
A Framework to Predict Gastric Cancer Based on Tongue Features and Deep Learning

Abstract
:1. Introduction
2. Related Works
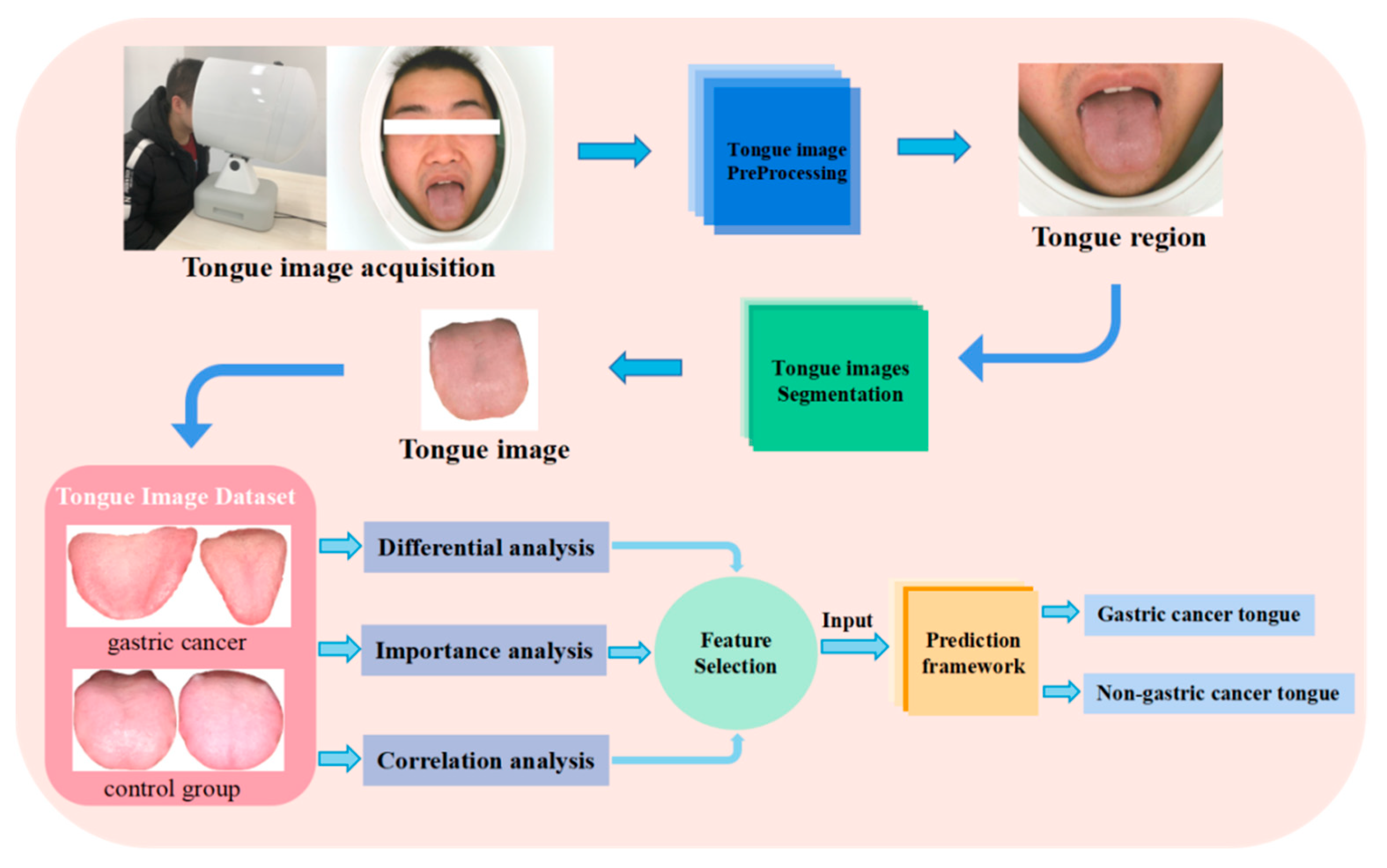
3. Methods
3.1. Date Sources
3.2. Date Preprocess
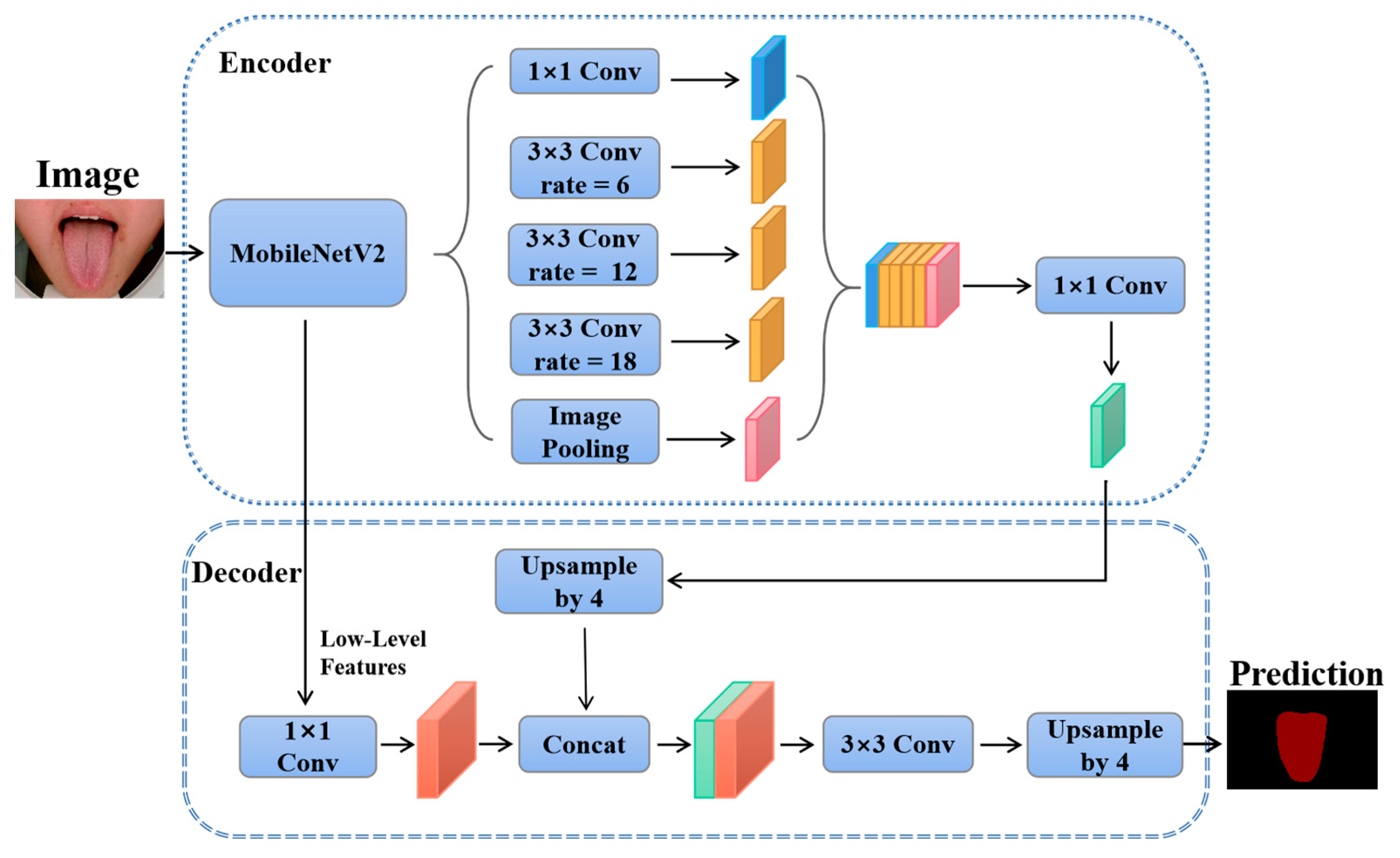
3.3. Segmentation of Tongue Images
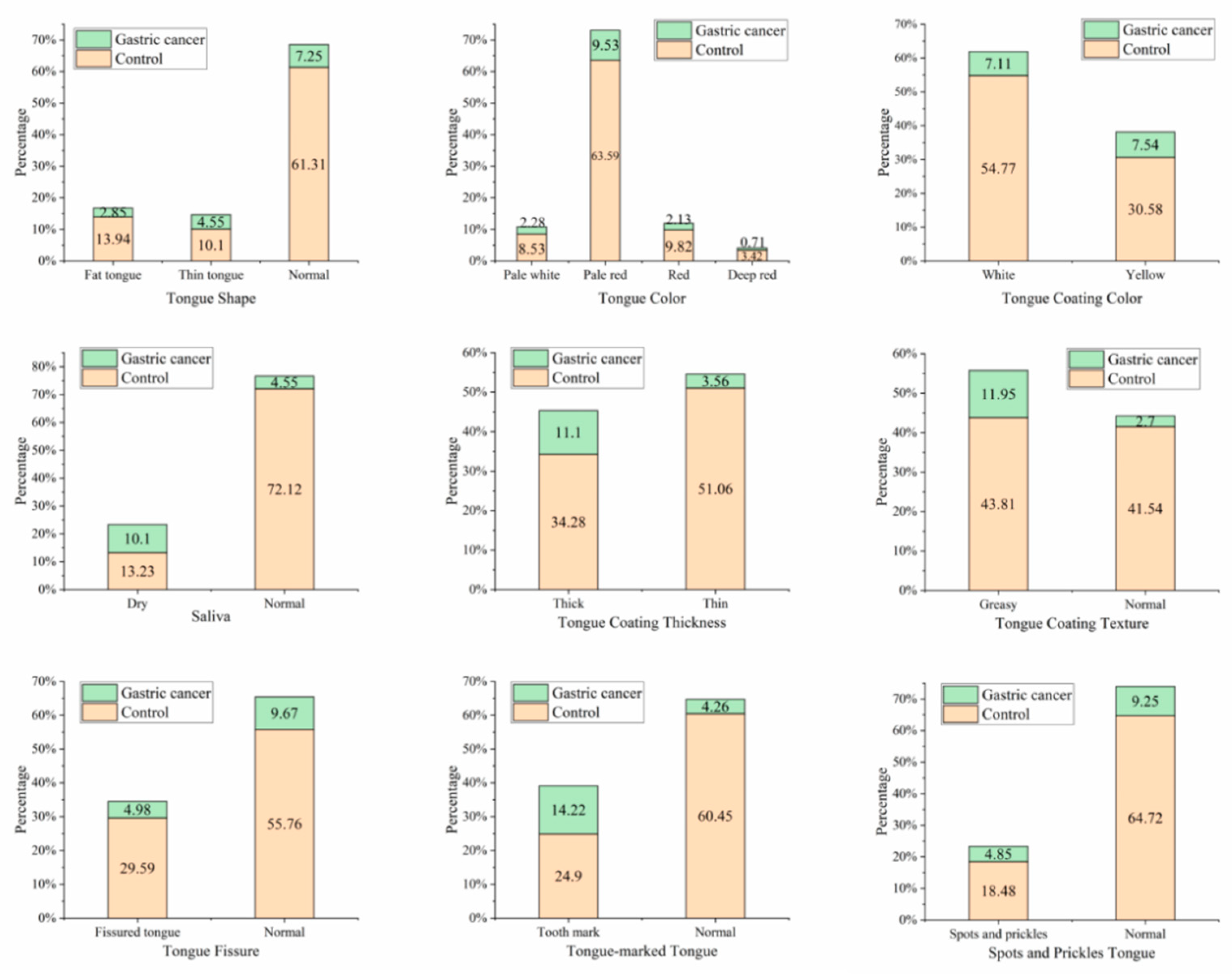
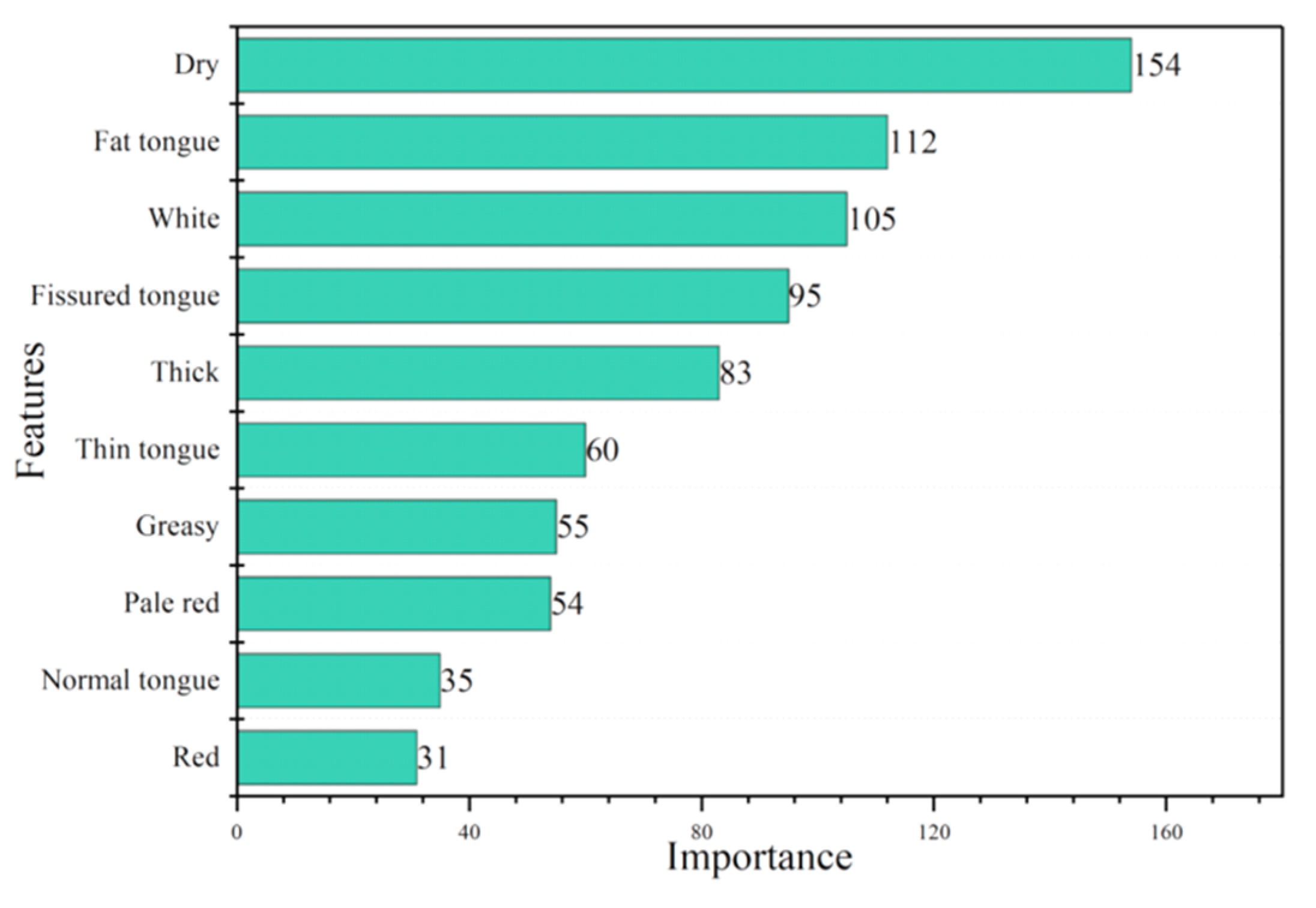
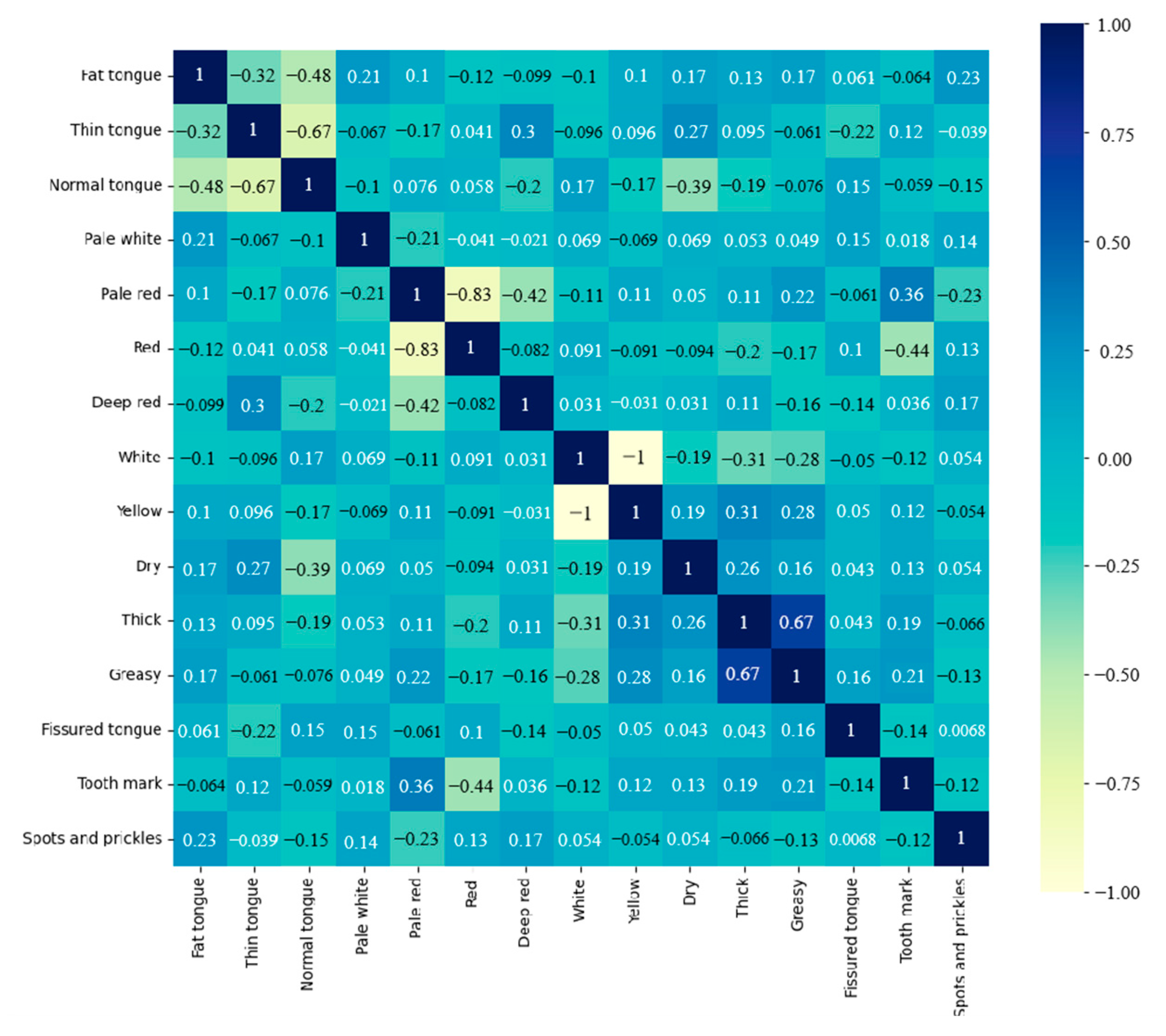
3.4. Extraction and Analysis of Tongue Features
- Tongue shape: fat tongue, thin tongue and normal tongue;
- Tooth-marked tongue: tooth mark and normal;
- Spots and prickles tongue: Spots and prickles and normal;
- Saliva: dry and normal;
- Tongue coating thickness: thick and thin;
- Tongue coating texture: greasy and normal;
- Tongue color: pale white, pale red, red and deep red;
- Tongue coating color: white and yellow;
- Tongue Fissure: fissured tongue and normal.
3.5. Performance Metrics
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Smyth, E.C.; Nilsson, M.; Grabsch, H.I.; van Grieken, N.C.T.; Lordick, F. Gastric cancer. Lancet 2020, 396, 635–648. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.L.; Huang, H.C.; Juan, H.F. Discovery of biomarkers for gastric cancer: A proteomics approach. J. Proteom. 2012, 75, 3081–3097. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Kim, S.G.; Im, J.P.; Kim, J.S.; Jung, H.C.; Song, I.S. Comparison of endoscopic ultrasonography and conventional endoscopy for prediction of depth of tumor invasion in early gastric cancer. Endoscopy 2010, 42, 705–713. [Google Scholar] [CrossRef] [PubMed]
- Yao, K.; Uedo, N.; Kamada, T.; Hirasawa, T.; Nagahama, T.; Yoshinaga, S.; Oka, M.; Inoue, K.; Mabe, K.; Yao, T.; et al. Guidelines for endoscopic diagnosis of early gastric cancer. Dig. Endosc. 2020, 32, 663–698. [Google Scholar] [CrossRef] [PubMed]
- Ueyama, H.; Kato, Y.; Akazawa, Y.; Yatagai, N.; Komori, H.; Takeda, T.; Matsumoto, K.; Ueda, K.; Matsumoto, K.; Hojo, M.; et al. Application of artificial intelligence using a convolutional neural network for diagnosis of early gastric cancer based on magnifying endoscopy with narrow-band imaging. J. Gastroenterol. Hepatol. 2021, 36, 482–489. [Google Scholar] [CrossRef]
- Niikura, R.; Aoki, T.; Shichijo, S.; Yamada, A.; Kawahara, T.; Kato, Y.; Hirata, Y.; Hayakawa, Y.; Suzuki, N.; Ochi, M.; et al. Artificial intelligence versus expert endoscopists for diagnosis of gastric cancer in patients who have undergone upper gastrointestinal endoscopy. Endoscopy 2022, 54, 780–784. [Google Scholar] [CrossRef] [PubMed]
- Emir, T.; Denijal, T. Systemic air embolism as a complication of gastroscopy. Oxf. Med. Case Reports. 2019, 2019, omz057. [Google Scholar] [CrossRef]
- Tania, M.H.; Lwin, K.; Hossain, M.A. Advances in automated tongue diagnosis techniques. Integr. Med. Res. 2019, 8, 42–56. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.R.; Choi, W.; Yeo, I.; Nam, D.H. Comparative Analysis of Tongue Indices between Patients with and without a Self-Reported Yin Deficiency: A Cross-Sectional Study. Evid.-Based Complement. Altern. Med. 2017, 2017, 1279052. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Han, G.; Ko, S.J.; Nam, D.H.; Park, J.W.; Ryu, B.; Kim, J. Tongue diagnosis system for quantitative assessment of tongue coating in patients with functional dyspepsia: A clinical trial. J. Ethnopharmacol. 2014, 155, 709–713. [Google Scholar] [CrossRef]
- Zhang, B.; Wang, X.; You, J.; Zhang, D. Tongue color analysis for medical application. Evid.-Based Complement. Altern. Med. 2013, 2013, 264742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cui, Y.; Liao, S.; Wang, H. ROC-Boosting: A Feature Selection Method for Health Identification Using Tongue Image. Comput. Math. Methods Med. 2015, 2015, 362806. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Wen, G.; Wang, C.; Jiang, L. Complexity perception classification method for tongue constitution recognition. Artif. Intell. Med. 2019, 96, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Li, J.; Li, Z.; Zhu, Z.; Shen, C.; Qi, G.; Yu, G. Detection of Diseases Using Machine Learning Image Recognition Technology in Artificial Intelligence. Comput. Intell. Neurosci. 2022, 2022, 5658641. [Google Scholar] [CrossRef] [PubMed]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Lo, L.C.; Cheng, T.L.; Chen, Y.J.; Natsagdorj, S.; Chiang, J.Y. TCM tongue diagnosis index of early-stage breast cancer. Complement. Ther. Med. 2015, 23, 705–713. [Google Scholar] [CrossRef]
- Li, J.; Yuan, P.; Hu, X.; Huang, J.; Cui, L.; Cui, J.; Ma, X.; Jiang, T.; Yao, X.; Li, J.; et al. A tongue features fusion approach to predicting prediabetes and diabetes with machine learning. J. Biomed. Inform. 2021, 115, 103693. [Google Scholar] [CrossRef] [PubMed]
- Cui, J.; Cui, H.; Yang, M.; Du, S.; Li, J.; Li, Y.; Liu, L.; Zhang, X.; Li, S. Tongue coating microbiome as a potential biomarker for gastritis including precancerous cascade. Protein Cell 2019, 10, 496–509. [Google Scholar] [CrossRef] [Green Version]
- Li, W.Q.; Ma, J.L.; Zhang, L.; Brown, L.M.; Li, J.Y.; Shen, L.; Pan, K.F.; Liu, W.D.; Hu, Y.; Han, Z.X.; et al. Effects of Helicobacter pylori treatment on gastric cancer incidence and mortality in subgroups. J. Natl. Cancer Inst. 2014, 106. [Google Scholar] [CrossRef] [Green Version]
- Kainuma, M.; Furusyo, N.; Urita, Y.; Nagata, M.; Ihara, T.; Oji, T.; Nakaguchi, T.; Namiki, T.; Hayashi, J. The association between objective tongue color and endoscopic findings: Results from the Kyushu and Okinawa population study (KOPS). BMC Complement. Altern. Med. 2015, 15, 372. [Google Scholar] [CrossRef]
- Hu, J.; Han, S.; Chen, Y.; Ji, Z. Variations of Tongue Coating Microbiota in Patients with Gastric Cancer. Biomed. Res. Int. 2015, 2015, 173729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, J.; Xiang, C.; Zhang, C.; Xu, B.; Wu, J.; Wang, R.; Yang, Y.; Shi, L.; Zhang, J.; Zhan, Z. Microbial biomarkers of common tongue coatings in patients with gastric cancer. Microb. Pathog. 2019, 127, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Gholami, E.; Kamel Tabbakh, S.R.; Kheirabadi, M. Increasing the accuracy in the diagnosis of stomach cancer based on color and lint features of tongue. Biomed. Signal Process. Control 2021, 69, 102782. [Google Scholar] [CrossRef]
- Tan, M.; Le, Q.V. Efficientnet: Rethinking model scaling for convolutional neural networks. arXiv 2019, arXiv:1905.11946. [Google Scholar]
- Xiao, Z.; Ji, D.; Li, F.; Li, Z.; Bao, Z. Application of Artificial Intelligence in Early Gastric Cancer Diagnosis. Digestion 2022, 103, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Chen, Y.; Shen, Z.; Zhang, X.; Sang, J.; Ding, Y.; Yang, X.; Li, J.; Chen, M.; Jin, C.; et al. Convolutional neural network for the diagnosis of early gastric cancer based on magnifying narrow band imaging. Gastric Cancer 2020, 23, 126–132. [Google Scholar] [CrossRef] [Green Version]
- Hirasawa, T.; Aoyama, K.; Tanimoto, T.; Ishihara, S.; Shichijo, S.; Ozawa, T.; Ohnishi, T.; Fujishiro, M.; Matsuo, K.; Fujisaki, J.; et al. Application of artificial intelligence using a convolutional neural network for detecting gastric cancer in endoscopic images. Gastric Cancer 2018, 21, 653–660. [Google Scholar] [CrossRef] [Green Version]
- Huang, L.; Zhu, Y.; Xu, C.; Cai, Y.; Yi, Y.; Li, K.; Ren, X.; Jiang, D.; Ge, Y.; Liu, X.; et al. Noninvasive Diagnosis of Gastric Cancer Based on Breath Analysis with a Tubular Surface-Enhanced Raman Scattering Sensor. ACS. Sens. 2022, 7, 1439–1450. [Google Scholar] [CrossRef]
- Hanna, G.B.; Boshier, P.R.; Markar, S.R.; Romano, A. Accuracy and Methodologic Challenges of Volatile Organic Compound-Based Exhaled Breath Tests for Cancer Diagnosis: A Systematic Review and Meta-analysis. JAMA Oncol. 2019, 5, 182815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, S.; Gao, H.; He, J.; Shi, J.; Tong, Y.; Wu, J. Machine learning: A non-invasive prediction method for gastric cancer based on a survey of lifestyle behaviors. Front. Artif. Intell. 2022, 5, 956385. [Google Scholar] [CrossRef]
- Zhu, S.L.; Dong, J.; Zhang, C.; Huang, Y.B.; Pan, W. Application of machine learning in the diagnosis of gastric cancer based on noninvasive characteristics. PLoS ONE 2020, 15, e0244869. [Google Scholar] [CrossRef] [PubMed]
- Hsu, P.C.; Wu, H.K.; Huang, Y.C.; Chang, H.H.; Lee, T.C.; Chen, Y.P.; Chiang, J.Y.; Lo, L.C. The tongue features associated with type 2 diabetes mellitus. Medicine 2019, 98, e15567. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Chen, Q.; Hu, X.; Yuan, P.; Cui, L.; Tu, L.; Cui, J.; Huang, J.; Jiang, T.; Ma, X.; et al. Establishment of noninvasive diabetes risk prediction model based on tongue features and machine learning techniques. Int. J. Med. Inform. 2021, 149, 104429. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Zhang, Z.; Zhu, X.; Zhao, Y.; Ma, Y.; Zang, J.; Li, B.; Cao, X.; Xue, C. Automatic Classification Framework of Tongue Feature Based on Convolutional Neural Networks. Micromachines 2022, 13, 501. [Google Scholar] [CrossRef]
- Shorten, C.; Khoshgoftaar, T.M. A survey on Image Data Augmentation for Deep Learning. J. Big Data 2019, 6, 60. [Google Scholar] [CrossRef]
- Mesejo, P.; Ibáñez, Ó.; Cordón, Ó.; Cagnoni, S. A survey on image segmentation using metaheuristic-based deformable models: State of the art and critical analysis. Appl. Soft Comput. 2016, 44, 1–29. [Google Scholar] [CrossRef] [Green Version]
- Pang, B.; Zhang, D.; Wang, K. The bi-elliptical deformable contour and its application to automated tongue segmentation in Chinese medicine. IEEE Trans. Med. Imaging 2005, 24, 946–956. [Google Scholar] [CrossRef] [Green Version]
- Ning, J.; Zhang, D.; Wu, C.; Yue, F. Automatic tongue image segmentation based on gradient vector flow and region merging. Neural Comput. Appl. 2010, 21, 1819–1826. [Google Scholar] [CrossRef]
- Chen, L.C.; Zhu, Y.; Papandreou, G.; Schroff, F.; Adam, H. Encoderdecoder with atrous separable convolution for semantic image segmentation. arXiv 2018, arXiv:1802.02611. [Google Scholar]
- Sandler, M.; Howard, A.; Zhu, M.; Zhmoginov, A.; Chen, L. MobileNetV2: Inverted Residuals and Linear Bottlenecks. arXiv 2019, arXiv:1801.04381. [Google Scholar]
- Diederik, P.K.; Jimmy, L.B. Adam: A Method for Stochastic Optimization. arXiv 2017, arXiv:1412.6980. [Google Scholar]
- Chen, T.; Guestrin, C. XGBoost: A Scalable Tree Boosting System. arXiv 2017, arXiv:1603.02754. [Google Scholar]
- Garcia-Garcis, A.; Orts-Escolano, S.; Oprea, S.O.; Villena-Martinez, V.; Garcia-Rodriguez, J. A Review on Deep Learning Techniques Applied to Semantic Segmentation. arXiv 2017, arXiv:1704.06857. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tongue Features (n, %) | Control n = 600 | Gastric Cancer n = 103 | Number of Features | p-Value | |
|---|---|---|---|---|---|
| Tongue Shape | Fat tongue | 98 (83.05%) | 20 (16.95%) | 118 (16.79%) | <0.001 |
| Thin tongue | 71 (68.93%) | 32 (31.07%) | 103 (14.65%) | ||
| Normal tongue | 431 (89.42%) | 51 (10.58%) | 482 (68.56%) | ||
| Tongue Color | Pale white | 60 (78.95%) | 16 (21.05%) | 76 (10.81%) | 0.22 |
| Pale red | 447 (86.96%) | 67 (13.04%) | 514 (73.12%) | ||
| Red | 69 (82.14%) | 15 (17.86%) | 84 (11.95%) | ||
| Deep red | 24 (82.76%) | 5 (17.24%) | 29 (4.13%) | ||
| Tongue Coating Color | White | 385 (88.51%) | 50 (11.49%) | 435 (61.88%) | 0.0036 |
| Yellow | 215 (80.22%) | 53 (19.78%) | 268 (38.12%) | ||
| Saliva | Dry | 93 (56.71%) | 71 (43.29%) | 164 (23.33%) | <0.001 |
| Normal | 507 (94.06%) | 32 (5.94%) | 539 (76.67%) | ||
| Tongue Coating Thickness | Thick | 241 (75.55%) | 78 (24.45%) | 319 (45.38%) | <0.001 |
| Thin | 359 (93.49%) | 25 (6.51%) | 384 (54.62%) | ||
| Tongue Coating Texture | Greasy | 308 (78.57%) | 84 (21.43%) | 392 (55.76%) | <0.001 |
| Normal | 292 (93.89%) | 19 (6.11%) | 311 (44.24%) | ||
| Tongue Fissure | Fissured tongue | 208 (85.60%) | 35 (14.40%) | 243 (34.57%) | 0.98 |
| Normal | 392 (85.22%) | 68 (14.78%) | 460 (65.43%) | ||
| Tooth-marked Tongue | Tooth mark | 175 (63.64%) | 100 (36.36%) | 275 (39.12%) | <0.001 |
| Normal | 425 (99.30%) | 3 (0.70%) | 428 (60.88%) | ||
| Spots and Prickles Tongue | Spots and prickles | 145 (79.23%) | 38 (20.77%) | 183 (23.33%) | 0.0096 |
| Normal | 455 (87.50%) | 65 (12.50%) | 520 (73.97%) | ||
| Method | MPA | MIoU |
|---|---|---|
| PSPNet | 97.58% | 96.6% |
| U-Net | 98.58% | 97.14% |
| Deeplabv3+ | 98.93% | 97.96% |
| Result | Image 1 | Image 2 | Image 3 | Image 4 |
|---|---|---|---|---|
| control | 16.9% | 13.3% | 98.6% | 99.2% |
| gastric cancer | 83.1% | 86.7% | 0.14% | 0.08% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, X.; Ma, Y.; Guo, D.; Men, J.; Xue, C.; Cao, X.; Zhang, Z. A Framework to Predict Gastric Cancer Based on Tongue Features and Deep Learning. Micromachines 2023, 14, 53. https://doi.org/10.3390/mi14010053
Zhu X, Ma Y, Guo D, Men J, Xue C, Cao X, Zhang Z. A Framework to Predict Gastric Cancer Based on Tongue Features and Deep Learning. Micromachines. 2023; 14(1):53. https://doi.org/10.3390/mi14010053
Chicago/Turabian StyleZhu, Xiaolong, Yuhang Ma, Dong Guo, Jiuzhang Men, Chenyang Xue, Xiyuan Cao, and Zhidong Zhang. 2023. "A Framework to Predict Gastric Cancer Based on Tongue Features and Deep Learning" Micromachines 14, no. 1: 53. https://doi.org/10.3390/mi14010053