
Feasibility and Short-Term Outcomes of Three-Dimensional Hand-Sewn Esophago-Jejunal Anastomosis in Completely Laparoscopic Total Gastrectomy for Cancer

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract

1. Introduction
2. Materials and Methods
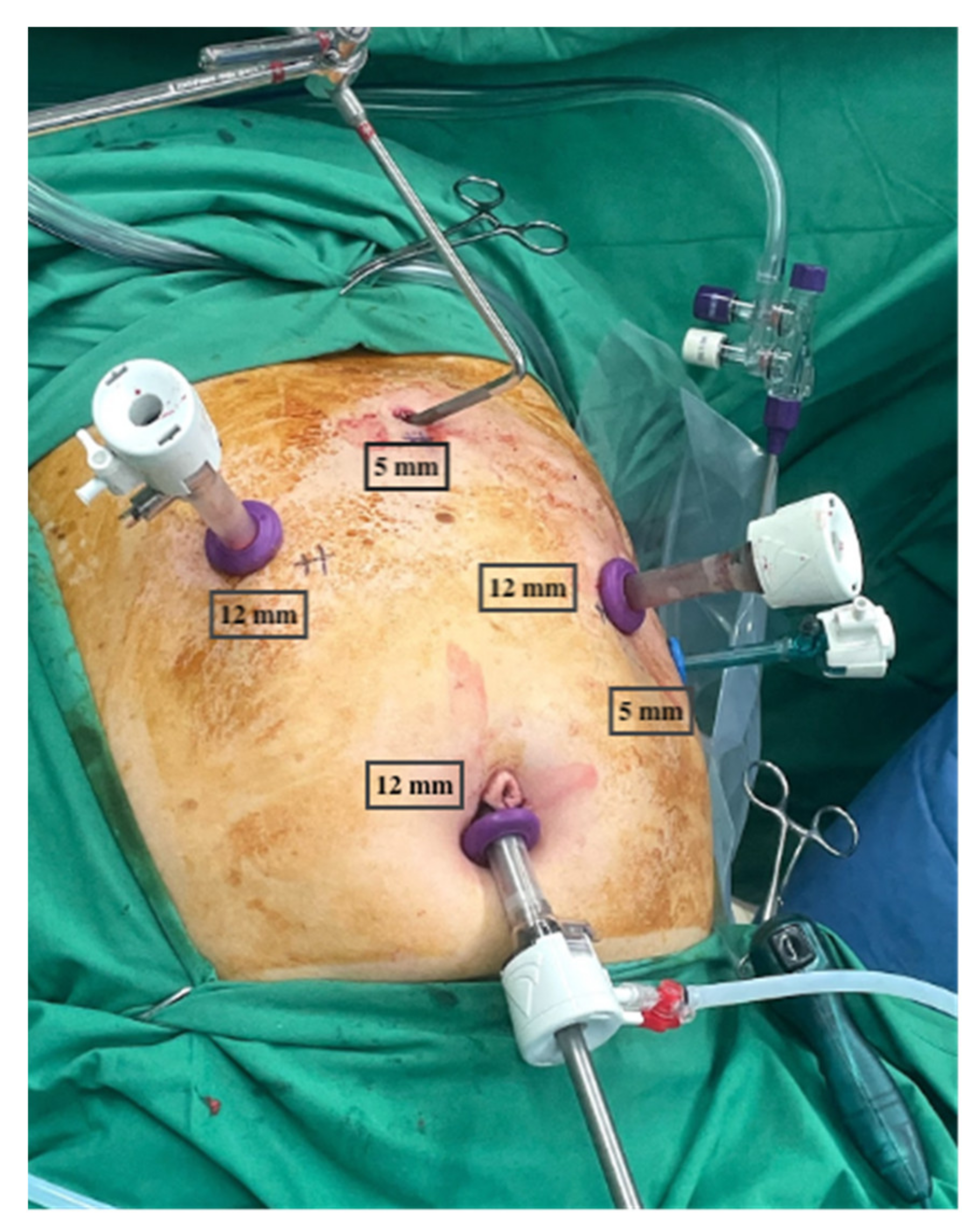
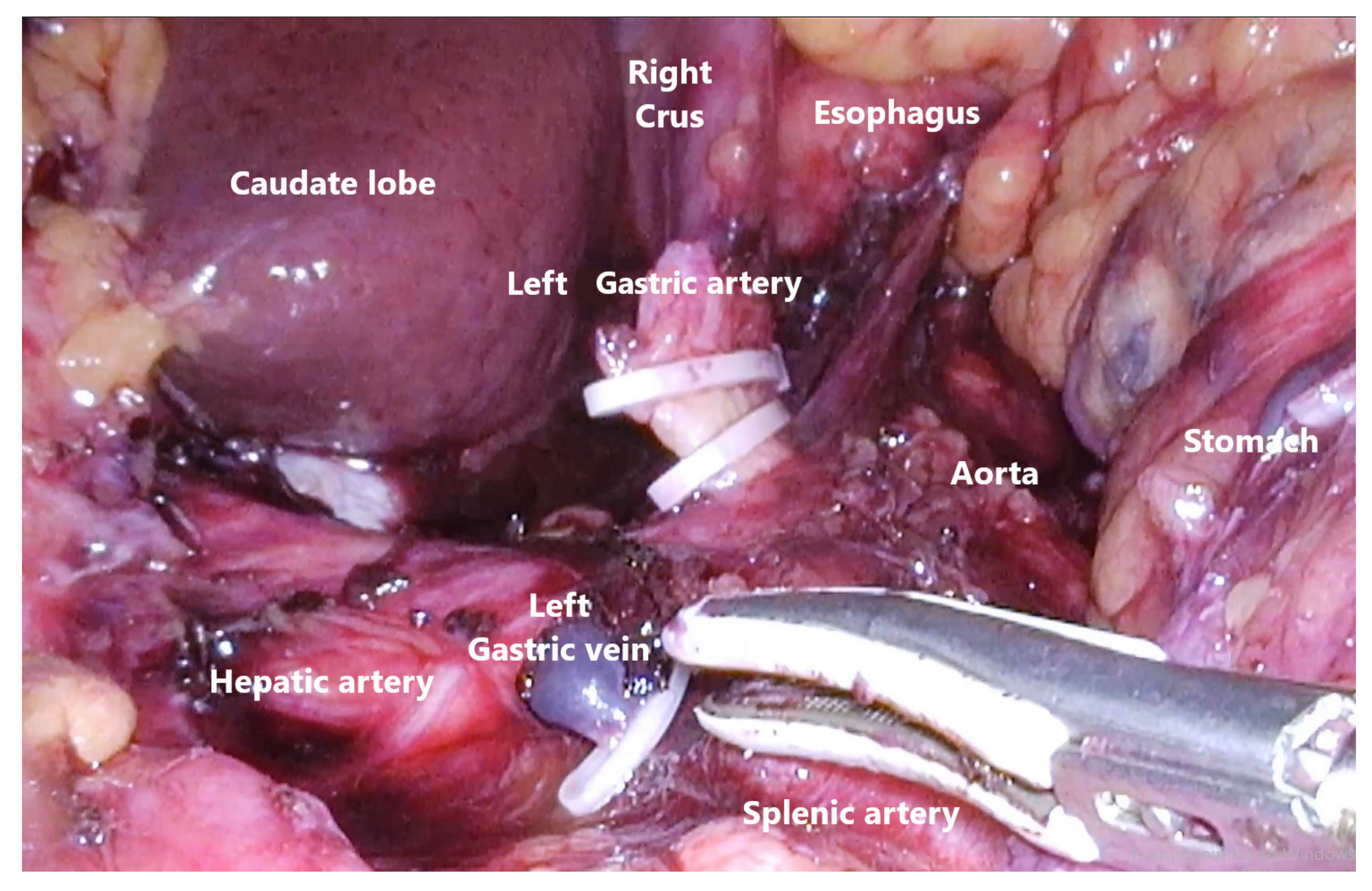
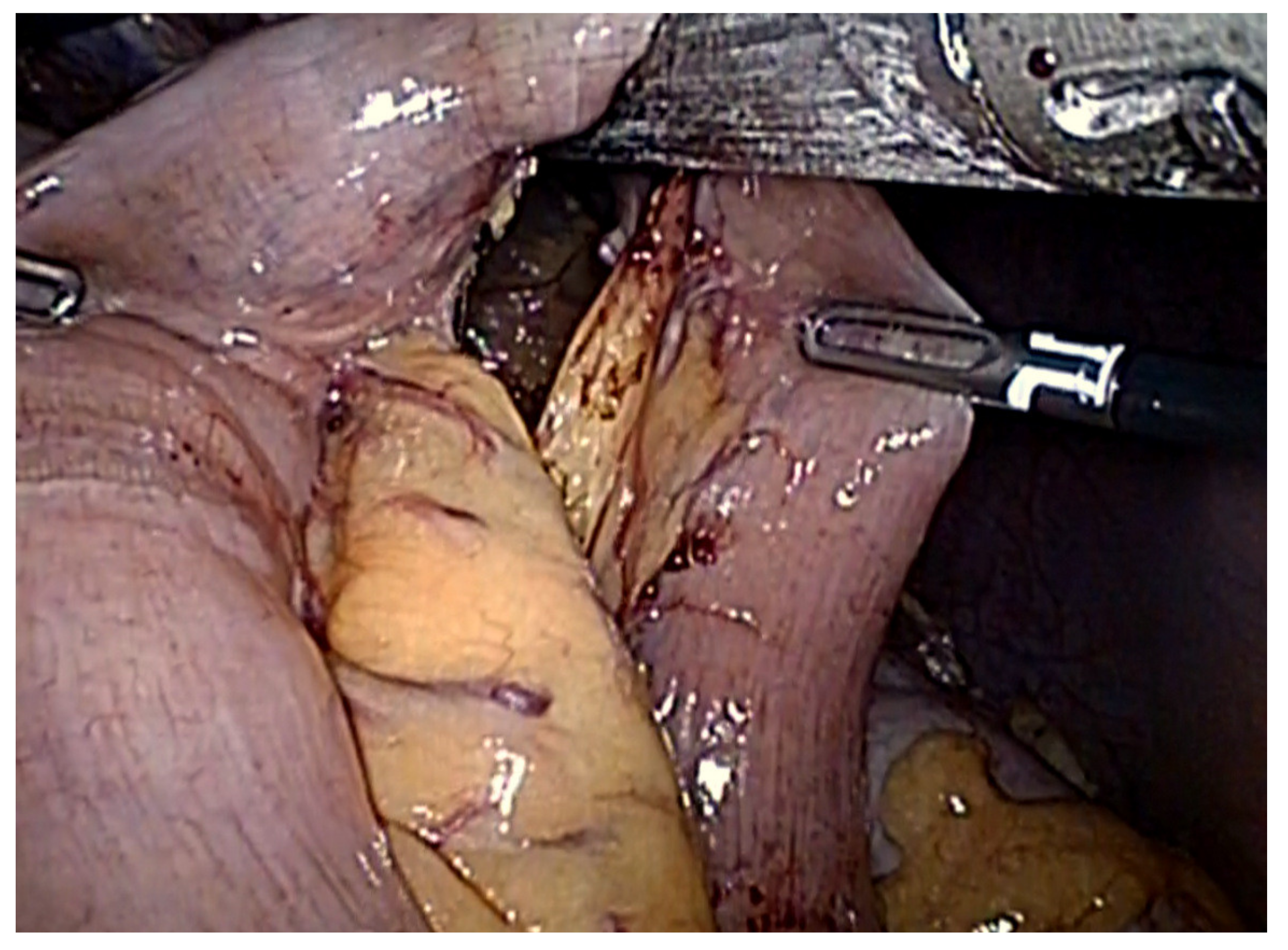
2.1. Laparoscopic Gastric Mobilization and D2 Lymphadenectomy
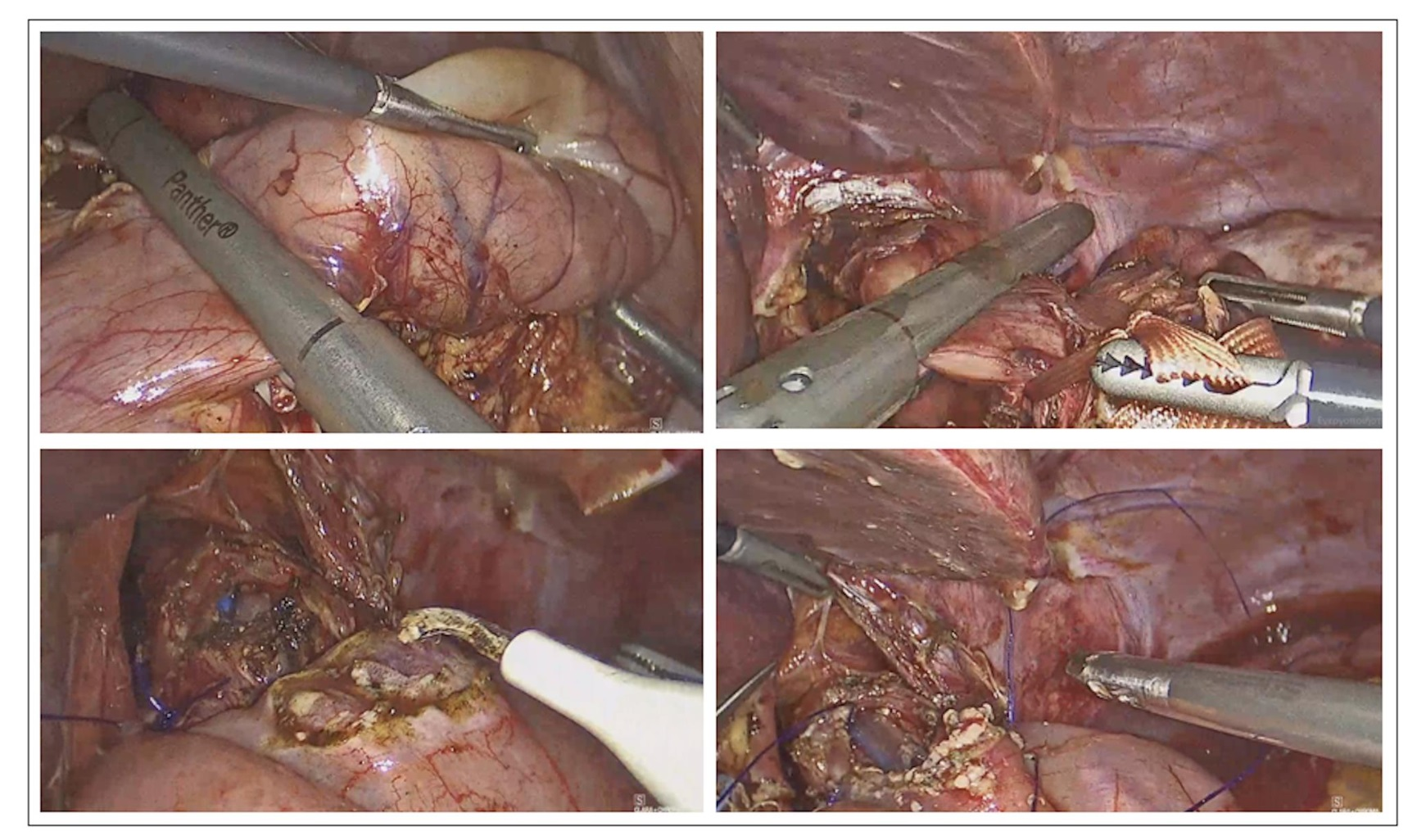
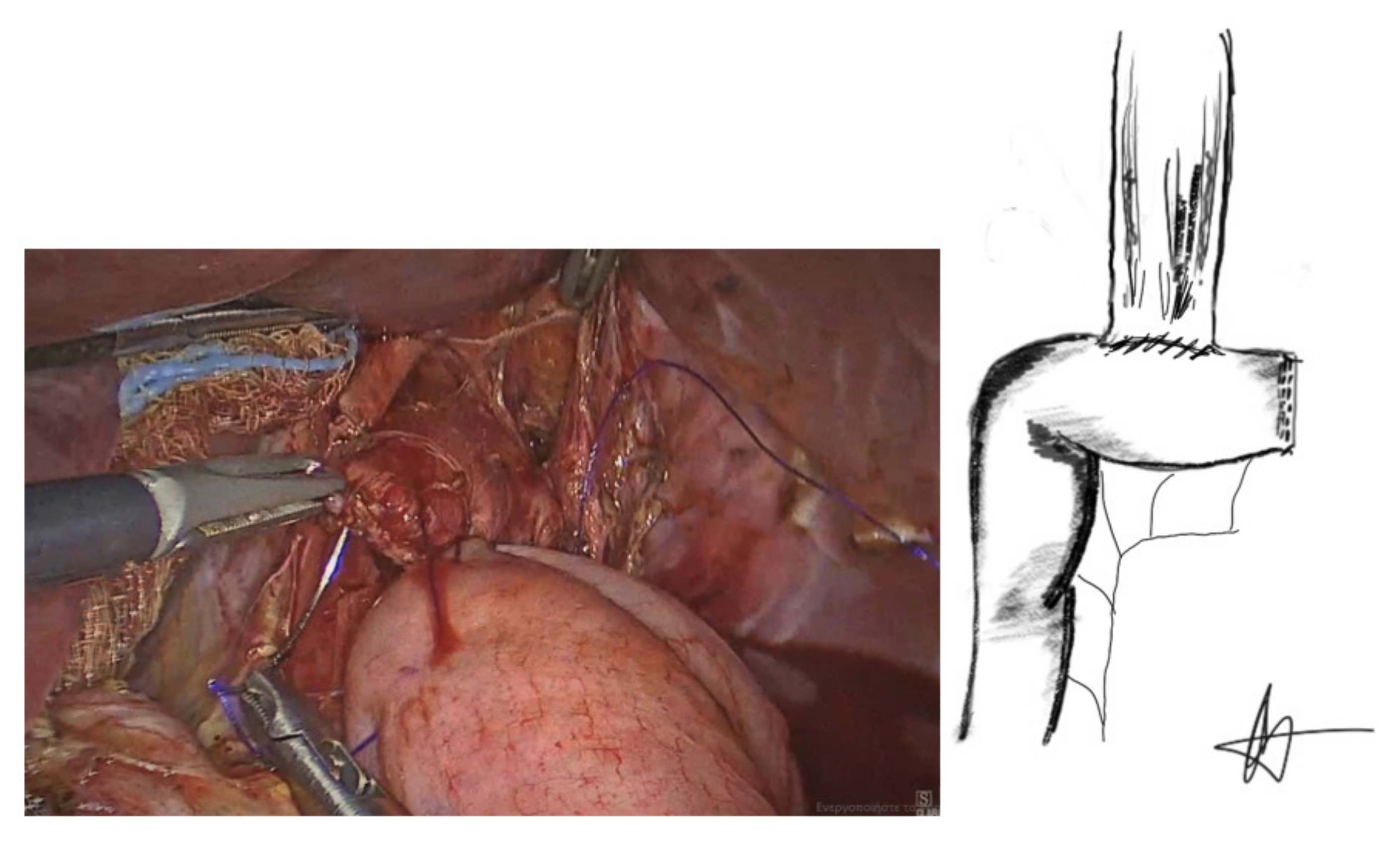
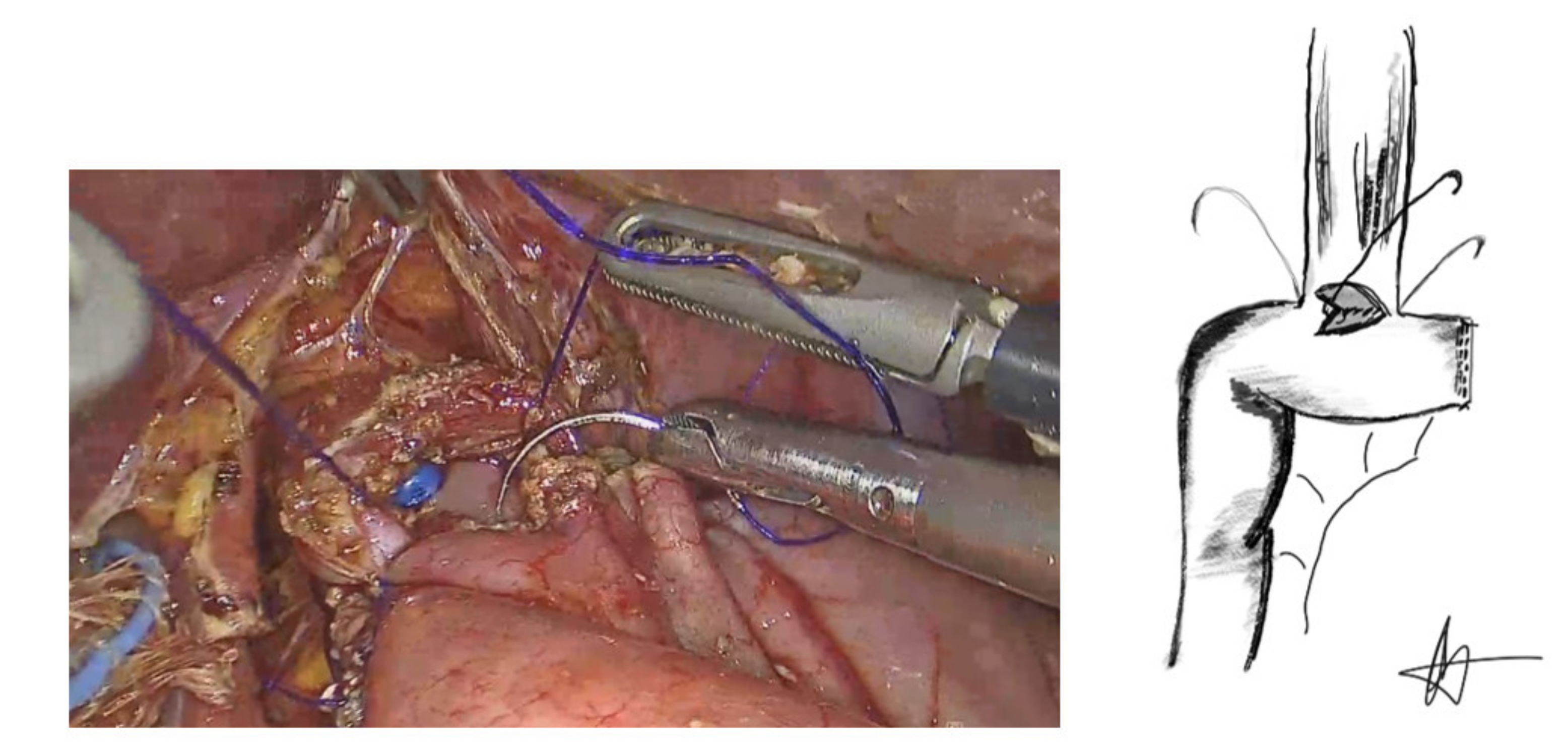
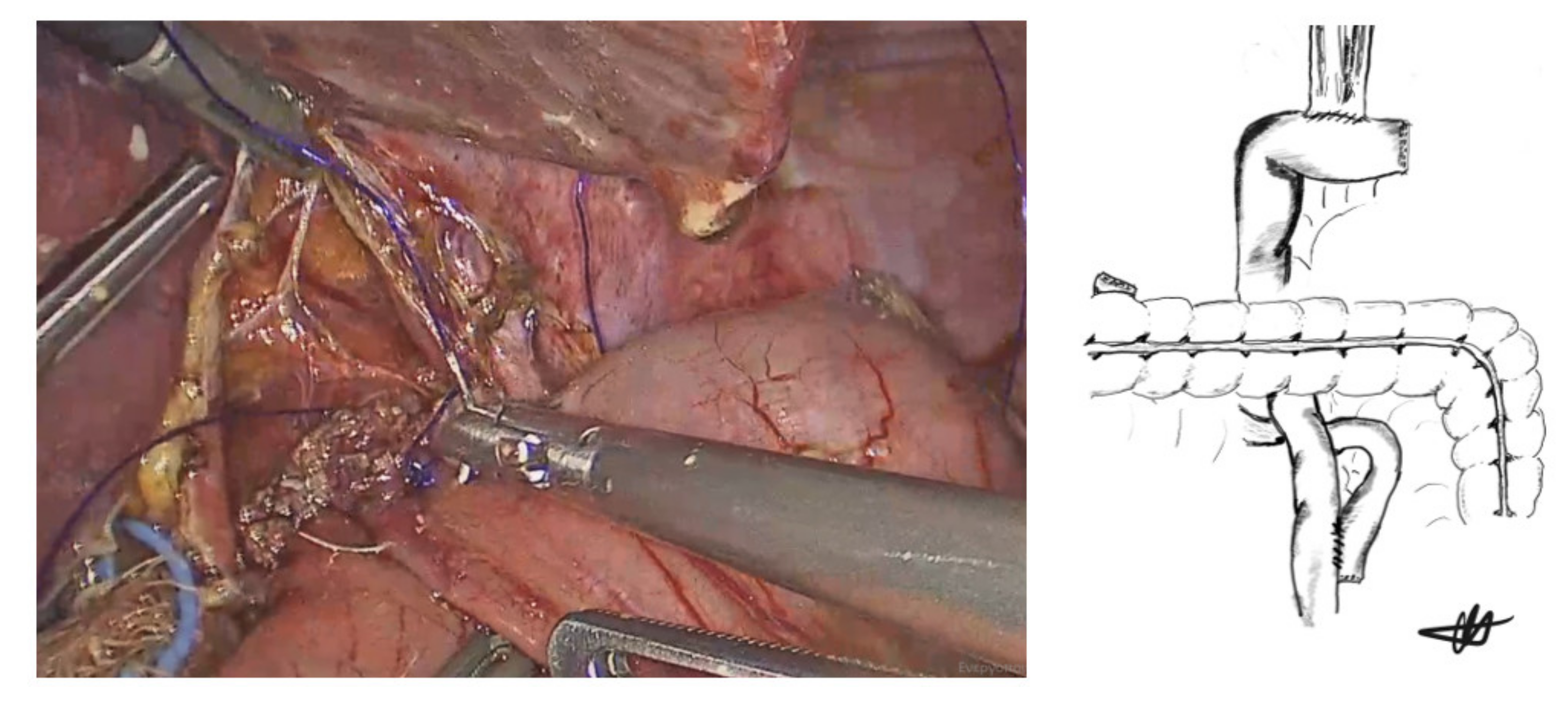
2.2. Laparoscopic Hand-Sewn Esophago-Jejunal Anastomosis
2.3. Postoperative Course
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Machlowska, J.; Baj, J.; Sitarz, M.; Maciejewski, R.; Sitarz, R. Gastric cancer: Epidemiology, risk factors, classification, genomic characteristics and treatment strategies. Int. J. Mol. Sci. 2020, 21, 4012. [Google Scholar] [CrossRef]
- Fuchs, C.S.; Muro, K.; Tomasek, J.; Van Cutsem, E.; Cho, J.Y.; Oh, S.C.; Safran, H.; Bodoky, G.; Chau, I.; Shimada, Y.; et al. Prognostic factor analysis of overall survival in gastric cancer from two phase III studies of second-line ramucirumab (REGARD and RAINBOW) using pooled patient data. J. Gastric Cancer 2017, 17, 132–144. [Google Scholar] [CrossRef] [Green Version]
- Ohgami, M.; Kumai, K.; Otani, Y.; Wakabayashi, G.; Kubota, T.; Kitajima, M. Laparoscopic wedge resection of the stomach for early gastric cancer using a lesion-lifting method. Dig. Surg. 1994, 11, 64–67. [Google Scholar] [CrossRef]
- Goh, P.; Tekant, Y.; Isaac, J.; Kum, C.K.; Ngoi, S.S. The technique of laparoscopic Billroth II gastrectomy. Surg. Laparosc. Endosc. Percutaneous Tech. 1992, 2, 258–260. [Google Scholar]
- Azagra, J.S.; Goergen, M.; De Simone, P.; Ibañez-Aguirre, J. Minimally invasive surgery for gastric cancer. Surg. Endosc. 1999, 13, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Parisi, A.; Reim, D.; Borghi, F.; Nguyen, N.T.; Qi, F.; Coratti, A.; Cianchi, F.; Cesari, M.; Bazzocchi, F.; Alimoglu, O.; et al. Minimally invasive surgery for gastric cancer: A comparison between robotic, laparoscopic and open surgery. World J. Gastroenterol. 2017, 23, 2376–2384. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Huang, C.; Sun, Y.; Su, X.; Cao, H.; Hu, J.; Wang, K.; Suo, J.; Tao, K.; He, X.; et al. Effect of laparoscopic vs open distal gastrectomy on 3-year disease-free survival in patients with locally advanced gastric cancer: The CLASS-01 randomized clinical trial. JAMA 2019, 321, 1983–1992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, H.; Myung, J.-E.; Yi, J.W.; Lee, S.-S.; Park, J. Laparoscopic surgery versus open surgery for gastric cancer: Big data analysis based on nationwide administrative claims data. Ann. Surg. Treat. Res. 2020, 99, 138–145. [Google Scholar] [CrossRef]
- Jung, D.H.; Son, S.-Y.; Park, Y.S.; Shin, D.J.; Ahn, H.S.; Ahn, S.-H.; Park, D.J.; Kim, H.-H. The learning curve associated with laparoscopic total gastrectomy. Gastric Cancer 2014, 19, 264–272. [Google Scholar] [CrossRef] [PubMed]
- Xiong, J.J.; Nunes, Q.M.; Huang, W.; Tan, C.L.; Ke, N.W.; Xie, S.M.; Ran, X.; Zhang, H.; Chen, Y.-H.; Liu, X.B. Laparoscopic vs. open total gastrectomy for gastric cancer: A meta-analysis. World J. Gastroenterol. 2013, 19, 8114–8132. [Google Scholar] [CrossRef] [PubMed]
- Kunisaki, C.; Makino, H.; Oshima, T.; Fujii, S.; Kimura, J.; Takagawa, R.; Kosaka, T.; Akiyama, H.; Morita, S.; Endo, I. Application of the transorally inserted anvil (OrVil) after laparoscopy-assisted total gastrectomy. Surg. Endosc. 2010, 25, 1300–1305. [Google Scholar] [CrossRef]
- Inokuchi, M.; Otsuki, S.; Fujimori, Y.; Sato, Y.; Nakagawa, M.; Kojima, K. Systematic review of anastomotic complications of esophagojejunostomy after laparoscopic total gastrectomy. World J. Gastroenterol. 2015, 21, 9656–9665. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-W.; Kawai, M.; Tashiro, K.; Kawashima, S.; Tanaka, R.; Tanaka, K.; Nomura, E.; Uchiyama, K. The crossover technique for intracorporeal esophagojejunostomy following laparoscopic total gastrectomy: A simple and safe technique using a linear stapler and two barbed sutures. Surg. Endosc. 2018, 33, 1386–1393. [Google Scholar] [CrossRef]
- Jeong, O.; Jung, M.R.; Kang, J.H.; Ryu, S.Y. Reduced anastomotic complications with intracorporeal esophagojejunostomy using endoscopic linear staplers (overlap method) in laparoscopic total gastrectomy for gastric carcinoma. Surg. Endosc. 2020, 34, 2313–2320. [Google Scholar] [CrossRef]
- Shi, Y.; Xu, X.; Zhao, Y.; Qian, F.; Tang, B.; Hao, Y.; Luo, H.; Chen, J.; Yu, P. Long-term oncologic outcomes of a randomized controlled trial comparing laparoscopic versus open gastrectomy with D2 lymph node dissection for advanced gastric cancer. Surgery 2019, 165, 1211–1216. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Yingxue, H.; Zhao, Y.; Qian, F.; Tang, B.; Hao, Y.; Luo, H.; Chen, J.; Yu, P. Short-term surgical outcomes of a randomized controlled trial comparing laparoscopic versus open gastrectomy with D2 lymph node dissection for advanced gastric cancer. Surg Endosc. 2018, 32, 2427–2433. [Google Scholar] [CrossRef]
- Lee, J.H.; Nam, B.; Ryu, K.W.; Ryu, S.Y.; Park, Y.K.; Kim, S.; Kim, Y.-W. Comparison of outcomes after laparoscopy-assisted and open total gastrectomy for early gastric cancer. Br. J. Surg. 2015, 102, 1500–1505. [Google Scholar] [CrossRef]
- Hu, Y.; Ying, M.; Huang, C.; Wei, H.; Jiang, Z.; Peng, X.; Hu, J.; Du, X.; Wang, B.; Lin, F.; et al. Oncologic outcomes of laparoscopy-assisted gastrectomy for advanced gastric cancer: A large-scale multicenter retrospective cohort study from China. Surg. Endosc. 2014, 28, 2048–2056. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-H.; Han, S.-U.; Kim, M.-C.; Hyung, W.J.; Kim, W.; Lee, H.-J.; Ryu, S.W.; Cho, G.S.; Song, K.Y.; Ryu, S.Y. Long-term results of laparoscopic gastrectomy for gastric cancer: A large-scale case-control and case-matched Korean multicenter study. J. Clin. Oncol. 2014, 32, 627–633. [Google Scholar] [CrossRef]
- Hu, Y.; Huang, C.; Sun, Y.; Su, X.; Cao, H.; Hu, J.; Xue, Y.; Suo, J.; Tao, K.; He, X.; et al. Morbidity and mortality of laparoscopic versus open D2 distal gastrectomy for advanced gastric cancer: A randomized controlled trial. J. Clin. Oncol. 2016, 34, 1350–1357. [Google Scholar] [CrossRef] [PubMed]
- Higgins, R.M.; Kubasiak, J.C.; Jacobson, R.A.; Janssen, I.; Myers, J.A.; Millikan, K.W.; Deziel, D.J.; Luu, M.B. Outcomes and use of laparoscopic versus open gastric resection. JSLS 2015, 19, e2015.00095. [Google Scholar] [CrossRef] [Green Version]
- Goh, P.M.Y.; Alponat, A.; Mak, K.; Kum, C.K. Early international results of laparoscopic gastrectomies. Surg. Endosc. 1997, 11, 650–652. [Google Scholar] [CrossRef]
- Umemura, A.; Koeda, K.; Sasaki, A.; Fujiwara, H.; Kimura, Y.; Iwaya, T.; Akiyama, Y.; Wakabayashi, G. Totally laparoscopic total gastrectomy for gastric cancer: Literature review and comparison of the procedure of esophagojejunostomy. Asian J. Surg. 2015, 38, 102–112. [Google Scholar] [CrossRef] [PubMed]
- Kyogoku, N.; Ebihara, Y.; Shichinohe, T.; Nakamura, F.; Murakawa, K.; Morita, T.; Okushiba, S.; Hirano, S. Circular versus linear stapling in esophagojejunostomy after laparoscopic total gastrectomy for gastric cancer: A propensity score-matched study. Langenbecks Arch. Surg. 2018, 403, 463–471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naito, M.; Miura, H.; Nakamura, T.; Sato, T.; Yamanashi, T.; Tsutsui, A.; Watanabe, M. Sutureless functional end-to-end anastomosis using a linear stapler with polyglycolic acid felt for intestinal anastomoses. Ann. Med. Surg. 2017, 17, 50–53. [Google Scholar] [CrossRef]
- Ko, C.S.; Gong, C.S.; Kim, B.S.; Kim, S.-O.; Kim, H.S. Overlap method versus functional method for esophagojejunal reconstruction using totally laparoscopic total gastrectomy. Surg. Endosc. 2020, 35, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Pan, Y.; Cai, J.-Q.; Wu, D.; Yan, J.-F.; Chen, D.-W.; Yu, H.-M.; Wang, X.-F. Totally laparoscopic versus laparoscopic-assisted total gastrectomy for upper and middle gastric cancer: A single-unit experience of 253 cases with meta-analysis. World J. Surg. Oncol. 2016, 14, 96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakuramoto, S.; Kikuchi, S.; Futawatari, N.; Moriya, H.; Katada, N.; Yamashita, K.; Watanabe, M. Technique of esophagojejunostomy using transoral placement of the pretilted anvil head after laparoscopic gastrectomy for gastric cancer. Surgery 2010, 147, 742–747. [Google Scholar] [CrossRef]
- Takayama, Y.; Kaneoka, Y.; Maeda, A.; Fukami, Y.; Takahashi, T.; Uji, M. A novel technique of hand-sewn purse-string suturing by double ligation method (DLM) for intracorporeal circular esophagojejunostomy. J. Gastric Cancer 2019, 19, 290–300. [Google Scholar] [CrossRef] [PubMed]
- Wada, N.; Kurokawa, Y.; Takiguchi, S.; Takahashi, T.; Yamasaki, M.; Miyata, H.; Nakajima, K.; Mori, M.; Doki, Y. Feasibility of laparoscopy-assisted total gastrectomy in patients with clinical stage I gastric cancer. Gastric Cancer 2014, 17, 137–140. [Google Scholar] [CrossRef] [Green Version]
- Usui, S.; Nagai, K.; Hiranuma, S.; Takiguchi, N.; Matsumoto, A.; Sanada, K. Laparoscopy-assisted esophagoenteral anastomosis using endoscopic purse-string suture instrument ‘’Endo-PSI (II)’’and circular stapler. Gastric Cancer 2008, 11, 233–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okabe, H.; Obama, K.; Tsunoda, S.; Tanaka, E.; Sakai, Y. Advantage of completely laparoscopic gastrectomy with linear stapled reconstruction: A long-term follow-up study. Ann. Surg. 2014, 259, 109–116. [Google Scholar] [CrossRef] [Green Version]
- Sugiyama, M.; Oki, E.; Ogaki, K.; Morita, M.; Sakaguchi, Y.; Koga, S.; Saeki, H.; Maehara, Y. Clinical outcomes of esophagojejunostomy in totally laparoscopic total gastrectomy: A multicenter study. Surg. Laparosc. Endosc. Percutaneous Tech. 2017, 27, e87–e91. [Google Scholar] [CrossRef] [PubMed]
- So, K.O.; Park, J.-M. Totally laparoscopic total gastrectomy using intracorporeally hand-sewn esophagojejunostomy. J. Gastric Cancer 2011, 11, 206–211. [Google Scholar] [CrossRef] [PubMed]
- Norero, E.; Muñoz, R.; Ceroni, M.; Manzor, M.; Crovari, F.; Gabrielli, M. Two-layer hand-sewn esophagojejunostomy in totally laparoscopic total gastrectomy for gastric cancer. J. Gastric Cancer 2017, 17, 267–276. [Google Scholar] [CrossRef] [Green Version]
- Xu, X.; Huang, C.; Mou, Y.; Zhang, R.; Pan, Y.; Chen, K.; Lu, C. Intra-corporeal hand-sewn esophagojejunostomy is a safe and feasible procedure for totally laparoscopic total gastrectomy: Short-term outcomes in 100 consecutive patients. Surg. Endosc. 2018, 32, 2689–2695. [Google Scholar] [CrossRef]
- Yan, J.-F.; Chen, K.; Pan, Y.; Maher, H.; Zhu, H.-P.; Lou, S.-M.; Wang, Y. Laparoscopic gastrectomy using intracorporeally hand-sewn anastomosis of esophagojejunostomy, gastroduodenostomy, or gastrojejunostomy for gastric cancer. Medicine 2020, 99, e19002. [Google Scholar] [CrossRef] [PubMed]
- Charalabopoulos, A.; Lorenzi, B.; Kordzadeh, A.; Tang, C.-B.; Kadirkamanathan, S.; Jayanthi, N.V. Role of 3D in minimally invasive esophagectomy. Langenbecks Arch Surg. 2017, 402, 555–561. [Google Scholar] [CrossRef]
- Charalabopoulos, A.; Davakis, S.; Syllaios, A.; Lorenzi, B. Intrathoracic hand-sewn esophagogastric anastomosis in prone position during totally minimally invasive two-stage esophagectomy for esophageal cancer. Dis. Esophagus 2020, 34, doaa106. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Patients (n = 40) |
|---|---|
| Mean Age (Range) | 63.2 years (Range: 32–84) |
| Gender Male Female | n = 31 (77.5%) n = 9 (22.5%) |
| Mean BMI | 27.5 kg/m2 (Range: 23–49) |
| ASA score I II III IV | n = 5 (12.5%) n = 20 (50%) n = 12 (30%) n = 3 (7.5%) |
| Neoadjuvant chemotherapy | n = 30 (75%) |
| Adjuvant chemotherapy | n = 26 (65%) |
| Primary Tumor Location Stomach Esophago-gastric junction (Siewert type III) | n = 25 (62.5%) n = 15 (37.5%) |
| Mean Operative Time | 240 min (Range: 180–300 min) |
| Mean anastomotic suturing time | 55 min (Range: 40–80 min) |
| Conversion to open | 0 |
| Postoperative complications Anastomotic leak Anastomotic stricture | 0 0 |
| 30-day mortality | 0 |
| 90-day mortality | 0 |
| Median length of stay | 8 days (Range: 7–9 days) |
| Median follow-up | 19 months (Range: 1–38 months) |
| Tumor Differentiation Poor Moderate Well-differentiated | n = 15 (37.5%) n = 17 (42.5%) n = 8 (20%) |
| Tumor T-status pT1a pT1b pT2 pT3 pT4a | n = 1 (2.5%) n = 3 (7.5%) n = 15 (37.5%) n = 16 (40%) n = 5 (12.5%) |
| Tumor N-status N0 N1 N2 N3a N3b | n = 14 (35%) n = 10 (25%) n = 11 (27.5%) n = 2 (5%) n = 3 (7.5%) |
| Median number of lymph-nodes extracted | n = 35 (Range: 18–50) |
| Authors | Design | Year | Number of Patients | Anastomotic-Related Complications * |
|---|---|---|---|---|
| So et al. [34] | Retrospective | 2011 | 6 | 0 |
| Chen et al. [28] | Retrospective | 2017 | 31 | 2 (6.45%) |
| Norero et al. [35] | Retrospective | 2017 | 51 | 3 (5.88%) |
| Xu et al. [36] | Retrospective | 2017 | 100 | 4 (4%) |
| Yan et al. [37] | Retrospective | 2020 | 44 | 1 (2.27%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Charalabopoulos, A.; Davakis, S.; Paraskeva, P.; Machairas, N.; Kapelouzou, A.; Kordzadeh, A.; Sakarellos, P.; Vailas, M.; Baili, E.; Bakoyiannis, C.; et al. Feasibility and Short-Term Outcomes of Three-Dimensional Hand-Sewn Esophago-Jejunal Anastomosis in Completely Laparoscopic Total Gastrectomy for Cancer. Cancers 2021, 13, 4709. https://doi.org/10.3390/cancers13184709
Charalabopoulos A, Davakis S, Paraskeva P, Machairas N, Kapelouzou A, Kordzadeh A, Sakarellos P, Vailas M, Baili E, Bakoyiannis C, et al. Feasibility and Short-Term Outcomes of Three-Dimensional Hand-Sewn Esophago-Jejunal Anastomosis in Completely Laparoscopic Total Gastrectomy for Cancer. Cancers. 2021; 13(18):4709. https://doi.org/10.3390/cancers13184709
Chicago/Turabian StyleCharalabopoulos, Alexandros, Spyridon Davakis, Panorea Paraskeva, Nikolaos Machairas, Alkistis Kapelouzou, Ali Kordzadeh, Panagiotis Sakarellos, Michail Vailas, Efstratia Baili, Christos Bakoyiannis, and et al. 2021. "Feasibility and Short-Term Outcomes of Three-Dimensional Hand-Sewn Esophago-Jejunal Anastomosis in Completely Laparoscopic Total Gastrectomy for Cancer" Cancers 13, no. 18: 4709. https://doi.org/10.3390/cancers13184709