
Virtual Monoenergetic Images of Dual-Energy CT—Impact on Repeatability, Reproducibility, and Classification in Radiomics

 , , , , ,
, , , , ,  , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
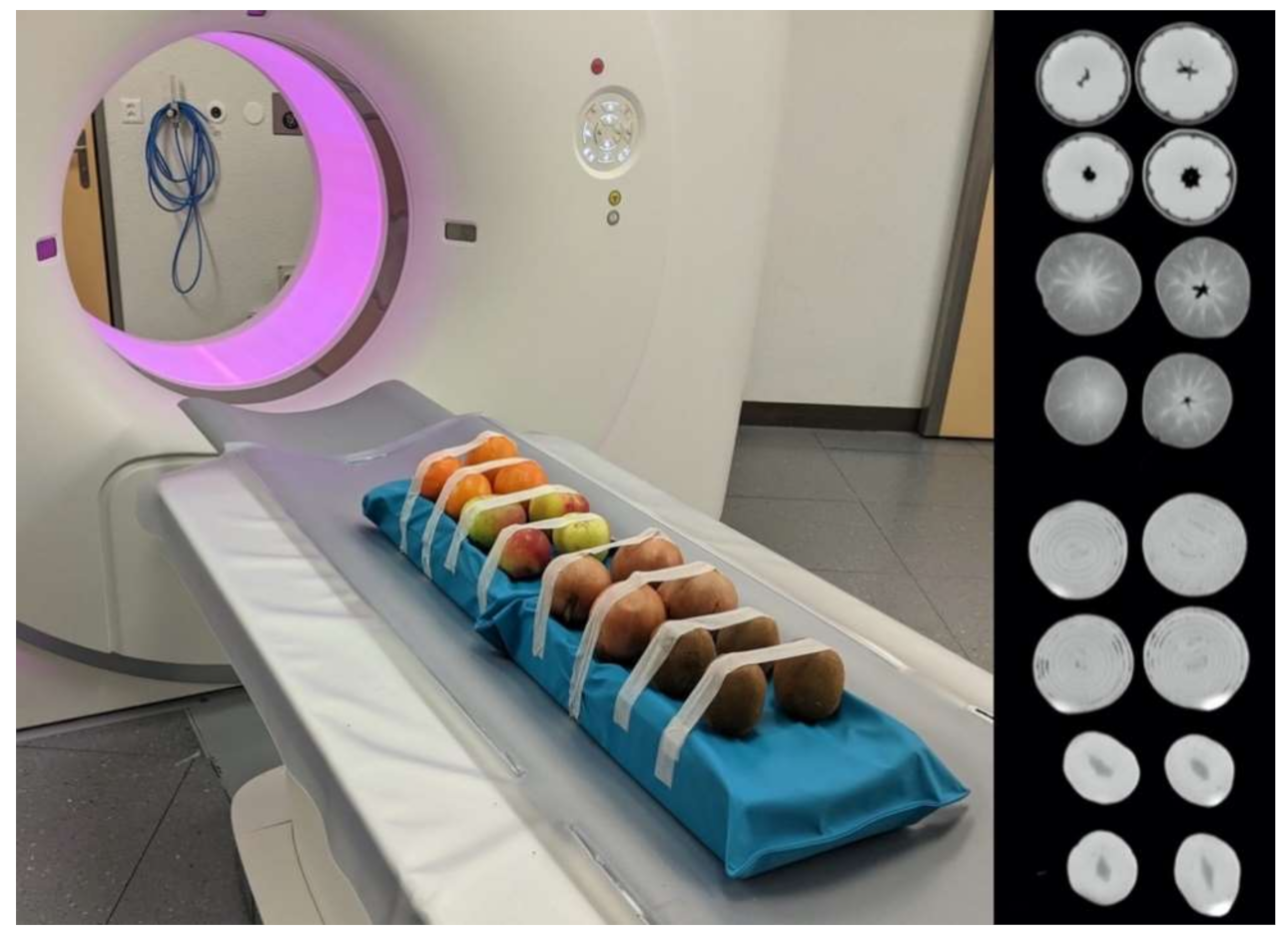
2.1. Part I—Ex Vivo Study
2.1.1. Phantom and Scan Setup
2.1.2. Image Segmentation and Feature Extraction
2.1.3. Analysis of Feature Repeatability and Reproducibility
2.1.4. Impact on Machine Learning Classification
2.2. Part II—In Vivo Study
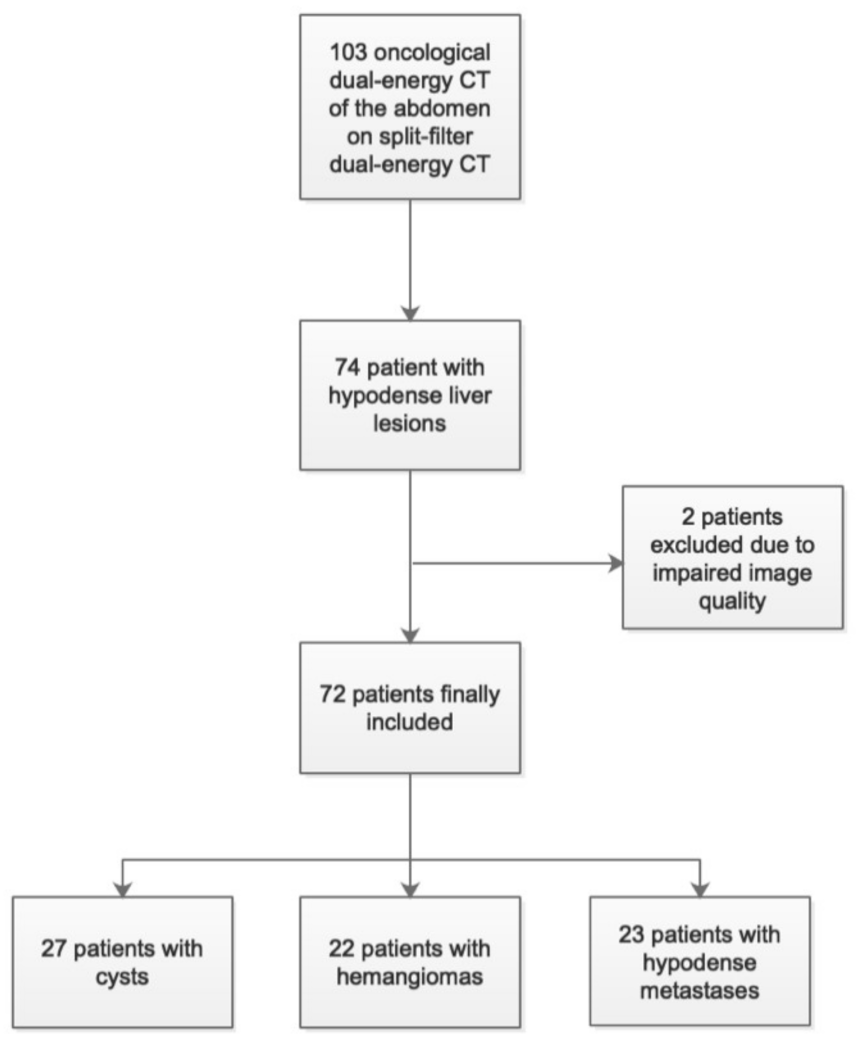
2.2.1. Patient Population and Image Reconstruction
2.2.2. Image Segmentation and Feature Extraction
2.2.3. Impact on Machine Learning Classification
3. Results
3.1. Part I—Ex Vivo Study
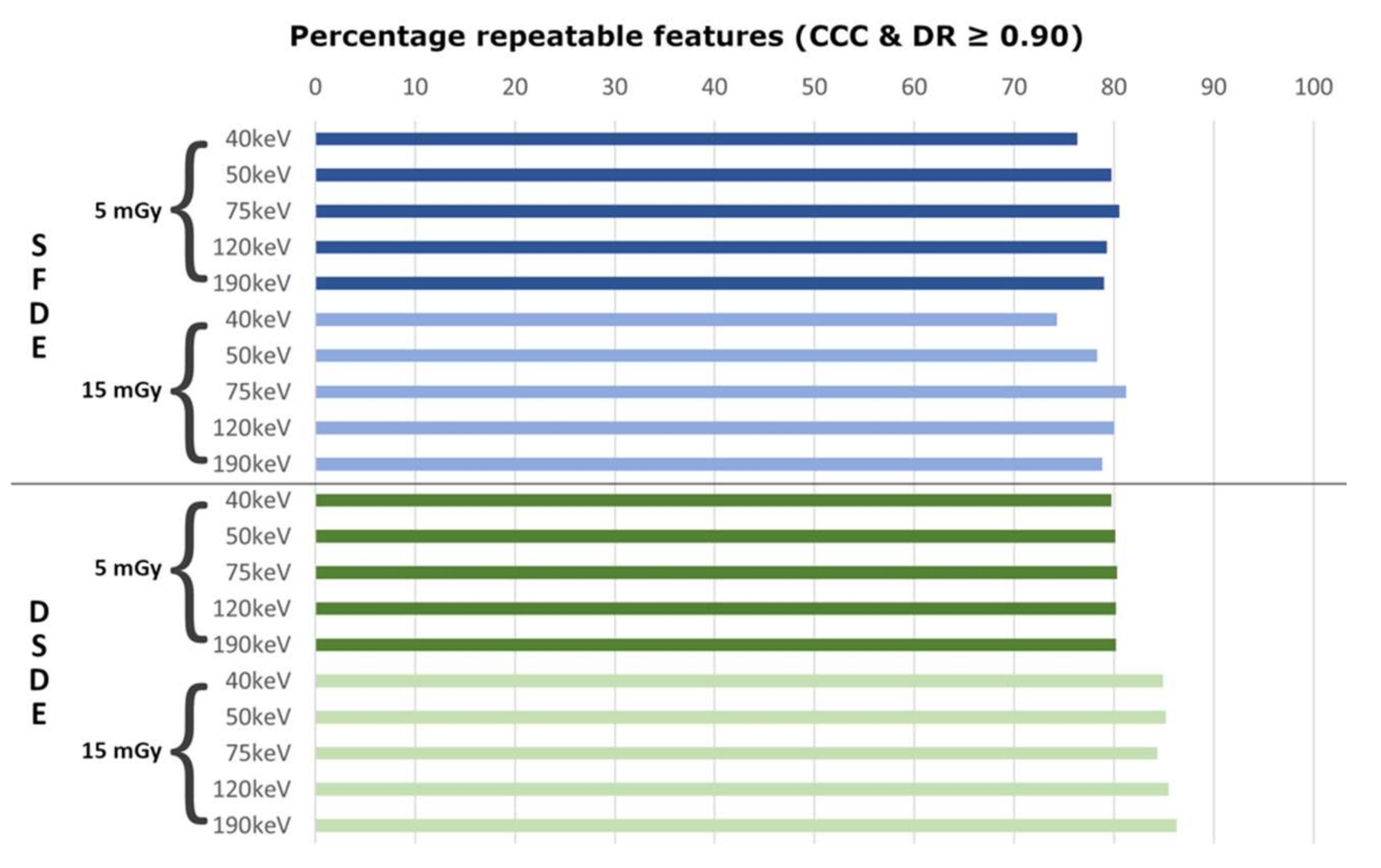
3.1.1. Test–Retest Repeatability of Radiomic Features
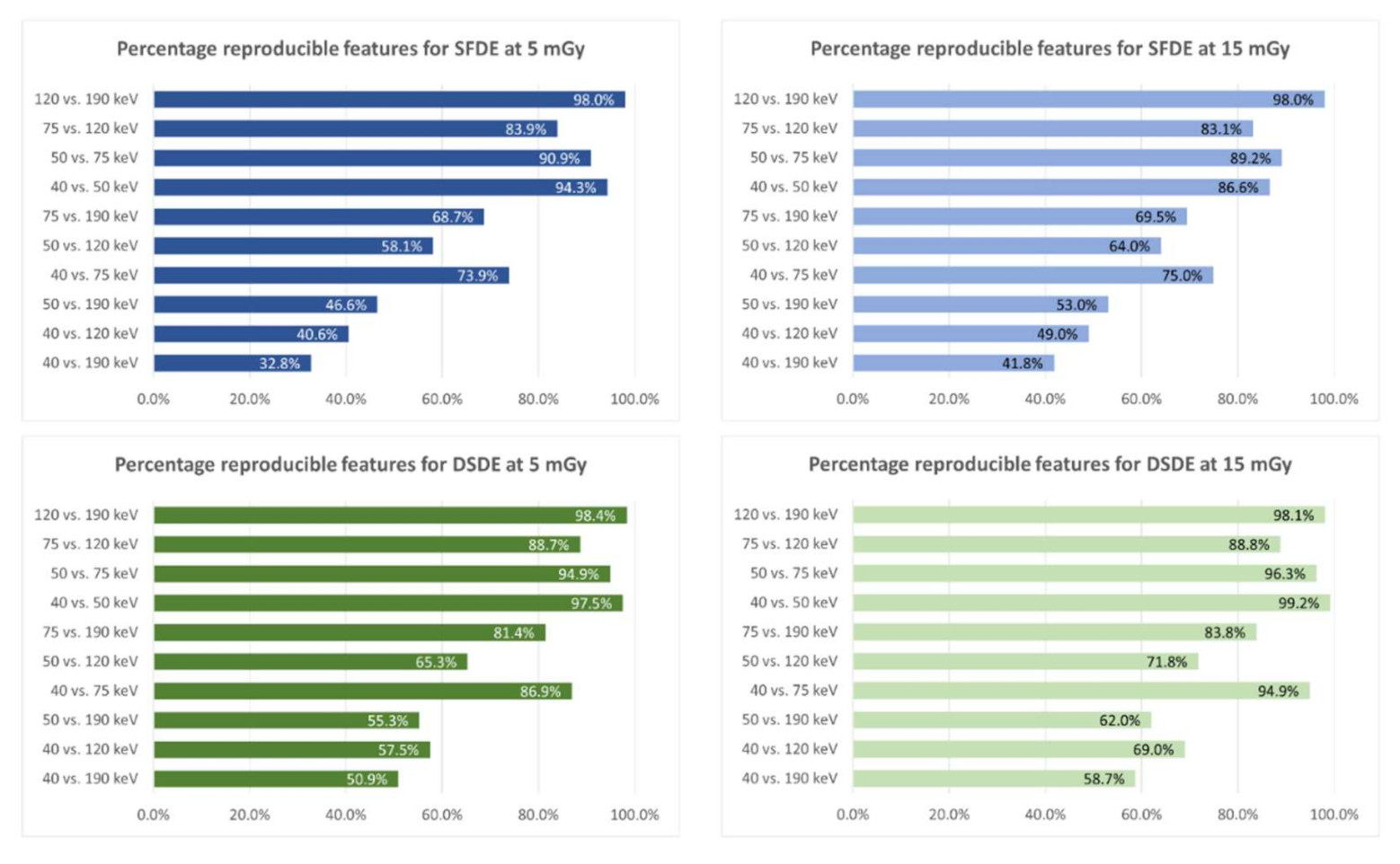
3.1.2. Reproducibility of Radiomic Features
3.1.3. Impact on Machine Learning Classification
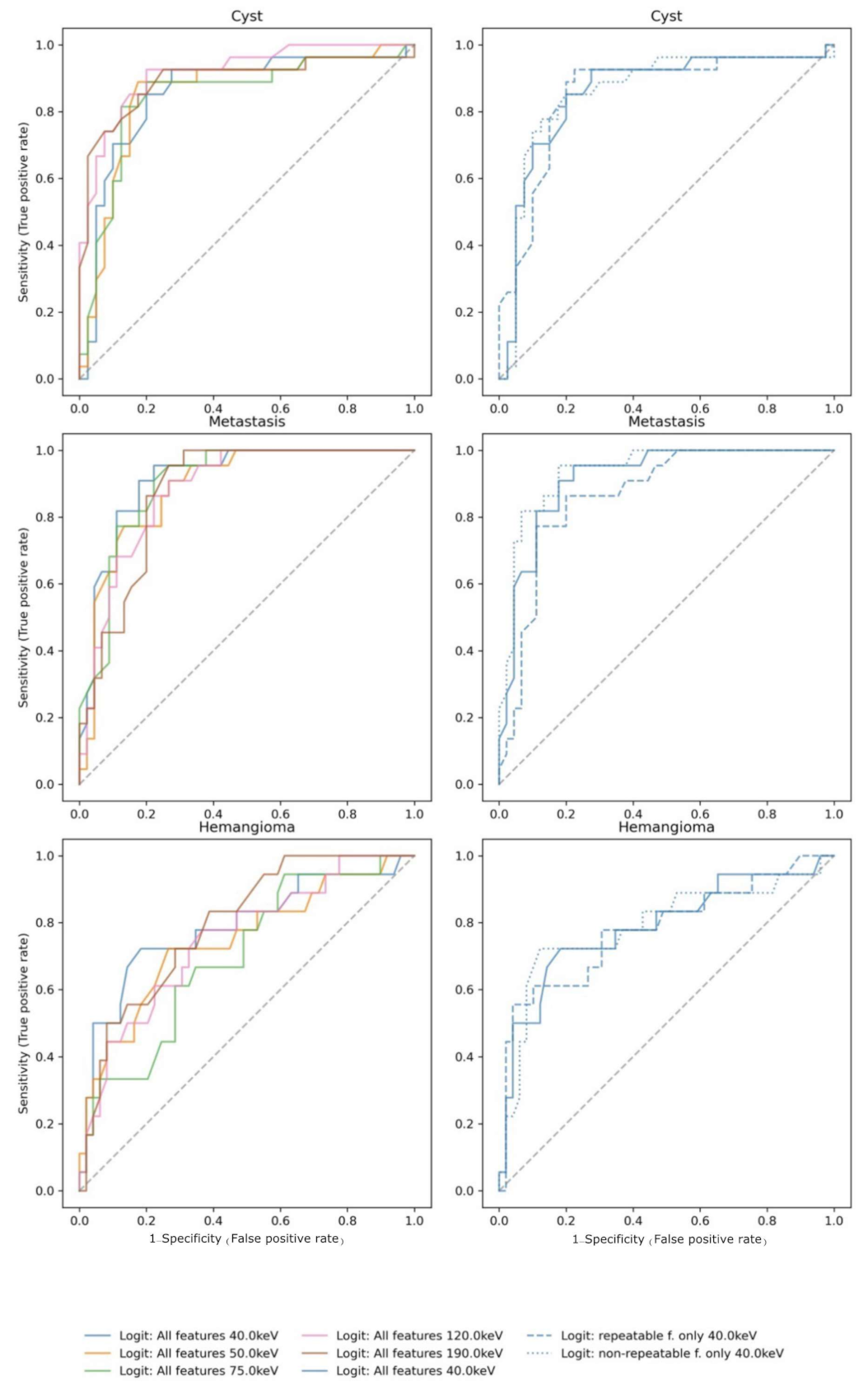
3.2. Part II—In Vivo
4. Discussion
4.1. Radiomic Feature Repeatability and Reproducibility
4.2. Impact on Machine Learning Classification
4.3. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Canellas, R.; Burk, K.S.; Parakh, A.; Sahani, D.V. Prediction of Pancreatic Neuroendocrine Tumor Grade Based on CT Features and Texture Analysis. Am. J. Roentgenol. 2018, 210, 341–346. [Google Scholar] [CrossRef]
- Hu, J.; Zhao, Y.; Li, M.; Liu, Y.; Wang, F.; Weng, Q.; You, R.; Cao, D. Machine-Learning-Based Computed Tomography Radiomic Analysis for Histologic Subtype Classification of Thymic Epithelial Tumours. Eur. J. Radiol. 2020, 126, 108929. [Google Scholar] [CrossRef] [PubMed]
- Ji, G.-W.; Zhu, F.-P.; Xu, Q.; Wang, K.; Wu, M.-Y.; Tang, W.-W.; Li, X.-C.; Wang, X.-H. Radiomic Features at Contrast-Enhanced CT Predict Recurrence in Early Stage Hepatocellular Carcinoma: A Multi-Institutional Study. Radiology 2020, 294, 568–579. [Google Scholar] [CrossRef]
- Mannil, M.; Kato, K.; Manka, R.; von Spiczak, J.; Peters, B.; Cammann, V.L.; Kaiser, C.; Osswald, S.; Nguyen, T.H.; Horowitz, J.D.; et al. Prognostic Value of Texture Analysis from Cardiac Magnetic Resonance Imaging in Patients with Takotsubo Syndrome: A Machine Learning Based Proof-of-Principle Approach. Sci. Rep. 2020, 10, 20537. [Google Scholar] [CrossRef]
- Mannil, M.; von Spiczak, J.; Hermanns, T.; Poyet, C.; Alkadhi, H.; Fankhauser, C.D. Three-Dimensional Texture Analysis with Machine Learning Provides Incremental Predictive Information for Successful Shock Wave Lithotripsy in Patients with Kidney Stones. J. Urol. 2018, 200, 829–836. [Google Scholar] [CrossRef]
- Li, H.; Zhang, R.; Wang, S.; Fang, M.; Zhu, Y.; Hu, Z.; Dong, D.; Shi, J.; Tian, J. CT-Based Radiomic Signature as a Prognostic Factor in Stage IV ALK-Positive Non-Small-Cell Lung Cancer Treated With TKI Crizotinib: A Proof-of-Concept Study. Front. Oncol. 2020, 10, 57. [Google Scholar] [CrossRef] [Green Version]
- Vaidya, P.; Bera, K.; Gupta, A.; Wang, X.; Corredor, G.; Fu, P.; Beig, N.; Prasanna, P.; Patil, P.D.; Velu, P.D.; et al. CT Derived Radiomic Score for Predicting the Added Benefit of Adjuvant Chemotherapy Following Surgery in Stage I, II Resectable Non-Small Cell Lung Cancer: A Retrospective Multicohort Study for Outcome Prediction. Lancet Digit. Health 2020, 2, e116–e128. [Google Scholar] [CrossRef] [Green Version]
- Tian, X.; Sun, C.; Liu, Z.; Li, W.; Duan, H.; Wang, L.; Fan, H.; Li, M.; Li, P.; Wang, L.; et al. Prediction of Response to Preoperative Neoadjuvant Chemotherapy in Locally Advanced Cervical Cancer Using Multicenter CT-Based Radiomic Analysis. Front. Oncol. 2020, 10, 77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, X.Z.; Wu, Z.Y.; Tao, R.; Guo, Y.; Li, J.Y.; Zhang, J.; Chen, K.M. Dual Energy Spectral CT Imaging of Insulinoma-Value in Preoperative Diagnosis Compared with Conventional Multi-Detector CT. Eur. J. Radiol. 2012, 81, 2487–2494. [Google Scholar] [CrossRef] [PubMed]
- Shuman, W.P.; Green, D.E.; Busey, J.M.; Mitsumori, L.M.; Choi, E.; Koprowicz, K.M.; Kanal, K.M. Dual-Energy Liver CT: Effect of Monochromatic Imaging on Lesion Detection, Conspicuity, and Contrast-to-Noise Ratio of Hypervascular Lesions on Late Arterial Phase. AJR Am. J. Roentgenol. 2014, 203, 601–606. [Google Scholar] [CrossRef] [PubMed]
- Parakh, A.; Patino, M.; Muenzel, D.; Kambadakone, A.; Sahani, D.V. Role of Rapid KV-Switching Dual-Energy CT in Assessment of Post-Surgical Local Recurrence of Pancreatic Adenocarcinoma. Abdom. Radiol. N. Y. 2018, 43, 497–504. [Google Scholar] [CrossRef] [PubMed]
- De Cecco, C.N.; Boll, D.T.; Bolus, D.N.; Foley, W.D.; Kaza, R.K.; Morgan, D.E.; Rofsky, N.M.; Sahani, D.V.; Schoepf, U.J.; Shuman, W.P.; et al. White Paper of the Society of Computed Body Tomography and Magnetic Resonance on Dual-Energy CT, Part 4: Abdominal and Pelvic Applications. J. Comput. Assist. Tomogr. 2017, 41, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Patel, B.N.; Alexander, L.; Allen, B.; Berland, L.; Borhani, A.; Mileto, A.; Moreno, C.; Morgan, D.; Sahani, D.; Shuman, W.; et al. Dual-Energy CT Workflow: Multi-Institutional Consensus on Standardization of Abdominopelvic MDCT Protocols. Abdom. Radiol. 2017, 42, 676–687. [Google Scholar] [CrossRef]
- Bae, J.M.; Jeong, J.Y.; Lee, H.Y.; Sohn, I.; Kim, H.S.; Son, J.Y.; Kwon, O.J.; Choi, J.Y.; Lee, K.S.; Shim, Y.M. Pathologic Stratification of Operable Lung Adenocarcinoma Using Radiomics Features Extracted from Dual Energy CT Images. Oncotarget 2017, 8. [Google Scholar] [CrossRef] [Green Version]
- Al Ajmi, E.; Forghani, B.; Reinhold, C.; Bayat, M.; Forghani, R. Spectral Multi-Energy CT Texture Analysis with Machine Learning for Tissue Classification: An Investigation Using Classification of Benign Parotid Tumours as a Testing Paradigm. Eur. Radiol. 2018, 28, 2604–2611. [Google Scholar] [CrossRef] [PubMed]
- Seidler, M.; Forghani, B.; Reinhold, C.; Pérez-Lara, A.; Romero-Sanchez, G.; Muthukrishnan, N.; Wichmann, J.L.; Melki, G.; Yu, E.; Forghani, R. Dual-Energy CT Texture Analysis With Machine Learning for the Evaluation and Characterization of Cervical Lymphadenopathy. Comput. Struct. Biotechnol. J. 2019, 17, 1009–1015. [Google Scholar] [CrossRef] [PubMed]
- Forghani, R.; Chatterjee, A.; Reinhold, C.; Pérez-Lara, A.; Romero-Sanchez, G.; Ueno, Y.; Bayat, M.; Alexander, J.W.M.; Kadi, L.; Chankowsky, J.; et al. Head and Neck Squamous Cell Carcinoma: Prediction of Cervical Lymph Node Metastasis by Dual-Energy CT Texture Analysis with Machine Learning. Eur. Radiol. 2019, 29, 6172–6181. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Dou, Y.; Lu, F.; Liu, L. A Study of Radiomics Parameters from Dual-Energy Computed Tomography Images for Lymph Node Metastasis Evaluation in Colorectal Mucinous Adenocarcinoma. Medicine 2020, 99, e19251. [Google Scholar] [CrossRef]
- Zwanenburg, A.; Vallières, M.; Abdalah, M.A.; Aerts, H.J.W.L.; Andrearczyk, V.; Apte, A.; Ashrafinia, S.; Bakas, S.; Beukinga, R.J.; Boellaard, R.; et al. The Image Biomarker Standardization Initiative: Standardized Quantitative Radiomics for High-Throughput Image-Based Phenotyping. Radiology 2020, 295, 328–338. [Google Scholar] [CrossRef] [Green Version]
- Berenguer, R.; Pastor-Juan, M.D.R.; Canales-Vazquez, J.; Castro-Garcia, M.; Villas, M.V.; Mansilla Legorburo, F.; Sabater, S. Radiomics of CT Features May Be Nonreproducible and Redundant: Influence of CT Acquisition Parameters. Radiology 2018, 288, 407–415. [Google Scholar] [CrossRef] [Green Version]
- Meyer, M.; Ronald, J.; Vernuccio, F.; Nelson, R.C.; Ramirez-Giraldo, J.C.; Solomon, J.; Patel, B.N.; Samei, E.; Marin, D. Reproducibility of CT Radiomic Features within the Same Patient: Influence of Radiation Dose and CT Reconstruction Settings. Radiology 2019, 293, 583–591. [Google Scholar] [CrossRef] [PubMed]
- Park, B.W.; Kim, J.K.; Heo, C.; Park, K.J. Reliability of CT Radiomic Features Reflecting Tumour Heterogeneity According to Image Quality and Image Processing Parameters. Sci. Rep. 2020, 10, 3852. [Google Scholar] [CrossRef]
- van Timmeren, J.E.; Cester, D.; Tanadini-Lang, S.; Alkadhi, H.; Baessler, B. Radiomics in Medical Imaging—“How-to” Guide and Critical Reflection. Insights Imaging 2020, 11, 91. [Google Scholar] [CrossRef] [PubMed]
- Milanese, G.; Mannil, M.; Martini, K.; Maurer, B.; Alkadhi, H.; Frauenfelder, T. Quantitative CT Texture Analysis for Diagnosing Systemic Sclerosis: Effect of Iterative Reconstructions and Radiation Doses. Medicine 2019, 98, e16423. [Google Scholar] [CrossRef] [PubMed]
- Mannil, M.; von Spiczak, J.; Muehlematter, U.J.; Thanabalasingam, A.; Keller, D.I.; Manka, R.; Alkadhi, H. Texture Analysis of Myocardial Infarction in CT: Comparison with Visual Analysis and Impact of Iterative Reconstruction. Eur. J. Radiol. 2019, 113, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Baliyan, V.; Kordbacheh, H.; Parameswaran, B.; Ganeshan, B.; Sahani, D.; Kambadakone, A. Virtual Monoenergetic Imaging in Rapid KVp-Switching Dual-Energy CT (DECT) of the Abdomen: Impact on CT Texture Analysis. Abdom. Radiol. 2018, 43, 2693–2701. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Sánchez, N.; Moreda, G.P.; Herre-ro-Langreo, A.; Melado-Herreros, Á. Assessment of Internal and External Quality of Fruits and Vegetables. In Imaging Technologies and Data Processing for Food Engineers; Sozer, N., Ed.; Food Engineering Series; Springer International Publishing: Cham, Switzerland, 2016; pp. 269–309. ISBN 978-3-319-24735-9. [Google Scholar]
- van Griethuysen, J.J.M.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.H.; Fillion-Robin, J.-C.; Pieper, S.; Aerts, H.J.W.L. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef] [Green Version]
- Balagurunathan, Y.; Kumar, V.; Gu, Y.; Kim, J.; Wang, H.; Liu, Y.; Goldgof, D.B.; Hall, L.O.; Korn, R.; Zhao, B.; et al. Test–Retest Reproducibility Analysis of Lung CT Image Features. J. Digit. Imaging 2014, 27, 805–823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, B.; Tan, Y.; Tsai, W.-Y.; Qi, J.; Xie, C.; Lu, L.; Schwartz, L.H. Reproducibility of Radiomics for Deciphering Tumor Phenotype with Imaging. Sci. Rep. 2016, 6, 23428. [Google Scholar] [CrossRef] [Green Version]
- Baeßler, B.; Weiss, K.; Pinto dos Santos, D. Robustness and Reproducibility of Radiomics in Magnetic Resonance Imaging: A Phantom Study. Investig. Radiol. 2019, 54, 221–228. [Google Scholar] [CrossRef]
- Akoglu, H. User’s Guide to Correlation Coefficients. Turk. J. Emerg. Med. 2018, 18, 91–93. [Google Scholar] [CrossRef] [PubMed]
- RStudio Team. RStudio: Integrated Development for R; RStudio, PBC: Boston, MA, USA, 2020. [Google Scholar]
- Wickham, H.; Averick, M.; Bryan, J.; Chang, W.; McGowan, L.D.; François, R.; Grolemund, G.; Hayes, A.; Henry, L.; Hester, J.; et al. Welcome to the Tidyverse. J. Open Source Softw. 2019, 4, 1686. [Google Scholar] [CrossRef]
- Comtois, D. Summarytools: Tools to Quickly and Neatly Summarize Data. 2019. software package. Available online: https://github.com/dcomtois/summarytools (accessed on 22 April 2021).
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016; ISBN 978-3-319-24277-4. [Google Scholar]
- Signorell, A. DescTools: Tools for Descriptive Statistics. 2019. R package version 0.99.43. Available online: https://cran.r-project.org/package=DescTools (accessed on 22 April 2021).
- Hothorn, T.; Bretz, F.; Westfall, P. Simultaneous Inference in General Parametric Models. Biom. J. 2008, 50, 346–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-learn: Machine Learning in {P}ython. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Montoya Perez, I.; Airola, A.; Boström, P.J.; Jambor, I.; Pahikkala, T. Tournament Leave-Pair-out Cross-Validation for Receiver Operating Characteristic Analysis. Stat. Methods Med. Res. 2019, 28, 2975–2991. [Google Scholar] [CrossRef]
- Tsamardinos, I.; Greasidou, E.; Borboudakis, G. Bootstrapping the Out-of-Sample Predictions for Efficient and Accurate Cross-Validation. Mach. Learn. 2018, 107, 1895–1922. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lv, W.; Yuan, Q.; Wang, Q.; Ma, J.; Jiang, J.; Yang, W.; Feng, Q.; Chen, W.; Rahmim, A.; Lu, L. Robustness versus Disease Differentiation When Varying Parameter Settings in Radiomics Features: Application to Nasopharyngeal PET/CT. Eur. Radiol. 2018, 28, 3245–3254. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Subjects (n = 72) | |
|---|---|
| Sex | 33 male, 39 female |
| Age | 66 ± 12 years |
| Final diagnoses | Lung cancer (n = 12) Colon cancer (n = 11) Kidney cancer (n = 9) Rectal cancer (n = 5) Sarcoma (n = 5) Leukemia (n = 4) Pancreatic cancer (n = 3) Breast cancer (n = 3) Peritoneal cancer (n = 3) Ovarian cancer (n = 3) Esophageal cancer (n = 2) Pleural mesothelioma (n = 2) Prostate cancer (n = 1) Gastrointestinal stromal tumor (n = 1) Stomach cancer (n = 1) Other (n = 7) |
| Model | Features | Energy (keV) | AUC | Brier Score (BS) | R2 (Scaled BS) |
|---|---|---|---|---|---|
| Penalized Logistic Regression | all | 40 | 0.84 (0.95; 0.72) | 0.45 (0.29; 0.69) | 0.29 (−0.11; 0.54) |
| 50 | 0.82 (0.93; 0.69) | 0.48 (0.32; 0.73) | 0.25 (−0.15; 0.49) | ||
| 75 | 0.80 (0.92; 0.70) | 0.50 (0.33; 0.76) | 0.22 (−0.18; 0.48) | ||
| 120 | 0.85 (0.94; 0.75) | 0.43 (0.31; 0.57) | 0.32 (0.11; 0.50) | ||
| 190 | 0.84 (0.94; 0.71) | 0.45 (0.32; 0.63) | 0.29 (0.026; 0.49) | ||
| repeatable | 40 | 0.81 (0.93; 0.68) | 0.50 (0.34; 0.72) | 0.22 (−0.13; 0.46) | |
| 50 | 0.84 (0.94; 0.72) | 0.45 (0.27; 0.65) | 0.29 (−0.0076; 0.57) | ||
| 75 | 0.81 (0.92; 0.69) | 0.50 (0.33; 0.69) | 0.22 (−0.091; 0.48) | ||
| 120 | 0.79 (0.91; 0.67) | 0.51 (0.36; 0.70) | 0.21 (−0.095; 0.43) | ||
| 190 | 0.80 (0.91; 0.66) | 0.51 (0.36; 0.70) | 0.20 (−0.079; 0.42) | ||
| non-repeatable | 40 | 0.84 (0.96; 0.72) | 0.45 (0.28; 0.71) | 0.29 (−0.13; 0.55) | |
| 50 | 0.81 (0.93; 0.68) | 0.48 (0.33; 0.68) | 0.25 (−0.063; 0.48) | ||
| 75 | 0.80 (0.92; 0.69) | 0.50 (0.34; 0.74) | 0.22 (−0.15; 0.46) | ||
| 120 | 0.84 (0.94; 0.73) | 0.45 (0.33; 0.57) | 0.30 (0.11; 0.48) | ||
| 190 | 0.83 (0.93; 0.70) | 0.47 (0.34; 0.65) | 0.27 (−0.0039; 0.46) | ||
| Random Forest | all | 40 | 0.84 (0.94; 0.72) | 0.45 (0.33; 0.58) | 0.30 (0.086; 0.47) |
| 50 | 0.85 (0.94; 0.74) | 0.45 (0.34; 0.59) | 0.30 (0.089; 0.47) | ||
| 75 | 0.81 (0.92; 0.69) | 0.48 (0.36; 0.62) | 0.25 (0.04; 0.43) | ||
| 120 | 0.80 (0.92; 0.67) | 0.49 (0.37; 0.63) | 0.23 (0.026; 0.41) | ||
| 190 | 0.79 (0.91; 0.66) | 0.50 (0.38; 0.64) | 0.21 (0.016; 0.38) | ||
| repeatable | 40 | 0.83 (0.93; 0.72) | 0.47 (0.35; 0.61) | 0.27 (0.038; 0.46) | |
| 50 | 0.82 (0.93; 0.71) | 0.48 (0.36; 0.62) | 0.25 (0.016; 0.43) | ||
| 75 | 0.80 (0.91; 0.68) | 0.50 (0.37; 0.64) | 0.22 (−0.0043; 0.41) | ||
| 120 | 0.79 (0.90; 0.66) | 0.51 (0.37; 0.65) | 0.20 (−0.0044; 0.39) | ||
| 190 | 0.77 (0.88; 0.64) | 0.53 (0.41; 0.67) | 0.17 (−0.037; 0.36) | ||
| non-repeatable | 40 | 0.85 (0.94; 0.74) | 0.46 (0.35; 0.57) | 0.29 (0.092; 0.44) | |
| 50 | 0.86 (0.94; 0.75) | 0.44 (0.34; 0.56) | 0.31 (0.11; 0.46) | ||
| 75 | 0.82 (0.92; 0.72) | 0.47 (0.36; 0.59) | 0.26 (0.08; 0.42) | ||
| 120 | 0.81 (0.92; 0.68) | 0.49 (0.38; 0.62) | 0.24 (0.051; 0.4) | ||
| 190 | 0.81 (0.92; 0.68) | 0.49 (0.38; 0.61) | 0.23 (0.05; 0.39) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Euler, A.; Laqua, F.C.; Cester, D.; Lohaus, N.; Sartoretti, T.; Pinto dos Santos, D.; Alkadhi, H.; Baessler, B. Virtual Monoenergetic Images of Dual-Energy CT—Impact on Repeatability, Reproducibility, and Classification in Radiomics. Cancers 2021, 13, 4710. https://doi.org/10.3390/cancers13184710
Euler A, Laqua FC, Cester D, Lohaus N, Sartoretti T, Pinto dos Santos D, Alkadhi H, Baessler B. Virtual Monoenergetic Images of Dual-Energy CT—Impact on Repeatability, Reproducibility, and Classification in Radiomics. Cancers. 2021; 13(18):4710. https://doi.org/10.3390/cancers13184710
Chicago/Turabian StyleEuler, André, Fabian Christopher Laqua, Davide Cester, Niklas Lohaus, Thomas Sartoretti, Daniel Pinto dos Santos, Hatem Alkadhi, and Bettina Baessler. 2021. "Virtual Monoenergetic Images of Dual-Energy CT—Impact on Repeatability, Reproducibility, and Classification in Radiomics" Cancers 13, no. 18: 4710. https://doi.org/10.3390/cancers13184710