
Efficient Prediction of Ki-67 Proliferation Index in Meningiomas on MRI: From Traditional Radiological Findings to a Machine Learning Approach


Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods and Materials
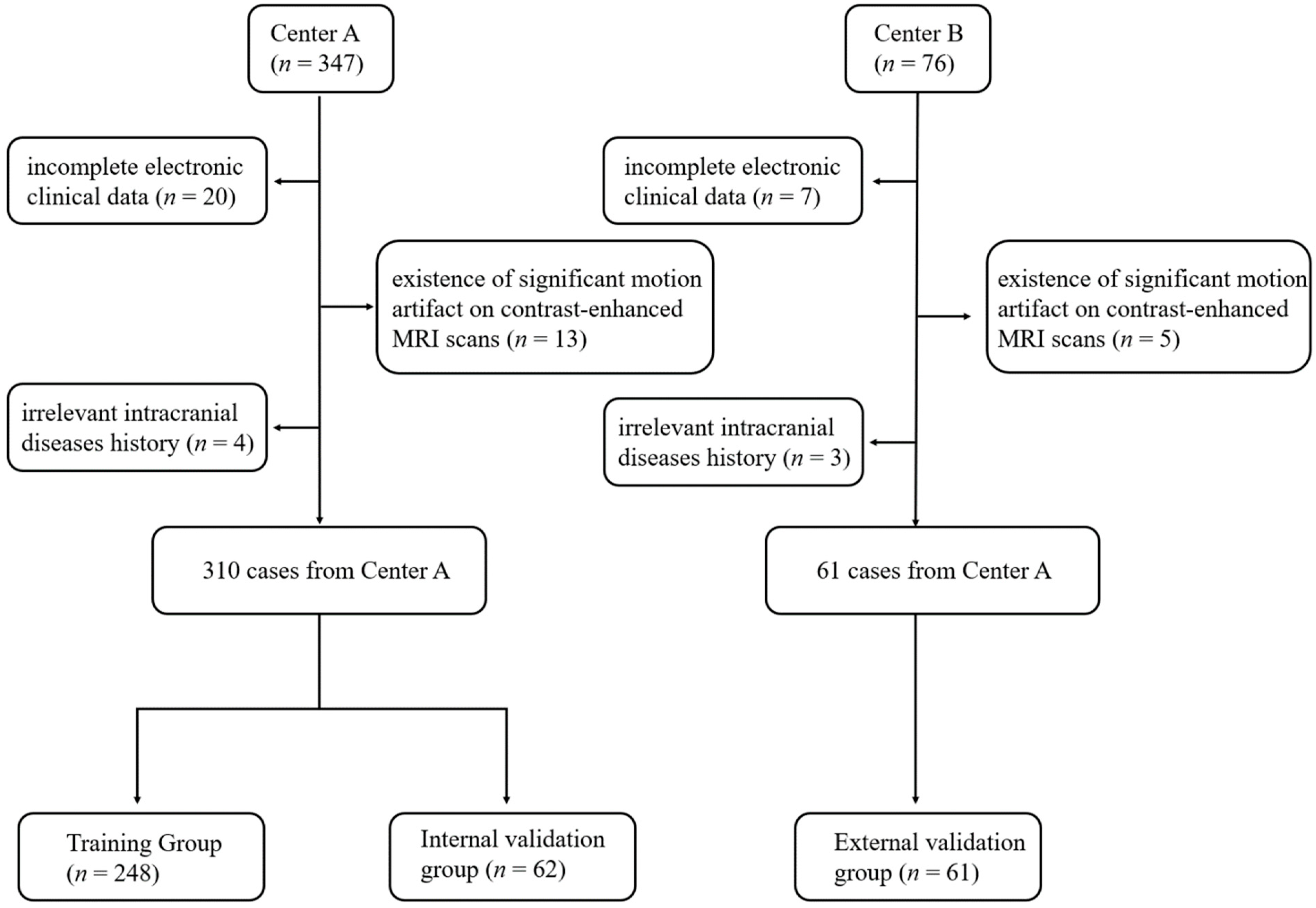
2.1. Patient Selection
2.2. MR Scan Protocols
2.3. Image Preprocessing and Tumor Segmentation
2.4. Collection of Clinical Features, Radiological Features, and Radiomic Features
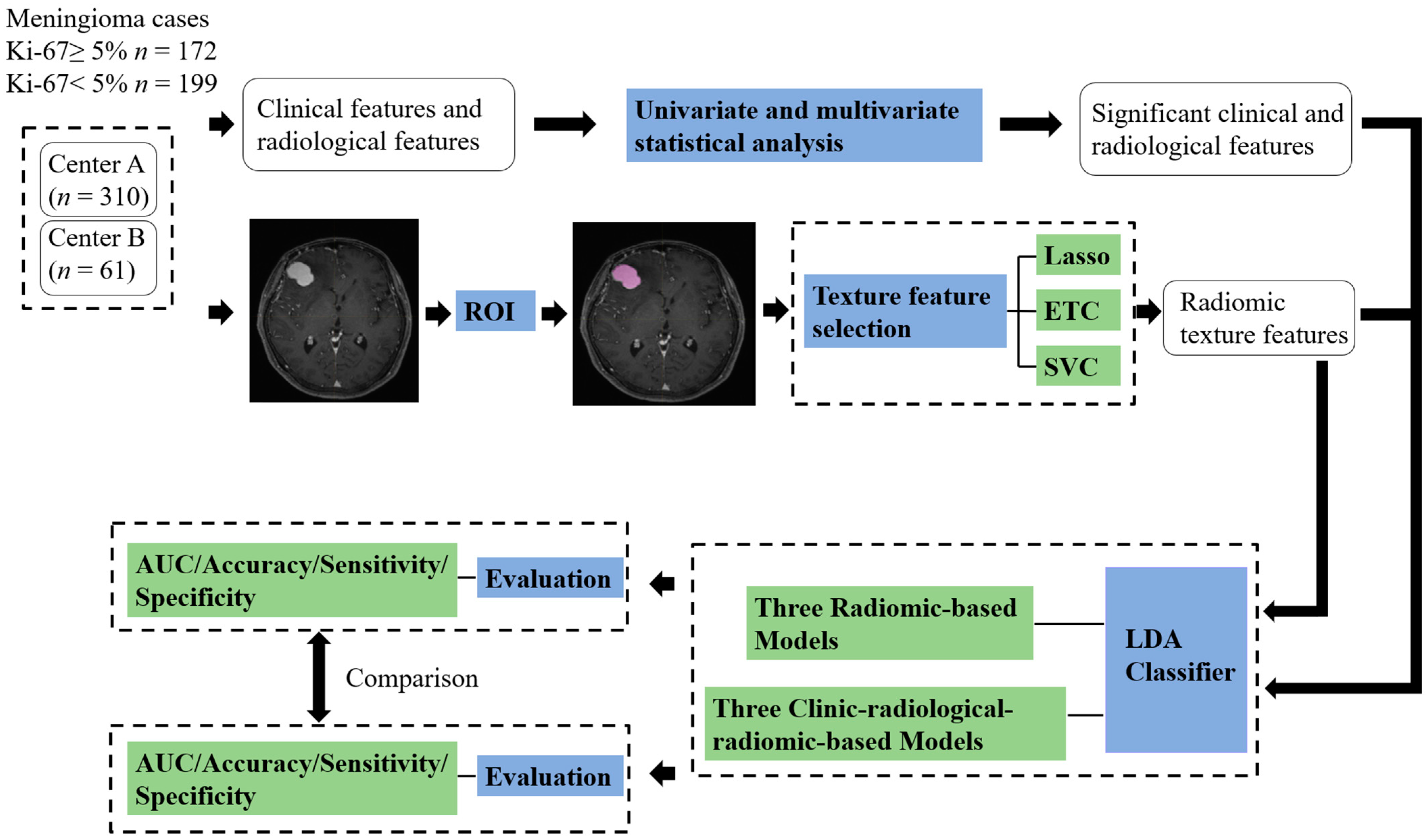
2.5. Feature Selection and Machine Learning Model Establishment
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
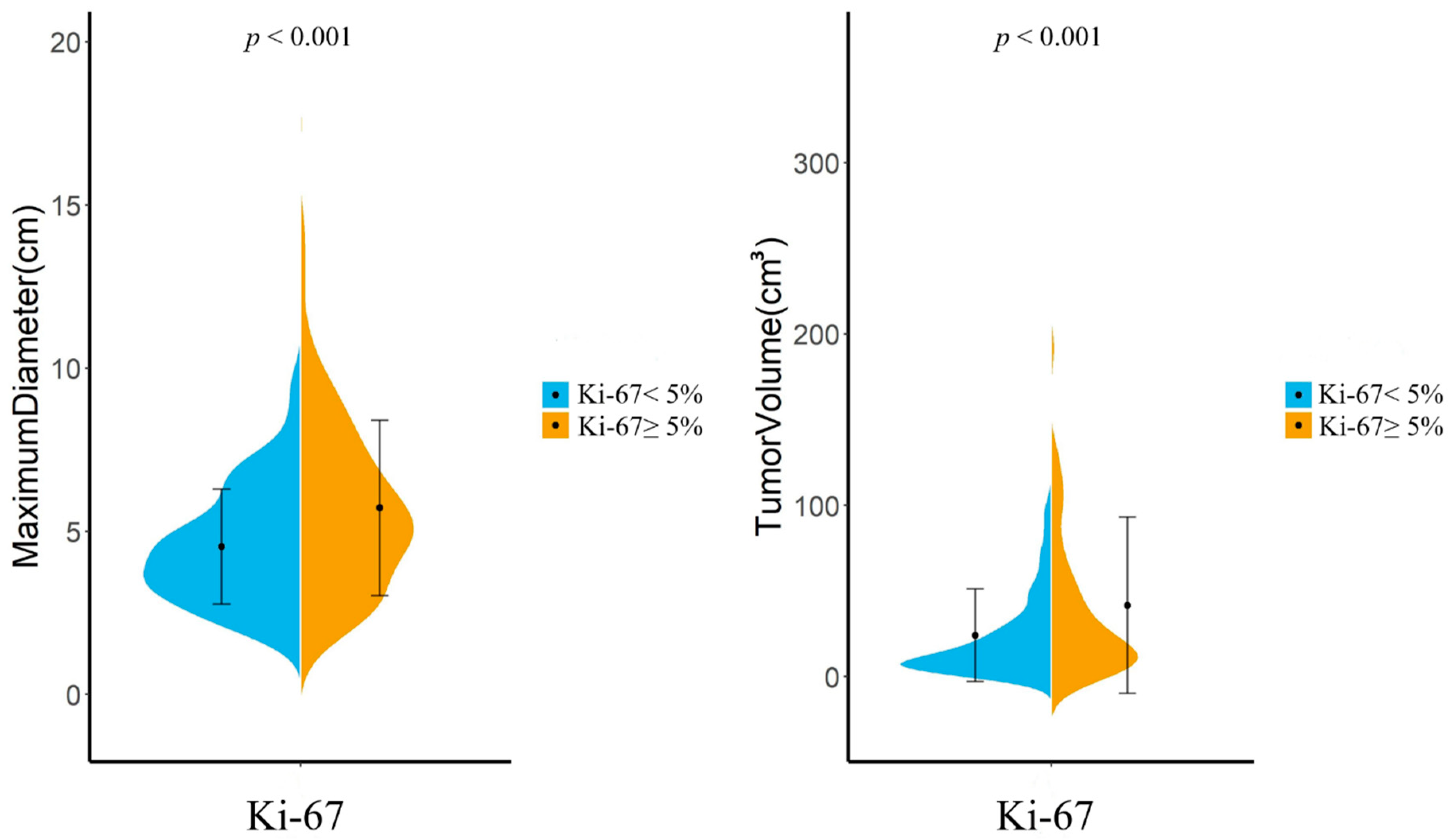
3.2. Morphologic Analysis and Radiological Findings
3.3. Clinical and Radiological Features Related to Ki-67 Index
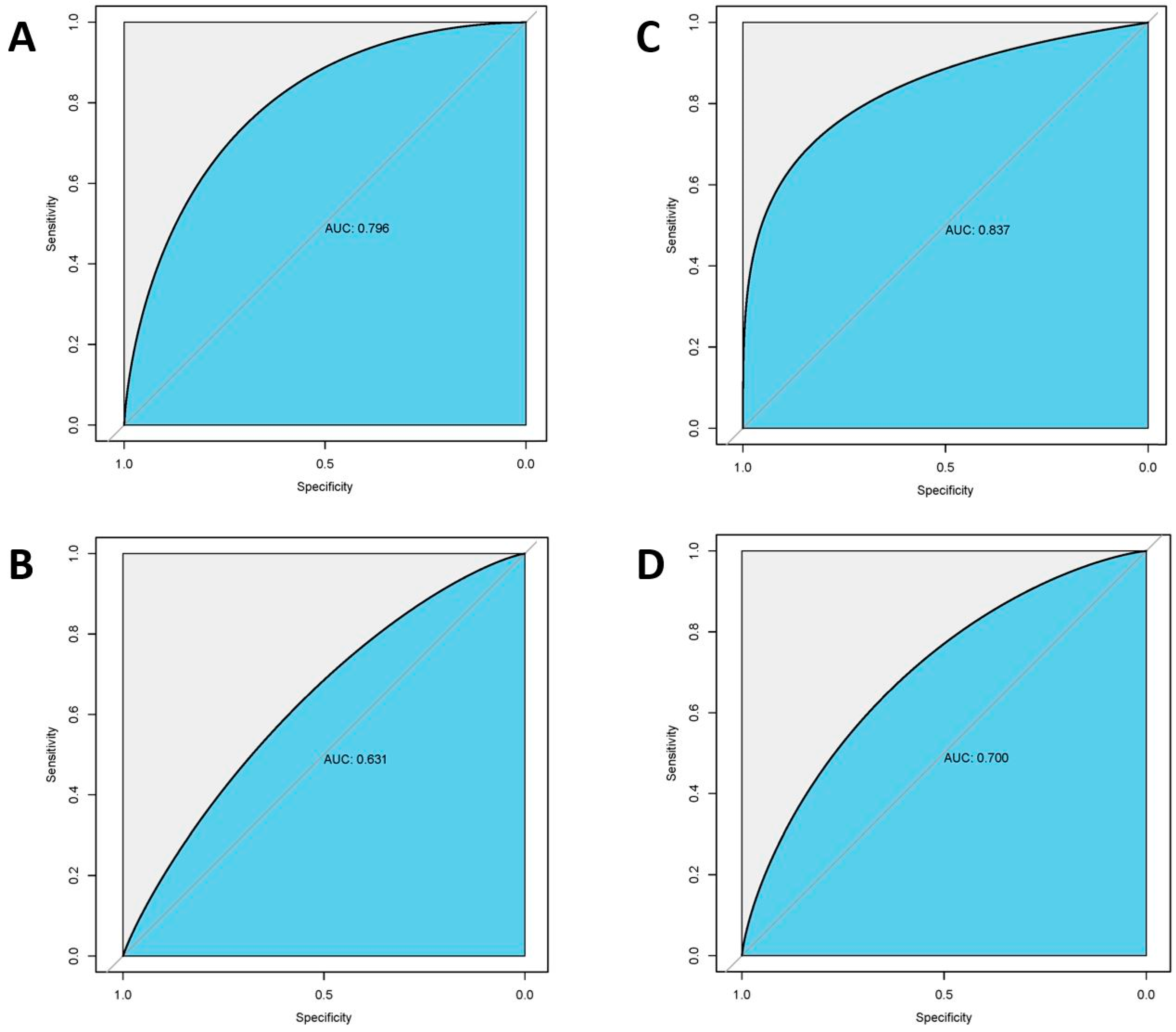
3.4. Radiomic Feature Selection and Model Performances
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- NCCN Clinical Practice Guidelines in Oncology- Central Nervous System Cancers, Version 3. 2020. Available online: http://www.nccn.org (accessed on 15 October 2021).
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro-oncology 2021, 23, 1231–1251. [Google Scholar] [CrossRef]
- Ostrom, Q.T.; Gittleman, H.; Truitt, G.; Boscia, A.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2011–2015. Neuro-oncology 2018, 20, iv1–iv86. [Google Scholar] [CrossRef] [Green Version]
- Goldbrunner, R.; Stavrinou, P.; Jenkinson, M.D.; Sahm, F.; Mawrin, C.; Weber, D.C.; Preusser, M.; Minniti, G.; Lund-Johansen, M.; Lefranc, F.; et al. EANO guideline on the diagnosis and management of meningiomas. Neuro-oncology 2021, 23, 1821–1834. [Google Scholar] [CrossRef]
- van Velthuysen, M.L.; Groen, E.J.; van der Noort, V.; van de Pol, A.; Tesselaar, M.E.; Korse, C.M. Grading of neuroendocrine neoplasms: Mitoses and Ki-67 are both essential. Neuroendocrinology 2014, 100, 221–227. [Google Scholar] [CrossRef]
- Pouget, C.; Hergalant, S.; Lardenois, E.; Lacomme, S.; Houlgatte, R.; Carpentier, C.; Dehais, C.; Rech, F.; Taillandier, L.; Sanson, M.; et al. Ki-67 and MCM6 labeling indices are correlated with overall survival in anaplastic oligodendroglioma, IDH1-mutant and 1p/19q-codeleted: A multicenter study from the French POLA network. Brain Pathol. 2020, 30, 465–478. [Google Scholar] [CrossRef]
- Masuda, D.; Masuda, R.; Matsuzaki, T.; Imamura, N.; Aruga, N.; Tanaka, M.; Inokuchi, S.; Kijima, H.; Iwazaki, M. Ki-67 labeling index affects tumor infiltration patterns of lung squamous cell carcinoma. Mol. Med. Rep. 2015, 12, 7303–7309. [Google Scholar] [CrossRef] [Green Version]
- Gerdes, J.; Schwab, U.; Lemke, H.; Stein, H. Production of a mouse monoclonal antibody reactive with a human nuclear antigen associated with cell proliferation. Int. J. Cancer 1983, 31, 13–20. [Google Scholar] [CrossRef]
- van Alkemade, H.; de Leau, M.; Dieleman, E.M.; Kardaun, J.W.; van Os, R.; Vandertop, W.P.; van Furth, W.R.; Stalpers, L.J. Impaired survival and long-term neurological problems in benign meningioma. Neuro-oncology 2012, 14, 658–666. [Google Scholar] [CrossRef]
- Haddad, A.F.; Young, J.S.; Kanungo, I.; Sudhir, S.; Chen, J.S.; Raleigh, D.R.; Magill, S.T.; McDermott, M.W.; Aghi, M.K. WHO Grade I Meningioma Recurrence: Identifying High Risk Patients Using Histopathological Features and the MIB-1 Index. Front. Oncol. 2020, 10, 1522. [Google Scholar] [CrossRef]
- Winther, T.L.; Torp, S.H. Significance of the Extent of Resection in Modern Neurosurgical Practice of World Health Organization Grade I Meningiomas. World Neurosurg. 2017, 99, 104–110. [Google Scholar] [CrossRef]
- Nowak-Choi, K.; Palmer, J.D.; Casey, J.; Chitale, A.; Kalchman, I.; Buss, E.; Keith, S.W.; Hegarty, S.E.; Curtis, M.; Solomides, C.; et al. Resected WHO grade I meningioma and predictors of local control. J. Neuro-Oncol. 2021, 152, 145–151. [Google Scholar] [CrossRef]
- Liu, N.; Song, S.Y.; Jiang, J.B.; Wang, T.J.; Yan, C.X. The prognostic role of Ki-67/MIB-1 in meningioma: A systematic review with meta-analysis. Medicine 2020, 99, e18644. [Google Scholar] [CrossRef]
- Huang, R.Y.; Bi, W.L.; Griffith, B.; Kaufmann, T.J.; la Fougère, C.; Schmidt, N.O.; Tonn, J.C.; Vogelbaum, M.A.; Wen, P.Y.; Aldape, K.; et al. Imaging and diagnostic advances for intracranial meningiomas. Neuro-oncology 2019, 21, i44–i61. [Google Scholar] [CrossRef]
- Kim, B.W.; Kim, M.S.; Kim, S.W.; Chang, C.H.; Kim, O.L. Peritumoral brain edema in meningiomas: Correlation of radiologic and pathologic features. J. Korean Neurosurg. Soc. 2011, 49, 26–30. [Google Scholar] [CrossRef]
- Villanueva-Meyer, J.E.; Chang, P.; Lupo, J.M.; Hess, C.P.; Flanders, A.E.; Kohli, M. Machine Learning in Neurooncology Imaging: From Study Request to Diagnosis and Treatment. Am. J. Roentgenol. 2019, 212, 52–56. [Google Scholar] [CrossRef]
- Rudie, J.D.; Rauschecker, A.M.; Bryan, R.N.; Davatzikos, C.; Mohan, S. Emerging Applications of Artificial Intelligence in Neuro-Oncology. Radiology 2019, 290, 607–618. [Google Scholar] [CrossRef]
- Machine Learning Improves Diagnosis of CNS Cancers. Cancer Discov. 2018, 8, 523–524. [CrossRef] [Green Version]
- Jian, A.; Jang, K.; Manuguerra, M.; Liu, S.; Magnussen, J.; Di Ieva, A. Machine Learning for the Prediction of Molecular Markers in Glioma on Magnetic Resonance Imaging: A Systematic Review and Meta-Analysis. Neurosurgery 2021, 89, 31–44. [Google Scholar] [CrossRef]
- Khanna, O.; Fathi Kazerooni, A.; Farrell, C.J.; Baldassari, M.P.; Alexander, T.D.; Karsy, M.; Greenberger, B.A.; Garcia, J.A.; Sako, C.; Evans, J.J.; et al. Machine Learning Using Multiparametric Magnetic Resonance Imaging Radiomic Feature Analysis to Predict Ki-67 in World Health Organization Grade I Meningiomas. Neurosurgery 2021, 89, 928–936. [Google Scholar] [CrossRef]
- Maillo, A.; Orfao, A.; Espinosa, A.B.; Sayagués, J.M.; Merino, M.; Sousa, P.; Lara, M.; Tabernero, M.D. Early recurrences in histologically benign/grade I meningiomas are associated with large tumors and coexistence of monosomy 14 and del(1p36) in the ancestral tumor cell clone. Neuro-oncology 2007, 9, 438–446. [Google Scholar] [CrossRef]
- Sun, S.Q.; Kim, A.H.; Cai, C.; Murphy, R.K.; DeWees, T.; Sylvester, P.; Dacey, R.G.; Grubb, R.L.; Rich, K.M.; Zipfel, G.J.; et al. Management of atypical cranial meningiomas, part 1: Predictors of recurrence and the role of adjuvant radiation after gross total resection. Neurosurgery 2014, 75, 347–354; discussion 345–354; quiz 355. [Google Scholar] [CrossRef] [Green Version]
- Barresi, V.; Lionti, S.; Caliri, S.; Caffo, M. Histopathological features to define atypical meningioma: What does really matter for prognosis? Brain Tumor Pathol. 2018, 35, 168–180. [Google Scholar] [CrossRef]
- Smirniotopoulos, J.G.; Murphy, F.M.; Rushing, E.J.; Rees, J.H.; Schroeder, J.W. Patterns of contrast enhancement in the brain and meninges. Radiogr. A Rev. Publ. Radiol. Soc. North Am. Inc. 2007, 27, 525–551. [Google Scholar] [CrossRef]
- Phuttharak, W.; Boonrod, A.; Thammaroj, J.; Kitkhuandee, A.; Waraasawapati, S. Preoperative MRI evaluation of meningioma consistency: A focus on detailed architectures. Clin. Neurol. Neurosurg. 2018, 169, 178–184. [Google Scholar] [CrossRef]
- Zhang, B.; Tian, J.; Dong, D.; Gu, D.; Dong, Y.; Zhang, L.; Lian, Z.; Liu, J.; Luo, X.; Pei, S.; et al. Radiomics Features of Multiparametric MRI as Novel Prognostic Factors in Advanced Nasopharyngeal Carcinoma. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2017, 23, 4259–4269. [Google Scholar] [CrossRef] [Green Version]
- Tang, T.Y.; Li, X.; Zhang, Q.; Guo, C.X.; Zhang, X.Z.; Lao, M.Y.; Shen, Y.N.; Xiao, W.B.; Ying, S.H.; Sun, K.; et al. Development of a Novel Multiparametric MRI Radiomic Nomogram for Preoperative Evaluation of Early Recurrence in Resectable Pancreatic Cancer. J. Magn. Reson. Imaging 2020, 52, 231–245. [Google Scholar] [CrossRef]
- Cui, E.; Li, Z.; Ma, C.; Li, Q.; Lei, Y.; Lan, Y.; Yu, J.; Zhou, Z.; Li, R.; Long, W.; et al. Predicting the ISUP grade of clear cell renal cell carcinoma with multiparametric MR and multiphase CT radiomics. Eur. Radiol. 2020, 30, 2912–2921. [Google Scholar] [CrossRef]
- Gitto, S.; Cuocolo, R.; Annovazzi, A.; Anelli, V.; Acquasanta, M.; Cincotta, A.; Albano, D.; Chianca, V.; Ferraresi, V.; Messina, C.; et al. CT radiomics-based machine learning classification of atypical cartilaginous tumours and appendicular chondrosarcomas. EBioMedicine 2021, 68, 103407. [Google Scholar] [CrossRef]
- Romeo, V.; Cuocolo, R.; Apolito, R.; Stanzione, A.; Ventimiglia, A.; Vitale, A.; Verde, F.; Accurso, A.; Amitrano, M.; Insabato, L.; et al. Clinical value of radiomics and machine learning in breast ultrasound: A multicenter study for differential diagnosis of benign and malignant lesions. Eur. Radiol. 2021, 31, 9511–9519. [Google Scholar] [CrossRef]
- Fiz, F.; Masci, C.; Costa, G.; Sollini, M.; Chiti, A.; Ieva, F.; Torzilli, G.; Viganò, L. PET/CT-based radiomics of mass-forming intrahepatic cholangiocarcinoma improves prediction of pathology data and survival. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 3387–3400. [Google Scholar] [CrossRef]
- Zhang, M.Z.; Ou-Yang, H.Q.; Liu, J.F.; Jin, D.; Wang, C.J.; Ni, M.; Liu, X.G.; Lang, N.; Jiang, L.; Yuan, H.S. Predicting postoperative recovery in cervical spondylotic myelopathy: Construction and interpretation of T(2)(*)-weighted radiomic-based extra trees models. Eur. Radiol. 2022, 32, 3565–3575. [Google Scholar] [CrossRef]
- Bos, P.; van den Brekel, M.W.M.; Gouw, Z.A.R.; Al-Mamgani, A.; Waktola, S.; Aerts, H.; Beets-Tan, R.G.H.; Castelijns, J.A.; Jasperse, B. Clinical variables and magnetic resonance imaging-based radiomics predict human papillomavirus status of oropharyngeal cancer. Head Neck 2021, 43, 485–495. [Google Scholar] [CrossRef]
- Morin, O.; Chen, W.C.; Nassiri, F.; Susko, M.; Magill, S.T.; Vasudevan, H.N.; Wu, A.; Vallières, M.; Gennatas, E.D.; Valdes, G.; et al. Integrated models incorporating radiologic and radiomic features predict meningioma grade, local failure, and overall survival. Neuro-Oncol. Adv. 2019, 1, vdz011. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Center A (n = 310) | Center B (n = 61) | Total | p Value | |||
|---|---|---|---|---|---|---|---|
| Ki-67 ≥ 5% (n = 158) | Ki-67 < 5% (n = 152) | Ki-67 ≥ 5% (n = 14) | Ki-67 < 5% (n = 47) | Ki-67 ≥ 5% (n = 172) | Ki-67 < 5% (n = 199) | ||
| Age | |||||||
| mean | 51.7 ± 14.8 | 56.0 ± 10.0 | 51.7 ± 14.2 | 55.0 ± 12.1 | 51.7 ± 14.5 | 55.2 ± 11.7 | 0.546 |
| range | 5−82 | 39−76 | 9−77 | 31−77 | 5−82 | 31−77 | |
| Gender | |||||||
| male | 53 (33.6%) | 42 (27.6%) | 5 (35.7%) | 13 (27.7%) | 58 (33.7%) | 55 (27.6%) | 0.215 |
| Female | 105 (66.4%) | 110 (72.4%) | 9 (64.3%) | 34 (72.3%) | 114 (66.3%) | 144 (72.4%) | |
| Location | |||||||
| Cerebral convexity | 90 (57.0%) | 78 (51.3%) | 5 (35.7%) | 25 (53.2%) | 95 (55.2%) | 103 (51.8%) | 0.433 |
| Falx | 23 (14.5%) | 32 (21.1%) | 2 (14.3%) | 7 (14.9%) | 25 (14.5%) | 39 (19.6%) | |
| Skull base | 45 (28.5%) | 42 (27.6%) | 7 (50%) | 15 (31.9%) | 52 (30.3%) | 57 (28.6%) | |
| Laterality | |||||||
| Left | 70 (44.3%) | 69 (45.4%) | 7 (50%) | 21 (44.7%) | 77 (44.8%) | 90 (45.2%) | 0.715 |
| Right | 71 (44.9%) | 71 (46.7%) | 6 (42.9%) | 22 (46.8%) | 77 (44.8%) | 93 (46.7%) | |
| Midline | 17 (10.8%) | 12 (7.9%) | 1 (7.1%) | 4 (8.5%) | 18 (10.4%) | 16 (8.1%) | |
| WHO grade | |||||||
| Low grade | |||||||
| WHO I | 94 (59.5%) | 133 (87.5%) | 8 (57.1%) | 42 (89.4%) | 102 (59.3%) | 175 (87.9%) | <0.001 |
| High grade | |||||||
| WHO II | 57 (36.1%) | 19 (12.5%) | 5 (35.7%) | 5 (10.6%) | 62 (36.0%) | 24 (12.1%) | <0.001 |
| WHO III | 7 (4.4%) | 0 (0%) | 1 (7.2%) | 0 (0%) | 8 (4.7%) | 0 (0%) | <0.001 |
| Peritumoral edema | 125 (79.1%) | 110 (72.4%) | 10 (71.4%) | 30 (63.8%) | 135 (78.5%) | 140 (70.4%) | 0.076 |
| CSF space surrounding tumor | 92 (58.2%) | 78 (51.3%) | 8 (57.1%) | 20 (42.6%) | 100 (58.1%) | 98 (49.2%) | 0.095 |
| Absent capsular enhancement | 39 (24.7%) | 25 (16.4%) | 4 (28.6%) | 9 (19.1%) | 43 (25.0%) | 34 (17.1%) | 0.072 |
| Heterogeneous enhancement | 93 (58.9%) | 75 (49.3%) | 9 (64.3%) | 21 (44.7%) | 102 (59.3%) | 96 (48.2%) | 0.037 |
| Intratumoral Necrosis | 48 (30.4%) | 35 (23%) | 5 (35.7%) | 10 (21.3%) | 53 (30.8%) | 45 (22.6%) | 0.078 |
| Maximum diameter | 5.76 ± 2.56 | 4.53 ± 1.63 | 5.16 ± 3.74 | 4.52 ± 2.13 | 5.72 ± 2.70 | 4.53 ± 1.76 | <0.001 |
| Tumor volume | 43.1 ± 52.4 | 23.0 ± 26.5 | 24.8 ± 33.5 | 27.4 ± 28.6 | 41.57 ± 51.32 | 24.03 ± 27.00 | <0.001 |
| Variables (Ki-67 ≥ 5% vs. Ki-67 < 5%) | Odds Ratio, 95% CI | p Value | |
|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | ||
| Peritumoral edema | 1.538 (0.957–2.470) | 0.076 | 0.279 |
| CSF space surrounding tumor | 1.403 (0.930–2.116) | 0.095 | 0.216 |
| Absent capsular enhancement | 1.618 (0.976–2.681) | 0.072 | 0.602 |
| Heterogeneous enhancement | 1.536 (1.035–2.361) | 0.037 | 0.320 |
| Intratumoral necrosis | 1.524 (0.959–2.424) | 0.078 | 0.032 |
| Tumor volume (cm3) | 1.013 (1.006–1.019) | <0.001 | 0.672 |
| Maximum diameter (cm) | 1.025 (1.014–1.035) | <0.001 | <0.001 |
| Radiomic Features | Lasso (n = 14) | SVC (n = 11) | ETC (n = 8) |
|---|---|---|---|
| First-Order Features | 3 | 3 | 0 |
| Shape Features (2D) | 1 | 1 | 0 |
| Shape Features (3D) | 0 | 0 | 0 |
| GLCM Features | 3 | 5 | 1 |
| GLSZM Features | 5 | 1 | 4 |
| GLRLM Features | 0 | 0 | 1 |
| GLDM Features | 2 | 1 | 2 |
| Features | Features | Test | AUC | Accuracy | Sensitivity | Specificity |
|---|---|---|---|---|---|---|
| Radiomics | Lasso + LDA | Internal Test | 0.795 ± 0.033 | 0.722 ± 0.042 | 0.724 ± 0.043 | 0.719 ± 0.046 |
| External Test | 0.631 ± 0.015 | 0.508 ± 0.027 | 0.278 ± 0.017 | 0.840 ± 0.019 | ||
| SVC + LDA | Internal Test | 0.782 ± 0.034 | 0.730 ± 0.042 | 0.703 ± 0.058 | 0.769 ± 0.029 | |
| External Test | 0.646 ± 0.013 | 0.590 ± 0.021 | 0.323 ± 0.018 | 0.867 ± 0.030 | ||
| ETC + LDA | Internal Test | 0.764 ± 0.038 | 0.645 ± 0.039 | 0.708 ± 0.033 | 0.605 ± 0.030 | |
| External Test | 0.56 ± 0.017 | 0.525 ± 0.032 | 0.143 ± 0.031 | 0.725 ± 0.23 | ||
| Radiomics+ Clinics | Lasso + LDA | Internal Test | 0.837 ± 0.036 | 0.810 ± 0.042 | 0.857 ± 0.040 | 0.771 ± 0.044 |
| External Test | 0.700 ± 0.026 | 0.557 ± 0.027 | 0.314 ± 0.017 | 0.885 ± 0.030 | ||
| SVC + LDA | Internal Test | 0.798 ± 0.033 | 0.698 ± 0.046 | 0.676 ± 0.056 | 0.731 ± 0.046 | |
| External Test | 0.702 ± 0.015 | 0.492 ± 0.017 | 0.282 ± 0.010 | 0.864 ± 0.014 | ||
| ETC + LDA | Internal Test | 0.754 ± 0.024 | 0.710 ± 0.039 | 0.760 ± 0.038 | 0.676 ± 0.028 | |
| External Test | 0.607 ± 0.025 | 0.574 ± 0.027 | 0.286 ± 0.024 | 0.818 ± 0.021 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, Y.; Xu, J.; Chen, B.; Cao, L.; Chen, C. Efficient Prediction of Ki-67 Proliferation Index in Meningiomas on MRI: From Traditional Radiological Findings to a Machine Learning Approach. Cancers 2022, 14, 3637. https://doi.org/10.3390/cancers14153637
Zhao Y, Xu J, Chen B, Cao L, Chen C. Efficient Prediction of Ki-67 Proliferation Index in Meningiomas on MRI: From Traditional Radiological Findings to a Machine Learning Approach. Cancers. 2022; 14(15):3637. https://doi.org/10.3390/cancers14153637
Chicago/Turabian StyleZhao, Yanjie, Jianfeng Xu, Boran Chen, Le Cao, and Chaoyue Chen. 2022. "Efficient Prediction of Ki-67 Proliferation Index in Meningiomas on MRI: From Traditional Radiological Findings to a Machine Learning Approach" Cancers 14, no. 15: 3637. https://doi.org/10.3390/cancers14153637