The Perceived Impact of Length of the Diagnostic Pathway Is Associated with Health-Related Quality of Life of Sarcoma Survivors: Results from the Dutch Nationwide SURVSARC Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Recruitment and Data Collection
2.3. Study Measures
2.4. Time to Diagnosis
2.5. Health-Related Quality of Life: EORTC QLQ-C30
2.6. Perceived Impact of Diagnostic Interval Length on HRQoL
2.7. Socio-Demographic and Tumour Characteristics
2.8. Coping
2.9. Statistical Analyses
3. Results
3.1. Participants
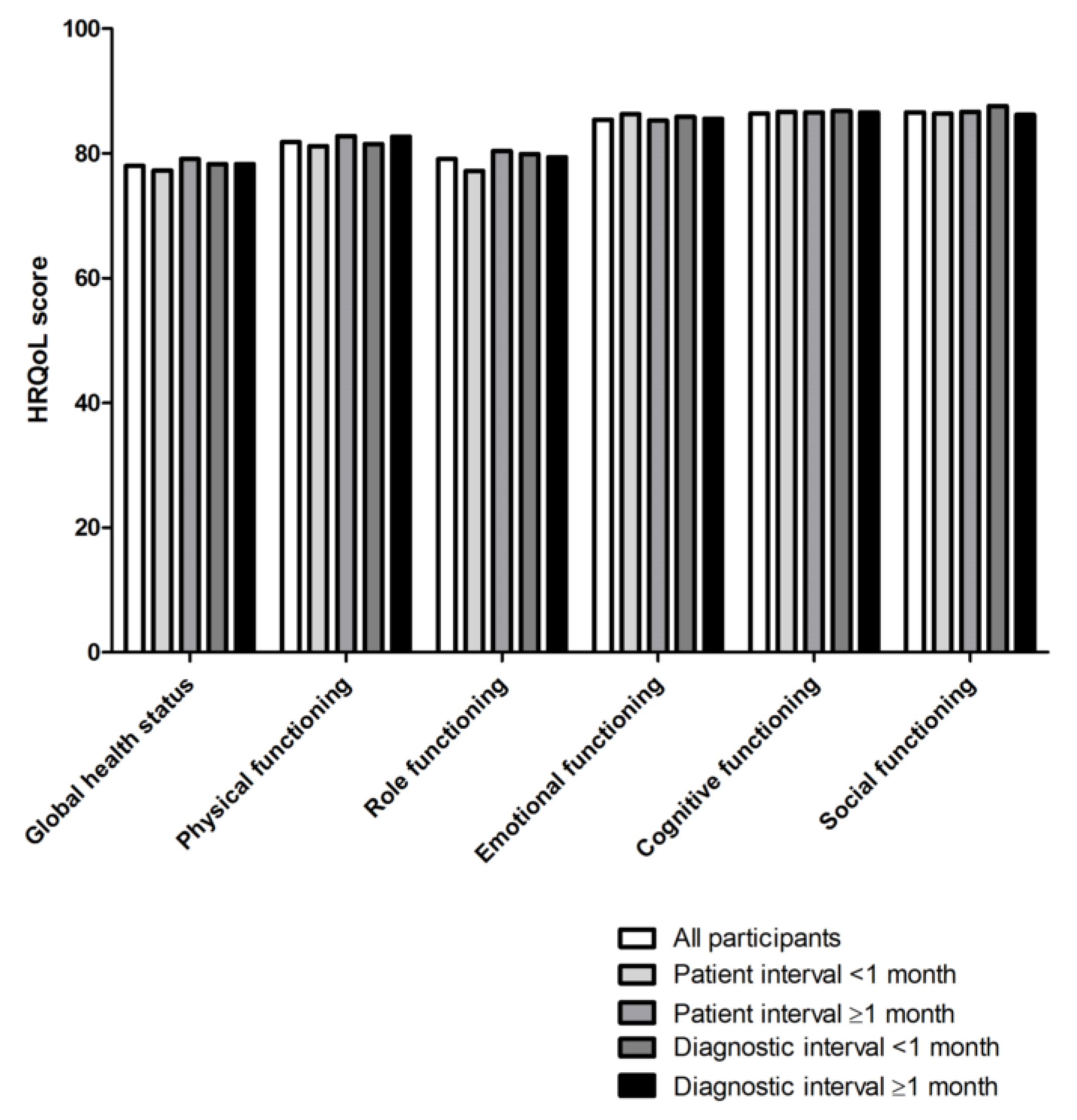
3.2. Health-Related Quality of Life by Patient and Diagnostic Interval Length
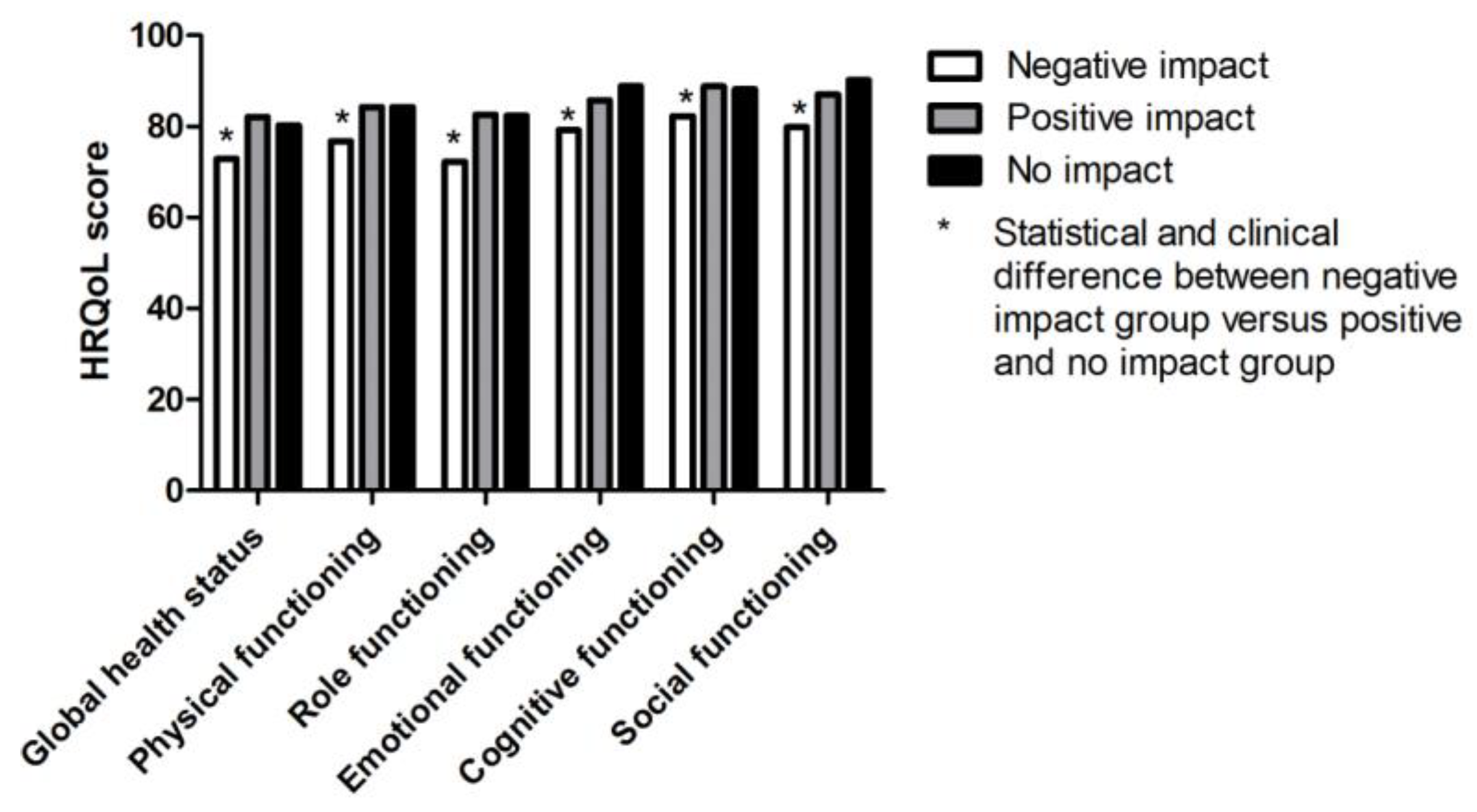
3.3. Influence of Perceived Impact of Diagnostic Interval on HRQoL
3.4. Independent Association of Patient Interval and Patient and Tumour Characteristics with HRQoL
3.5. Independent Association of Diagnostic Interval and Patient and Tumour Characteristics with HRQoL
3.6. Consideration of Patients Who Perceive a Negative Impact of Their Diagnostic Interval Length on HRQoL; Qualitative Analyses
- “Fear, you don’t know when and where it recurs. You continuously monitor your body.”
- “Heavy psychological stress during the diagnostic trajectory.”
- “A lot of pain longer than necessary. Surgical intervention was not possible anymore due to the long diagnostic trajectory.”
- “Then they would not have to cut it out this far, so I would have fewer complaints now.”
- “Yes, because if there had been an earlier intervention, then the sarcoma would not have been this large and I would not have had metastases.”
- “Due to not tackling it immediately it came back twice.”
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Stiller, C.A.; Trama, A.; Serraino, D.; Rossi, S.; Navarro, C.; Chirlaque, M.D.; Casali, P.G. Descriptive epidemiology of sarcomas in Europe: Report from the RARECARE project. Eur. J. Cancer 2013, 49, 684–695. [Google Scholar] [CrossRef] [PubMed]
- IKNL. Overlevingscijfers; IKNL, 2020; Available online: https://www.kanker.nl/kankersoorten/botkanker/wat-is/overlevingscijfers (accessed on 24 July 2020).
- Blay, J.Y.; Coindre, J.M.; Ducimetiere, F.; Ray-Coquard, I. The value of research collaborations and consortia in rare cancers. Lancet Oncol. 2016, 17, e62–e69. [Google Scholar] [CrossRef]
- EORTC. EORTC Quality of Life Group. Available online: https://qol.eortc.org/ (accessed on 24 July 2020).
- Neal, R.D.; Tharmanathan, P.; France, B.; Din, N.U.; Cotton, S.; Fallon-Ferguson, J.; Hamilton, W.; Hendry, A.; Hendry, M.; Lewis, R.; et al. Is increased time to diagnosis and treatment in symptomatic cancer associated with poorer outcomes? Systematic review. Br. J. Cancer 2015, 112 (Suppl. S1), S92–S107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soomers, V.; Husson, O.; Young, R.; Desar, I.; Van der Graaf, W. The sarcoma diagnostic interval: A systematic review on length, contributing factors and patient outcomes. ESMO Open 2020, 5. [Google Scholar] [CrossRef] [Green Version]
- Soomers, V.L.M.N.; van der Graaf, W.T.A.; Zaidi, S.; Kaal, S.; Hayes, A.; Schreuder, H.; Jones, R.L.; Desar, I.M.E.; Husson, O. The route to diagnosis of sarcoma patients: Results from an interview study in the Netherlands and the United Kingdom. PLoS ONE 2020. under review. [Google Scholar]
- (NCI). N.C.I. Dictionary of Cancer Terms. Available online: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/survivorship (accessed on 1 March 2020).
- Soomers, V.L.M.N.; Husson, O.; Desar, I.; van de Sande, M.A.J.; de Haan, J.J.; Verhoef, C.; Vriens, I.J.H.; van Houdt, W.J.; Van de Poll-Franse, L.V.; Van der Graaf, W.T.A. Patient and diagnostic intervals of sarcoma survivors: Results from the SURVSARC study. Cancer 2020. under review. [Google Scholar]
- Van de Poll-Franse, L.V.; Horevoorts, N.; van Eenbergen, M.; Denollet, J.; Roukema, J.A.; Aaronson, N.K.; Vingerhoets, A.; Coebergh, J.W.; de Vries, J.; Essink-Bot, M.L.; et al. The Patient Reported Outcomes Following Initial treatment and Long term Evaluation of Survivorship registry: Scope, rationale and design of an infrastructure for the study of physical and psychosocial outcomes in cancer survivorship cohorts. Eur. J. Cancer 2011, 47, 2188–2194. [Google Scholar] [CrossRef] [Green Version]
- Olesen, F.; Hansen, R.P.; Vedsted, P. Delay in diagnosis: The experience in Denmark. Br. J. Cancer 2009, 101 (Suppl. S2), S5–S8. [Google Scholar] [CrossRef] [Green Version]
- Weller, D.; Vedsted, P.; Rubin, G.; Walter, F.M.; Emery, J.; Scott, S.; Campbell, C.; Andersen, R.S.; Hamilton, W.; Olesen, F.; et al. The Aarhus statement: Improving design and reporting of studies on early cancer diagnosis. Br. J. Cancer 2012, 106, 1262–1267. [Google Scholar] [CrossRef]
- Keeble, S.; Abel, G.A.; Saunders, C.L.; McPhail, S.; Walter, F.M.; Neal, R.D.; Rubin, G.P.; Lyratzopoulos, G. Variation in promptness of presentation among 10,297 patients subsequently diagnosed with one of 18 cancers: Evidence from a National Audit of Cancer Diagnosis in Primary Care. Int. J. Cancer 2014, 135, 1220–1228. [Google Scholar] [CrossRef] [Green Version]
- Forbes, L.J.; Warburton, F.; Richards, M.A.; Ramirez, A.J. Risk factors for delay in symptomatic presentation: A survey of cancer patients. Br. J. Cancer 2014, 111, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Herbert, A.; Lyratzopoulos, G.; Whelan, J.; Taylor, R.M.; Barber, J.; Gibson, F.; Fern, L.A. Diagnostic timeliness in adolescents and young adults with cancer: A cross-sectional analysis of the BRIGHTLIGHT cohort. Lancet Child. Adolesc. Health 2018, 2, 180–190. [Google Scholar] [CrossRef] [Green Version]
- Younger, E.; Husson, O.; Bennister, L.; Whelan, J.; Wilson, R.; Roast, A.; Jones, R.L.; van der Graaf, W.T. Age-related sarcoma patient experience: Results from a national survey in England. BMC Cancer 2018, 18, 991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- SONCOS, S.O.S. Multidisciplinary guideline oncological care in the Netherlands. In SONCOS Normeringsrapport, 8th ed.; 2020; Available online: https://www.soncos.org/kwaliteit/normeringsrapport/ (accessed on 1 April 2020).
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; de Haes, J.C.; et al. The European Organization for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Fayers, P.; Aaronson, N.; Bjordal, K.; Groenvold, M.; Curran, D.; Bottomly, A. The EORTC QLQ-C30 Scoring Manual, 3rd ed.; European Organisation for Research and Treatment of Cancer: Brussels, Belgium, 2001. [Google Scholar]
- Cocks, K.; King, M.T.; Velikova, G.; Martyn St-James, M.; Fayers, P.M.; Brown, J.M. Evidence-based guidelines for determination of sample size and interpretation of the European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30. J. Clin. Oncol. 2011, 29, 89–96. [Google Scholar] [CrossRef]
- Mols, F.; Husson, O.; Oudejans, M.; Vlooswijk, C.; Horevoorts, N.; van de Poll-Franse, L.V. Reference data of the EORTC QLQ-C30 questionnaire: Five consecutive annual assessments of approximately 2000 representative Dutch men and women. Acta Oncol. 2018, 57, 1381–1391. [Google Scholar] [CrossRef] [Green Version]
- Sociaal en Cultureel Planbureau, S. Statusscores. Available online: https://www.scp.nl/english;https://www.scp.nl/Onderzoek/Statusscores (accessed on 24 July 2020).
- Lazarus, R.S. Coping theory and research: Past, present, and future. Psychosom. Med. 1993, 55, 234–247. [Google Scholar] [CrossRef]
- Evers, A.W.; Kraaimaat, F.W.; van Lankveld, W.; Jongen, P.J.; Jacobs, J.W.; Bijlsma, J.W. Beyond unfavorable thinking: The illness cognition questionnaire for chronic diseases. J. Consult. Clin. Psychol. 2001, 69, 1026–1036. [Google Scholar] [CrossRef]
- Jarkovsky, J.; Skrivanova, K.; Benesova, K.; Snajdrova, L.; Gregor, J.; Peterkova, H.; Bendova, M.; Brancikova, D.; Elfmarkova, N.; Sverak, T.; et al. Predictors of quality of life in Czech female breast cancer survivors following treatment with special interest to coping strategies. Vnitr. Lek. 2017, 63, 389–396. [Google Scholar]
- Pan, C.J.; Liu, H.C.; Liang, S.Y.; Liu, C.Y.; Wu, W.W.; Cheng, S.F. Resilience and Coping Strategies Influencing the Quality of Life in Patients With Brain Tumor. Clin. Nurs. Res. 2019, 28, 107–124. [Google Scholar] [CrossRef]
- Chirico, A.; Lucidi, F.; Merluzzi, T.; Alivernini, F.; Laurentiis, M.; Botti, G.; Giordano, A. A meta-analytic review of the relationship of cancer coping self-efficacy with distress and quality of life. Oncotarget 2017, 8, 36800–36811. [Google Scholar] [CrossRef] [Green Version]
- Salika, T.; Abel, G.A.; Mendonca, S.C.; von Wagner, C.; Renzi, C.; Herbert, A.; McPhail, S.; Lyratzopoulos, G. Associations between diagnostic pathways and care experience in colorectal cancer: Evidence from patient-reported data. Frontline Gastroenterol. 2018, 9, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Dahl, T.L.; Vedsted, P.; Jensen, H. The effect of standardised cancer pathways on Danish cancer patients’ dissatisfaction with waiting time. Dan. Med. J. 2017, 64, A5322. [Google Scholar] [PubMed]
- Pham, T.M.; Gomez-Cano, M.; Salika, T.; Jardel, D.; Abel, G.A.; Lyratzopoulos, G. Diagnostic route is associated with care satisfaction independently of tumour stage: Evidence from linked English Cancer Patient Experience Survey and cancer registration data. Cancer Epidemiol. 2019, 61, 70–78. [Google Scholar] [CrossRef]
- Sandager, M.; Jensen, H.; Lipczak, H.; Sperling, C.D.; Vedsted, P. Cancer patients’ experiences with urgent referrals to cancer patient pathways. Eur. J. Cancer Care 2019, 28, e12927. [Google Scholar] [CrossRef] [Green Version]
- Stull, D.E.; Leidy, N.K.; Parasuraman, B.; Chassany, O. Optimal recall periods for patient-reported outcomes: Challenges and potential solutions. Curr. Med. Res. Opin. 2009, 25, 929–942. [Google Scholar] [CrossRef] [PubMed]
- Burt, C.D.; Kemp, S.; Conway, M. What happens if you retest autobiographical memory 10 years on? Mem. Cognit. 2001, 29, 127–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| All Patients (n = 1099) | |
|---|---|
| Gender n (%) | |
| Male | 595 (54) |
| Female | 504 (46) |
| Age at diagnosis in years: Mean (SD) | 54.6 (15.4) |
| Socio-economic status n (%) | |
| Low | 286 (26.1) |
| Intermediate | 462 (42.1) |
| High | 349 (31.8) |
| Coping: mean (SD) | |
| Helplessness | 8.8 (3.6) |
| Acceptance | 18.8 (4.2) |
| Disease benefits | 15.8 (4.8) |
| Time since diagnosis in months: Mean (SD) | 67.4 (30.4) |
| Location n (%) | |
| Extremities | 514 (47) |
| Non-extremities | 585 (53) |
| Histology n (%) | |
| Soft tissue sarcoma | 835 (76) |
| Dermatofibrosarcoma protuberans | 74 (7) |
| Liposarcoma | 177 (16) |
| Myxofibrosarcoma | 137 (13) |
| Leiomyosarcoma | 113 (10) |
| Rhabdomyosarcoma | 15 (1) |
| Malignant peripheral nerve sheath tumors (MPNST) | 34 (3) |
| Synovial sarcoma | 35 (3) |
| Vascular sarcoma | 43 (4) |
| Other soft tissue sarcoma | 201 (18) |
| Bone sarcoma | 264 (24) |
| Osteosarcoma | 69 (6) |
| Chondrosarcoma | 130 (12) |
| Chordoma | 30 (3) |
| Ewing sarcoma | 28 (3) |
| Other bone sarcoma | 13 (1) |
| Grade n (%) | |
| Low grade | 614 (60) |
| Intermediate or high grade | 407 (40) |
| Metastases at diagnosis n (%) | |
| Not present | 1067 (97) |
| Present | 32 (3) |
| Treatment modalities n (%) | |
| Surgery | 448 (43) |
| Surgery and radiotherapy | 422 (41) |
| Surgery and chemotherapy | 79 (8) |
| Surgery and radiotherapy and chemotherapy | 86 (8) |
| Global QoL | Physical Functioning | Role Functioning | Emotional Functioning | Cognitive Functioning | Social Functioning | |
|---|---|---|---|---|---|---|
| Patient interval | ||||||
| <1 month | ref | ref | ref | ref | ref | ref |
| ≥1 month | 0.031 | 0.017 | 0.047 | –0.032 | –0.006 | –0.008 |
| Perceived impact of diagnostic interval length | ||||||
| –negative | ref | ref | ref | ref | ref | ref |
| –positive | 0.088 ** | 0.040 | 0.044 | 0.026 | 0.051 | 0.027 |
| –no impact | 0.065 * | 0.032 | 0.034 | 0.092 ** | 0.044 | 0.086 ** |
| Gender | ||||||
| –male | ref | ref | ref | ref | ref | ref |
| –female | –0.038 | –0.064 * | 0.009 | –0.039 | –0.042 | –0.010 |
| Age at diagnosis | –0.018 | –0.231 ** | –0.086 ** | 0.174 ** | 0.103 ** | 0.071 * |
| Socio–economic status | ||||||
| –low | ref | ref | ref | ref | ref | ref |
| –intermediate | 0.029 | 0.060* | 0.007 | 0.014 | –0.019 | 0.018 |
| –high | 0.034 | 0.062* | 0.029 | 0.020 | 0.044 | 0.038 |
| Coping | ||||||
| –helplessness | –0.441 ** | –0.601 ** | –0.601 ** | –0.386 ** | –0.323 ** | –0.518 ** |
| –acceptance | 0.157 ** | –0.005 | 0.063 * | 0.239 ** | 0.113 ** | 0.122 ** |
| –disease benefits | 0.118 ** | 0.017 | 0.030 | 0.010 | 0.013 | 0.011 |
| Time since diagnosis | –0.036 | –0.064 ** | –0.035 | 0.042 | 0.005 | –0.006 |
| Location | ||||||
| –non–extremity | ref | ref | (0.0 ref) | ref | ref | ref |
| –extremity | 0.081 ** | –0.060 * | 0.037 | 0.049 | 0.106 ** | 0.045 |
| Histology # | ||||||
| –dermatofibrosarcoma | ref | ref | ref | ref | ref | ref |
| –liposarcoma | –0.103 * | 0.041 | 0.063 | 0.12 | 0.061 | 0.000 |
| –myxofibrosarcoma | –0.135 ** | 0.013 | 0.013 | –0.025 | –0.020 | –0.035 |
| –leiomyosarcoma | –0.058 | 0.036 | 0.087 * | –0.026 | –0.018 | 0.040 |
| –rhabdomyosarcoma | 0.011 | 0.011 | 0.042 | 0.018 | 0.031 | 0.044 |
| –malignant peripheral nerve sheath tumors (MPNST) | 0.000 | –0.065 * | –0.005 | 0.010 | 0.002 | 0015 |
| –synovial | –0.037 | 0.015 | –0.014 | 0.013 | 0.019 | 0.002 |
| sarcoma | ||||||
| –vascular | –0.014 | –0.019 | –0.001 | –0.020 | 0.023 | –0.006 |
| sarcoma | ||||||
| –other STS | –0.132 * | 0.041 | 0.049 | 0.078 | 0.028 | 0.034 |
| –osteosarcoma | –0.053 | –0.098 ** | –0.049 | 0.067 | 0.026 | 0.026 |
| –chondrosarcoma | –0.075 | –0.048 | –0.041 | 0.061 | 0.010 | 0.011 |
| –chordoma | –0.125 ** | –0.102 ** | –0.042 | –0.008 | 0.003 | –0.046 |
| –Ewing sarcoma | –0.012 | –0.033 | 0.010 | 0.080 * | –0.002 | 0.028 |
| –other BS | –0.042 | –0.024 | 0.003 | 0.007 | 0.026 | 0.014 |
| Grade | ||||||
| –low | ref | ref | ref | ref | ref | |
| –high | –0.059 | –0.055 | –0.044 | –0.011 | –0.014 | |
| Metastases at diagnosis | ||||||
| –not present | ref | ref | ref | ref | ref | ref |
| –present | –0.037 | 0.027 | –0.016 | –0.054 | –0.038 | |
| Treatment modality | ||||||
| –surgery plus | ref | ref | ref | ref | ref | ref |
| CHx, RTx, or both | ||||||
| –surgery alone | –0.009 | –0.002 | 0.000 | 0.079 * | 0.028 |
| Global QoL | Physical Functioning | Role Functioning | Emotional Functioning | Cognitive Functioning | Social Functioning | |
|---|---|---|---|---|---|---|
| Diagnostic interval | ||||||
| <1 month | ref | ref | ref | ref | ref | ref |
| ≥1 month | 0.012 | 0.016 | –0.015 | 0.019 | 0.012 | –0.027 |
| Perceived impact of diagnostic interval length | ||||||
| –negative | ref | ref | ref | ref | ref | ref |
| –positive | 0.087 ** | 0.042 | 0.035 | 0.034 | 0.055 | 0.021 |
| –no impact | 0.066 * | 0.035 | 0.027 | 0.099 ** | 0.048 | 0.079 * |
| Gender | ||||||
| –male | ref | ref | ref | ref | ref | ref |
| –female | –0.037 | –0.064 ** | 0.011 | –0.041 | –0.043 | –0.009 |
| Age at diagnosis | –0.018 | –0.230 ** | –0.089 ** | 0.177 ** | 0.104 ** | 0.069 * |
| Socio–economic status | ||||||
| –low | ref | ref | ref | ref | ref | ref |
| –intermediate | 0.029 | 0.060 * | 0.007 | 0.015 | –0.019 | 0.018 |
| –high | 0.035 | 0.062 * | 0.03 | 0.019 | 0.044 | 0.038 |
| Coping | ||||||
| –helplessness | –0.441 ** | –0.600 ** | –0.604 ** | –0.384 ** | –0.322 ** | –0.520 ** |
| –acceptance | 0.157 ** | –0.005 | 0.064 * | 0.238 ** | 0.113 ** | 0.122 ** |
| –disease benefits | 0.117 ** | 0.017 | 0.027 | 0.012 | 0.014 | 0.01 |
| Time since diagnosis | –0.036 | –0.066 ** | –0.035 | 0.042 | 0.005 | –0.007 |
| Location | ||||||
| –non–extremity | ref | ref | ref | ref | ref | ref |
| –extremity | 0.083 ** | –0.059 * | 0.04 | 0.046 | 0.105 ** | 0.045 |
| Histology # | ||||||
| –dermatofibrosarcoma | ref | ref | ref | ref | ref | ref |
| –liposarcoma | –0.110 * | 0.037 | 0.054 | 0.017 | 0.061 | 0.003 |
| –myxofibrosarcoma | –0.141 ** | 0.009 | 0.005 | –0.02 | –0.02 | –0.032 |
| –leiomyosarcoma | –0.062 | 0.033 | 0.083 * | –0.024 | –0.018 | 0.043 |
| –rhabdomyosarcoma | 0.008 | 0.009 | 0.038 | 0.021 | 0.031 | 0.045 |
| –malignant peripheral nerve sheath tumors (MPNST) | –0.003 | –0.067* | –0.007 | 0.01 | 0.002 | 0.017 |
| –synovial | –0.039 | 0.013 | –0.012 | 0.011 | 0.017 | 0.005 |
| sarcoma | ||||||
| –vascular | –0.018 | –0.022 | –0.006 | –0.017 | 0.023 | –0.004 |
| sarcoma | ||||||
| –other STS | –0.139 ** | 0.037 | 0.04 | 0.084 | 0.029 | 0.038 |
| –osteosarcoma | –0.055 | –0.100 ** | –0.051 | 0.068 | 0.026 | 0.028 |
| –chondrosarcoma | –0.079 | –0.051 | –0.042 | 0.061 | 0.009 | 0.015 |
| –chordoma | –0.127 ** | –0.103 ** | –0.042 | –0.008 | 0.003 | –0.044 |
| –Ewing sarcoma | –0.013 | –0.034 | 0.008 | 0.081 * | –0.001 | 0.029 |
| –other BS | –0.044 | –0.025 | –0.001 | 0.009 | 0.026 | 0.014 |
| Grade | ||||||
| –low | ref | ref | ref | ref | ref | ref |
| –high | –0.058 | –0.054 | –0.011 | –0.044 | –0.01 | –0.015 |
| Metastases at diagnosis | ||||||
| –not present | ref | ref | ref | ref | ref | ref |
| –present | –0.037 | 0.027 | 0.005 | –0.017 | –0.054 | –0.037 |
| Treatment modality | ||||||
| –surgery plus | ref | ref | ref | ref | ref | ref |
| CHx, RTx, or both | ||||||
| –surgery alone | –0.006 | –0.001 | 0.037 | –0.003 | 0.078* | 0.028 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soomers, V.L.M.N.; Desar, I.M.E.; van de Poll-Franse, L.V.; van de Sande, M.A.J.; de Haan, J.J.; Verhoef, C.; Vriens, I.J.H.; van Houdt, W.J.; Bonenkamp, J.J.; van der Graaf, W.T.A.; et al. The Perceived Impact of Length of the Diagnostic Pathway Is Associated with Health-Related Quality of Life of Sarcoma Survivors: Results from the Dutch Nationwide SURVSARC Study. Cancers 2020, 12, 2088. https://doi.org/10.3390/cancers12082088
Soomers VLMN, Desar IME, van de Poll-Franse LV, van de Sande MAJ, de Haan JJ, Verhoef C, Vriens IJH, van Houdt WJ, Bonenkamp JJ, van der Graaf WTA, et al. The Perceived Impact of Length of the Diagnostic Pathway Is Associated with Health-Related Quality of Life of Sarcoma Survivors: Results from the Dutch Nationwide SURVSARC Study. Cancers. 2020; 12(8):2088. https://doi.org/10.3390/cancers12082088
Chicago/Turabian StyleSoomers, Vicky L. M. N., Ingrid M. E. Desar, Lonneke V. van de Poll-Franse, Michiel A. J. van de Sande, Jacco J. de Haan, Cornelis Verhoef, Ingeborg J. H. Vriens, Winan J. van Houdt, Johannes J. Bonenkamp, Winette T. A. van der Graaf, and et al. 2020. "The Perceived Impact of Length of the Diagnostic Pathway Is Associated with Health-Related Quality of Life of Sarcoma Survivors: Results from the Dutch Nationwide SURVSARC Study" Cancers 12, no. 8: 2088. https://doi.org/10.3390/cancers12082088