
Whole-Brain Radiotherapy vs. Localized Radiotherapy after Resection of Brain Metastases in the Era of Targeted Therapy: A Retrospective Study


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Patient and Treatment Characteristics
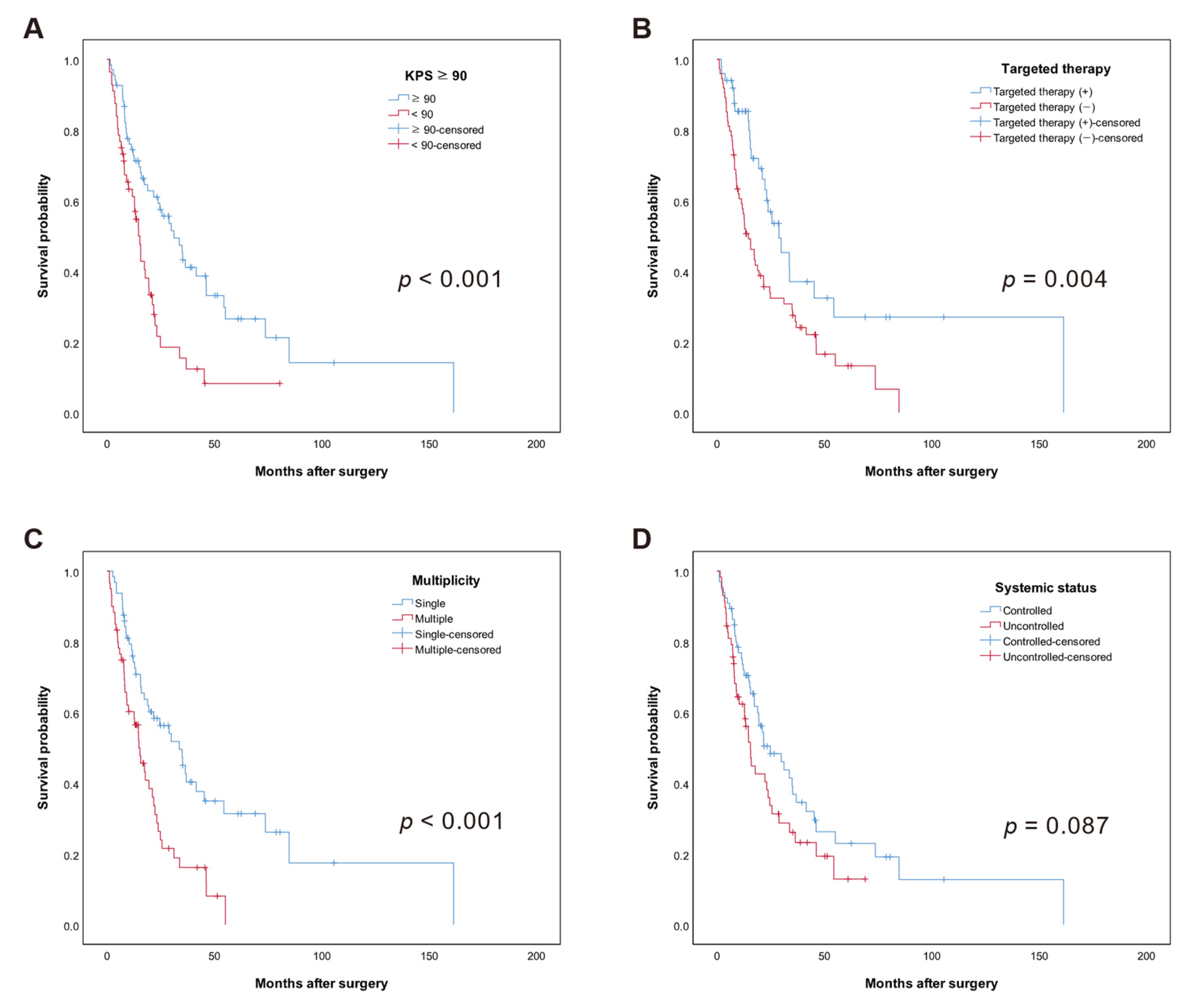
3.2. Overall Survival (OS)
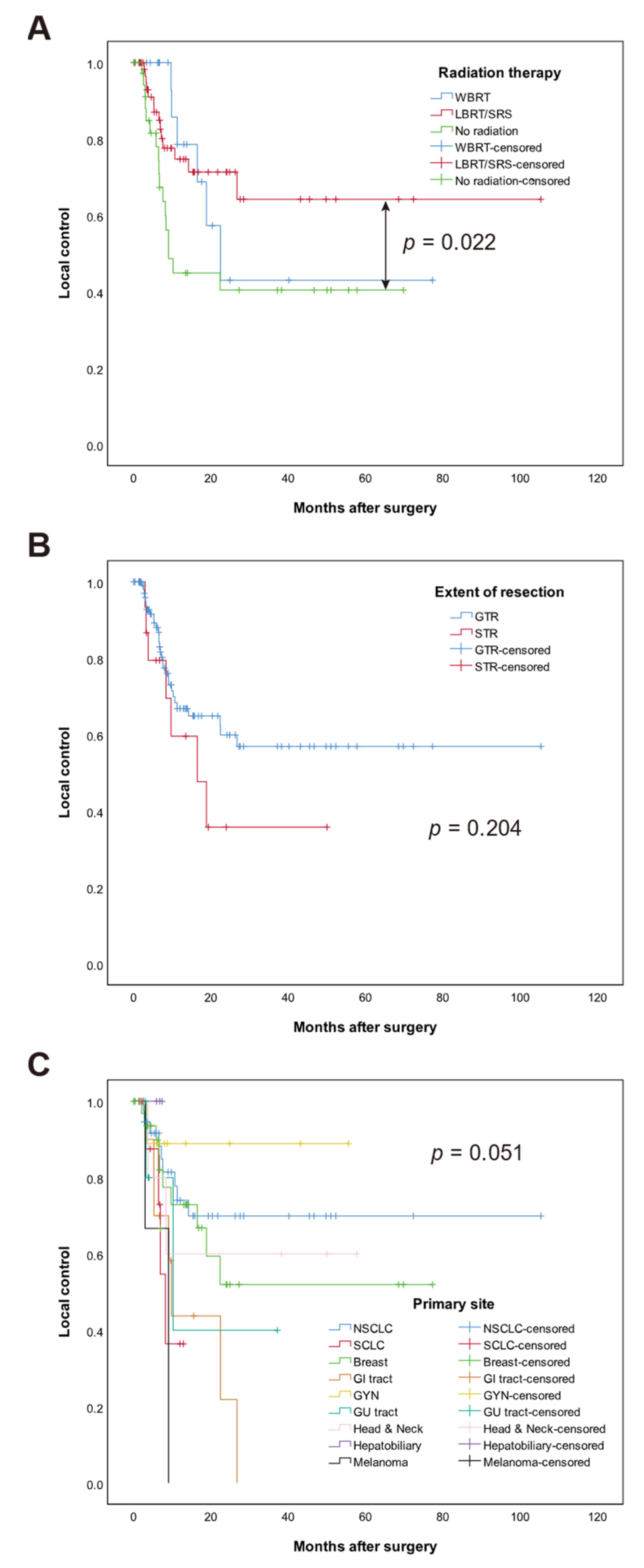
3.3. Local Control (LC)
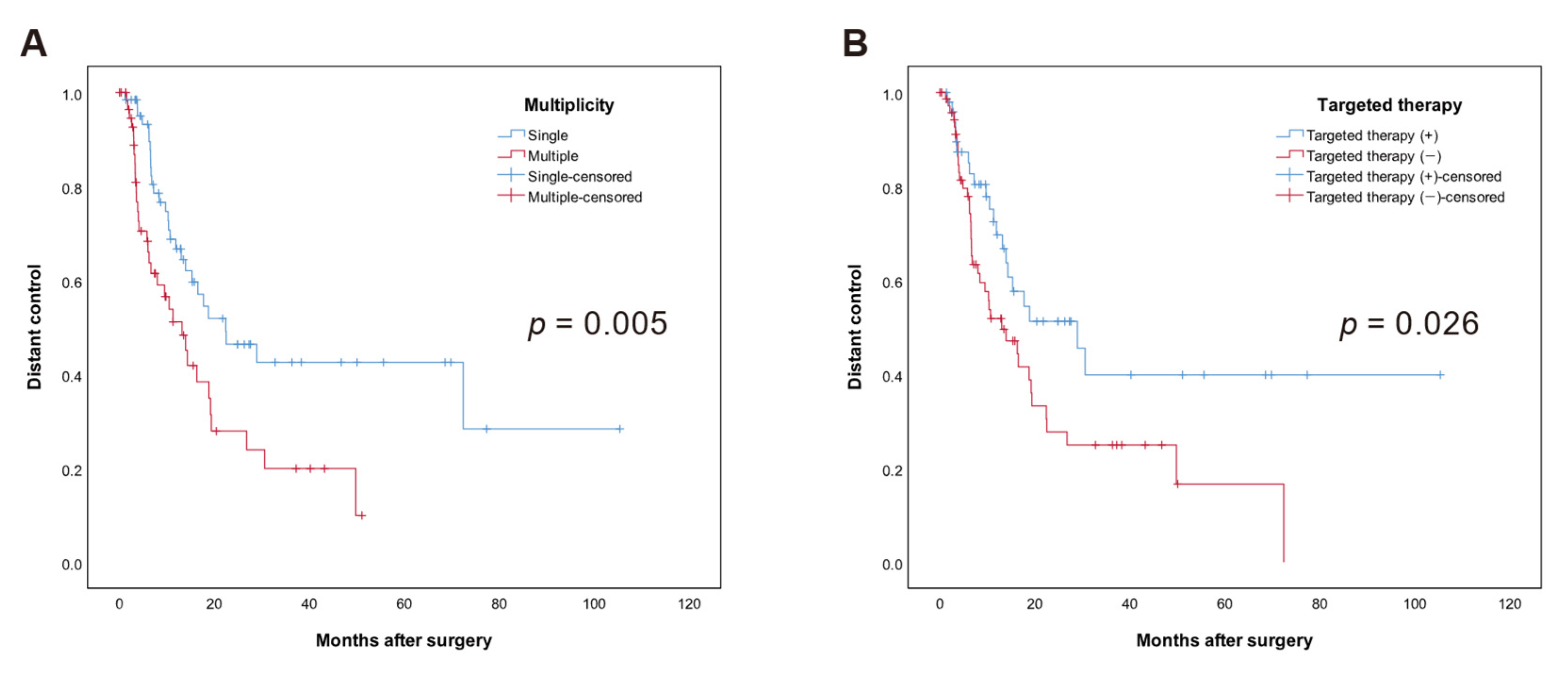
3.4. Distant Control (DC)
3.5. Leptomeningeal Metastases (LMM)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhang, X.; Zhang, W.; Cao, W.-D.; Cheng, G.; Liu, B.; Cheng, J. A Review of Current Management of Brain Metastases. Ann. Surg. Oncol. 2012, 19, 1043–1050. [Google Scholar] [CrossRef] [PubMed]
- Paek, S.H.; Audu, P.B.; Sperling, M.R.; Cho, J.; Andrews, D.W. Reevaluation of Surgery for the Treatment of Brain Metastases: Review of 208 Patients with Single or Multiple Brain Metastases Treated at One Institution with Modern Neurosurgical Techniques. Neurosurgery 2005, 56, 1021–1034. [Google Scholar] [CrossRef] [PubMed]
- Chamberlain, M.C.; Baik, C.S.; Gadi, V.K.; Bhatia, S.; Chow, L.Q.M. Systemic Therapy of Brain Metastases: Non–Small Cell Lung Cancer, Breast Cancer, and Melanoma. Neuro-Oncol. 2017, 19, i1–i24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patchell, R.A.; Tibbs, P.A.; Regine, W.F.; Dempsey, R.J.; Mohiuddin, M.; Kryscio, R.J.; Markesbery, W.R.; Foon, K.A.; Young, B. Postoperative Radiotherapy in the Treatment of Single Metastases to the Brain: A Randomized Trial. JAMA 1998, 280, 1485–1489. [Google Scholar] [CrossRef]
- Yamamoto, M.; Serizawa, T.; Shuto, T.; Akabane, A.; Higuchi, Y.; Kawagishi, J.; Yamanaka, K.; Sato, Y.; Jokura, H.; Yomo, S.; et al. Stereotactic Radiosurgery for Patients with Multiple Brain Metastases (JLGK0901): A Multi-Institutional Prospective Observational Study. Lancet Oncol. 2014, 15, 387–395. [Google Scholar] [CrossRef]
- Kocher, M.; Soffietti, R.; Abacioglu, U.; Villà, S.; Fauchon, F.; Baumert, B.G.; Fariselli, L.; Tzuk-Shina, T.; Kortmann, R.-D.; Carrie, C.; et al. Adjuvant Whole-Brain Radiotherapy Versus Observation After Radiosurgery or Surgical Resection of One to Three Cerebral Metastases: Results of the EORTC 22952-26001 Study. J. Clin. Oncol. 2011, 29, 134–141. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Bentzen, S.M.; Li, J.; Renschler, M.; Mehta, M.P. Relationship Between Neurocognitive Function and Quality of Life After Whole-Brain Radiotherapy in Patients With Brain Metastasis. Int. J. Radiat. Oncol. 2008, 71, 64–70. [Google Scholar] [CrossRef]
- Bhangoo, S.S.; Linskey, M.E.; Kalkanis, S.N. Evidence-Based Guidelines for the Management of Brain Metastases. Neurosurg. Clin. N. Am. 2011, 22, 97–104. [Google Scholar] [CrossRef]
- Al-Shamy, G.; Sawaya, R. Management of Brain Metastases: The Indispensable Role of Surgery. J. Neurooncol. 2009, 92, 275. [Google Scholar] [CrossRef]
- Patchell, R.A.; Tibbs, P.A.; Walsh, J.W.; Dempsey, R.J.; Maruyama, Y.; Kryscio, R.J.; Markesbery, W.R.; Macdonald, J.S.; Young, B. A Randomized Trial of Surgery in the Treatment of Single Metastases to the Brain. N. Engl. J. Med. 1990, 322, 494–500. [Google Scholar] [CrossRef]
- Jung, J.; Kim, S.; Joo, J.; Shin, K.H.; Gwak, H.-S.; Lee, S.H. Incidence and Risk Factors for Leptomeningeal Carcinomatosis in Breast Cancer Patients with Parenchymal Brain Metastases. J. Korean Neurosurg. Soc. 2012, 52, 193–199. [Google Scholar] [CrossRef]
- Patel, A.J.; Suki, D.; Hatiboglu, M.A.; Abouassi, H.; Shi, W.; Wildrick, D.M.; Lang, F.F.; Sawaya, R. Factors Influencing the Risk of Local Recurrence after Resection of a Single Brain Metastasis: Clinical Article. J. Neurosurg. 2010, 113, 181–189. [Google Scholar] [CrossRef]
- Johnson, M.D.; Avkshtol, V.; Baschnagel, A.M.; Meyer, K.; Ye, H.; Grills, I.S.; Chen, P.Y.; Maitz, A.; Olson, R.E.; Pieper, D.R.; et al. Surgical Resection of Brain Metastases and the Risk of Leptomeningeal Recurrence in Patients Treated With Stereotactic Radiosurgery. Int. J. Radiat. Oncol. 2016, 94, 537–543. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.L.; Wefel, J.S.; Hess, K.R.; Allen, P.K.; Lang, F.F.; Kornguth, D.G.; Arbuckle, R.B.; Swint, J.M.; Shiu, A.S.; Maor, M.H.; et al. Neurocognition in Patients with Brain Metastases Treated with Radiosurgery or Radiosurgery plus Whole-Brain Irradiation: A Randomised Controlled Trial. Lancet Oncol. 2009, 10, 1037–1044. [Google Scholar] [CrossRef]
- Kim, Y.-J.; Cho, K.H.; Kim, J.-Y.; Lim, Y.K.; Min, H.S.; Lee, S.H.; Kim, H.J.; Gwak, H.S.; Yoo, H.; Lee, S.H. Single-Dose Versus Fractionated Stereotactic Radiotherapy for Brain Metastases. Int. J. Radiat. Oncol. 2011, 81, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Suh, J.H.; Kotecha, R.; Chao, S.T.; Ahluwalia, M.S.; Sahgal, A.; Chang, E.L. Current Approaches to the Management of Brain Metastases. Nat. Rev. Clin. Oncol. 2020, 17, 279–299. [Google Scholar] [CrossRef]
- Minniti, G.; Niyazi, M.; Andratschke, N.; Guckenberger, M.; Palmer, J.D.; Shih, H.A.; Lo, S.S.; Soltys, S.; Russo, I.; Brown, P.D.; et al. Current Status and Recent Advances in Resection Cavity Irradiation of Brain Metastases. Radiat. Oncol. 2021, 16, 73. [Google Scholar] [CrossRef]
- Barbour, A.B.; Jacobs, C.D.; Williamson, H.; Floyd, S.R.; Suneja, G.; Torok, J.A.; Kirkpatrick, J.P. Radiation Therapy Practice Patterns for Brain Metastases in the United States in the Stereotactic Radiosurgery Era. Adv. Radiat. Oncol. 2020, 5, 43–52. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.K.; Park, J.E.; Kim, K.H.; Cho, J.M.; Moon, J.; Yoon, W.-S.; Kim, S.H.; Kim, Y.I.; Kim, Y.Z.; Kim, H.S.; et al. A National Consensus Survey for Current Practice in Brain Tumor Management III: Brain Metastasis and Primary Central Nervous System Lymphoma. Brain Tumor Res. Treat. 2020, 8, 20–28. [Google Scholar] [CrossRef]
- Lin, N.U.; Lee, E.Q.; Aoyama, H.; Barani, I.J.; Barboriak, D.P.; Baumert, B.G.; Bendszus, M.; Brown, P.D.; Camidge, D.R.; Chang, S.M.; et al. Response Assessment Criteria for Brain Metastases: Proposal from the RANO Group. Lancet Oncol. 2015, 16, e270–e278. [Google Scholar] [CrossRef]
- Sperduto, P.W.; Berkey, B.; Gaspar, L.E.; Mehta, M.; Curran, W. A New Prognostic Index and Comparison to Three Other Indices for Patients With Brain Metastases: An Analysis of 1,960 Patients in the RTOG Database. Int. J. Radiat. Oncol. 2008, 70, 510–514. [Google Scholar] [CrossRef] [PubMed]
- Sperduto, P.W.; Jiang, W.; Brown, P.D.; Braunstein, S.; Sneed, P.; Wattson, D.A.; Shih, H.A.; Bangdiwala, A.; Shanley, R.; Lockney, N.A.; et al. Estimating Survival in Melanoma Patients With Brain Metastases: An Update of the Graded Prognostic Assessment for Melanoma Using Molecular Markers (Melanoma-MolGPA). Int. J. Radiat. Oncol. 2017, 99, 812–816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sperduto, P.W.; Yang, T.J.; Beal, K.; Pan, H.; Brown, P.D.; Bangdiwala, A.; Shanley, R.; Yeh, N.; Gaspar, L.E.; Braunstein, S.; et al. Estimating Survival in Patients With Lung Cancer and Brain Metastases: An Update of the Graded Prognostic Assessment for Lung Cancer Using Molecular Markers (Lung-MolGPA). JAMA Oncol. 2017, 3, 827–831. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.R.; Roh, T.H.; Jeong, D.H.; You, N.; Jang, A.H.; Seo, M.R.; Choung, J.H.; Park, B.; Kim, S.-H. A Simple and Practical Scoring System for Radiosurgical Treatment in Patients with Brain Metastases. Stereotact. Funct. Neurosurg. 2020, 98, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Roh, T.H.; Choi, M.S.; You, N.; Jeong, D.; Jang, A.H.; Seo, M.R.; Lee, S.R.; Kim, S.-H. Identifying Candidates for Gamma Knife Radiosurgery among Elderly Patients with Brain Metastases. J. Neurooncol. 2018, 137, 559–565. [Google Scholar] [CrossRef]
- Gaspar, L.; Scott, C.; Rotman, M.; Asbell, S.; Phillips, T.; Wasserman, T.; McKenna, W.G.; Byhardt, R. Recursive Partitioning Analysis (RPA) of Prognostic Factors in Three Radiation Therapy Oncology Group (RTOG) Brain Metastases Trials. Int. J. Radiat. Oncol. Biol. Phys. 1997, 37, 745–751. [Google Scholar] [CrossRef]
- Kalkanis, S.N.; Kondziolka, D.; Gaspar, L.E.; Burri, S.H.; Asher, A.L.; Cobbs, C.S.; Ammirati, M.; Robinson, P.D.; Andrews, D.W.; Loeffler, J.S.; et al. The Role of Surgical Resection in the Management of Newly Diagnosed Brain Metastases: A Systematic Review and Evidence-Based Clinical Practice Guideline. J. Neurooncol. 2010, 96, 33–43. [Google Scholar] [CrossRef] [Green Version]
- Nieder, C.; Mehta, M.P. Prognostic Indices for Brain Metastases—Usefulness and Challenges. Radiat. Oncol. 2009, 4, 10. [Google Scholar] [CrossRef] [Green Version]
- Weltman, E.; Salvajoli, J.V.; Brandt, R.A.; de Morais Hanriot, R.; Prisco, F.E.; Cruz, J.C.; de Oliveira Borges, S.R.; Wajsbrot, D.B. Radiosurgery for Brain Metastases: A Score Index for Predicting Prognosis. Int. J. Radiat. Oncol. 2000, 46, 1155–1161. [Google Scholar] [CrossRef]
- El Shafie, R.A.; Dresel, T.; Weber, D.; Schmitt, D.; Lang, K.; König, L.; Höne, S.; Forster, T.; von Nettelbladt, B.; Eichkorn, T.; et al. Stereotactic Cavity Irradiation or Whole-Brain Radiotherapy Following Brain Metastases Resection—Outcome, Prognostic Factors, and Recurrence Patterns. Front. Oncol. 2020, 10, 693. [Google Scholar] [CrossRef]
- McPherson, C.M.; Suki, D.; Feiz-Erfan, I.; Mahajan, A.; Chang, E.; Sawaya, R.; Lang, F.F. Adjuvant Whole-Brain Radiation Therapy after Surgical Resection of Single Brain Metastases. Neuro-Oncology 2010, 12, 711–719. [Google Scholar] [CrossRef] [Green Version]
- Stelzer, K.J. Epidemiology and Prognosis of Brain Metastases. Surg. Neurol. Int. 2013, 4, S192–S202. [Google Scholar] [CrossRef]
- Erickson, A.W.; Das, S. The Impact of Targeted Therapy on Intracranial Metastatic Disease Incidence and Survival. Front. Oncol. 2019, 9, 797. [Google Scholar] [CrossRef]
- Tonse, R.; Tom, M.C.; Mehta, M.P.; Ahluwalia, M.S.; Kotecha, R. Integration of Systemic Therapy and Stereotactic Radiosurgery for Brain Metastases. Cancers 2021, 13, 3682. [Google Scholar] [CrossRef]
- Ahn, B.-C.; Kim, J.H.; Pyo, K.-H.; Lim, S.M.; Hong, M.H.; Kim, H.R.; Cho, B.C. Analyses of CNS Response to Osimertinib in Patients with T790M-Positive Advanced NSCLC from ASTRIS Korean Subset, Open-Label Real-World Study. Cancers 2021, 13, 3681. [Google Scholar] [CrossRef]
- Yang, S.-H.; Kim, H.Y.; Lee, S.; Jin, S.J. The Effect of Epidermal Growth Factor Receptor Mutation on Intracranial Progression-Free Survival of Non-Small Cell Lung Cancer Patients with Brain Metastasis Underwent Gamma Knife Radiosurgery. Brain Tumor Res. Treat. 2020, 8, 103–108. [Google Scholar] [CrossRef]
- Colclough, N.; Chen, K.; Johnström, P.; Strittmatter, N.; Yan, Y.; Wrigley, G.L.; Schou, M.; Goodwin, R.; Varnäs, K.; Adua, S.J.; et al. Preclinical Comparison of the Blood–Brain Barrier Permeability of Osimertinib with Other EGFR TKIs. Clin. Cancer Res. 2021, 27, 189–201. [Google Scholar] [CrossRef] [PubMed]
- Brown, P.D.; Ballman, K.V.; Cerhan, J.H.; Anderson, S.K.; Carrero, X.W.; Whitton, A.C.; Greenspoon, J.; Parney, I.F.; Laack, N.N.I.; Ashman, J.B.; et al. Postoperative Stereotactic Radiosurgery Compared with Whole Brain Radiotherapy for Resected Metastatic Brain Disease (NCCTG N107C/CEC·3): A Multicentre, Randomised, Controlled, Phase 3 Trial. Lancet Oncol. 2017, 18, 1049–1060. [Google Scholar] [CrossRef]
- Soffietti, R.; Kocher, M.; Abacioglu, U.M.; Villa, S.; Fauchon, F.; Baumert, B.G.; Fariselli, L.; Tzuk-Shina, T.; Kortmann, R.-D.; Carrie, C.; et al. A European Organisation for Research and Treatment of Cancer Phase III Trial of Adjuvant Whole-Brain Radiotherapy Versus Observation in Patients With One to Three Brain Metastases From Solid Tumors After Surgical Resection or Radiosurgery: Quality-of-Life Results. J. Clin. Oncol. 2013, 31, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, A.; Ahmed, S.; McAleer, M.F.; Weinberg, J.S.; Li, J.; Brown, P.; Settle, S.; Prabhu, S.S.; Lang, F.F.; Levine, N.; et al. Post-Operative Stereotactic Radiosurgery versus Observation for Completely Resected Brain Metastases: A Single-Centre, Randomised, Controlled, Phase 3 Trial. Lancet Oncol. 2017, 18, 1040–1048. [Google Scholar] [CrossRef]
- Zhen, J.; Wen, L.; Lai, M.; Zhou, Z.; Shan, C.; Li, S.; Lin, T.; Wu, J.; Wang, W.; Xu, S.; et al. Whole Brain Radiotherapy (WBRT) for Leptomeningeal Metastasis from NSCLC in the Era of Targeted Therapy: A Retrospective Study. Radiat. Oncol. 2020, 15, 185. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Ahn, H.K.; Park, Y.H.; Nam, D.H.; Lee, J.I.; Park, W.; Choi, D.H.; Huh, S.J.; Park, K.T.; Ahn, J.S.; et al. Leptomeningeal Metastases from Breast Cancer: Intrinsic Subtypes May Affect Unique Clinical Manifestations. Breast Cancer Res. Treat. 2011, 129, 809–817. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Choi, Y.L.; Han, J.; Park, S.; Jung, H.A.; Su, J.-M.; Lee, S.-H.; Ahn, J.S.; Park, K.; Ahn, M.-J. Osimertinib Improves Overall Survival in Patients With EGFR-Mutated NSCLC With Leptomeningeal Metastases Regardless of T790M Mutational Status. J. Thorac. Oncol. 2020, 15, 1758–1766. [Google Scholar] [CrossRef] [PubMed]
- Liao, B.-C.; Lee, J.-H.; Lin, C.-C.; Chen, Y.-F.; Chang, C.-H.; Ho, C.-C.; Shih, J.-Y.; Yu, C.-J.; Yang, J.C.-H. Epidermal Growth Factor Receptor Tyrosine Kinase Inhibitors for Non–Small-Cell Lung Cancer Patients with Leptomeningeal Carcinomatosis. J. Thorac. Oncol. 2015, 10, 1754–1761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baliga, S.; Garg, M.K.; Fox, J.; Kalnicki, S.; Lasala, P.A.; Welch, M.R.; Tomé, W.A.; Ohri, N. Fractionated Stereotactic Radiation Therapy for Brain Metastases: A Systematic Review with Tumour Control Probability Modelling. Br. J. Radiol. 2017, 90, 20160666. [Google Scholar] [CrossRef] [Green Version]
- Soltys, S.G.; Adler, J.R.; Lipani, J.D.; Jackson, P.S.; Choi, C.Y.H.; Puataweepong, P.; White, S.; Gibbs, I.C.; Chang, S.D. Stereotactic Radiosurgery of the Postoperative Resection Cavity for Brain Metastases. Int. J. Radiat. Oncol. 2008, 70, 187–193. [Google Scholar] [CrossRef]
- Choi, C.Y.H.; Chang, S.D.; Gibbs, I.C.; Adler, J.R.; Harsh IV, G.R.; Lieberson, R.E.; Soltys, S.G. Stereotactic Radiosurgery of the Postoperative Resection Cavity for Brain Metastases: Prospective Evaluation of Target Margin on Tumor Control. Int. J. Radiat. Oncol. 2012, 84, 336–342. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Count (%) |
|---|---|
| Age | 59 (28–78) * |
| Sex | |
| Men | 59 (47.6) |
| Women | 65 (52.4) |
| Postoperative radiotherapy | |
| LBRT/SRS | 63 (50.8) |
| WBRT | 24 (19.4) |
| No radiation | 37 (29.8) |
| Karnofsky Performance Scale | 90 (30–100) * |
| ≥90 | 68 (54.8) |
| <90 | 56 (45.2) |
| Primary site | |
| Non-small cell lung cancer | 41 (33.1) |
| Small cell lung cancer | 9 (7.3) |
| Breast | 34 (27.4) |
| Gastrointestinal | 12 (9.7) |
| Gynecologic | 10 (8.1) |
| Genitourinary | 6 (4.8) |
| Head and Neck | 5 (4.0) |
| Hepatobiliary | 4 (3.2) |
| Melanoma | 3 (2.4) |
| Synchronicity | |
| Metachronous | 91 (73.4) |
| Synchronous | 33 (26.6) |
| Tumor size | 3.75 cm (1.3–7.6 cm) * |
| ≥3cm | 97 (78.2) |
| <3cm | 27 (21.8) |
| Targeted therapy | |
| Targeted therapy (+) | 50 (40.3) |
| EGFR | 15 |
| HER2 | 11 |
| ER/PR | 8 |
| VEGF | 6 |
| PD-1 | 4 |
| ALK | 2 |
| mTOR | 2 |
| PARP | 2 |
| Targeted therapy (−) | 74 (59.7) |
| Systemic control | |
| Controlled | 66 (53.2) |
| Uncontrolled | 58 (46.8) |
| Extent of resection | |
| Gross total resection | 109 (87.9) |
| Subtotal resection | 15 (12.1) |
| Multiplicity | |
| Single | 64 (51.6) |
| Multiple | 60 (48.4) |
| Overall Survival | Univariable | Multivariable | ||
|---|---|---|---|---|
| Parameters | HR (95% CI) | p | HR (95% CI) | p |
| Age (per 1 increase) | 1.00 (0.97–1.02) | 0.795 | ||
| Sex (Women: Men) | 0.73 (0.32–1.68) | 0.464 | ||
| Radiation method | ||||
| No radiation | 1 | |||
| WBRT | 1.15 (0.56–2.36) | 0.701 | ||
| LBRT/SRS | 1.07 (0.48–2.37) | 0.864 | ||
| KPS ≥ 90 | 0.53 (0.27–1.03) | 0.062 | 0.53 (0.32–0.87) | 0.011 |
| Primary site | - | 0.701 | ||
| Synchronicity | 0.85 (0.46–1.60) | 0.621 | ||
| Size (≥3 cm: <3 cm) | 1.11 (0.62–1.99) | 0.737 | ||
| Targeted therapy | 0.43 (0.25–0.75) | 0.003 | 0.43 (0.26–0.70) | 0.001 |
| Systemic control | 0.58 (0.34–0.98) | 0.042 | 0.63 (0.40–1.00) | 0.047 |
| Gross total resection | 1.00 (0.48–2.07) | 0.996 | ||
| Single metastasis | 0.61 (0.36–1.04) | 0.070 | 0.55 (0.34–0.90) | 0.016 |
| Local Control | Univariable | Multivariable | ||
|---|---|---|---|---|
| Parameters | HR (95% CI) | p | HR (95% CI) | p |
| Age (per 1 increase) | 0.99 (0.95–1.03) | 0.469 | ||
| Sex (Women: Men) | 0.92 (0.28–3.00) | 0.883 | ||
| Radiation method | ||||
| No radiation | 1 | 1 | ||
| WBRT | 0.21 (0.06–0.68) | 0.009 | 0.32 (0.11–0.92) | 0.034 |
| LBRT/SRS | 0.37 (0.15–0.88) | 0.025 | 0.018 | |
| KPS ≥ 90 | 0.59 (0.22–1.63) | 0.31 | ||
| Primary site | ||||
| Non-small cell lung cancer | 1 | |||
| Small cell lung cancer | 2.15 (0.56–8.28) | 0.266 | 3.46 (1.02–11.72) | 0.047 |
| Breast | 0.85 (0.20–3.68) | 0.823 | 1.01 (0.39–2.64) | 0.983 |
| Gastrointestinal | 3.30 (1.14–9.59) | 0.028 | 3.83 (1.39–10.56) | 0.009 |
| Gynecologic | 0.40 (0.04–4.04) | 0.433 | 0.40 (0.05–3.14) | 0.38 |
| Genitourinary | 0.45 (0.07–2.90) | 0.398 | 1.12 (0.22–5.68) | 0.892 |
| Head and neck | 0.33 (0.04–2.55) | 0.287 | 0.34 (0.06–1.96) | 0.227 |
| Hepatobiliary | - | 0.981 | - | 0.981 |
| Melanoma | 3.01 (0.52–17.43) | 0.219 | 3.88 (0.78–19.37) | 0.098 |
| Synchronicity | 0.47 (0.17–1.26) | 0.133 | 0.44 (0.18–1.07) | 0.071 |
| Size (≥3 cm: <3 cm) | 0.76 (0.32–1.81) | 0.539 | ||
| Targeted therapy | 0.64 (0.26–1.58) | 0.335 | ||
| Systemic control | 0.96 (0.44–2.09) | 0.91 | ||
| Gross total resection | 0.30 (0.11–0.83) | 0.021 | 0.29 (0.11–0.78) | 0.014 |
| Single metastasis | 0.95 (0.40–2.26) | 0.905 | ||
| Distant Control | Univariable | Multivariable | ||
|---|---|---|---|---|
| Parameters | HR (95% CI) | p | HR (95% CI) | p |
| Age (per 1 increase) | 0.98 (0.95–1.01) | 0.184 | ||
| Sex (Women: Men) | 0.68 (0.27–1.71) | 0.411 | ||
| Radiation method | ||||
| No radiation | 1 | |||
| WBRT | 0.86 (0.34–2.18) | 0.756 | ||
| LBRT/SRS | 1.41 (0.69–2.89) | 0.349 | ||
| KPS ≥ 90 | 0.65 (0.30–1.38) | 0.261 | ||
| Primary site | - | 0.865 | ||
| Synchronicity | 0.80 (0.38–1.66) | 0.542 | ||
| Size (≥3 cm; <3 cm) | 1.35 (0.71–2.58) | 0.355 | ||
| Targeted therapy | 0.45 (0.23–0.88) | 0.020 | 0.54 (0.32–0.91) | 0.022 |
| Systemic control | 0.70 (0.37–1.32) | 0.265 | ||
| Gross total resection | 0.71 (0.34–1.52) | 0.384 | ||
| Single metastasis | 0.53 (0.28–0.98) | 0.044 | 0.47 (0.29–0.79) | 0.004 |
| Leptomeningeal Metastases | Univariable | Multivariable | ||
|---|---|---|---|---|
| Parameters | HR (95% CI) | p | HR (95% CI) | p |
| Age (per 1 increase) | 1.03 (0.96–1.09) | 0.430 | ||
| Sex (Women: Men) | 3.98 (0.43–37.31) | 0.226 | ||
| Radiation method | ||||
| No radiation | 1 | |||
| WBRT | 1.72 (0.36–8.13) | 0.493 | ||
| LBRT/SRS | 1.31 (0.41–4.15) | 0.646 | ||
| KPS ≥ 90 | 1.23 (0.36–4.18) | 0.741 | ||
| Primary site | - | 0.293 | ||
| Synchronicity | 0.29 (0.07–1.26) | 0.099 | 0.25 (0.08–0.86) | 0.028 |
| Size (≥3 cm; <3 cm) | 0.65 (0.21–2.02) | 0.458 | ||
| Targeted therapy | 0.46 (0.16–1.33) | 0.153 | 0.42 (0.18–0.95) | 0.038 |
| Systemic control | 0.55 (0.21–1.44) | 0.223 | 0.44 (0.20–0.99) | 0.047 |
| Gross total resection | 0.79 (0.24–2.66) | 0.707 | ||
| Single metastasis | 0.47 (0.19–1.17) | 0.105 | 0.47 (0.22–1.02) | 0.055 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koo, J.; Roh, T.H.; Lee, S.R.; Heo, J.; Oh, Y.-T.; Kim, S.-H. Whole-Brain Radiotherapy vs. Localized Radiotherapy after Resection of Brain Metastases in the Era of Targeted Therapy: A Retrospective Study. Cancers 2021, 13, 4711. https://doi.org/10.3390/cancers13184711
Koo J, Roh TH, Lee SR, Heo J, Oh Y-T, Kim S-H. Whole-Brain Radiotherapy vs. Localized Radiotherapy after Resection of Brain Metastases in the Era of Targeted Therapy: A Retrospective Study. Cancers. 2021; 13(18):4711. https://doi.org/10.3390/cancers13184711
Chicago/Turabian StyleKoo, Jaho, Tae Hoon Roh, Sang Ryul Lee, Jaesung Heo, Young-Taek Oh, and Se-Hyuk Kim. 2021. "Whole-Brain Radiotherapy vs. Localized Radiotherapy after Resection of Brain Metastases in the Era of Targeted Therapy: A Retrospective Study" Cancers 13, no. 18: 4711. https://doi.org/10.3390/cancers13184711