic invasion (+/−) | 11/45 | ||||
| Vascular invasion (+/−) | 5/51 | ||||
| Budding grade (1/2, 3/NA) | 40/14/2 | ||||
| (B) | |||||
| Clinical diagnosis | AI diagnosis | ||||
| SM-s | SM-d | SM-s | SM-d | ||
| Pathological classification | SM-s n = 9 90 images | n = 5 | n = 4 | 24 images | 66 images |
| SM-d n = 47 470 images | n = 17 | n = 30 | 114 images | 356 images | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minami, S.; Saso, K.; Miyoshi, N.; Fujino, S.; Kato, S.; Sekido, Y.; Hata, T.; Ogino, T.; Takahashi, H.; Uemura, M.; et al. Diagnosis of Depth of Submucosal Invasion in Colorectal Cancer with AI Using Deep Learning. Cancers 2022, 14, 5361. https://doi.org/10.3390/cancers14215361
Minami S, Saso K, Miyoshi N, Fujino S, Kato S, Sekido Y, Hata T, Ogino T, Takahashi H, Uemura M, et al. Diagnosis of Depth of Submucosal Invasion in Colorectal Cancer with AI Using Deep Learning. Cancers. 2022; 14(21):5361. https://doi.org/10.3390/cancers14215361
Chicago/Turabian StyleMinami, Soichiro, Kazuhiro Saso, Norikatsu Miyoshi, Shiki Fujino, Shinya Kato, Yuki Sekido, Tsuyoshi Hata, Takayuki Ogino, Hidekazu Takahashi, Mamoru Uemura, and et al. 2022. "Diagnosis of Depth of Submucosal Invasion in Colorectal Cancer with AI Using Deep Learning" Cancers 14, no. 21: 5361. https://doi.org/10.3390/cancers14215361