
Design and Validation of a Handheld Optical Polarization Imager for Preoperative Delineation of Basal Cell Carcinoma

 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
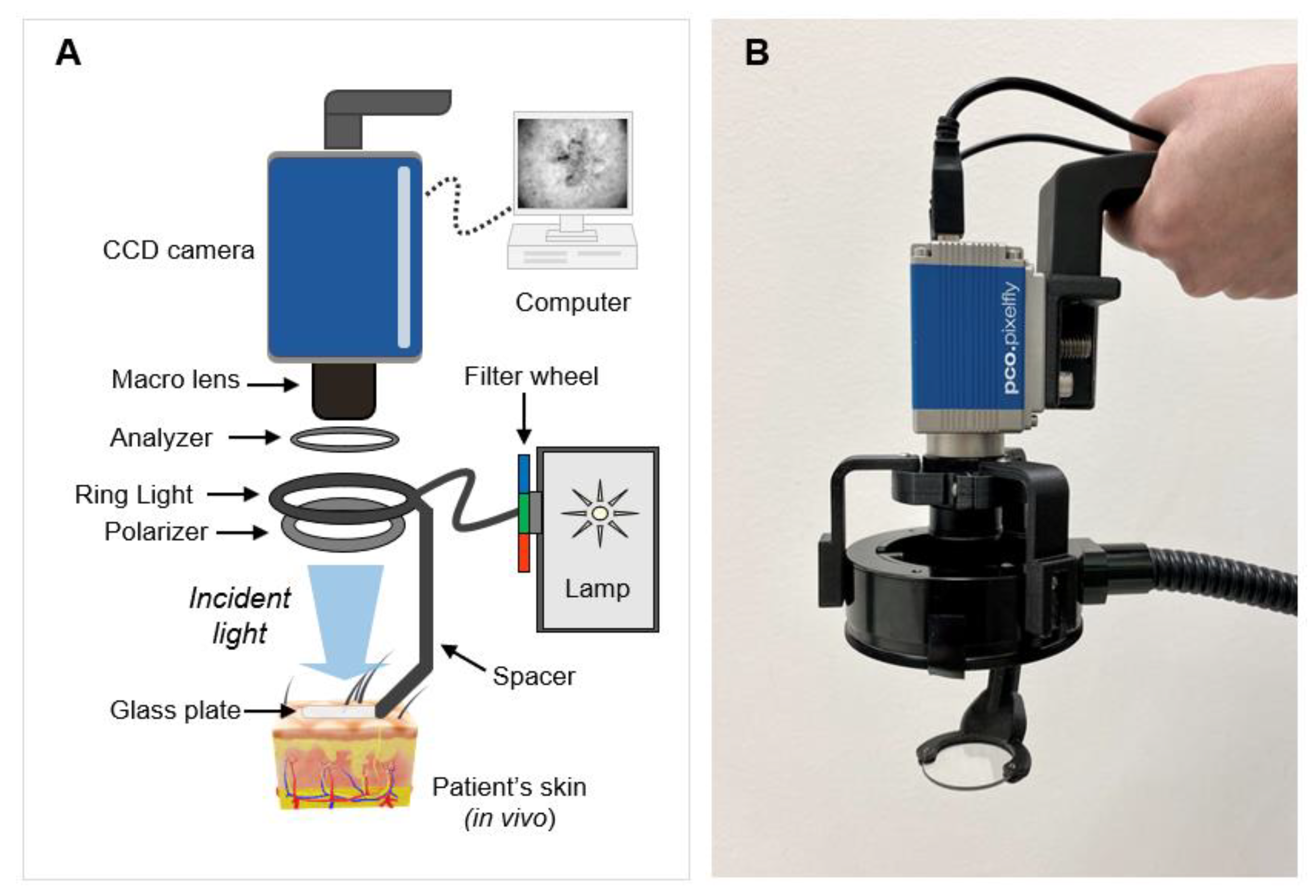
2.1. Handheld Optical Polarization Imager
2.2. Image Processing
2.3. OPI Clinical Evaluation
2.4. Data Analysis
3. Results
3.1. System Characterization
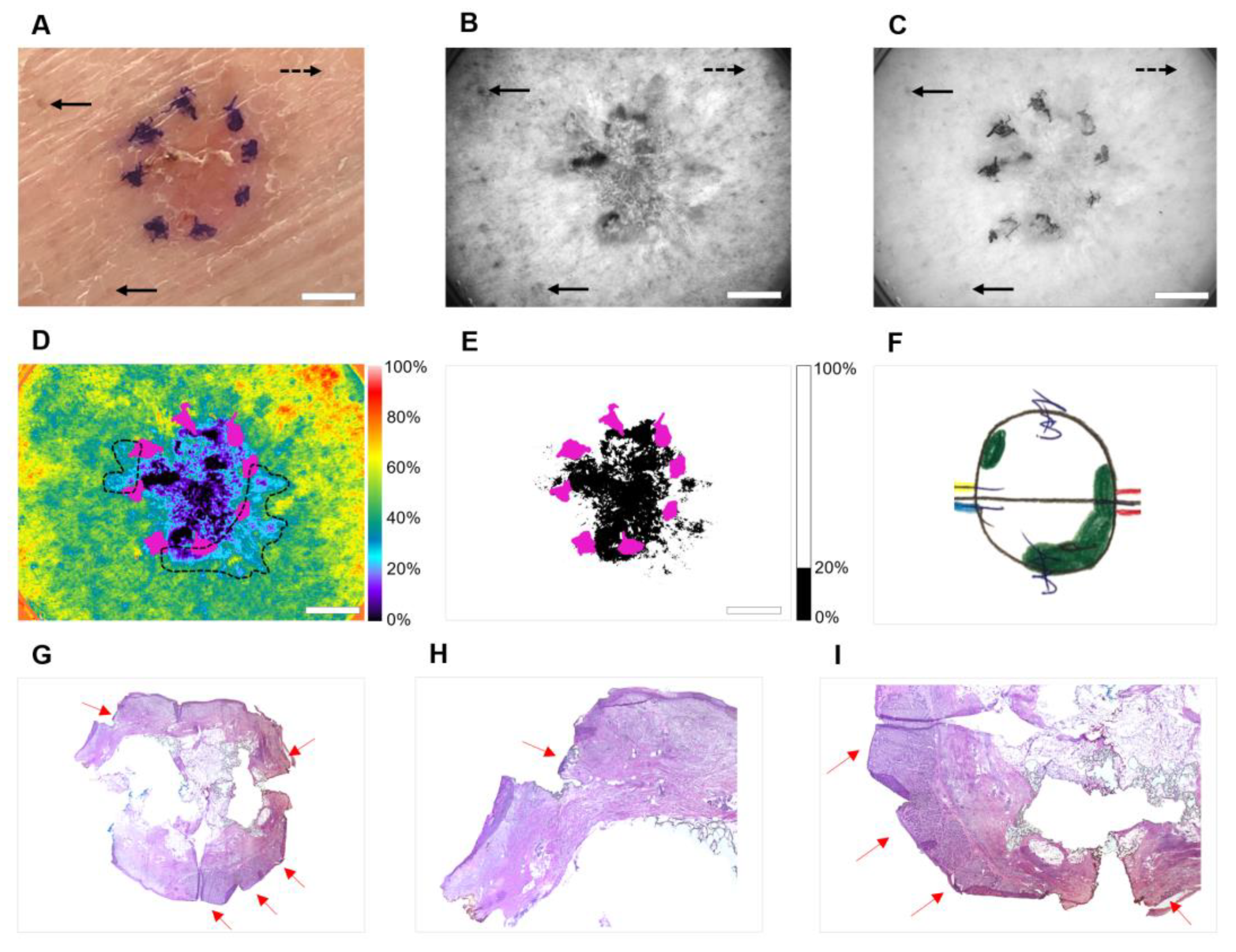
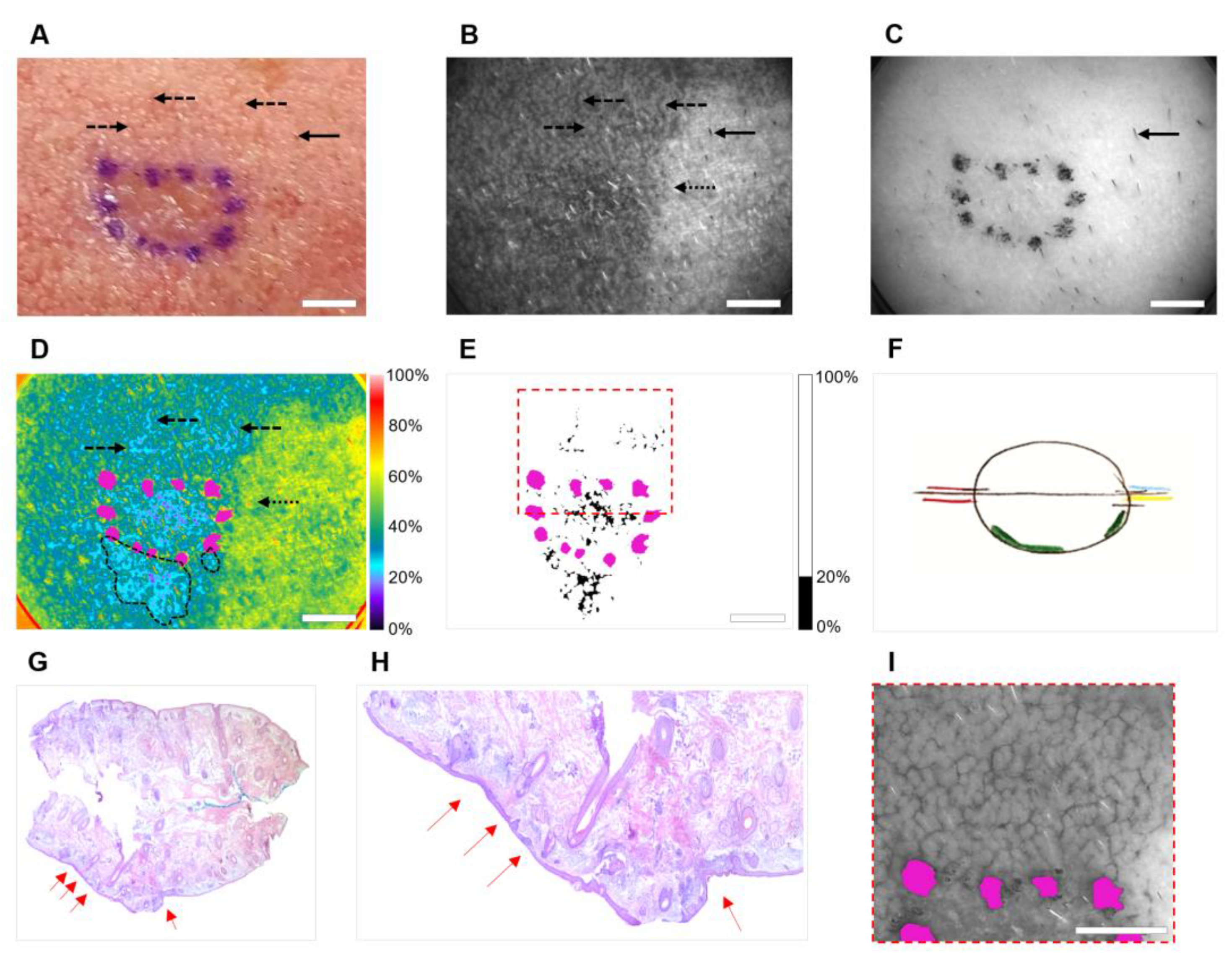
3.2. Clinical Validation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rogers, H.W.; Weinstock, M.A.; Feldman, S.R.; Coldiron, B.M. Incidence Estimate of Nonmelanoma Skin Cancer (Keratinocyte Carcinomas) in the US Population, 2012. JAMA Dermatol. 2015, 151, 1081–1086. [Google Scholar] [CrossRef] [PubMed]
- American Cancer Society. Available online: https://www.cancer.org/cancer/basal-and-squamous-cell-skin-cancer/about/key-statistics.html (accessed on 26 May 2022).
- Leiter, U.; Keim, U.; Garbe, C. Epidemiology of Skin Cancer: Update 2019. Adv. Exp. Med. Biol. 2020, 1268, 123–139. [Google Scholar] [CrossRef] [PubMed]
- Barea, A.; Martinucci, M.; Wertheim, D.; Morley, I.F.I.; Thomson, D.; Soldin, M.G. Five year basal cell carcinoma recurrence rates treated with curettage and cautery, a single centre retrospective cohort study. J. Plast. Reconstr. Aesthetic Surg. 2021, 74, 1931–1971. [Google Scholar] [CrossRef] [PubMed]
- Tchanque-Fossuo, C.N.; Eisen, D.B. A systematic review on the use of cryotherapy versus other treatments for basal cell carcinoma. Dermatol. Online J. 2018, 24, 13030. [Google Scholar] [CrossRef] [PubMed]
- Collier, N.J.; Rhodes, L.E. Photodynamic Therapy for Basal Cell Carcinoma: The Clinical Context for Future Research Priorities. Molecules 2020, 25, 5398. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.-C.; Fu, C.; Qin, L.; Zeng, X.-Y.; Liu, Q. Photodynamic therapy with methyl-5-aminolevulinate for basal cell carcinoma: A systematic review and meta-analysis. Photodiagnosis Photodyn. Ther. 2020, 29, 101667. [Google Scholar] [CrossRef] [PubMed]
- Eibenschutz, L.; Marenda, S.; Buccini, P.; De Simone, P.; Ferrari, A.; Mariani, G.; Silipo, V.; Catricalà, C. Giant and large basal cell carcinoma treated with topical photodynamic therapy. Eur. J. Dermatol. 2008, 18, 663–666. [Google Scholar] [CrossRef] [PubMed]
- Likhacheva, A.; Awan, M.; Barker, C.A.; Bhatnagar, A.; Bradfield, L.; Brady, M.S.; Buzurovic, I.; Geiger, J.L.; Parvathaneni, U.; Zaky, S.; et al. Definitive and Postoperative Radiation Therapy for Basal and Squamous Cell Cancers of the Skin: Executive Summary of an American Society for Radiation Oncology Clinical Practice Guideline. Pr. Radiat. Oncol. 2020, 10, 8–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navarrete-Dechent, C.; Cordova, M.; Liopyris, K.; Aleissa, S.; Rajadhyaksha, M.; Cohen, G.; Marghoob, A.A.; Rossi, A.M.; Barker, C.A. In vivo imaging characterization of basal cell carcinoma and cutaneous response to high-dose ionizing radiation therapy: A prospective study of reflectance confocal microscopy, dermoscopy, and ultrasonography. J. Am. Acad. Dermatol. 2020, 84, 1575–1584. [Google Scholar] [CrossRef]
- Tanese, K. Diagnosis and Management of Basal Cell Carcinoma. Curr. Treat. Options Oncol. 2019, 20, 13. [Google Scholar] [CrossRef] [PubMed]
- Bernardini, N.; Skroza, N.; Zuber, S.; Tolino, E.; Balduzzi, V.; Mambrin, A.; Marchesiello, A.; Anzalone, A.; Colapietra, D.; Proietti, I.; et al. Face and Scalp Basal Cell Carcinoma Treatment: A Review of the Literature. Acta Dermatovenerol. Croat. ADC 2019, 27, 22–27. [Google Scholar] [PubMed]
- Johnson, T.M.; Smith, N.R. Mohs Surgery versus Standard Local Excision for Basal Cell Carcinoma, Squamous Cell Carcinoma, and Melanoma Skin Cancer. Facial Plast. Surg. 2020, 36, 133–140, Erratum in Facial Plast Surg. 2020. [Google Scholar] [CrossRef] [PubMed]
- Weesie, F.; Naus, N.C.; Vasilic, D.; Hollestein, L.M.; Bos, R.R.V.D.; Wakkee, M. Recurrence of periocular basal cell carcinoma and squamous cell carcinoma after Mohs micrographic surgery: A retrospective cohort study. Br. J. Dermatol. 2018, 180, 1176–1182. [Google Scholar] [CrossRef] [PubMed]
- Luz, F.B.; Ferron, C.; Cardoso, G.P. Surgical treatment of basal cell carcinoma: An algorithm based on the literature. An. Bras. Dermatol. 2015, 90, 377–383. [Google Scholar] [CrossRef] [Green Version]
- Van Delft, L.; Nelemans, P.; Van Loo, E.; Hamid, M.A.; Kelleners-Smeets, N. The illusion of conventional histological resection margin control. Br. J. Dermatol. 2018, 180, 1240–1241. [Google Scholar] [CrossRef] [PubMed]
- Highsmith, J.T.; Highsmith, M.J.; Monheit, G.D. Histologic Accuracy of Mohs Micrographic Surgery. Dermatol. Surg. 2018, 44, 350–353. [Google Scholar] [CrossRef] [PubMed]
- Calvão, J.; Pinho, A.; Brinca, A.; Vieira, R. Clinicopathological factors influencing the number of stages of Mohs surgery for basal cell carcinoma. An. Bras. Dermatol. 2022, 97, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Gross, K.G.; Steinman, H.K.; Rapini, R.P. (Eds.) Mohs Surgery: Fundamentals and Techniques; Mosby: St. Louis, MO, USA, 1999. [Google Scholar]
- Weber, W.N. Cost analysis studies of Mohs micrographic surgery. J. Am. Acad. Dermatol. 1999, 41, 130. [Google Scholar] [CrossRef] [PubMed]
- Ravitskiy, L.; Brodland, D.G.; Zitelli, J.A. Cost Analysis: Mohs Micrographic Surgery. Dermatol. Surg. 2012, 38, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Conforti, C.; Giuffrida, R.; Zalaudek, I.; Guarneri, F.; Cannavò, S.P.; Pizzichetta, M.A.; Bonin, S.; Corneli, P.; Bussani, R.; Bazzacco, G.; et al. Dermoscopic Findings in the Presurgical Evaluation of Basal Cell Carcinoma. A Prospective Study. Dermatol. Surg. 2020, 47, e37–e41. [Google Scholar] [CrossRef] [PubMed]
- Shin, K.; Kim, H.-J.; Ko, H.-C.; Kim, B.-S.; Kim, M.-B.; Kim, H.-S. Dermoscopy-guided Mohs micrographic surgery in post-laser basal cell carcinomas: Is dermoscopy helpful for demarcation of the surgical margin? J. Dermatol. Treat. 2021, 33, 433–436. [Google Scholar] [CrossRef] [PubMed]
- Sahu, A.; Yélamos, O.; Iftimia, N.; Cordova, M.; Alessi-Fox, C.; Gill, M.; Maguluri, G.; Dusza, S.W.; Navarrete-Dechent, C.; Gonzalez, S.; et al. Evaluation of a Combined Reflectance Confocal Microscopy–Optical Coherence Tomography Device for Detection and Depth Assessment of Basal Cell Carcinoma. JAMA Dermatol. 2018, 154, 1175–1183. [Google Scholar] [CrossRef] [PubMed]
- Aleissa, S.; Navarrete-Dechent, C.; Cordova, M.; Sahu, A.; Dusza, S.W.; Phillips, W.; Rossi, A.; Lee, E.; Nehal, K.S. Presurgical evaluation of basal cell carcinoma using combined reflectance confocal microscopy–optical coherence tomography: A prospective study. J. Am. Acad. Dermatol. 2019, 82, 962–968. [Google Scholar] [CrossRef] [PubMed]
- Iftimia, N.; Sahu, A.; Cordova, M.; Maguluri, G.; Gill, M.; Alessi-Fox, C.; Gonzalez, S.; Navarrete-Dechent, C.; Marghoob, A.; Chen, C.-S.J.; et al. The potential utility of integrated reflectance confocal microscopy-optical coherence tomography for guiding triage and therapy of basal cell carcinomas. J. Cancer 2020, 11, 6019–6024. [Google Scholar] [CrossRef] [PubMed]
- Epstein, E. How accurate is the visual assessment of basal carcinoma margins? Br. J. Dermatol. 1973, 89, 37–43. [Google Scholar] [CrossRef] [PubMed]
- ANSI Z136.3-2018; American National Standard for the Safe Use of Lasers in Health Care. American National Standards Institute: Orlando, FL, USA; Laser Institute of America: Orlando, FL, USA, 2018.
- Rohani, P.; Yaroslavsky, A.N.; Feng, X.; Jermain, P.; Shaath, T.; Neel, V.A. Collagen disruption as a marker for basal cell carcinoma in presurgical margin detection. Lasers Surg. Med. 2018, 50, 902–907. [Google Scholar] [CrossRef] [PubMed]
- Yaroslavsky, A.N.; Feng, X.; Yu, S.H.; Jermain, P.R.; Iorizzo, T.W.; Neel, V.A. Dual-Wavelength Optical Polarization Imaging for Detecting Skin Cancer Margins. J. Investig. Dermatol. 2020, 140, 1994–2000.e1. [Google Scholar] [CrossRef] [PubMed]
- Momeni, I.; Asilian, A. Comparison between examination with naked eye, curretage and dermoscopy in determining tumor extension before Mohs micrographic surgery. Adv. Biomed. Res. 2013, 2, 2. [Google Scholar] [CrossRef]
- Suzuki, H.S.; Serafini, S.Z.; Sato, M.S. Utility of dermoscopy for demarcation of surgical margins in Mohs micrographic surgery. An. Bras. Dermatol. 2014, 89, 38–43. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Specifications | Handheld OPI | Previous System | |
|---|---|---|---|
| Weight | 1.21 lbs. | 2.51 lbs. | |
| Field of View | 3.2 × 2.3 cm2 | 2.2 × 1.6 cm2 | |
| Lateral Resolution | 12.4 µm | 12.4 µm | |
| Image Acquisition Time | 440 nm | 50 ms | 620 ms |
| 570 nm | 41 ms | n/a | |
| 640 nm | 5 ms | 64 ms | |
| Power Density | 440 nm | 0.2 mW/cm2 | 0.2 mW/cm2 |
| 570 nm | 0.4 mW/cm2 | n/a | |
| 640 nm | 0.5 mW/cm2 | 0.6 mW/cm2 | |
| Data Processing | Automated | Manual | |
| Subject No. | Sex | Age | Diagnosis | Tumor Site | Tumor Size [cm] | No. of Mohs Stages | OPI Classification | OPI/Histopathology Correlation |
|---|---|---|---|---|---|---|---|---|
| 1 | M | 76 | BCC, nodular | Glabella | 0.4 × 0.4 | 1 | TN | + |
| 2 | M | 71 | BCC, nodular | R forearm | 1.7 × 1.2 | 1 | TN | + |
| 3 | M | 77 | BCC, nodular | R cheek | 1.1 × 0.7 | 1 | TN | + |
| 4 | M | 67 | BCC, nodular | L temple | 1.0 × 0.8 | 1 | TN | + |
| 5 | F | 81 | BCC, nodular | R nasal | 1.1 × 0.6 | 2 | TP | + |
| 6 | M | 55 | BCC, superficial | L cheek | 1.0 × 0.5 | 2 | FP * | +/− |
| 7 | M | 69 | BCC, nodular/superficial | R jaw | 1.1 × 0.9 | 1 | TN | + |
| 8 | F | 72 | BCC, nodular/superficial | R eyebrow | 0.6 × 0.6 | 2 | TP | + |
| 9 | F | 83 | BCC, nodular with squamous differentiation | R tibia | 1.7 × 1.1 | 2 | TP | + |
| 10 | M | 60 | BCC, micronodular/cystic with ductal differentiation | R shoulder | 2.5 × 2.0 | 1 | TN | + |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jermain, P.R.; Iorizzo, T.W.; Maloney, M.; Mahmoud, B.; Yaroslavsky, A.N. Design and Validation of a Handheld Optical Polarization Imager for Preoperative Delineation of Basal Cell Carcinoma. Cancers 2022, 14, 4049. https://doi.org/10.3390/cancers14164049
Jermain PR, Iorizzo TW, Maloney M, Mahmoud B, Yaroslavsky AN. Design and Validation of a Handheld Optical Polarization Imager for Preoperative Delineation of Basal Cell Carcinoma. Cancers. 2022; 14(16):4049. https://doi.org/10.3390/cancers14164049
Chicago/Turabian StyleJermain, Peter R., Tyler W. Iorizzo, Mary Maloney, Bassel Mahmoud, and Anna N. Yaroslavsky. 2022. "Design and Validation of a Handheld Optical Polarization Imager for Preoperative Delineation of Basal Cell Carcinoma" Cancers 14, no. 16: 4049. https://doi.org/10.3390/cancers14164049