
Predicting the Performance of Concurrent Systematic Random Biopsies during Image Fusion Targeted Sampling of Multi-Parametric MRI Detected Prostate Cancer. A Prospective Study (PRESET Study)


Abstract
:Simple Summary
Abstract
1. Introduction
- (1)
- Compare the diagnostic accuracy of MRI/US fusion targeted biopsies, systematic biopsies and combined approaches in the detection of csPCa and define predictive factors where a combined approach could be used.
- (2)
- Quantify additional benefits of adding systematic biopsies to the targeted biopsies approach by constructing a nomogram and assessing its net clinical benefits.
2. Materials and Methods
2.1. Study Population
2.2. Outcomes
2.3. Sample Size Estimation
2.4. Multi-Parametric MRI
2.5. Biopsy Procedures
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Comparison of the Detection Rate of csPCa between SB, TB and Combined Approaches
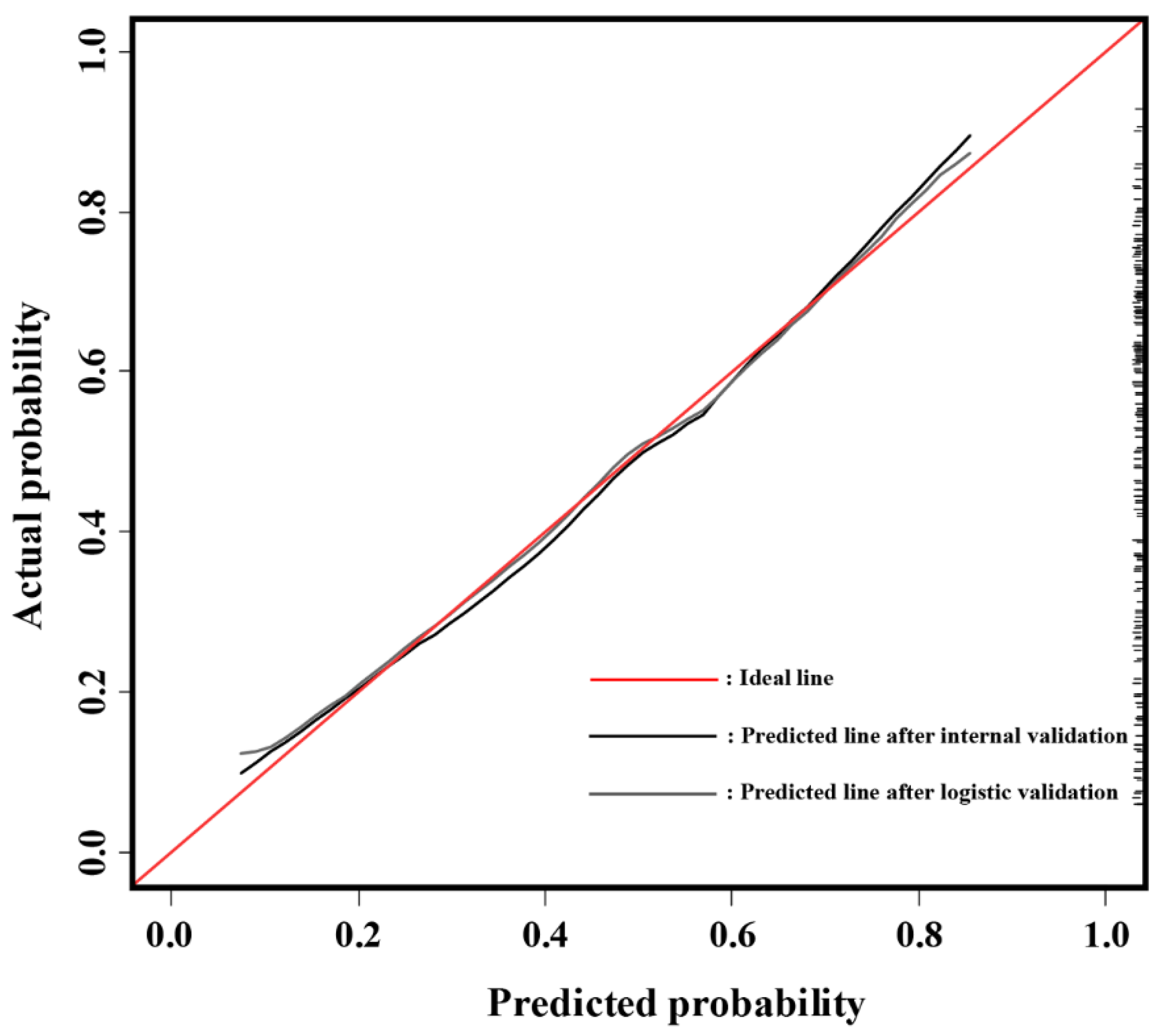
3.3. Univariate and Multivariate Logistic Regression Analysis and Developed Nomogram
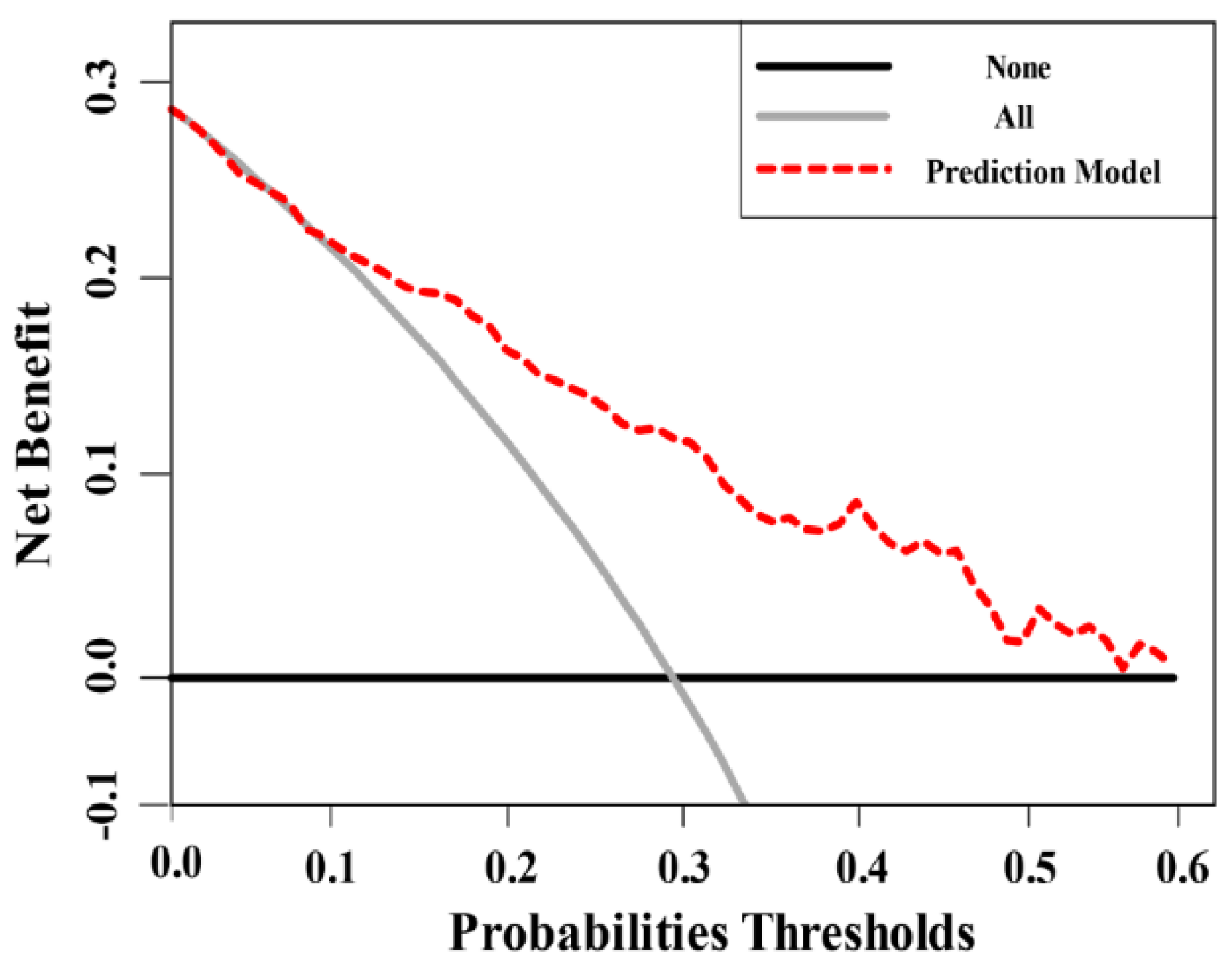
3.4. Decision Curve Analysis
4. Discussion
4.1. Principal Findings of the Study
4.2. Study Findings in Context of the Reported Literature
4.3. Clinical Implications of the Study Findings and Limitation of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kasivisvanathan, V.; Rannikko, A.S.; Borghi, M.; Panebianco, V.; Mynderse, L.A.; Vaarala, M.H.; Briganti, A.; Budäus, L.; Hellawell, G.; Hindley, R.G.; et al. MRI-Targeted or Standard Biopsy for Prostate-Cancer Diagnosis. N. Engl. J. Med. 2018, 378, 1767–1777. [Google Scholar] [CrossRef]
- Ahmed, H.U.; El-Shater Bosaily, A.; Brown, L.C.; Gabe, R.; Kaplan, R.; Parmar, M.K.; Collaco-Moraes, Y.; Ward, K.; Hindley, R.G.; Freeman, A.; et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): A paired validating confirmatory study. Lancet 2017, 389, 815–822. [Google Scholar] [CrossRef] [Green Version]
- Pokorny, M.R.; de Rooij, M.; Duncan, E.; Schröder, F.H.; Parkinson, R.; Barentsz, J.O.; Thompson, L.C. Prospective study of diagnostic accuracy comparing prostate cancer detection by transrectal ultrasound-guided biopsy versus magnetic resonance (MR) imaging with subsequent mr-guided biopsy in men without previous prostate biopsies. Eur. Urol. 2014, 66, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer—2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2021, 79, 243–262. [Google Scholar] [CrossRef] [PubMed]
- Drost, F.J.H.; Osses, D.; Nieboer, D.; Bangma, C.H.; Steyerberg, E.W.; Roobol, M.J.; Schoots, I.G. Prostate Magnetic Resonance Imaging, with or Without Magnetic Resonance Imaging-targeted Biopsy, and Systematic Biopsy for Detecting Prostate Cancer: A Cochrane Systematic Review and Meta-analysis. Eur. Urol. 2020, 77, 78–94. [Google Scholar] [CrossRef] [PubMed]
- Padhani, A.R.; Weinreb, J.; Rosenkrantz, A.B.; Villeirs, G.; Turkbey, B.; Barentsz, J. Prostate Imaging-Reporting and Data System Steering Committee: PI-RADS v2 Status Update and Future Directions. Eur. Urol. 2019, 75, 385–396. [Google Scholar] [CrossRef] [Green Version]
- Kasivisvanathan, V.; Stabile, A.; Neves, J.B.; Giganti, F.; Valerio, M.; Shanmugabavan, Y.; Clement, K.D.; Sarkar, D.; Philippou, Y.; Thurtle, D.; et al. Magnetic Resonance Imaging-targeted Biopsy Versus Systematic Biopsy in the Detection of Prostate Cancer: A Systematic Review and Meta-analysis. Eur. Urol. 2019, 76, 284–303. [Google Scholar] [CrossRef] [Green Version]
- Sonn, G.A.; Natarajan, S.; Margolis, D.J.A.; MacAiran, M.; Lieu, P.; Huang, J.; Dorey, F.J.; Marks, L.S. Targeted biopsy in the detection of prostate cancer using an office based magnetic resonance ultrasound fusion device. J. Urol. 2013, 189, 86–92. [Google Scholar] [CrossRef] [Green Version]
- Wysock, J.S.; Rosenkrantz, A.B.; Huang, W.C.; Stifelman, M.D.; Lepor, H.; Deng, F.-M.; Melamed, J.; Taneja, S.S. A Prospective, Blinded Comparison of Magnetic Resonance (MR) Imaging–Ultrasound Fusion and Visual Estimation in the Performance of MR-targeted Prostate Biopsy: The PROFUS Trial. Eur. Urol. 2014, 66, 343–351. [Google Scholar] [CrossRef]
- Ahdoot, M.; Wilbur, A.R.; Reese, S.E.; Lebastchi, A.H.; Mehralivand, S.; Gomella, P.T.; Bloom, J.; Gurram, S.; Siddiqui, M.; Pinsky, P.; et al. MRI-Targeted, Systematic, and Combined Biopsy for Prostate Cancer Diagnosis. N. Engl. J. Med. 2020, 382, 917–928. [Google Scholar] [CrossRef]
- Rouvière, O.; Puech, P.; Renard-Penna, R.; Claudon, M.; Roy, C.; Mège-Lechevallier, F.; Decaussin-Petrucci, M.; Dubreuil-Chambardel, M.; Magaud, L.; Remontet, L.; et al. Use of prostate systematic and targeted biopsy on the basis of multiparametric MRI in biopsy-naive patients (MRI-FIRST): A prospective, multicentre, paired diagnostic study. Lancet Oncol. 2019, 20, 100–109. [Google Scholar] [CrossRef]
- Elkhoury, F.F.; Felker, E.R.; Kwan, L.; Sisk, A.E.; Delfin, M.; Natarajan, S.; Marks, L.S. Comparison of Targeted vs Systematic Prostate Biopsy in Men Who Are Biopsy Naive: The Prospective Assessment of Image Registration in the Diagnosis of Prostate Cancer (PAIREDCAP) Study. JAMA Surg. 2019, 154, 811–818. [Google Scholar] [CrossRef] [PubMed]
- Dell’Oglio, P.; Stabile, A.; Soligo, M.; Brembilla, G.; Esposito, A.; Gandaglia, G.; Fossati, N.; Bravi, C.A.; Dehò, F.; De Cobelli, F.; et al. There Is No Way to Avoid Systematic Prostate Biopsies in Addition to Multiparametric Magnetic Resonance Imaging Targeted Biopsies. Eur. Urol. Oncol. 2020, 3, 112–118. [Google Scholar] [CrossRef]
- Siddiqui, M.M.; Rais-Bahrami, S.; Turkbey, B.; George, A.K.; Rothwax, J.; Shakir, N.; Okoro, C.; Raskolnikov, D.; Parnes, H.L.; Linehan, W.M.; et al. Comparison of MR/ultrasound fusion-guided biopsy with ultrasound-guided biopsy for the diagnosis of prostate cancer. JAMA 2015, 313, 390–397. [Google Scholar] [CrossRef]
- Sonn, G.A.; Chang, E.; Natarajan, S.; Margolis, D.J.; MacAiran, M.; Lieu, P.; Huang, J.; Dorey, F.J.; Reiter, R.E.; Marks, L.S. Value of targeted prostate biopsy using magnetic resonance-ultrasound fusion in men with prior negative biopsy and elevated prostate-specific antigen. Eur. Urol. 2014, 65, 809–815. [Google Scholar] [CrossRef] [Green Version]
- Puech, P.; Rouvière, O.; Renard-Penna, R.; Villers, A.; Devos, P.; Colombel, M.; Bitker, M.-O.; Leroy, X.; Mège-Lechevallier, F.; Comperat, E.; et al. Prostate cancer Diagnosis: Multiparametric MR-targeted Biopsy with Cognitive and Transrectal US–MR Fusion Guidance versus Systematic Biopsy—Prospective Multicenter Study. Radiology 2013, 268, 461–469. [Google Scholar] [CrossRef]
- Wei, C.; Jin, B.; Szewczyk-Bieda, M.; Gandy, S.; Lang, S.; Zhang, Y.; Huang, Z.; Nabi, G. Quantitative parameters in dynamic contrast-enhanced magnetic resonance imaging for the detection and characterisation of prostate cancer. Oncotarget 2018, 9, 15997–16007. [Google Scholar] [CrossRef] [Green Version]
- Filson, C.P.; Natarajan, S.; Margolis, D.J.A.; Huang, J.; Lieu, P.; Dorey, F.J.; Reiter, R.E.; Marks, L.S. Prostate cancer detection with magnetic resonance-ultrasound fusion biopsy: The role of systematic and targeted biopsies. Cancer 2016, 122, 884–892. [Google Scholar] [CrossRef] [PubMed]
- Cash, H.; Günzel, K.; Maxeiner, A.; Stephan, C.; Fischer, T.; Durmus, T.; Miller, K.; Asbach, P.; Haas, M.; Kempkensteffen, C. Prostate cancer detection on transrectal ultrasonography-guided random biopsy despite negative real-time magnetic resonance imaging/ultrasonography fusion-guided targeted biopsy: Reasons for targeted biopsy failure. BJU Int. 2016, 118, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Connor, M.J.; Miah, S.; Jayadevan, R.; Khoo, C.C.; Eldred-Evans, D.; Shah, T.; Ahmed, H.U.; Marks, L. Value of systematic sampling in an mp-MRI targeted prostate biopsy strategy. Transl. Androl. Urol. 2020, 9, 1501–1509. [Google Scholar] [CrossRef]
- Alqahtani, S.; Wei, C.; Zhang, Y.; Szewczyk-Bieda, M.; Wilson, J.; Huang, Z.; Nabi, G. Prediction of prostate cancer Gleason score upgrading from biopsy to radical prostatectomy using pre-biopsy multiparametric MRI PIRADS scoring system. Sci. Rep. 2020, 10, 1–9. [Google Scholar] [CrossRef]
- Epstein, J.I.; Feng, Z.; Trock, B.J.; Pierorazio, P.M. Upgrading and Downgrading of Prostate Cancer from Biopsy to Radical Prostatectomy: Incidence and Predictive Factors Using the Modified Gleason Grading System and Factoring in Tertiary Grades. Eur. Urol. 2012, 61, 1019–1024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sathianathen, N.J.; Warlick, C.A.; Weight, C.J.; Ordonez, M.A.; Spilseth, B.; Metzger, G.J.; Murugan, P.; Konety, B.R. A clinical prediction tool to determine the need for concurrent systematic sampling at the time of magnetic resonance imaging-guided biopsy. BJU Int. 2019, 123, 612–617. [Google Scholar] [CrossRef]
- Sathianathen, N.J.; Butaney, M.; Bongiorno, C.; Konety, B.R.; Bolton, D.M.; Lawrentschuk, N. Accuracy of the magnetic resonance imaging pathway in the detection of prostate cancer: A systematic review and meta-analysis. Prostate Cancer Prostatic Dis. 2019, 22, 39–48. [Google Scholar] [CrossRef]
- Muthigi, A.; George, A.K.; Sidana, A.; Kongnyuy, M.; Simon, R.; Moreno, V.; Merino, M.J.; Choyke, P.L.; Turkbey, B.; Wood, B.J.; et al. Missing the Mark: Prostate Cancer Upgrading by Systematic Biopsy over Magnetic Resonance Imaging/Transrectal Ultrasound Fusion Biopsy. J. Urol. 2017, 197, 327–334. [Google Scholar] [CrossRef]
- Siddiqui, M.M.; Rais-Bahrami, S.; Truong, H.; Stamatakis, L.; Vourganti, S.; Nix, J.; Hoang, A.N.; Walton-Diaz, A.; Shuch, B.; Weintraub, M.; et al. Magnetic Resonance Imaging/Ultrasound–Fusion Biopsy Significantly Upgrades Prostate Cancer Versus Systematic 12-core Transrectal Ultrasound Biopsy. Eur. Urol. 2013, 64, 713–719. [Google Scholar] [CrossRef] [PubMed]
- Falagario, U.; Jambor, I.; Taimen, P.; Syvänen, K.T.; Kähkönen, E.; Merisaari, H.; Montoya Perez, I.; Knaapila, J.; Steiner, A.; Verho, J.; et al. Added value of systematic biopsy in men with a clinical suspicion of prostate cancer undergoing biparametric MRI-targeted biopsy: Multi-institutional external validation study. World J. Urol. 2020, 39, 1879–1887. [Google Scholar] [CrossRef] [PubMed]
- Schieda, N.; Quon, J.S.; Lim, C.; El-Khodary, M.; Shabana, W.; Singh, V.; Morash, C.; Breau, R.H.; McInnes, M.D.F.; Flood, T.A. Evaluation of the European Society of Urogenital Radiology (ESUR) PI-RADS scoring system for assessment of extra-prostatic extension in prostatic carcinoma. Eur. J. Radiol. 2015, 84, 1843–1848. [Google Scholar] [CrossRef] [PubMed]
- Perez, I.M.; Jambor, I.; Kauko, T.; Verho, J.; Ettala, O.; Falagario, U.; Merisaari, H.; Kiviniemi, A.; Taimen, P.; Syvänen, K.T.; et al. Qualitative and Quantitative Reporting of a Unique Biparametric MRI: Towards Biparametric MRI-Based Nomograms for Prediction of Prostate Biopsy Outcome in Men With a Clinical Suspicion of Prostate Cancer (IMPROD and MULTI-IMPROD Trials). J. Magn. Reson. Imaging 2020, 51, 1556–1567. [Google Scholar] [CrossRef]
- Jambor, I.; Boström, P.J.; Taimen, P.; Syvänen, K.; Kähkönen, E.; Kallajoki, M.; Perez, I.M.; Kauko, T.; Matomäki, J.; Ettala, O.; et al. Novel biparametric MRI and targeted biopsy improves risk stratification in men with a clinical suspicion of prostate cancer (IMPROD Trial). J. Magn. Reson. Imaging 2017, 46, 1089–1095. [Google Scholar] [CrossRef] [PubMed]
- Truong, M.; Hollenberg, G.; Weinberg, E.; Messing, E.M.; Miyamoto, H.; Frye, T.P. Impact of Gleason Subtype on Prostate Cancer Detection Using Multiparametric Magnetic Resonance Imaging: Correlation with Final Histopathology. J. Urol. 2017, 198, 316–321. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Overall (n = 198) | |
|---|---|---|
| Basic information | Age, median (IQR), in years | 67 (71–61) |
| Prostate specific antigen (PSA), median (IQR), ng/mL | 8.2 (10.6–6.4) | |
| Prostate volume, median (IQR), mL | 47 (63–33) | |
| PSA Density, median (IQR), ng/mL2 | 0.18 (0.27–0.11) | |
| mp-MRI | Number of lesions, n (%) | |
| 1 | 102 (51.5%) | |
| 2 | 75 (38%) | |
| 3 | 14 (7%) | |
| 4 | 6 (3%) | |
| 5 | 1 (0.5%) | |
| Index lesion size, median (IQR), mm | 16 (25–13) | |
| Prostate Imaging Reporting and Data System (PIRADS score), n (%) | ||
| PIRADS 3 | 22 (11%) | |
| PIRADS 4 | 55 (28%) | |
| PIRADS 5 | 121 (61%) | |
| Lesion location, n (%) | ||
| Peripheral zone (PZ) | 79 (40%) | |
| Transition zone (TZ) | 44 (22%) | |
| Both zones (TZ-PZ) | 75 (38%) | |
| Targeted (TB)/Systematic random (SB) biopsy | Detection of prostate cancer in TB, n (%) | 129 (65%) |
| Detection of prostate cancer in SB, n (%) | 127 (64%) | |
| Covariate | N | Univariate Logistic Regression | Multivariate Logistic Regression | ||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | OR | 95% CI | p Value | ||||
| Lower | Upper | Lower | Upper | ||||||
| Age (year) | 198 | 1.07 | 1.02 | 1.12 | 0.009 | 1.06 | 1.01 | 1.12 | 0.036 |
| PSAD | 198 | 92.79 | 7.61 | 1130.69 | <0.001 | 25.63 | 1.93 | 341.27 | 0.014 |
| Index lesion size | 198 | 1.06 | 1.03 | 1.10 | <0.001 | 1.02 | 0.98 | 1.06 | 0.399 |
| PIRADS | 198 | <0.001 | 0.001 | ||||||
| 3 | 22 | Ref | - | - | Ref | - | - | ||
| 4 | 55 | 1.69 | 0.49 | 5.80 | 0.406 | 1.51 | 0.42 | 5.43 | 0.525 |
| 5 | 121 | 9.46 | 3.00 | 29.84 | <0.001 | 5.94 | 1.77 | 19.93 | 0.004 |
| Number of Lesions | 0.309 | ||||||||
| 1 | 102 | Ref | - | - | |||||
| 2 | 75 | 1.11 | 0.61 | 2.02 | 0.730 | ||||
| 3 and above | 21 | 2.16 | 0.81 | 5.80 | 0.125 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alqahtani, S.; Zhang, X.; Wei, C.; Zhang, Y.; Szewczyk-Bieda, M.; Wilson, J.; Huang, Z.; Nabi, G. Predicting the Performance of Concurrent Systematic Random Biopsies during Image Fusion Targeted Sampling of Multi-Parametric MRI Detected Prostate Cancer. A Prospective Study (PRESET Study). Cancers 2022, 14, 1. https://doi.org/10.3390/cancers14010001
Alqahtani S, Zhang X, Wei C, Zhang Y, Szewczyk-Bieda M, Wilson J, Huang Z, Nabi G. Predicting the Performance of Concurrent Systematic Random Biopsies during Image Fusion Targeted Sampling of Multi-Parametric MRI Detected Prostate Cancer. A Prospective Study (PRESET Study). Cancers. 2022; 14(1):1. https://doi.org/10.3390/cancers14010001
Chicago/Turabian StyleAlqahtani, Saeed, Xinyu Zhang, Cheng Wei, Yilong Zhang, Magdalena Szewczyk-Bieda, Jennifer Wilson, Zhihong Huang, and Ghulam Nabi. 2022. "Predicting the Performance of Concurrent Systematic Random Biopsies during Image Fusion Targeted Sampling of Multi-Parametric MRI Detected Prostate Cancer. A Prospective Study (PRESET Study)" Cancers 14, no. 1: 1. https://doi.org/10.3390/cancers14010001