
Evaluation of the Cellular Dissociation Grading, Based on Tumor Budding and Cell Nest Size, in Squamous Cell Carcinoma of the Penis

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Microscopy
2.3. Cellular Dissociation Grade (CDG)
2.4. Statistics
3. Results
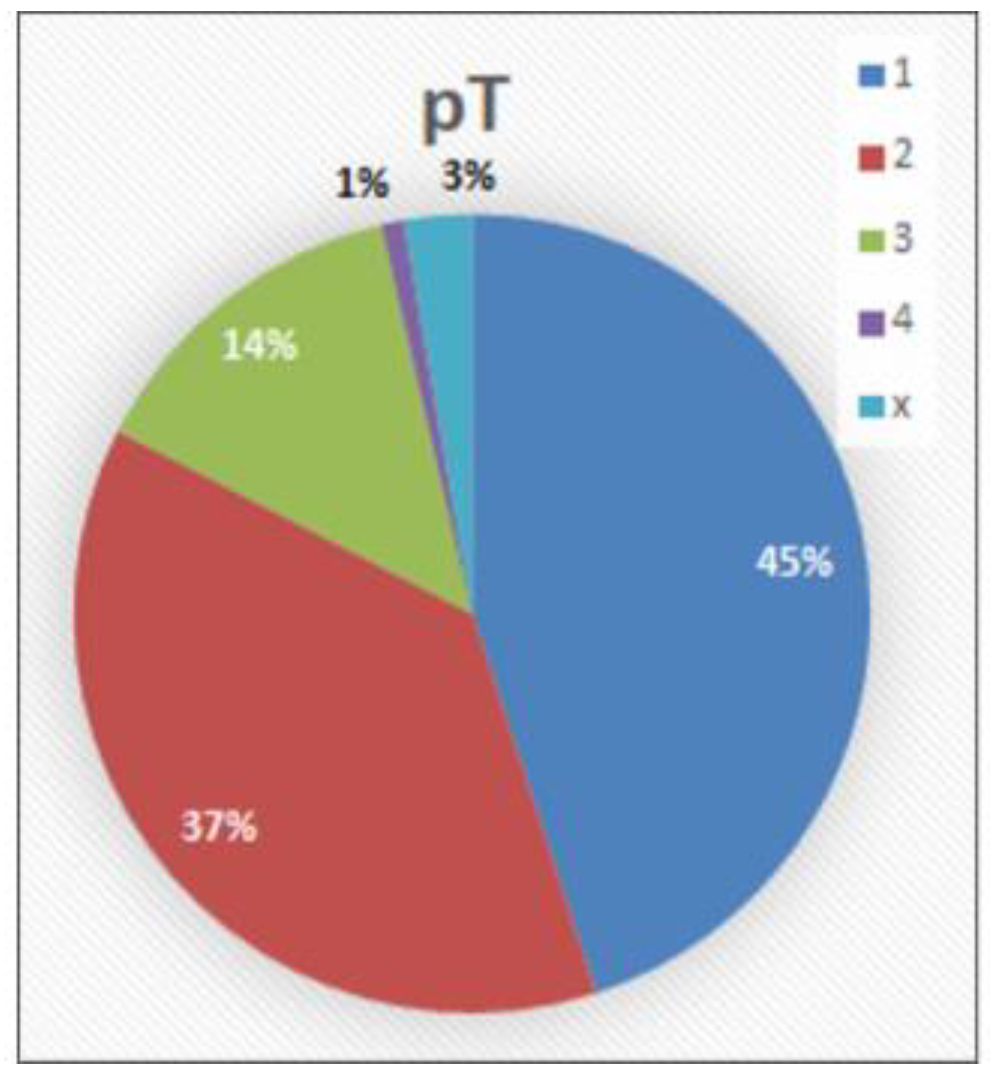
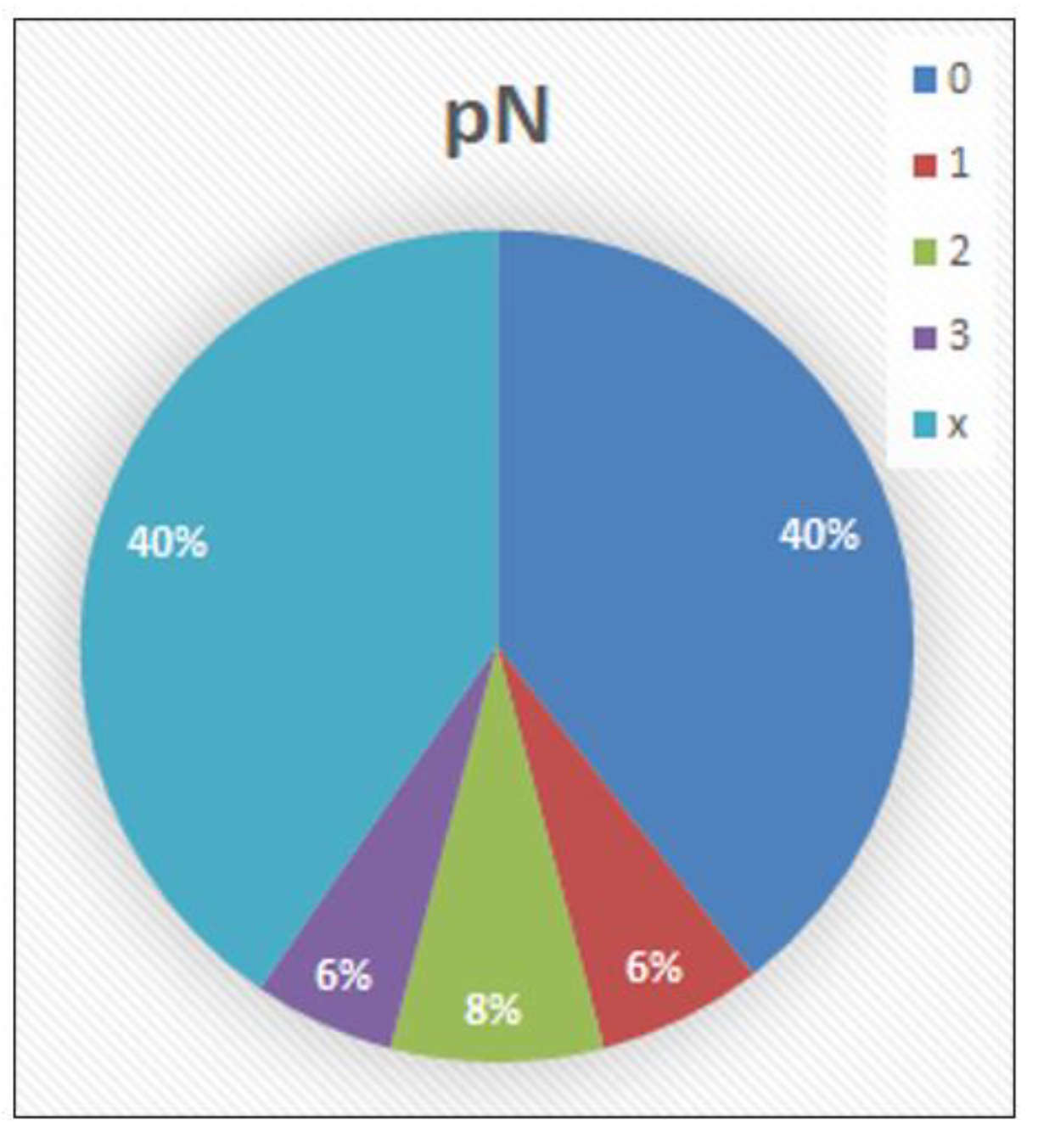
3.1. Distribution of Collective Characteristics
3.2. Comparison of Grading Systems
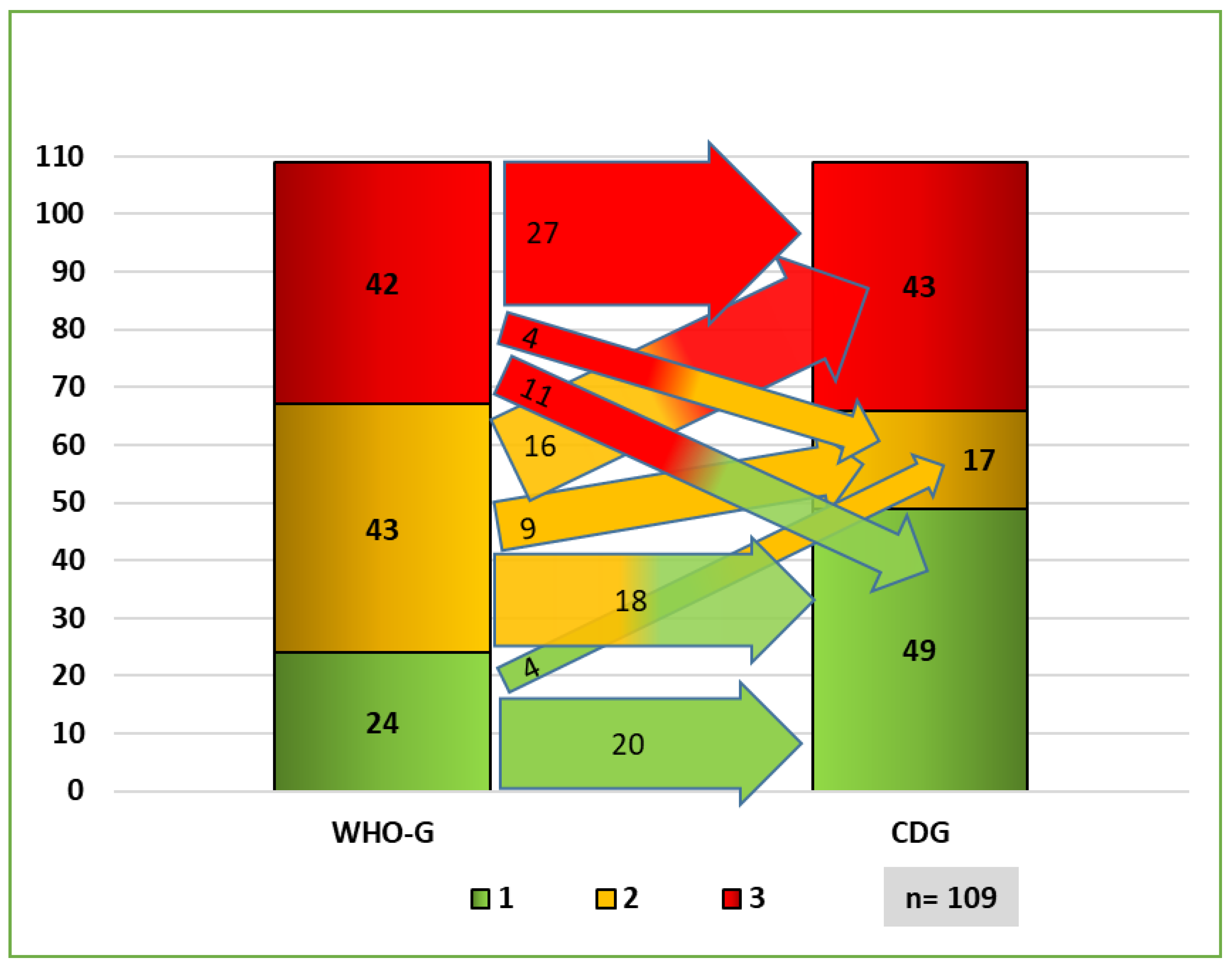
3.2.1. Distribution of Grading Systems
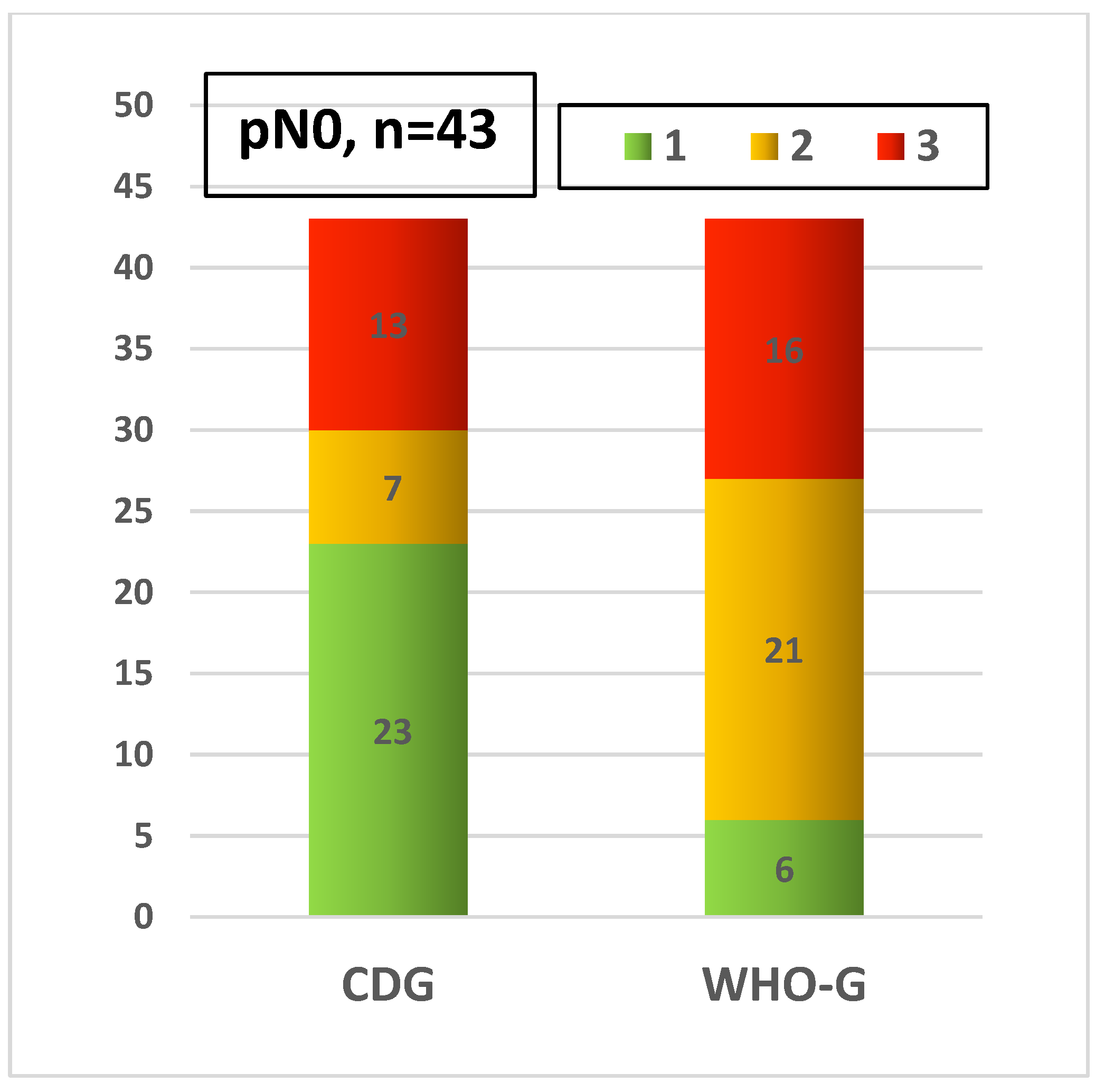
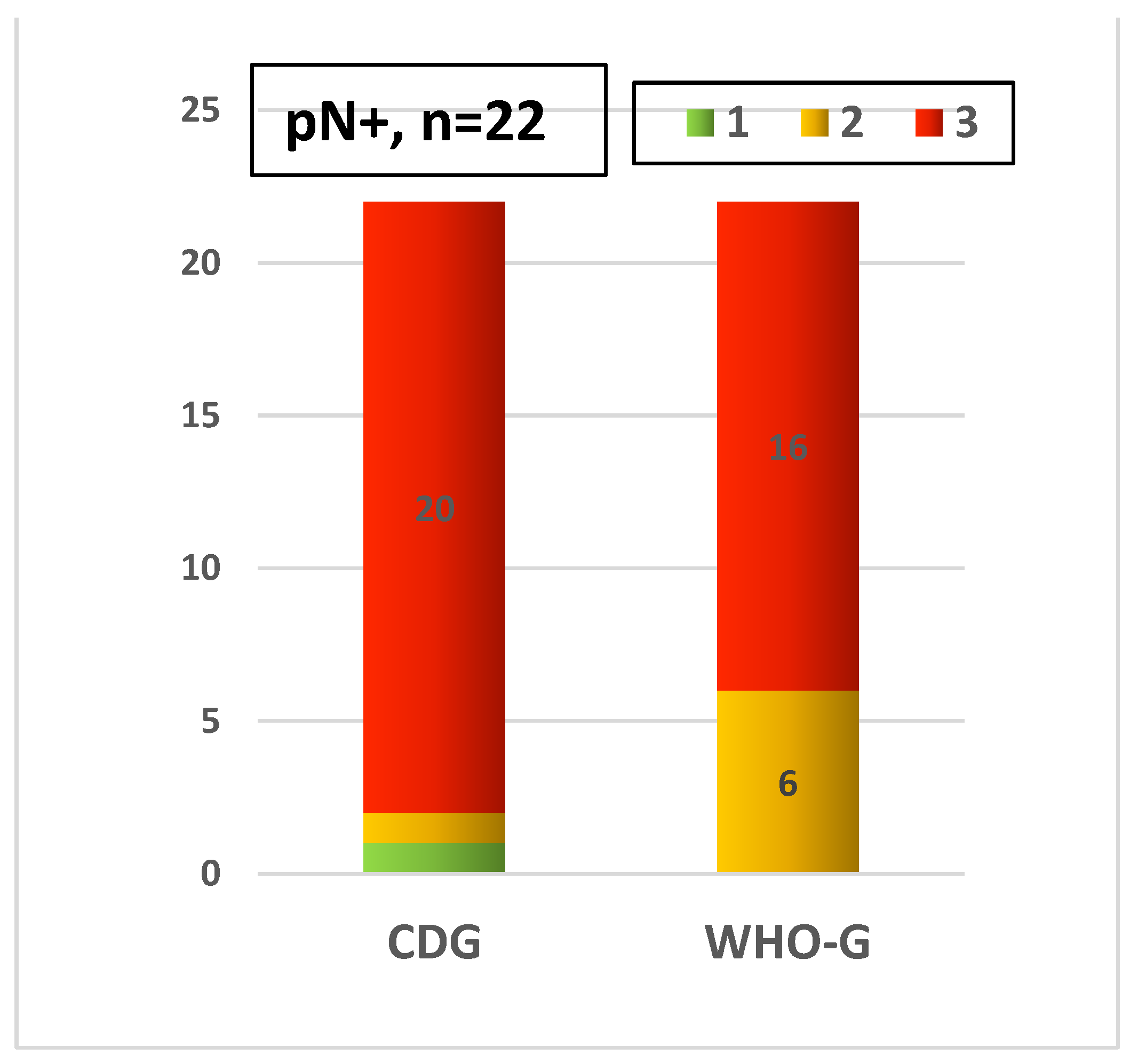
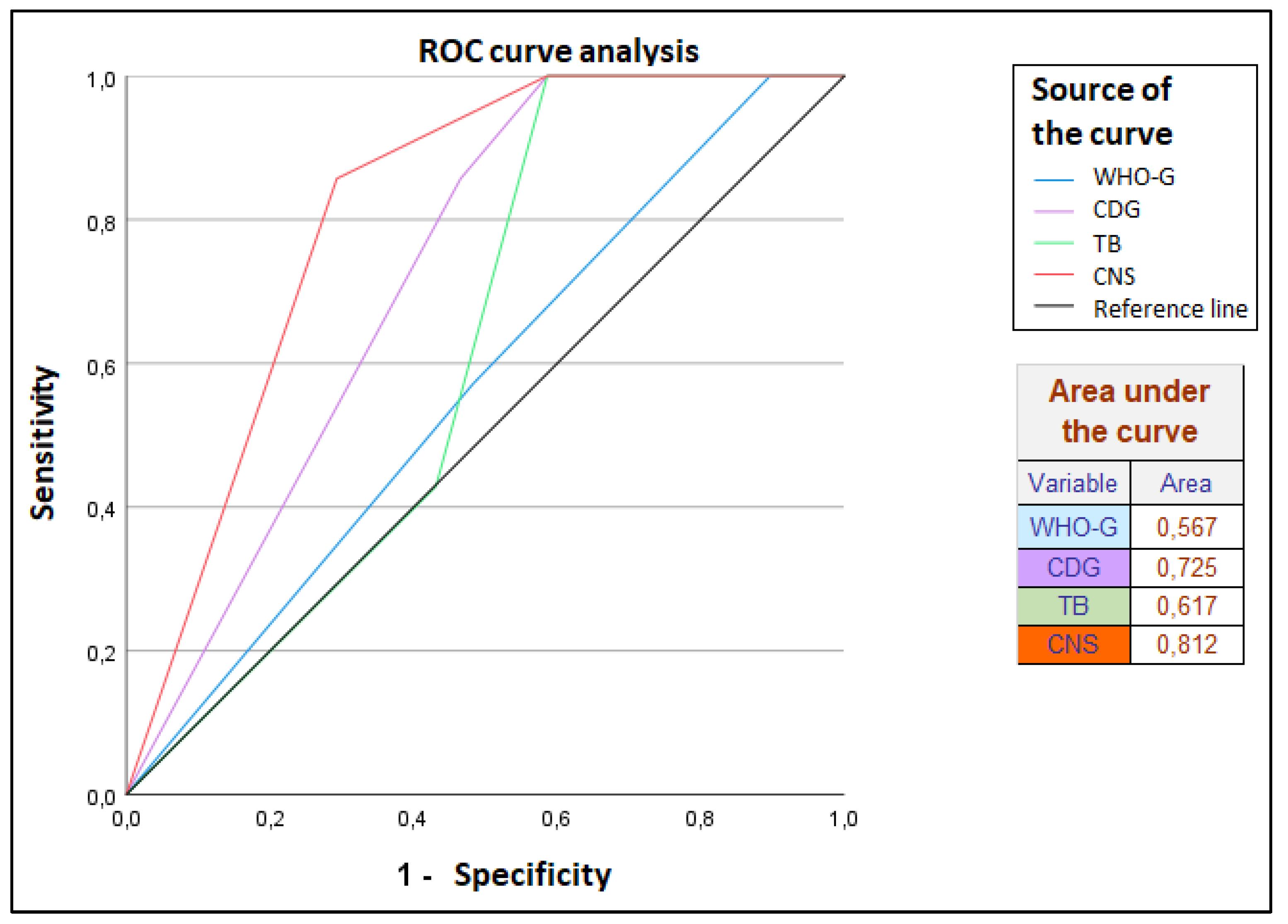
3.2.2. Prognostic Validity of Grading Systems for Lymph Node Status (pN)
3.3. Interobserver Concordance
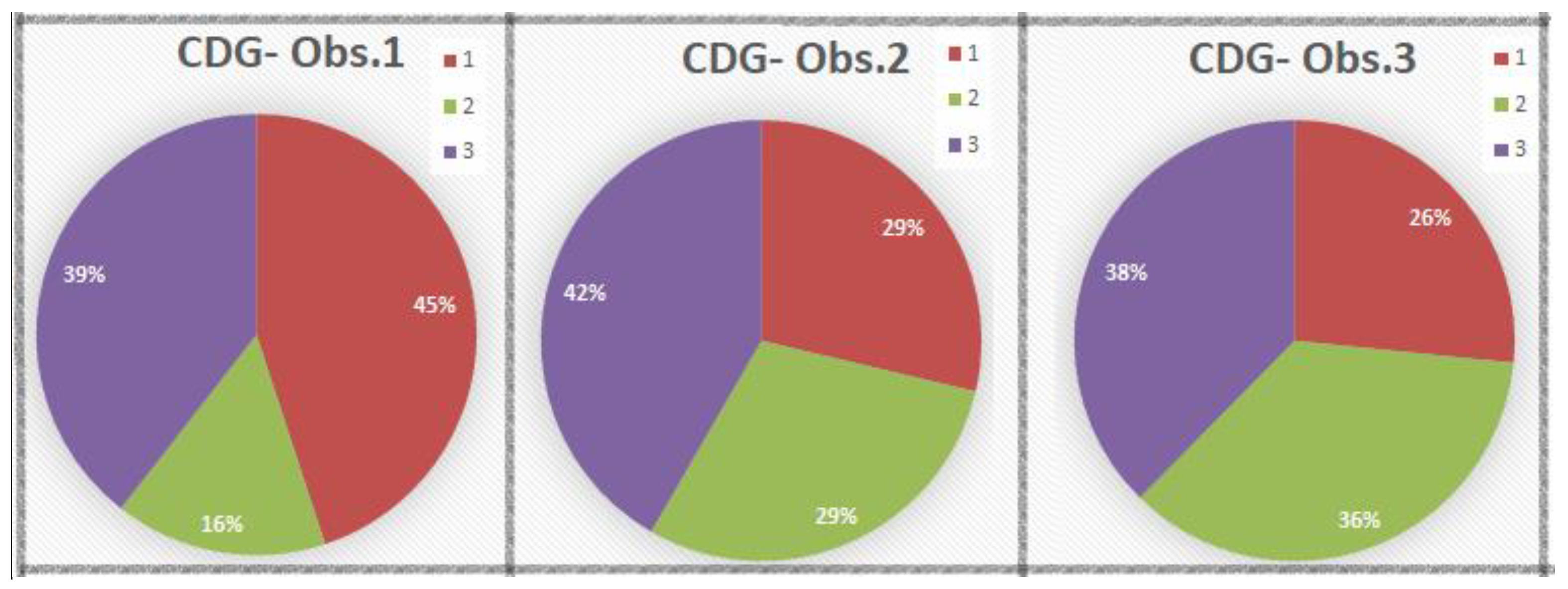
3.4. CDG Spectrum of the Three Pathologists
4. Discussion
4.1. Significance and Problems of the WHO Grading in Penile Carcinoma
4.2. Cellular Dissociation Grading (CDG) in International Studies
4.3. Evaluation of Cellular Dissociation Grading (CDG) in Penile Carcinoma
4.4. Limitations and Problems of CDG Grading
4.5. Interobserver Variation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alkatout, I.; Naumann, C.M.; Hedderich, J.; Hegele, A.; Bolenz, C.; Jünemann, K.-P.; Klöppel, G. Squamous cell carcinoma of the penis: Predicting nodal metastases by histologic grade, pattern of invasion and clinical examination. Urol. Oncol. Semin. Orig. Investig. 2011, 29, 774–781. [Google Scholar] [CrossRef]
- Gravas (Chair), S.; Cornu, J.N.; Gacci, M.; Gratzke, C.; Herrmann, T.R.W.; Mamoulakis, C.; Rieken, M.; Speakman, M.J.; Tikkinen, K.A.O. EAU Guidelines: Management of Non-Neurogenic Male LUTS; EAU: Arnhem, The Netherlands, 2020; ISBN 978-94-92671-07-3. [Google Scholar]
- Leitlinienprogramm Onkologie (Deutsche Krebsgesellschaft, Deutsche Krebshilfe, AWMF): S3-Leitlinie Diagnostik, Therapie und Nachsorge des Peniskarzinoms, Langversion 1.0, 2020, AWMF Registernummer: 043-042OL. Available online: https://www.leitlinienprogramm-onkologie.de/leitlinien/peniskarzinom/ (accessed on 16 January 2022).
- Boxberg, M.; Bollwein, C.; Jöhrens, K.; Kuhn, P.-H.; Haller, B.; Steiger, K.; Wolff, K.-D.; Kolk, A.; Jesinghaus, M.; Weichert, W. Novel prognostic histopathological grading system in oral squamous cell carcinoma based on tumour budding and cell nest size shows high interobserver and intraobserver concordance. J. Clin. Pathol. 2018, 72, 285–294. [Google Scholar] [CrossRef] [PubMed]
- Boxberg, M.; Jesinghaus, M.; Dorfner, C.; Mogler, C.; Drecoll, E.; Warth, A.; Steiger, K.; Bollwein, C.; Meyer, P.; Wolff, K.D.; et al. Tumour budding activity and cell nest size determine patient outcome in oral squamous cell carcinoma: Proposal for an adjusted grading system. Histopathology 2017, 70, 1125–1137. [Google Scholar] [CrossRef]
- Boxberg, M.; Kuhn, P.-H.; Reiser, M.; Erb, A.; Steiger, K.; Pickhard, A.; Straßen, U.; Koob, I.; Kolk, A.; Warth, A.; et al. Tumor Budding and Cell Nest Size Are Highly Prognostic in Laryngeal and Hypopharyngeal Squamous Cell Carcinoma. Am. J. Surg. Pathol. 2019, 43, 303–313. [Google Scholar] [CrossRef] [PubMed]
- Jesinghaus, M.; Boxberg, M.; Konukiewitz, B.; Slotta-Huspenina, J.; Schlitter, A.M.; Steiger, K.; Specht, K.; Wieczorek, K.; Warth, A.; Schmidt, T.; et al. A Novel Grading System Based on Tumor Budding and Cell Nest Size Is a Strong Predictor of Patient Outcome in Esophageal Squamous Cell Carcinoma. Am. J. Surg. Pathol. 2017, 41, 1112–1120. [Google Scholar] [CrossRef]
- Jesinghaus, M.; Strehl, J.; Boxberg, M.; Bruehl, F.; Wenzel, A.; Konukiewitz, B.; Schlitter, A.M.; Steiger, K.; Warth, A.; Schnelzer, A.; et al. Introducing a novel highly prognostic grading scheme based on tumour budding and cell nest size for squamous cell carcinoma of the uterine cervix. J. Pathol. Clin. Res. 2018, 4, 93–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jesinghaus, M.; Boxberg, M.; Wilhelm, D.; Münch, S.; Dapper, H.; Quante, M.; Schlag, C.; Lange, S.; Budczies, J.; Konukiewitz, B.; et al. Post-neoadjuvant cellular dissociation grading based on tumour budding and cell nest size is associated with therapy response and survival in oesophageal squamous cell carcinoma. Br. J. Cancer 2019, 121, 1050–1057. [Google Scholar] [CrossRef]
- Jesinghaus, M.; Bruehl, F.; Steiger, K.; Klare, P.; Reiser, M.; Scheiter, A.; Konukiewitz, B.; Kuhn, P.; Münch, S.; Quante, M.; et al. Cellular Dissociation Grading Based on the Parameters Tumor Budding and Cell Nest Size in Pretherapeutic Biopsy Specimens Allows for Prognostic Patient Stratification in Esophageal Squamous Cell Carcinoma Independent from Clinical Staging. Am. J. Surg. Pathol. 2019, 43, 618–627. [Google Scholar] [CrossRef] [PubMed]
- Jesinghaus, M.; Steiger, K.; Stögbauer, F.; Haller, B.; Kolk, A.; Straßen, U.; Pickhard, A.; Wirth, M.; Silva, M.; Budczies, J.; et al. Pre-operative cellular dissociation grading in biopsies is highly predictive of post-operative tumour stage and patient outcome in head and neck squamous cell carcinoma. Br. J. Cancer 2020, 122, 835–846. [Google Scholar] [CrossRef]
- Dawson, H.; Galuppini, F.; Träger, P.; Berger, M.D.; Studer, P.; Brügger, L.; Zlobec, I.; Inderbitzin, D.; Lugli, A. Validation of the International Tumor Budding Consensus Conference 2016 recommendations on tumor budding in stage I–IV colorectal cancer. Hum. Pathol. 2018, 85, 145–151. [Google Scholar] [CrossRef]
- Lugli, A.; Cathomas, G. Pathologie: Tumor Budding beim kolorektalen Karzinom: Ein Spitzenspieler auf der Ersatzbank? Swiss Med. Forum-Schweiz. Med. 2012, 12. [Google Scholar] [CrossRef] [Green Version]
- Lugli, A.; Kirsch, R.; Ajioka, Y.; Bosman, F.; Cathomas, G.; Dawson, H.; El Zimaity, H.; Fléjou, J.-F.; Hansen, T.P.; Hartmann, A.; et al. Recommendations for reporting tumor budding in colorectal cancer based on the International Tumor Budding Consensus Conference (ITBCC) 2016. Mod. Pathol. 2017, 30, 1299–1311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Müller, F.; Lugli, A.; Dawson, H. Tumor Budding beim kolorektalen Karzinom—Informationen zur klinischen Anwendung und Anleitung zur praktischen Bestimmung. Der Pathol. 2021, 43, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Prall, F. Tumour budding in colorectal carcinoma. Histopathology 2007, 50, 151–162. [Google Scholar] [CrossRef]
- Prall, F.; Nizze, H.; Barten, M. Tumour budding as prognostic factor in stage I/II colorectal carcinoma. Histopathology 2005, 47, 17–24. [Google Scholar] [CrossRef]
- Moch, H.; Humphrey, P.; Ulbright, T.; Reuter, V. WHO Classification of Tumours of the Urinary System and Male Genital Organs. In World Health Organization Classification of Tumours, 4th ed.; International Agency for Research on Cancer: Lyon, France, 2016; Volume 8, ISBN 978-92-832-2437-2. [Google Scholar]
- WHO Classification of Tumours Editorial Board. Urinary and Male Genital Tumours. In WHO Classification of Tumours Series, 5th ed.; International Agency for Research on Cancer: Lyon, France, 2022; Volume 8, ISBN 9789283245124. [Google Scholar]
- Wittekind, C. TNM Klassifikation Maligner Tumoren. Achte Auflage; WILEY-VCH: Weinheim, Germany, 2017; ISBN 978-3-527-34280-8. [Google Scholar]
- Kim, D.; Pantanowitz, L.; Schüttler, P.; Yarlagadda, D.V.K.; Ardon, O.; Reuter, V.E.; Hameed, M.; Klimstra, D.S.; Hanna, M.G. (Re) Defining the High-Power Field for Digital Pathology. J. Pathol. Inform. 2020, 11, 33. [Google Scholar] [CrossRef] [PubMed]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Erbersdobler, A. Pathologie und histopathologische Begutachtung des Peniskarzinoms. Der Urol. 2018, 57, 391–397. [Google Scholar] [CrossRef]
- Kreppel, M.; Nazarli, P.; Grandoch, A.; Safi, A.-F.; Zirk, M.; Nickenig, H.-J.; Scheer, M.; Rothamel, D.; Hellmich, M.; Zöller, J.E. Clinical and histopathological staging in oral squamous cell carcinoma—Comparison of the prognostic significance. Oral Oncol. 2016, 60, 68–73. [Google Scholar] [CrossRef]
- Koch, W.M.; Ridge, J.A.; Forastiere, A.; Manola, J. Comparison of clinical and pathological staging in head and neck squamous cell carcinoma: Results from Intergroup Study ECOG 4393/RTOG 9614. Arch. Otolaryngol. Head Neck Surg. 2009, 135, 851–858. [Google Scholar] [CrossRef]
- Weichert, W.; Kossakowski, C.; Harms, A.; Schirmacher, P.; Muley, T.; Dienemann, H.; Warth, A. Proposal of a prognostically relevant grading scheme for pulmonary squamous cell carcinoma. Eur. Respir. J. 2015, 47, 938–946. [Google Scholar] [CrossRef]
- Kadota, K.; Miyai, Y.; Katsuki, N.; Kushida, Y.; Matsunaga, T.; Okuda, M.; Yokomise, H.; Kanaji, N.; Bandoh, S.; Haba, R. A Grading System Combining Tumor Budding and Nuclear Diameter Predicts Prognosis in Resected Lung Squamous Cell Carcinoma. Am. J. Surg. Pathol. 2017, 41, 750–760. [Google Scholar] [CrossRef]
- Kadota, K.; Nitadori, J.-I.; Woo, K.M.; Sima, C.S.; Finley, D.J.; Rusch, V.W.; Adusumilli, P.S.; Travis, W.D. Comprehensive Pathological Analyses in Lung Squamous Cell Carcinoma: Single Cell Invasion, Nuclear Diameter, and Tumor Budding Are Independent Prognostic Factors for Worse Outcomes. J. Thorac. Oncol. 2014, 9, 1126–1139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neppl, C.; Zlobec, I.; Schmid, R.A.; Berezowska, S. Validation of the International Tumor Budding Consensus Conference (ITBCC) 2016 recommendation in squamous cell carcinoma of the lung—A single-center analysis of 354 cases. Mod. Pathol. 2019, 33, 802–811. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Shen, H.; Qiu, C.; Zhang, T.; Hu, P.; Qu, X.; Liu, Q.; Du, J. Invasion Types Are Associated with Poor Prognosis in Lung Squamous Carcinoma Patients. Medicine 2015, 94, e1634. [Google Scholar] [CrossRef]
- Almangush, A.; Bello, I.O.; Keski–Säntti, H.; Mäkinen, L.K.; Kauppila, J.H.; Pukkila, M.; Hagström, J.; Laranne, J.; Tommola, S.; Nieminen, O.; et al. Depth of invasion, tumor budding, and worst pattern of invasion: Prognostic indicators in early-stage oral tongue cancer. Head Neck 2013, 36, 811–818. [Google Scholar] [CrossRef]
- Shimizu, S.; Miyazaki, A.; Sonoda, T.; Koike, K.; Ogi, K.; Kobayashi, J.-I.; Kaneko, T.; Igarashi, T.; Ueda, M.; Dehari, H.; et al. Tumor budding is an independent prognostic marker in early stage oral squamous cell carcinoma: With special reference to the mode of invasion and worst pattern of invasion. PLoS ONE 2018, 13, e0195451. [Google Scholar] [CrossRef] [Green Version]
- Karpathiou, G.; Gavid, M.; Prevot-Bitot, N.; Dhomps, A.; Dumollard, J.M.; Vieville, M.; Lelonge, Y.; Prades, J.M.; Froudarakis, M.; Peoc’H, M. Correlation Between Semiquantitative Metabolic Parameters After PET/CT and Histologic Prognostic Factors in Laryngeal and Pharyngeal Carcinoma. Head Neck Pathol. 2020, 14, 724–732. [Google Scholar] [CrossRef]
- Sarioglu, S.; Acara, C.; Akman, F.C.; Dag, N.; Ecevit, C.; Ikiz, A.O.; Cetinayak, O.H.; Ada, E. Tumor budding as a prognostic marker in laryngeal carcinoma. Pathol.-Res. Pr. 2010, 206, 88–92. [Google Scholar] [CrossRef]
- Morodomi, T.; Isomoto, H.; Shirouzu, K.; Kakegawa, K.; Irie, K.; Morimatsu, M. An index for estimating the probability of lymph node metastasis in rectal cancers. Lymph node metastasis and the histopathology of actively invasive regions of cancer. Cancer 1989, 63, 539–543. [Google Scholar] [CrossRef]
- Karamitopoulou, E.; Zlobec, I.; Koelzer, V.; Kondi-Pafiti, A.; Patsouris, E.S.; Gennatas, K.; Lugli, A. Proposal for a 10-high-power-fields scoring method for the assessment of tumor budding in colorectal cancer. Mod. Pathol. 2012, 26, 295–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ueno, H.; Ishiguro, M.; Nakatani, E.; Ishikawa, T.; Uetake, H.; Matsuda, C.; Nakamoto, Y.; Kotake, M.; Kurachi, K.; Egawa, T.; et al. Prospective Multicenter Study on the Prognostic and Predictive Impact of Tumor Budding in Stage II Colon Cancer: Results from the SACURA Trial. J. Clin. Oncol. 2019, 37, 1886–1894. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, Y.; Ishii, G.; Kojima, M.; Yoh, K.; Otsuka, H.; Otaki, Y.; Aokage, K.; Yanagi, S.; Nagai, K.; Nishiwaki, Y.; et al. Histopathologic Features of the Tumor Budding in Adenocarcinoma of the Lung: Tumor Budding As an Index to Predict the Potential Aggressiveness. J. Thorac. Oncol. 2010, 5, 1361–1368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prezzano, J.C.; Scott, G.A.; Smith, F.L.; Mannava, K.A.; Ibrahim, S.F. Concordance of Squamous Cell Carcinoma Histologic Grading Among Dermatopathologists and Mohs Surgeons. Dermatol. Surg. 2021, 47, 1433–1437. [Google Scholar] [CrossRef]
- Allsbrook, W.C.; Mangold, K.; Johnson, M.H.; Lane, R.B.; Lane, C.G.; Amin, M.B.; Bostwick, D.G.; Humphrey, P.A.; Jones, E.C.; Reuter, V.E.; et al. Interobserver reproducibility of Gleason grading of prostatic carcinoma: Urologic pathologists. Hum. Pathol. 2001, 32, 74–80. [Google Scholar] [CrossRef] [Green Version]
- Dorofte, L.; Grélaud, D.; Fiorentino, M.; Giunchi, F.; Ricci, C.; Franceschini, T.; Riefolo, M.; Davidsson, S.; Carlsson, J.; Larsson, G.L.; et al. Low level of interobserver concordance in assessing histological subtype and tumor grade in patients with penile cancer may impair patient care. Virchows Arch. 2021, 480, 879–886. [Google Scholar] [CrossRef]
- Velazquez, E.F.; Amin, M.B.; Epstein, J.I.; Grignon, D.J.; Humphrey, P.A.; Pettaway, C.A.; Renshaw, A.A.; Reuter, V.E.; Srigley, J.R.; Zhou, M.; et al. Protocol for the Examination of Specimens From Patients With Carcinoma of the Penis, College of American Pathologists (CAP), October 2013. Available online: https://documents.cap.org/protocols/cp-penis-2013-v3200.pdf (accessed on 1 July 2015).
- Kakies, C.; López-Beltrán, A.; Comperat, E.; Erbersdobler, A.; Grobholz, R.; Hakenberg, O.W.; Hartmann, A.; Horn, L.-C.; Höhn, A.K.; Köllermann, J.; et al. Reproducibility of histopathologic tumor grading in penile cancer—results of a European project. Virchows Arch. 2014, 464, 453–461. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Histological Feature | Classification | Score & Grade |
|---|---|---|
| Tumor Budding * (TB) | No tumor budding | Score 1 |
| 1–5 tumor buds/HPF | Score 2 | |
| >5 tumor buds/HPF | Score 3 | |
| Cell Nest Size (CNS) | >15 cells per nest 5–15 cells per nest 2–4 cells per nest | Score 1 Score 2 Score 3 |
| single cell invasion | Score 4 | |
| Cellular Dissociation Grade (CDG) | Sum TB + CNS = 2–3 Sum TB + CNS = 4–5 | CDG-1 CDG-2 |
| Sum TB + CNS = 6–7 | CDG-3 |
| Statistical Test | WHO-G | CDG | TB | CNS |
|---|---|---|---|---|
| Asymptotic Significance-Pearson Chi-Square | 0.112 | <0.001–0.033 | <0.001–0.057 | 0.006–0.029 |
| Between-subjects effects-univariate analysis | 0.018 | <0.001–0.010 | <0.001–0.012 | 0.004–0.041 |
| Statistical Test | Cohens Kappa | Fleiss, Kappa Obs.1,2,3 | ||
|---|---|---|---|---|
| Obs.1 vs. Obs.2 | Obs.1 vs. Obs.3 | Obs.2 vs. Obs.3 | ||
| Value | 0.495 | 0.484 | 0.565 | 0.512 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Derani, H.; Becker, A.-S.; Hakenberg, O.; Erbersdobler, A. Evaluation of the Cellular Dissociation Grading, Based on Tumor Budding and Cell Nest Size, in Squamous Cell Carcinoma of the Penis. Cancers 2022, 14, 4949. https://doi.org/10.3390/cancers14194949
Derani H, Becker A-S, Hakenberg O, Erbersdobler A. Evaluation of the Cellular Dissociation Grading, Based on Tumor Budding and Cell Nest Size, in Squamous Cell Carcinoma of the Penis. Cancers. 2022; 14(19):4949. https://doi.org/10.3390/cancers14194949
Chicago/Turabian StyleDerani, Hayel, Anne-Sophie Becker, Oliver Hakenberg, and Andreas Erbersdobler. 2022. "Evaluation of the Cellular Dissociation Grading, Based on Tumor Budding and Cell Nest Size, in Squamous Cell Carcinoma of the Penis" Cancers 14, no. 19: 4949. https://doi.org/10.3390/cancers14194949