
Immune Checkpoint Blockade for Metastatic Uveal Melanoma: Patterns of Response and Survival According to the Presence of Hepatic and Extrahepatic Metastasis

 , ,
, ,  , , , , , , , and add
Show full author list
, , , , , , , and add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population and Study Design
2.2. Data Collection and Treatment Outcomes
2.3. Statistical Analyses
3. Results
3.1. Baseline Patient Characteristics
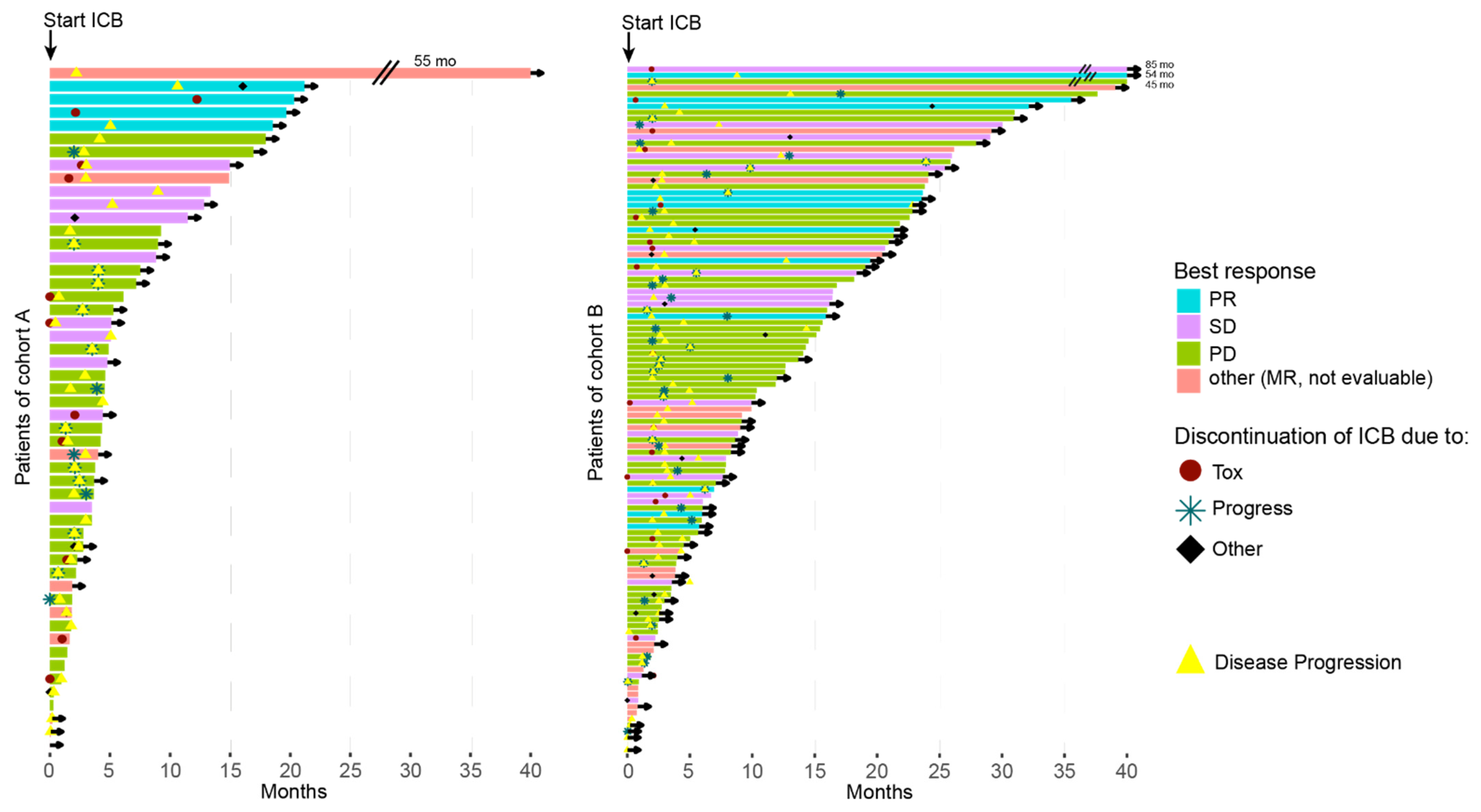
3.2. Response Rates to ICB
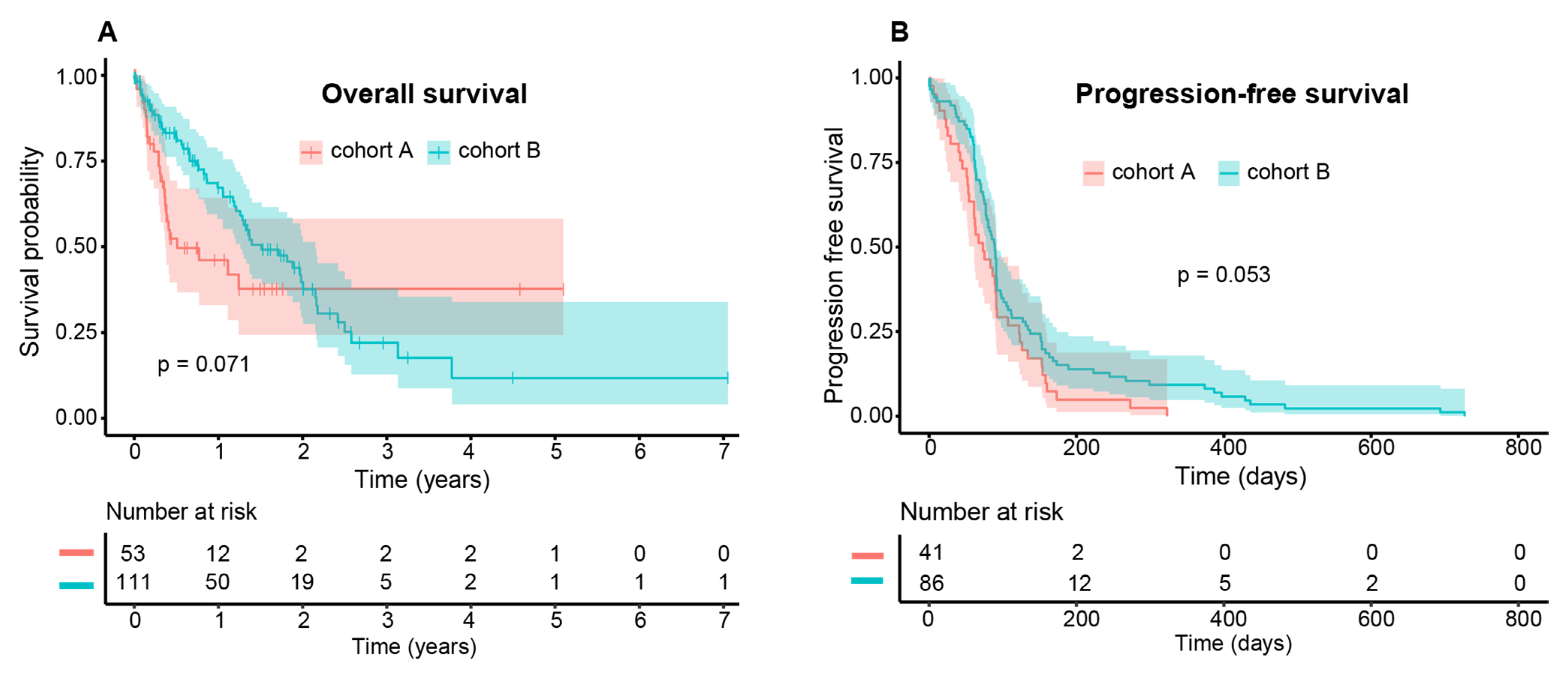
3.3. Survival Data
3.4. Adverse Events (AE)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gonzales, C.A.; Ladas, J.G.; Davis, J.L.; Feuer, W.J.; Holland, G.N. Collaborative ocular melanoma study group. Assessment of metastatic disease status at death in 435 patients with large choroidal melanoma in the collaborative ocular melanoma study (COMS). Arch. Ophthalmol. 2001, 119, 670–676. [Google Scholar] [CrossRef]
- Heppt, M.V.; Steeb, T.; Schlager, J.G.; Rosumeck, S.; Dressler, C.; Ruzicka, T.; Nast, A.; Berking, C. Immune checkpoint blockade for unresectable or metastatic uveal melanoma: A systematic review. Cancer Treat. Rev. 2017, 60, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Rantala, E.S.; Hernberg, M.; Kivelä, T.T. Overall survival after treatment for metastatic uveal melanoma: A systematic review and meta-analysis. Melanoma Res. 2019, 29, 561–568. [Google Scholar] [CrossRef] [PubMed]
- Piulats, J.M.; Espinosa, E.; Merino, L.D.L.C.; Varela, M.; Carrión, L.A.; Martín-Algarra, S.; Castro, R.L.; Curiel, T.; Rodríguez-Abreu, D.; Redrado, M.; et al. Nivolumab plus ipilimumab for treatment-naïve metastatic uveal melanoma: An open-label, multicenter, phase II trial by the Spanish multidisciplinary melanoma group (GEM-1402). J. Clin. Oncol. 2021, 39, 586–598. [Google Scholar] [CrossRef] [PubMed]
- Pelster, M.S.; Gruschkus, S.K.; Bassett, R.; Gombos, D.S.; Shephard, M.; Liberty, P.; Glover, M.S.; Simien, R.; Diab, A.; Hwu, P.; et al. Nivolumab and ipilimumab in metastatic uveal melanoma: Results from a single-arm phase II study. J. Clin. Oncol. 2021, 39, 599–607. [Google Scholar] [CrossRef]
- Khoja, L.; Atenafu, E.; Suciu, S.; Leyvraz, S.; Sato, T.; Marshall, E.; Keilholz, U.; Zimmer, L.; Patel, S.; Piperno-Neumann, S.; et al. Meta-analysis in metastatic uveal melanoma to determine progression free and overall survival benchmarks: An international rare cancers initiative (IRCI) ocular melanoma study. Ann. Oncol. 2019, 30, 1370–1380. [Google Scholar] [CrossRef]
- Heppt, M.V.; Heinzerling, L.; Kähler, K.C.; Forschner, A.; Kirchberger, M.C.; Loquai, C.; Meissner, M.; Meier, F.; Terheyden, P.; Schell, B.; et al. Prognostic factors and outcomes in metastatic uveal melanoma treated with programmed cell death-1 or combined PD-1/cytotoxic T-lymphocyte antigen-4 inhibition. Eur. J. Cancer 2017, 82, 56–65. [Google Scholar] [CrossRef]
- Wessely, A.; Steeb, T.; Erdmann, M.; Heinzerling, L.; Vera, J.; Schlaak, M.; Berking, C.; Heppt, M.V. The Role of Immune Checkpoint Blockade in Uveal Melanoma. Int. J. Mol. Sci. 2020, 21, 879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Najjar, Y.G.; Navrazhina, K.; Ding, F.; Bhatia, R.; Tsai, K.; Abbate, K.; Durden, B.; Eroglu, Z.; Bhatia, S.; Park, S.; et al. Ipilimumab plus nivolumab for patients with metastatic uveal melanoma: A multicenter, retrospective study. J. Immunother. Cancer 2020, 8, e000331. [Google Scholar] [CrossRef] [PubMed]
- Heppt, M.V.; Amaral, T.; Kähler, K.C.; Heinzerling, L.; Hassel, J.C.; Meissner, M.; Kreuzberg, N.; Loquai, C.; Reinhardt, L.; Utikal, J.; et al. Combined immune checkpoint blockade for metastatic uveal melanoma: A retrospective, multi-center study. J. Immunother. Cancer 2019, 7, 299. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Carvajal, R.D. Dual Immunological Checkpoint Blockade for Uveal Melanoma. J. Clin. Oncol. 2021, 39, 554–556. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, I.P.; Long, G.; Quek, C.; Gonzalez, M.; Carlino, M.S.; Long, G.V.; Menzies, A.M. Site-specific response patterns, pseudoprogression, and acquired resistance in patients with melanoma treated with ipilimumab combined with anti–PD-1 therapy. Cancer 2020, 126, 86–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Somasundaram, R.; Zhang, G.; Fukunaga-Kalabis, M.; Perego, M.; Krepler, C.; Xu, X.; Wagner, C.; Hristova, D.; Zhang, J.; Tian, T.; et al. Tumor-associated B-cells induce tumor heterogeneity and therapy resistance. Nat. Commun. 2017, 8, 607. [Google Scholar] [CrossRef] [Green Version]
- Somasundaram, R.; Connelly, T.; Choi, R.; Choi, H.; Samarkina, A.; Li, L.; Gregorio, E.; Chen, Y.; Thakur, R.; Abdel-Mohsen, M.; et al. Tumor-infiltrating mast cells are associated with resistance to anti-PD-1 therapy. Nat. Commun. 2021, 12, 346. [Google Scholar] [CrossRef]
- Lindblad, K.E.; Lujambio, A. Liver metastases inhibit immunotherapy efficacy. Nat. Med. 2021, 27, 25–27. [Google Scholar] [CrossRef]
- Hoefsmit, E.P.; A Rozeman, E.; Van, T.M.; Dimitriadis, P.; Krijgsman, O.; Conway, J.W.; Da Silva, I.P.; E Van Der Wal, J.; Ketelaars, S.L.C.; Bresser, K.; et al. Comprehensive analysis of cutaneous and uveal melanoma liver metastases. J. Immunother. Cancer 2020, 8, e001501. [Google Scholar] [CrossRef]
- Zou, W.; Wolchok, J.D.; Chen, L. PD-L1 (B7-H1) and PD-1 pathway blockade for cancer therapy: Mechanisms, response biomarkers, and combinations. Sci. Transl. Med. 2016, 8, 328rv4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schumacher, T.N.; Schreiber, R.D. Neoantigens in cancer immunotherapy. Science 2015, 348, 69–74. [Google Scholar] [CrossRef] [Green Version]
- Qin, Y.; Bollin, K.; De Macedo, M.P.; Carapeto, F.; Kim, K.B.; Roszik, J.; Wani, K.M.; Reuben, A.; Reddy, S.T.; Williams, M.D.; et al. Immune profiling of uveal melanoma identifies a potential signature associated with response to immunotherapy. J. Immunother. Cancer 2020, 8, e000960. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total | Cohort A | Cohort B | A vs. B | ||
|---|---|---|---|---|---|
| Sex | Women | 89 (50.0%) | 25 (45.5%) | 64 (52.0%) | p = 0.52 |
| Men | 89 (50.0%) | 30 (54.5%) | 59 (48.0%) | ||
| Age | Median in years (range) | 65.6 (17.7–87.6) | 63.4 (32.4–87.6) | 65.8 (17.7–85.4) | p = 0.79 |
| LDH | Not elevated | 42 (23.6%) | 16 (29.1%) | 26 (21.1%) | p = 0.34 |
| Elevated | 89 (50.0%) | 28 (50.9%) | 61 (49.6%) | ||
| NA | 47 (26.4%) | 11 (20.0%) | 36 (29.3%) | ||
| ECOG | ECOG 0 | 88 (49.4%) | 30 (54.5%) | 58 (44.7%) | p = 0.44 |
| ECOG 1 | 20 (11.2%) | 3 (5.5%) | 17 (13.8% | ||
| ECOG 2 | 4 (2.2%) | 1 (1.8%) | 3 (2.4%) | ||
| ECOG 3 | 2 (1.1%) | 1 (1.8%) | 1 (0.8%) | ||
| ECOG 4 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | ||
| ECOG 5 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | ||
| NA | 64 (36.0%) | 20 (36.4%) | 44 (35.8%) | ||
| Number of affected organ systems | Median (range) | 2 (1–7) | 1 | 3 (2–7) | p < 0.001 |
| Affected organ systems | Liver | 178 (100%) | 55 (100%) | 123 (100%) | |
| Pulmonary | 82 (46.1%) | 0 (0.0%) | 82 (66.7%) | ||
| Bone | 47 (26.4%) | 0 (0.0%) | 47 (38.2%) | ||
| CNS | 25 (14.0%) | 0 (0.0%) | 25 (20.3%) | ||
| Lymph node | 41 (23.0%) | 0 (0.0%) | 41 (33.3%) | ||
| Connective tissue | 8 (4.5%) | 0 (0.0%) | 8 (6.5%) | ||
| Skin | 24 (13.5%) | 0 (0.0%) | 24 (19.5%) | ||
| Disseminated | 10 (5.6%) | 0 (0.0%) | 10 (8.1%) | ||
| Other | 51 (28.7%) | 0 (0.0%) | 51 (41.5%) | ||
| ICB as first-line therapy | 146 (82.0%) | 49 (89.1%) | 97 (78.9%) | p = 0.15 | |
| Other therapies | Gemcitabine & Treosulfan | 34 (19.1%) | 4 (7.2%) | 30 (24.3%) | p = 0.013 |
| Nivolumab | 38 (21.3%) | 10 (18.1%) | 28 (22.7%) | p = 0.623 | |
| Pembrolizumab | 25 (14%) | 6 (10.9%) | 19 (15.4%) | p = 0.568 | |
| Sorafenib | 18 (10.1%) | 1 (1.8%) | 17 (13.8%) | p = 0.029 | |
| DC vaccine | 14 (7.8%) | 2 (3.6%) | 12 (9.7%) | p = 0.26 | |
| Dacarbazine | 9 (5%) | 0 (0%) | 9 (7.3%) | p = 0.091 | |
| Trametinib | 10 (5.6%) | 2 (3.6%) | 8 (6.5%) | p = 0.678 | |
| Fotemustine | 9 (5%) | 2 (3.6%) | 7 (5.6%) | p = 0.835 | |
| ICB substance | Any | 177 (99.4%) | 55 (100%) | 122 (99.2%) | p = 1 |
| anti-PD-1 (pembrolizumab, nivolumab) | 53 (29.8%) | 17 (30.9%) | 36 (29.3%) | p = 0.97 | |
| anti-CTLA-4 (ipilimumab) | 15 (8.4%) | 0 (0.0%) | 15 (12.2%) | p = 0.016 | |
| Dual | 109 (61.2%) | 38 (69.1%) | 71 (57.7%) | p = 0.20 | |
| NA | 1 (0.6%) | 0 (0.0%) | 1 (0.8%) |
| ICB—Any Type | Total | Cohort A | Cohort B | Test (Cohorts A vs. B) |
|---|---|---|---|---|
| CR | 0/150 (0.0%) | 0/48 (0.0%) | 0/102 (0.0%) | |
| PR | 17/150 (11.3%) | 5/48 (10.4%) | 12/102 (11.8%) | p = 1 |
| SD | 36/150 (24.0%) | 11/48 (22.9%) | 25/102 (24.5%) | p = 0.99 |
| PD | 91/150 (60.7%) | 30/48 (62.5%) | 61/102 (59.8%) | p = 0.89 |
| ORR | 17/150 (11.3%) | 5/48 (10.4%) | 12/102 (11.8%) | p = 1 |
| DCR | 53/150 (35.3%) | 16/48 (33.3%) | 37/102 (36.3%) | p = 0.87 |
| anti-PD-1 | Total | Cohort A | Cohort B | Test (Cohorts A vs. B) |
| CR | 0/45 (0.0%) | 0/14 (0.0%) | 0/31 (0.0%) | |
| PR | 4/45 (8.9%) | 2/14 (14.3%) | 2/31 (6.5%) | p = 0.77 |
| SD | 9/45 (20%) | 2/14 (14.3%) | 7/31 (22.6%) | p = 0.81 |
| PD | 30/45 (66.7%) | 10/14 (71.4%) | 20/31 (64.5%) | p = 0.91 |
| ORR | 4/45 (8.9%) | 2/14 (14.3%) | 2/31 (6.5%) | p = 0.77 |
| DCR | 13/45 (28.9%) | 4/14 (28.6%) | 9/31 (29.0%) | p = 1 |
| Dual ICB | Total | Cohort A | Cohort B | Test (Cohorts A vs. B) |
| CR | 0/94 (0.0%) | 0/34 (0.0%) | 0/60 (0.0%) | |
| PR | 13/94 (13.8%) | 3/34 (8.7%) | 10/60 (16.7%) | p = 0.45 |
| SD | 25/94 (26.6%) | 9/34 (26.5%) | 16/60 (26.7%) | p = 1 |
| PD | 52/94 (55.3%) | 20/34 (58.8%) | 32/60 (53.3%) | p = 0.77 |
| ORR | 13/94 (13.8%) | 3/34 (8.7%) | 10/60 (16.7%) | p = 0.45 |
| DCR | 38/94 (40.4%) | 12/34 (35.3%) | 26/60 (43.3%) | p = 0.59 |
| anti-CTLA-4 | Total | Cohort A | Cohort B | Test (cohorts A vs. B) |
| CR | 0/11 (0.0%) | 0/0 | 0/11 (0.0%) | Not possible |
| PR | 0/11 (0.0%) | 0/0 | 0/11 (0.0%) | |
| SD | 2/11 (18.2%) | 0/0 | 2/11 (18.2%) | |
| PD | 9/11 (81.8%) | 0/0 | 9/11 (81.8%) | |
| ORR | 0/11 (0.0%) | 0/0 | 0/11 (0.0%) | |
| DCR | 2/11 (18.2%) | 0/0 | 2/11 (18.2%) |
| Total | Cohort A | Cohort B | Test (Cohorts A vs. B) | |
|---|---|---|---|---|
| Number of AE | 133 | 43 | 90 | |
| Number of severe AE | 72 (54.1%) | 24 (55.8%) | 48 (53.3%) | p = 0.93 |
| Number of patients with AE | 74 (41.6%) | 26 (47.3%) | 48 (39.0%) | p = 0.39 |
| Number of patients with severe AE | 47 (26.3%) | 16 (29.1%) | 31 (25.2%) | p = 0.72 |
| anti-PD1 | Dual ICB | Test (Cohorts A vs. B) | ||
| Number of AE | 25 | 103 | ||
| Number of severe AE (grade 3 + 4) | 6 (24.0%) | 60 (58.3%) | p = 0.0044 | |
| Number of patients with AE | 11 (20.8%) | 60 (55.0%) | p < 0.001 | |
| Number of patients with severe AE (grade 3 + 4) | 4 (7.5%) | 34 (31.2%) | p = 0.0017 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koch, E.A.T.; Petzold, A.; Wessely, A.; Dippel, E.; Gesierich, A.; Gutzmer, R.; Hassel, J.C.; Haferkamp, S.; Hohberger, B.; Kähler, K.C.; et al. Immune Checkpoint Blockade for Metastatic Uveal Melanoma: Patterns of Response and Survival According to the Presence of Hepatic and Extrahepatic Metastasis. Cancers 2021, 13, 3359. https://doi.org/10.3390/cancers13133359
Koch EAT, Petzold A, Wessely A, Dippel E, Gesierich A, Gutzmer R, Hassel JC, Haferkamp S, Hohberger B, Kähler KC, et al. Immune Checkpoint Blockade for Metastatic Uveal Melanoma: Patterns of Response and Survival According to the Presence of Hepatic and Extrahepatic Metastasis. Cancers. 2021; 13(13):3359. https://doi.org/10.3390/cancers13133359
Chicago/Turabian StyleKoch, Elias A. T., Anne Petzold, Anja Wessely, Edgar Dippel, Anja Gesierich, Ralf Gutzmer, Jessica C. Hassel, Sebastian Haferkamp, Bettina Hohberger, Katharina C. Kähler, and et al. 2021. "Immune Checkpoint Blockade for Metastatic Uveal Melanoma: Patterns of Response and Survival According to the Presence of Hepatic and Extrahepatic Metastasis" Cancers 13, no. 13: 3359. https://doi.org/10.3390/cancers13133359