
Somatic Disease in Survivors of Childhood Malignant Bone Tumors in the Nordic Countries

 , ,
, ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
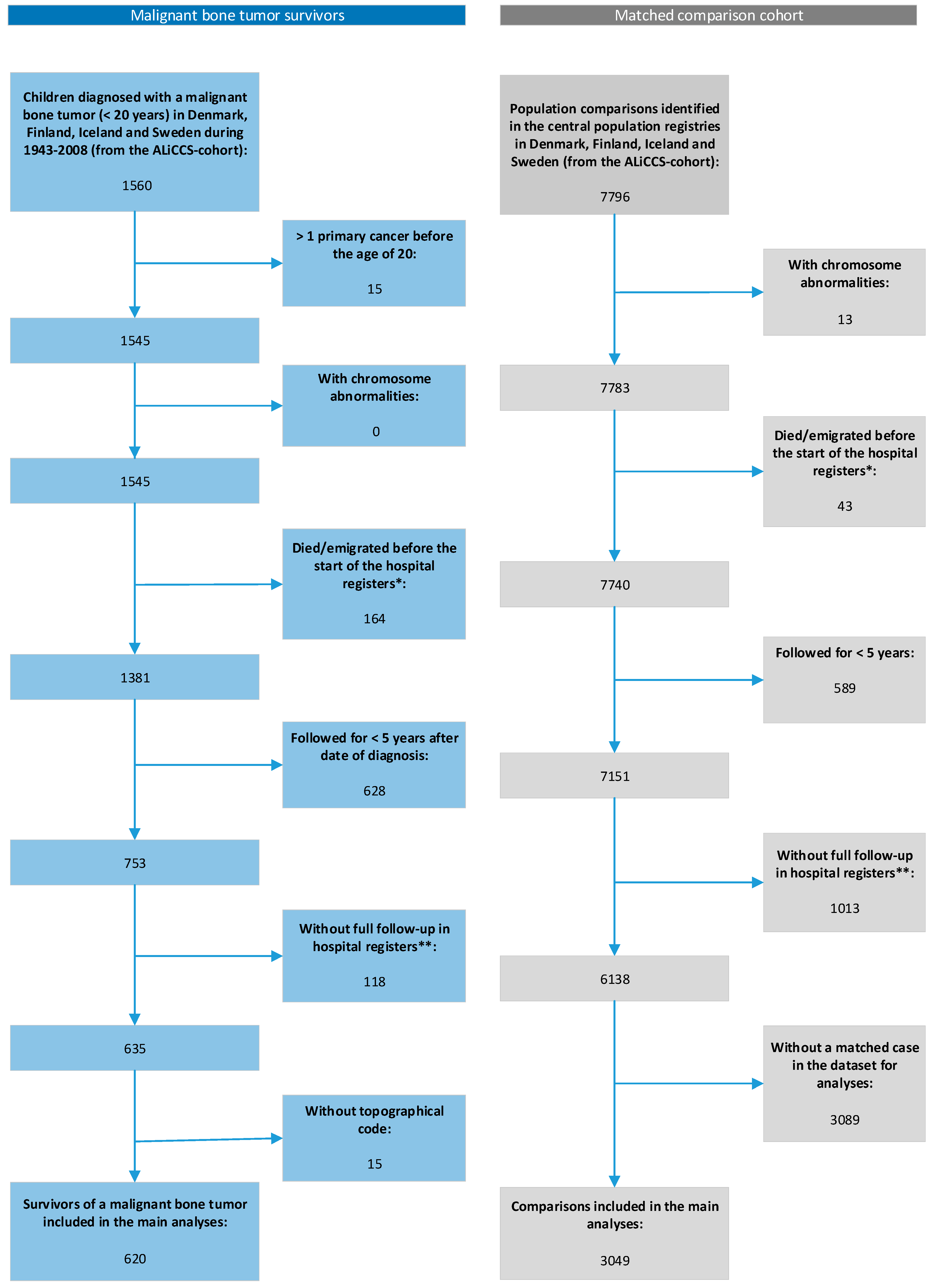
2.1. Survivors of Malignant Bone Tumors and Comparison Cohort
2.2. Hospital Contacts for Somatic Diseases
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Heare, T.; Hensley, M.A.; Dell’Orfano, S. Bone tumors: Osteosarcoma and Ewing’s sarcoma. Curr. Opin. Pediatr. 2009, 21, 365–372. [Google Scholar] [CrossRef]
- Gorlick, R.; Perisoglou, M.; Whelan, J. Bone tumors. In Pediatric Hematology and Oncology Scientific Principles and Clinical Practice; Estlin, E., Gilbertson, R., Wynn, R., Eds.; Wiley-Blackwell: Hoboken, NJ, USA, 2010; pp. 234–257. [Google Scholar]
- Gaspar, N.; Hawkins, D.S.; Dirksen, U.; Lewis, I.J.; Ferrari, S.; Le Deley, M.-C.; Kovar, H.; Grimer, R.; Whelan, J.; Claude, L.; et al. Ewing Sarcoma: Current Management and Future Approaches through Collaboration. J. Clin. Oncol. 2015, 33, 3036–3046. [Google Scholar] [CrossRef] [PubMed]
- Fidler, M.M.; Frobisher, C.; Guha, J.; Wong, K.; Kelly, J.; Winter, D.L.; Sugden, E.; Duncan, R.; Whelan, J.; Reulen, R.C.; et al. Long-term adverse outcomes in survivors of childhood bone sarcoma: The British Childhood Cancer Survivor Study. Br. J. Cancer 2015, 112, 1857–1865. [Google Scholar] [CrossRef] [Green Version]
- Kirchhoff, A.C.; Fluchel, M.N.; Wright, J.; Ying, J.; Sweeney, C.; Bodson, J.; Stroup, A.M.; Smith, K.R.; Fraser, A.; Kinney, A. Risk of hospitalization for survivors of childhood and adolescent cancer. Cancer Epidemiol. Biomark. Prev. 2014, 23, 1280–1289. [Google Scholar] [CrossRef] [Green Version]
- Oeffinger, K.C.; Mertens, A.C.; Sklar, C.A.; Kawashima, T.; Hudson, M.M.; Meadows, A.T.; Friedman, D.L.; Marina, N.; Hobbie, W.; Kadan-Lottick, N.; et al. Chronic health conditions in adult survivors of childhood cancer. N. Engl. J. Med. 2006, 355, 1572–1582. [Google Scholar] [CrossRef] [PubMed]
- Aung, L.; Gorlick, R.G.; Shi, W.; Thaler, H.; Shorter, N.A.; Healey, J.H.; Huvos, A.G.; Meyers, P.A. Second malignant neoplasms in long-term survivors of osteosarcoma: Memorial Sloan-Kettering Cancer Center Experience. Cancer 2002, 95, 1728–1734. [Google Scholar] [CrossRef] [PubMed]
- Bacci, G.; Ferrari, C.; Longhi, A.; Ferrari, S.; Forni, C.; Bacchini, P.; Palmerini, E.; Briccoli, A.; Pignotti, E.; Balladelli, A.; et al. Second malignant neoplasm in patients with osteosarcoma of the extremities treated with adjuvant and neoadjuvant chemotherapy. J. Pediatr. Hematol. Oncol. 2006, 28, 774–780. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, S.; Krailo, M.D.; Chen, Z.; Burden, L.; Askin, F.B.; Dickman, P.S.; Grier, H.E.; Link, M.P.; Meyers, P.; Perlman, E.; et al. Therapy-related myelodysplasia and acute myeloid leukemia after Ewing sarcoma and primitive neuroectodermal tumor of bone: A report from the Children’s Oncology Group. Blood 2007, 109, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Friedman, D.L.; Whitton, J.; Leisenring, W.; Mertens, A.C.; Hammond, S.; Stovall, M.; Donaldson, S.S.; Meadows, A.T.; Robison, L.L.; Neglia, J.P. Subsequent neoplasms in 5-year survivors of childhood cancer: The Childhood Cancer Survivor Study. J. Natl. Cancer Inst. 2010, 102, 1083–1095. [Google Scholar] [CrossRef]
- Goldsby, R.; Burke, C.; Nagarajan, R.; Zhou, T.; Chen, Z.; Marina, N.; Friedman, D.; Neglia, J.; Chuba, P.; Bhatia, S. Second solid malignancies among children, adolescents, and young adults diagnosed with malignant bone tumors after 1976: Follow-up of a Children’s Oncology Group cohort. Cancer 2008, 113, 2597–2604. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, S.N.; Carlson, R.; Hasan, H.; Rassekh, S.R.; Goddard, K. Long-term Outcomes and Complications in Pediatric Ewing Sarcoma. Am. J. Clin. Oncol. 2017, 40, 423–428. [Google Scholar] [CrossRef] [PubMed]
- Kuttesch, J.F., Jr.; Wexler, L.H.; Marcus, R.B.; Fairclough, D.; Weaver-McClure, L.; White, M.; Mao, L.; Delaney, T.F.; Pratt, C.B.; Horowitz, M.E.; et al. Second malignancies after Ewing’s sarcoma: Radiation dose-dependency of secondary sarcomas. J. Clin. Oncol. 1996, 14, 2818–2825. [Google Scholar] [CrossRef] [PubMed]
- Longhi, A.; Ferrari, S.; Tamburini, A.; Luksch, R.; Fagioli, F.; Bacci, G.; Ferrari, C. Late effects of chemotherapy and radiotherapy in osteosarcoma and Ewing sarcoma patients: The Italian Sarcoma Group Experience (1983–2006). Cancer 2012, 118, 5050–5059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navid, F.; Billups, C.; Liu, T.; Krasin, M.J.; Rodriguez-Galindo, C. Second cancers in patients with the Ewing sarcoma family of tumours. Eur. J. Cancer 2008, 44, 983–991. [Google Scholar] [CrossRef] [Green Version]
- Novakovic, B.; Fears, T.R.; Horowitz, M.E.; Tucker, M.A.; Wexler, L.H. Late effects of therapy in survivors of Ewing’s sarcoma family tumors. J. Pediatr. Hematol. Oncol. 1997, 19, 220–225. [Google Scholar] [CrossRef]
- Olsen, J.H.; Moller, T.; Anderson, H.; Langmark, F.; Sankila, R.; Tryggvadottir, L.; Winther, J.F.; Rechnitzer, C.; Jonmundsson, G.; Christensen, J.; et al. Lifelong cancer incidence in 47,697 patients treated for childhood cancer in the Nordic countries. J. Natl. Cancer Inst. 2009, 101, 806–813. [Google Scholar] [CrossRef] [Green Version]
- Nagarajan, R.; Kamruzzaman, A.; Ness, K.K.; Marchese, V.G.; Sklar, C.; Mertens, A.; Yasui, Y.; Robison, L.L.; Marina, N. Twenty years of follow-up of survivors of childhood osteosarcoma: A report from the Childhood Cancer Survivor Study. Cancer 2011, 117, 625–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ginsberg, J.P.; Goodman, P.; Leisenring, W.; Ness, K.K.; Meyers, P.A.; Wolden, S.L.; Smith, S.M.; Stovall, M.; Hammond, S.; Robison, L.L.; et al. Long-term survivors of childhood Ewing sarcoma: Report from the childhood cancer survivor study. J. Natl. Cancer Inst. 2010, 102, 1272–1283. [Google Scholar] [CrossRef] [Green Version]
- Marina, N.M.; Liu, Q.; Donaldson, S.S.; Sklar, C.A.; Armstrong, G.T.; Oeffinger, K.C.; Leisenring, W.; Ginsberg, J.P.; Henderson, T.O.; Neglia, J.; et al. Longitudinal follow-up of adult survivors of Ewing sarcoma: A report from the Childhood Cancer Survivor Study. Cancer 2017, 123, 2551–2560. [Google Scholar] [CrossRef]
- Brewster, D.H.; Clark, D.; Hopkins, L.; Bauer, J.; Wild, S.H.; Edgar, A.B.; Wallace, W.H. Subsequent hospitalisation experience of 5-year survivors of childhood, adolescent, and young adult cancer in Scotland: A population based, retrospective cohort study. Br. J. Cancer 2014, 110, 1342–1350. [Google Scholar] [CrossRef]
- Kurt, B.A.; Nolan, V.G.; Ness, K.K.; Neglia, J.P.; Tersak, J.M.; Hudson, M.M.; Armstrong, G.T.; Hutchinson, R.J.; Leisenring, W.M.; Oeffinger, K.C.; et al. Hospitalization rates among survivors of childhood cancer in the Childhood Cancer Survivor Study cohort. Pediatr. Blood Cancer 2012, 59, 126–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Fine Licht, S.; Rugbjerg, K.; Gudmundsdottir, T.; Bonnesen, T.G.; Asdahl, P.H.; Holmqvist, A.S.; Madanat-Harjuoja, L.; Tryggvadottir, L.; Wesenberg, F.; Hasle, H.; et al. Long-term inpatient disease burden in the Adult Life after Childhood Cancer in Scandinavia (ALiCCS) study: A cohort study of 21,297 childhood cancer survivors. PLoS Med. 2017, 14, e1002296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asdahl, P.H.; Winther, J.F.; Bonnesen, T.G.; Licht, S.D.F.; Gudmundsdottir, T.; Anderson, H.; Madanat-Harjuoja, L.; Tryggvadottir, L.; Småstuen, M.C.; Holmqvist, A.S.; et al. The Adult Life after Childhood Cancer in Scandinavia (ALiCCS) Study: Design and Characteristics. Pediatr. Blood Cancer 2015, 62, 2204–2210. [Google Scholar] [CrossRef] [PubMed]
- Birch, J.M.; Marsden, H.B. A classification scheme for childhood cancer. Int. J. Cancer 1987, 40, 620–624. [Google Scholar] [CrossRef]
- Steliarova-Foucher, E.; Stiller, C.; Lacour, B.; Kaatsch, P. International Classification of Childhood Cancer, third edition. Cancer 2005, 103, 1457–1467. [Google Scholar] [CrossRef]
- Ludvigsson, J.F.; Andersson, E.; Ekbom, A.; Feychting, M.; Kim, J.-L.; Reuterwall, C.; Heurgren, M.; Olausson, P.O. External review and validation of the Swedish national inpatient register. BMC Public Health 2011, 11, 450. [Google Scholar] [CrossRef] [Green Version]
- Lynge, E.; Sandegaard, J.L.; Rebolj, M. The Danish National Patient Register. Scand. J. Public Health 2011, 39 (Suppl. 7), 30–33. [Google Scholar] [CrossRef]
- Schmidt, M.; Schmidt, S.A.; Sandegaard, J.L.; Ehrenstein, V.; Pedersen, L.; Sorensen, H.T. The Danish National Patient Registry: A review of content, data quality, and research potential. Clin. Epidemiol. 2015, 7, 449–490. [Google Scholar] [CrossRef] [Green Version]
- Sund, R. Quality of the Finnish Hospital Discharge Register: A systematic review. Scand. J. Public Health 2012, 40, 505–515. [Google Scholar] [CrossRef]
- Amorim, L.D.; Cai, J. Modelling recurrent events: A tutorial for analysis in epidemiology. Int. J. Epidemiol. 2015, 44, 324–333. [Google Scholar] [CrossRef]
- Lipshultz, S.E.; Adams, M.J.; Colan, S.D.; Constine, L.S.; Herman, E.H.; Hsu, D.T.; Hudson, M.M.; Kremer, L.C.; Landy, D.C.; Miller, T.L.; et al. Long-term cardiovascular toxicity in children, adolescents, and young adults who receive cancer therapy: Pathophysiology, course, monitoring, management, prevention, and research directions: A scientific statement from the American Heart Association. Circulation 2013, 128, 1927–1995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lohmann, D.J.; Hasle, H. Hematological Changes Mimicking Myelodysplastic Syndrome Following Treatment for Osteosarcoma. J. Pediatr. Hematol. Oncol. 2015, 37, 170–174. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 5-Year Survivors of Malignant Bone Tumors | Comparisons | |||
|---|---|---|---|---|
| All N (%) | Osteosarcoma a N (%) | Ewing Sarcoma N (%) | N (%) | |
| Overall | 620 (100.0) cb | 440 (100.0) | 180 (100.0) | 3049 (100.0) c |
| Country | ||||
| Denmark and Iceland | 145 (23.4) | 92 (20.9) | 53 (29.4) | 699 (22.9) |
| Finland | 176 (28.4) | 146 (33.2) | 30 (16.7) | 870 (28.5) |
| Sweden | 299 (48.2) | 202 (45.9) | 97 (53.9) | 1480 (48.5) |
| Period of diagnosis | ||||
| 1961–1979 | 129 (20.8) | 90 (20.5) | 39 (21.7) | - |
| 1980–1989 | 152 (24.5) | 112 (25.5) | 40 (22.2) | - |
| 1990–2008 | 339 (54.7) | 238 (54.1) | 101 (56.1) | - |
| Sex | ||||
| Male | 338 (54.5) | 234 (53.2) | 104 (57.8) | 1666 (54.6) |
| Female | 282 (45.5) | 206 (46.8) | 76 (42.2) | 1383 (45.4) |
| Age at diagnosis | ||||
| Mean (SD) | 13.7 (4.0) | 14.2 (3.7) | 12.3 (4.4) | - |
| 0–14 | 347 (56.0) | 226 (51.4) | 121 (67.2) | - |
| 15–19 | 273 (44.0) | 214 (48.6) | 59 (32.8) | - |
| Cancer site | ||||
| Extremities | 485 (78.2) | 382 (86.8) | 103 (57.2) | - |
| Axial skeleton | 135 (21.8) | 58 (13.2) | 77 (42.8) | - |
| All Survivors of Malignant Bone Tumors | p-Value | Osteosarcoma | Ewing Sarcoma | ||||
|---|---|---|---|---|---|---|---|
| Observed Number of Hospital Contacts | RR (95% CI) | Observed Number of Hospital Contacts | RR (95% CI) | Observed Number of Hospital Contacts | RR (95% CI) | ||
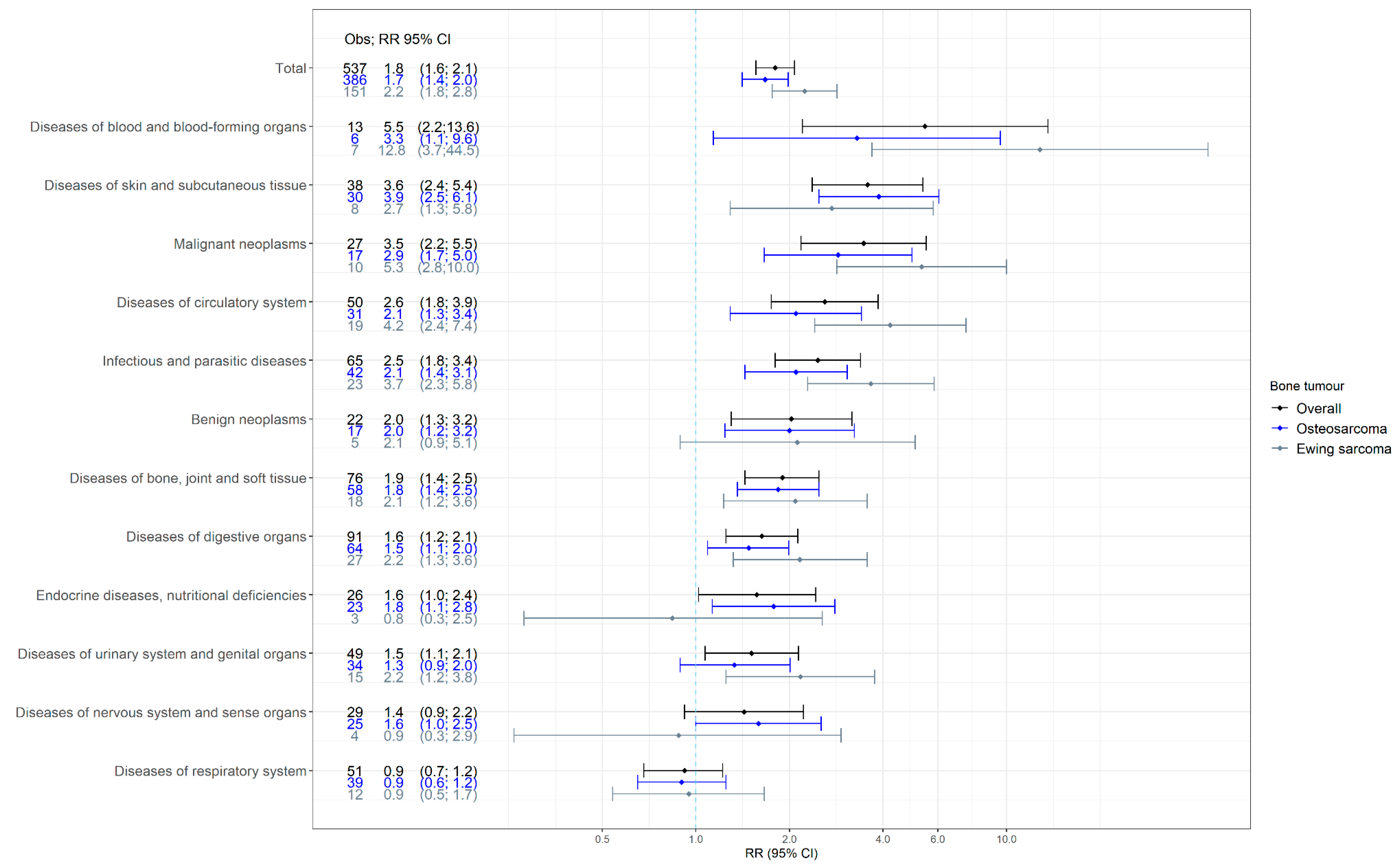
| Overall | 537 | 1.80 (1.56 to 2.08) | 386 | 1.67 (1.41 to 1.98) | 151 | 2.24 (1.76 to 2.85) | |
| Test for same effect in survivors of osteosarcoma and Ewing sarcoma | 0.044 | ||||||
| Sex | |||||||
| Men | 302 | 2.08 (1.69 to 2.56) | 210 | 1.91 (1.50 to 2.42) | 92 | 2.63 (1.85 to 3.73) | |
| Women | 235 | 1.54 (1.26 to 1.87) | 176 | 1.46 (1.16 to 1.84) | 59 | 1.82 (1.37 to 2.42) | |
| Test for interaction * | 0.038 | ||||||
| Age at diagnosis (years) | |||||||
| 0–14 | 299 | 1.64 (1.36 to 1.98) | 198 | 1.51 (1.20 to 1.89) | 101 | 1.99 (1.48 to 2.67) | |
| 15–19 | 238 | 2.05 (1.63 to 2.58) | 188 | 1.90 (1.47 to 2.45) | 50 | 2.93 (1.89 to 4.54) | |
| Test for interaction * | 0.138 | ||||||
| Period of diagnosis | |||||||
| 1961–1969 | 54 | 3.54 (1.84 to 6.80) | 44 | 3.13 (1.48 to 6.59) | 10 | 8.19 (5.37 to 12.47) | |
| 1970–1979 | 174 | 1.47 (1.15 to 1.86) | 117 | 1.30 (0.98 to 1.71) | 57 | 1.99 (1.34 to 2.95) | |
| 1980–1989 | 163 | 1.69 (1.31 to 2.17) | 127 | 1.65 (1.23 to 2.21) | 36 | 1.87 (1.30 to 2.67) | |
| ≥1990 | 146 | 2.17 (1.69 to 2.79) | 98 | 2.02 (1.53 to 2.67) | 48 | 2.58 (1.63 to 4.08) | |
| Test for interaction * | 0.025 | ||||||
| Time since diagnosis (years) | |||||||
| 5–9 | 185 | 2.14 (1.73 to 2.64) | 127 | 1.94 (1.53 to 2.46) | 58 | 2.76 (1.90 to 4.03) | |
| 10–19 | 160 | 1.44 (1.16 to 1.79) | 113 | 1.34 (1.03 to 1.74) | 47 | 1.74 (1.26 to 2.41) | |
| ≥20 | 192 | 1.92 (1.50 to 2.45) | 146 | 1.80 (1.36 to 2.39) | 46 | 2.40 (1.59 to 3.62) | |
| Test for interaction * | 0.016 | ||||||
| Cancer site | |||||||
| Extremities | 412 | 1.75 (1.48 to 2.08) | 320 | 1.66(1.37 to 2.01) | 92 | 2.16 (1.57 to 2.98) | |
| Axial skeleton | 125 | 1.98 (1.56 to 2.53) | 66 | 1.73(1.27 to 2.37) | 59 | 2.37 (1.67 to 3.36) | |
| Test for interaction * | 0.394 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pedersen, C.; Rechnitzer, C.; Andersen, E.A.W.; Kenborg, L.; Norsker, F.N.; Bautz, A.; Baad-Hansen, T.; Tryggvadottir, L.; Madanat-Harjuoja, L.-M.; Holmqvist, A.S.; et al. Somatic Disease in Survivors of Childhood Malignant Bone Tumors in the Nordic Countries. Cancers 2021, 13, 4505. https://doi.org/10.3390/cancers13184505
Pedersen C, Rechnitzer C, Andersen EAW, Kenborg L, Norsker FN, Bautz A, Baad-Hansen T, Tryggvadottir L, Madanat-Harjuoja L-M, Holmqvist AS, et al. Somatic Disease in Survivors of Childhood Malignant Bone Tumors in the Nordic Countries. Cancers. 2021; 13(18):4505. https://doi.org/10.3390/cancers13184505
Chicago/Turabian StylePedersen, Camilla, Catherine Rechnitzer, Elisabeth Anne Wreford Andersen, Line Kenborg, Filippa Nyboe Norsker, Andrea Bautz, Thomas Baad-Hansen, Laufey Tryggvadottir, Laura-Maria Madanat-Harjuoja, Anna Sällfors Holmqvist, and et al. 2021. "Somatic Disease in Survivors of Childhood Malignant Bone Tumors in the Nordic Countries" Cancers 13, no. 18: 4505. https://doi.org/10.3390/cancers13184505