
A Multiparametric MR-Based RadioFusionOmics Model with Robust Capabilities of Differentiating Glioblastoma Multiforme from Solitary Brain Metastasis

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Cohort
2.2. Image Acquisition and Histopathology
2.3. Delineation of Volume of Interest (VOI)
2.4. Extraction of Radiomics Features
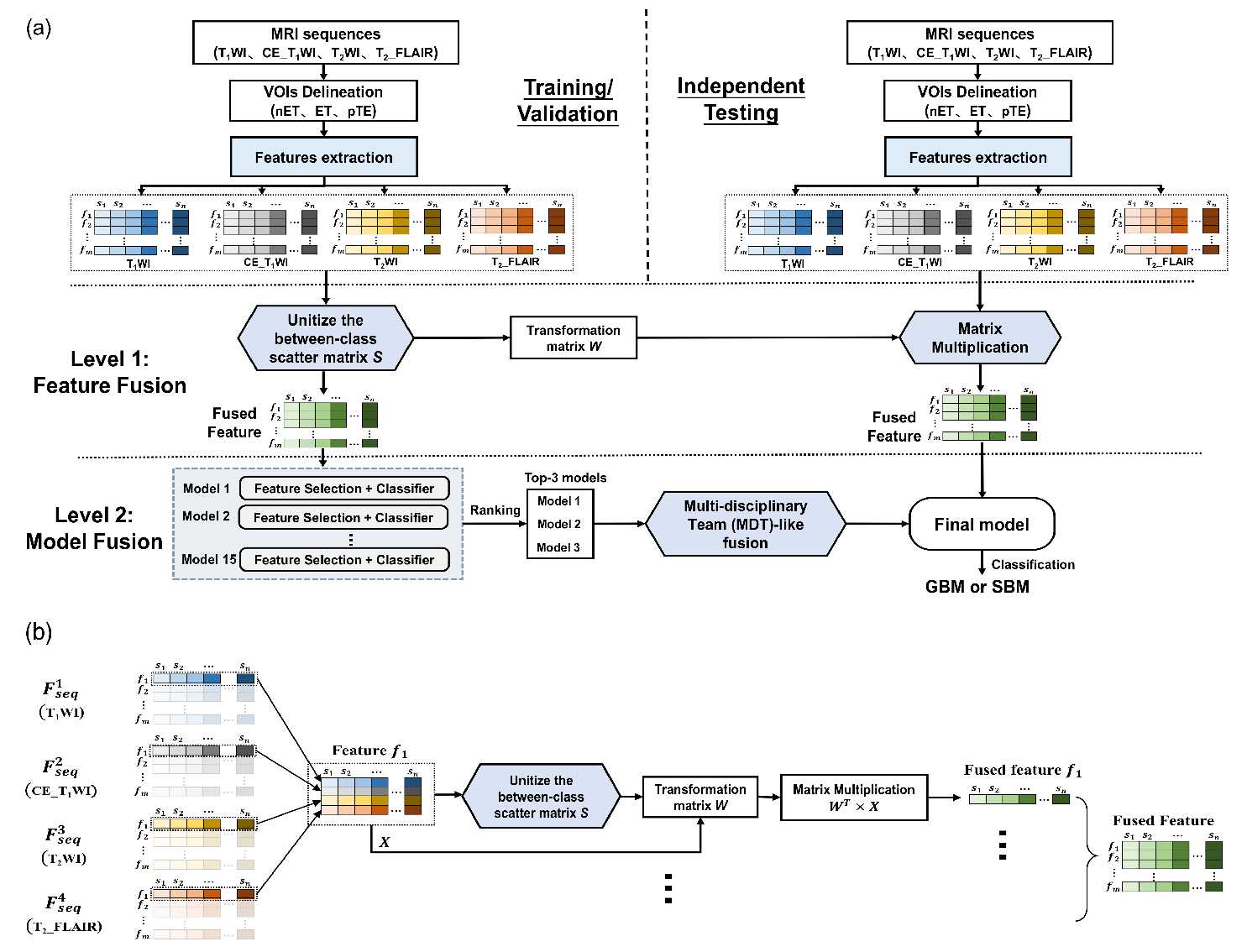
2.5. RadioFusionOmics
2.5.1. Level 1: Feature Fusion
2.5.2. Level 2: Model Fusion
2.5.3. Independent Testing
2.6. Evaluation of the Model
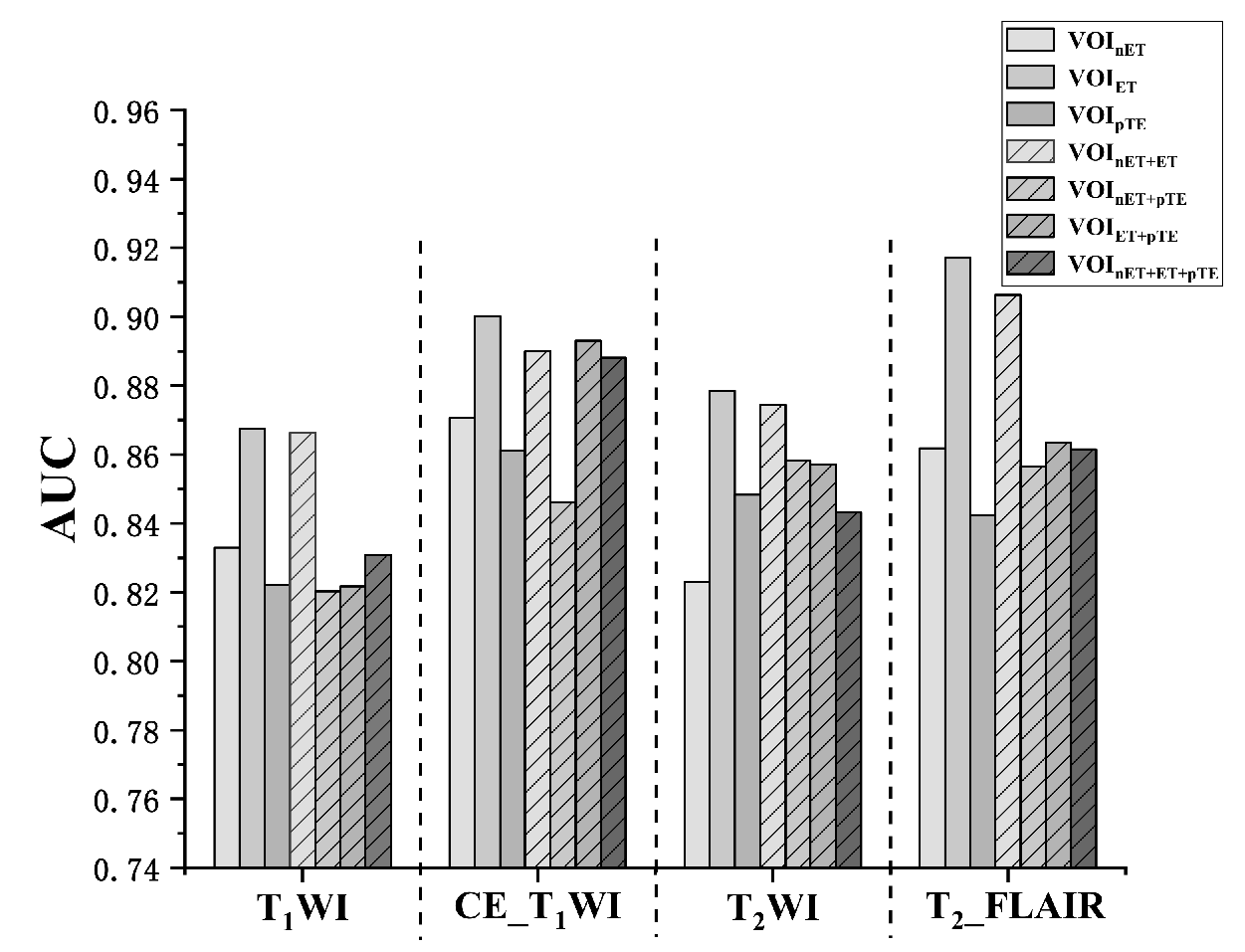
2.6.1. Study 1: Comparison of Lesion VOI
2.6.2. Study 2: Comparisons of the Different Combinations of Mri Sequences Used in the Fusion
2.6.3. Study 3: Comparison with Radiologist Performance
2.6.4. Study 4: Top Features
2.7. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Study 1: Comparison of the Lesion VOIs
3.3. Study 2: Combination of the MRI Sequences for Fusion
3.4. Study 3: The RFO Model vs. Radiologist Performance
3.5. Study 4: Highly Correlated Radiomics Markers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Feature Level Fusion:
References
- Louis, D.N.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization classification of tumors of the central nervous system: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [Green Version]
- Hanif, F.; Muzaffar, K.; Perveen, K.; Malhi, S.M.; Simjee, S.U. Glioblastoma multiforme: A review of its epidemiology and pathogenesis through clinical presentation and treatment. Asian Pac. J. Cancer Prev. 2017, 18, 3. [Google Scholar] [PubMed]
- Pruitt, A.A. Epidemiology, Treatment, and Complications of Central Nervous System Metastases. Contin. Lifelong Learn. Neurol. 2017, 23, 1580–1600. [Google Scholar] [CrossRef]
- Meier, R.; Pahud de Mortanges, A.; Wiest, R.; Knecht, U. Exploratory Analysis of Qualitative MR Imaging Features for the Differentiation of Glioblastoma and Brain Metastases. Front. Oncol. 2020, 10, 2756. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Ramón, R.; Ruiz-España, S.; Mollá-Olmos, E.; Moratal, D. Glioblastomas and brain metastases differentiation following an MRI texture analysis-based radiomics approach. Phys. Med. 2020, 76, 44–54. [Google Scholar] [CrossRef] [PubMed]
- Razek, A.A.K.A.; Talaat, M.; El-Serougy, L.; Abdelsalam, M.; Gaballa, G. Differentiating Glioblastomas from Solitary Brain Metastases Using Arterial Spin Labeling Perfusion− and Diffusion Tensor Imaging−Derived Metrics. World Neurosurg. 2019, 127, e593–e598. [Google Scholar] [CrossRef]
- Bauer, A.H.; Erly, W.; Moser, F.G.; Maya, M.; Nael, K. Differentiation of solitary brain metastasis from glioblastoma multiforme: A predictive multiparametric approach using combined MR diffusion and perfusion. Neuroradiology 2015, 57, 697–703. [Google Scholar] [CrossRef]
- Chiang, I.C.; Kuo, Y.-T.; Lu, C.-Y.; Yeung, K.-W.; Lin, W.-C.; Sheu, F.-O.; Liu, G.-C. Distinction between high-grade gliomas and solitary metastases using peritumoral 3-T magnetic resonance spectroscopy, diffusion, and perfusion imagings. Neuroradiology 2004, 46, 619–627. [Google Scholar] [CrossRef]
- El-Serougy, L.G.; Razek, A.A.K.A.; Mousa, A.E.; Eldawoody, H.A.F.; El-Morsy, A.E.M.E. Medicine N: Differentiation between high-grade gliomas and metastatic brain tumors using Diffusion Tensor Imaging metrics. Egypt. J. Radiol. Nucl. Med. 2015, 46, 1099–1104. [Google Scholar] [CrossRef] [Green Version]
- Jung, B.C.; Arevalo-Perez, J.; Lyo, J.K.; Holodny, A.I.; Karimi, S.; Young, R.J.; Peck, K.K. Comparison of glioblastomas and brain metastases using dynamic contrast-enhanced perfusion MRI. J. Neuroimaging 2016, 26, 240–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Law, M.; Cha, S.; Knopp, E.A.; Johnson, G.; Arnett, J.; Litt, A.W. High-grade gliomas and solitary metastases: Differentiation by using perfusion and proton spectroscopic MR imaging. Radiology 2002, 222, 715–721. [Google Scholar] [CrossRef] [PubMed]
- She, D.; Xing, Z.; Cao, D. Differentiation of Glioblastoma and Solitary Brain Metastasis by Gradient of Relative Cerebral Blood Volume in the Peritumoral Brain Zone Derived from Dynamic Susceptibility Contrast Perfusion Magnetic Resonance Imaging. J. Comput. Assist. Tomogr. 2019, 43, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Aneja, S.; Chang, E.; Omuro, A. Applications of artificial intelligence in neuro-oncology. Curr. Opin. Neurol. 2019, 32, 850–856. [Google Scholar] [CrossRef] [PubMed]
- Lotan, E.; Jain, R.; Razavian, N.; Fatterpekar, G.M.; Lui, Y.W. State of the art: Machine learning applications in glioma imaging. Am. J. Roentgenol. 2019, 212, 26–37. [Google Scholar] [CrossRef]
- Dong, F.; Li, Q.; Jiang, B.; Zhu, X.; Zeng, Q.; Huang, P.; Chen, S.; Zhang, M. Differentiation of supratentorial single brain metastasis and glioblastoma by using peri-enhancing oedema region–derived radiomic features and multiple classifiers. Eur. Radiol. 2020, 30, 3015–3022. [Google Scholar] [CrossRef]
- Kamimura, K.; Nakajo, M.; Yoneyama, T.; Fukukura, Y.; Hirano, H.; Goto, Y.; Sasaki, M.; Akamine, Y.; Keupp, J.; Yoshiura, T. Histogram analysis of amide proton transfer–weighted imaging: Comparison of glioblastoma and solitary brain metastasis in enhancing tumors and peritumoral regions. Eur. Radiol. 2018, 29, 4133–4140. [Google Scholar] [CrossRef]
- Skogen, K.; Schulz, A.; Helseth, E.; Ganeshan, B.; Dormagen, J.B.; Server, A. Texture analysis on diffusion tensor imaging: Discriminating glioblastoma from single brain metastasis. Acta Radiol. 2018, 60, 356–366. [Google Scholar] [CrossRef]
- Swinburne, N.C.; Schefflein, J.; Sakai, Y.; Oermann, E.K.; Titano, J.J.; Chen, I.; Tadayon, S.; Aggarwal, A.; Doshi, A.; Nael, K. Machine learning for semi automated classification of glioblastoma, brain metastasis and central nervous system lymphoma using magnetic resonance advanced imaging. Ann. Transl. Med. 2019, 7, 232. [Google Scholar] [CrossRef]
- Tateishi, M.; Nakaura, T.; Kitajima, M.; Uetani, H.; Nakagawa, M.; Inoue, T.; Kuroda, J.-I.; Mukasa, A.; Yamashita, Y. An initial experience of machine learning based on multi-sequence texture parameters in magnetic resonance imaging to differentiate glioblastoma from brain metastases. J. Neurol. Sci. 2019, 410, 116514. [Google Scholar] [CrossRef]
- Zhang, G.; Chen, X.; Zhang, S.; Ruan, X.; Gao, C.; Liu, Z.; Wei, X. Discrimination between solitary brain metastasis and glioblastoma multiforme by using ADC-based texture analysis: A comparison of two different ROI placements. Acad. Radiol. 2019, 26, 1466–1472. [Google Scholar] [CrossRef]
- Csutak, C.; Ștefan, P.-A.; Lenghel, L.M.; Moroșanu, C.O.; Lupean, R.-A.; Șimonca, L.; Mihu, C.M.; Lebovici, A. Differentiating High-Grade Gliomas from Brain Metastases at Magnetic Resonance: The Role of Texture Analysis of the Peritumoral Zone. Brain Sci. 2020, 10, 638. [Google Scholar] [CrossRef] [PubMed]
- Artzi, M.; Bressler, I.; Ben Bashat, D. Differentiation between glioblastoma, brain metastasis and subtypes using radiomics analysis. J. Magn. Reson. Imaging 2019, 50, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Ou, X.; Wang, J.; Guo, W.; Ma, X. Radiomics-based machine learning in differentiation between glioblastoma and metastatic brain tumors. Front. Oncol. 2019, 9, 806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bae, S.; An, C.; Ahn, S.S.; Kim, H.; Han, K.; Kim, S.W.; Park, J.E.; Kim, H.S.; Lee, S.-K. Robust performance of deep learning for distinguishing glioblastoma from single brain metastasis using radiomic features: Model development and validation. Sci. Rep. 2020, 10, 1–10. [Google Scholar]
- Yang, R.; Wu, J.; Sun, L.; Lai, S.; Xu, Y.; Liu, X.; Ma, Y.; Zhen, X. Radiomics of small renal masses on multiphasic CT: Accuracy of machine learning–based classification models for the differentiation of renal cell carcinoma and angiomyolipoma without visible fat. Eur. Radiol. 2020, 30, 1254–1263. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Yang, R.; Liang, F.; Liu, G.; Chen, A.; Wu, H.; Lai, S.; Ding, W.; Wei, X.; Zhen, X.; et al. Prediction of Microvascular Invasion in Hepatocellular Carcinoma With a Multi-Disciplinary Team-Like Radiomics Fusion Model on Dynamic Contrast-Enhanced Computed Tomography. Front. Oncol. 2021, 11, 771. [Google Scholar] [CrossRef] [PubMed]
- Van Griethuysen, J.J.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.; Fillion-Robin, J.-C.; Pieper, S.; Aerts, H.J. Computational radiomics system to decode the radiographic phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef] [Green Version]
- Haghighat, M.; Abdel-Mottaleb, M.; Alhalabi, W. Security: Discriminant correlation analysis: Real-time feature level fusion for multimodal biometric recognition. Trans. Inf. Forensics Secur. 2016, 11, 1984–1996. [Google Scholar] [CrossRef] [Green Version]
- Janjua, T.I.; Rewatkar, P.; Ahmed-Cox, A.; Saeed, I.; Mansfeld, F.M.; Kulshreshtha, R.; Kumeria, T.; Ziegler, D.S.; Kavallaris, M.; Mazzieri, R.; et al. Frontiers in the treatment of glioblastoma: Past, present and emerging. Adv. Drug Deliv. Rev. 2021, 171, 108–138. [Google Scholar] [CrossRef]
- Xu, X.; Zhang, H.-L.; Liu, Q.-P.; Sun, S.-W.; Zhang, J.; Zhu, F.-P.; Yang, G.; Yan, X.; Zhang, Y.-D.; Liu, X.-S. Radiomic analysis of contrast-enhanced CT predicts microvascular invasion and outcome in hepatocellular carcinoma. J. Hepatol. 2019, 70, 1133–1144. [Google Scholar] [CrossRef]
- Qian, Z.; Li, Y.; Wang, Y.; Li, L.; Li, R.; Wang, K.; Li, S.; Tang, K.; Zhang, C.; Fan, X.; et al. Differentiation of glioblastoma from solitary brain metastases using radiomic machine-learning classifiers. Cancer Lett. 2019, 451, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Warrington, N.M.; Taylor, S.J.; Whitmire, P.; Carrasco, E.; Singleton, K.W.; Wu, N.; Lathia, J.D.; Berens, M.E.; Kim, A.H.; et al. Sex differences in GBM revealed by analysis of patient imaging, transcriptome, and survival data. Sci. Transl. Med. 2019, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bayramoglu, N.; Tiulpin, A.; Hirvasniemi, J.; Nieminen, M.T.; Saarakkala, S. Adaptive segmentation of knee radiographs for selecting the optimal ROI in texture analysis. Osteoarthr. Cartil. 2020, 28, 941–952. [Google Scholar] [CrossRef] [Green Version]
- Petrujkić, K.; Milošević, N.; Rajković, N.; Stanisavljević, D.; Gavrilović, S.; Dželebdžić, D.; Ilić, R.; Di Ieva AMaksimović, R. Computational quantitative MR image features-a potential useful tool in differentiating glioblastoma from solitary brain metastasis. Eur. J. Radiol. 2019, 119, 108634. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Knopp, M.V. Quantifying tumor vascular heterogeneity with dynamic contrast-enhanced magnetic resonance imaging: A review. J. Biomed. Biotechnol. 2011, 2011, 732848. [Google Scholar] [CrossRef]
- Tozer, D.J.; Jäger, H.R.; Danchaivijitr, N.; Benton, C.E.; Tofts, P.S.; Rees, J.H.; Waldman, A.D. Apparent diffusion coefficient histograms may predict low-grade glioma subtype. NMR Biomed. 2007, 20, 49–57. [Google Scholar] [CrossRef]
- Lopes, M.B. Angiogenesis in brain tumors. Microsc. Res. Tech. 2003, 60, 225–230. [Google Scholar] [CrossRef]
- Schwartz, K.M.; Erickson, B.J.; Lucchinetti, C. Pattern of T2 hypointensity associated with ring-enhancing brain lesions can help to differentiate pathology. Neuroradiology 2006, 48, 143–149. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | Total | Training/Validation Cohort | Independent Testing Cohort 1 | Independent Testing Cohort 2 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| GBM (n = 131) | SBM (n = 113) | p-Value | GBM (n = 61) | SBM (n = 60) | p-Value | GBM (n = 33) | SBM (n = 29) | p-Value | GBM (n = 37) | SBM (n = 24) | p-Value | ||
| Age, mean ± SD (years) | 52.22 ± 15.59 | 58.18 ± 9.83 | 0.012 c | 49.92 ± 16.07 | 58.02 ± 9.89 | 0.001 a | 54.79 ± 15.48 | 59.34 ± 11.29 | 0.196 a | 53.73 ± 14.75 | 57.17 ± 7.95 | 0.251 a | |
| Sex | Female | 51 | 37 | 0.316 b | 26 | 20 | 0.293 b | 11 | 7 | 0.426 b | 14 | 10 | 0.765 b |
| Male | 80 | 76 | 35 | 40 | 22 | 22 | 23 | 14 | |||||
| Lesion location | Supratentorial | 128 | 91 | 0.001 b | 61 | 50 | 0.001 b | 30 | 19 | 0.014 b | 37 | 22 | 0.074 b |
| Infratentorial | 3 | 22 | 0 | 10 | 3 | 10 | 0 | 2 | |||||
| Models | Independent Testing Cohort 1 (n = 62) | Independent Testing Cohort 2 (n = 61) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| AUC | ACC | SEN | SPE | AUC | ACC | SEN | SPE | ||
| Top 3 models’ mean | 0.916 | 0.852 | 0.857 | 0.843 | 0.864 | 0.825 | 0.708 | 0.901 | |
| Proposed RFO model (radiomics) | 0.925 | 0.855 | 0.856 | 0.853 | 0.859 | 0.836 | 0.708 | 0.919 | |
| Proposed RFO model (age + radiomics) | 0.922 | 0.855 | 0.857 | 0.853 | 0.866 | 0.820 | 0.708 | 0.892 | |
| Proposed RFO model (location + radiomics) | 0.929 | 0.871 | 0.893 | 0.853 | 0.858 | 0.836 | 0.708 | 0.919 | |
| Proposed RFO model (age + location + radiomics) | 0.927 | 0.855 | 0.848 | 0.860 | 0.865 | 0.852 | 0.750 | 0.919 | |
| Neuroradiologists | #1 (3 years experiences) | 0.607 | 0.597 | 0.576 | 0.621 | 0.610 | 0.607 | 0.625 | 0.595 |
| #2 (5 years experiences) | 0.628 | 0.629 | 0.546 | 0.724 | 0.658 | 0.656 | 0.667 | 0.649 | |
| #3 (15 years experiences) | 0.754 | 0.758 | 0.758 | 0.759 | 0.782 | 0.770 | 0.833 | 0.730 | |
| MDT-decision of three specialists | 0.722 | 0.726 | 0.788 | 0.655 | 0.692 | 0.689 | 0.708 | 0.676 | |
| Models | Independent Testing Cohort 1 (n = 62) | Independent Testing Cohort 2 (n = 61) | ||||||
|---|---|---|---|---|---|---|---|---|
| AUC | ACC | SEN | SPE | AUC | ACC | SEN | SPE | |
| p-value (RFO vs. mean performance of three neuroradiologists) | 0.03 | 0.01 | 0.02 | 0.01 | 0.02 | 0.01 | 0.45 | 0.02 |
| p-value (RFO vs. MDT-decision of three specialists) | 0.03 | 0.02 | 0.03 | 0.02 | 0.03 | 0.02 | 0.44 | 0.03 |
| Category | Top10 Features | p-Value | M | (<M | >M) | |||
|---|---|---|---|---|---|---|---|
| T1WI | T2_FLAIR | T1WI | T2_FLAIR | T1WI | T2_FLAIR | ||
| Firstorder (n = 4) | 90Percentile (1st) | 0.016 a | <10−7, a | 1.01 | 2.86 | GBM (50.82% | 49.18%) | GBM (27.87% | 72.13%) |
| SBM (66.67% | 33.33%) | SBM (73.33% | 26.67%) | ||||||
| Median (3rd) | 0.707 a | <10−10, b | 0.66 | 2.17 | GBM (44.26% | 55.74%) | GBM (32.79% | 67.21%) | |
| SBM (50.00% | 50.00%) | SBM (81.67% | 18.33%) | ||||||
| Maximum (8th) | <10−4, a | <10−8, a | 1.85 | 4.02 | GBM (55.74% | 44.26%) | GBM (31.15% | 68.85%) | |
| SBM (76.67% | 23.33%) | SBM (80.00% | 20.00%) | ||||||
| Range (10th) | <10−6, a | <10−8, a | 2.03 | 3.91 | GBM (36.07% | 63.93%) | GBM (36.07% | 63.93%) | |
| SBM (80.00% | 20.00%) | SBM (80.00% | 20.00%) | ||||||
| Shape (n = 6) | MinorAxisLength (2nd) | <10−11, a | <10−11, a | 49.30 | 48.8 | GBM (44.26% | 55.74%) | GBM (37.70%| 62.30%) |
| SBM (86.67% | 13.33%) | SBM (86.67% | 13.33%) | ||||||
| Maximum2DDiameterColumn (4th) | <10−13, a | <10−13, a | 62.20 | 61.60 | GBM (34.43% | 65.57%) | GBM (31.15% | 68.85%) | |
| SBM (88.33% | 11.67%) | SBM (88.33% | 11.67%) | ||||||
| Maximum2DDiameterSlice (5th) | <10−12, a | <10−12, a | 64.37 | 63.73 | GBM (44.26% | 55.74%) | GBM (44.26% | 55.74%) | |
| SBM (90.00% | 10.00%) | SBM (90.00% | 10.00%) | ||||||
| Flatness (6th) | <10−8, a | <10−8, a | 0.57 | 0.57 | GBM (49.18% | 50.82%) | GBM (50.82% | 49.18%) | |
| SBM (8.33% | 91.67%) | SBM (8.33% | 91.67%) | ||||||
| MajorAxisLength (7th) | <10−14, a | <10−13, a | 61.79 | 61.05 | GBM (42.62% | 57.38%) | GBM (40.98% | 59.02%) | |
| SBM (91.67% | 8.33%) | SBM (90.00% | 10.00%) | ||||||
| VoxelVolume (9th) | <10−9, a | <10−9, a | 34001.88 | 33353.47 | GBM (39.34% | 60.66%) | GBM (37.70% | 62.30%) | |
| SBM (76.67% | 23.33%) | SBM (76.67% | 23.33%) | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, J.; Liang, F.; Wei, R.; Lai, S.; Lv, X.; Luo, S.; Wu, Z.; Chen, H.; Zhang, W.; Zeng, X.; et al. A Multiparametric MR-Based RadioFusionOmics Model with Robust Capabilities of Differentiating Glioblastoma Multiforme from Solitary Brain Metastasis. Cancers 2021, 13, 5793. https://doi.org/10.3390/cancers13225793
Wu J, Liang F, Wei R, Lai S, Lv X, Luo S, Wu Z, Chen H, Zhang W, Zeng X, et al. A Multiparametric MR-Based RadioFusionOmics Model with Robust Capabilities of Differentiating Glioblastoma Multiforme from Solitary Brain Metastasis. Cancers. 2021; 13(22):5793. https://doi.org/10.3390/cancers13225793
Chicago/Turabian StyleWu, Jialiang, Fangrong Liang, Ruili Wei, Shengsheng Lai, Xiaofei Lv, Shiwei Luo, Zhe Wu, Huixian Chen, Wanli Zhang, Xiangling Zeng, and et al. 2021. "A Multiparametric MR-Based RadioFusionOmics Model with Robust Capabilities of Differentiating Glioblastoma Multiforme from Solitary Brain Metastasis" Cancers 13, no. 22: 5793. https://doi.org/10.3390/cancers13225793