
Evaluating and Visualizing the Contribution of ECG Characteristic Waveforms for PPG-Based Blood Pressure Estimation
 ,
,
Abstract
:1. Introduction
- (1)
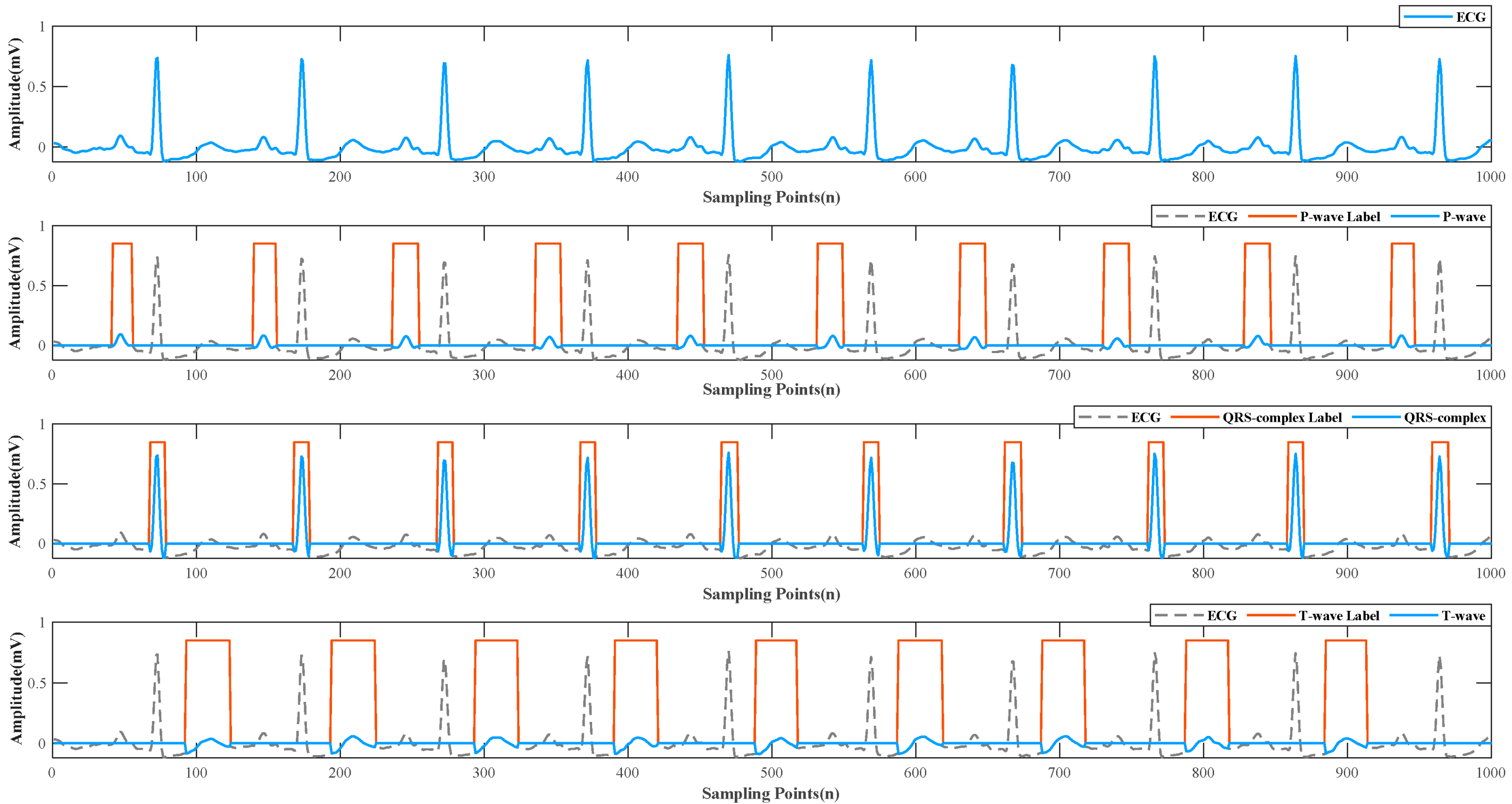
- This paper specifically compares the contribution of the three characteristic waveforms of ECG to the BP prediction model. Each ECG signal is masked as separate P, QRS, and T waves. Then these signals are put into different networks combined with PPG signal for training, rather than directly adding or deleting whole ECG signals [20].
- (2)
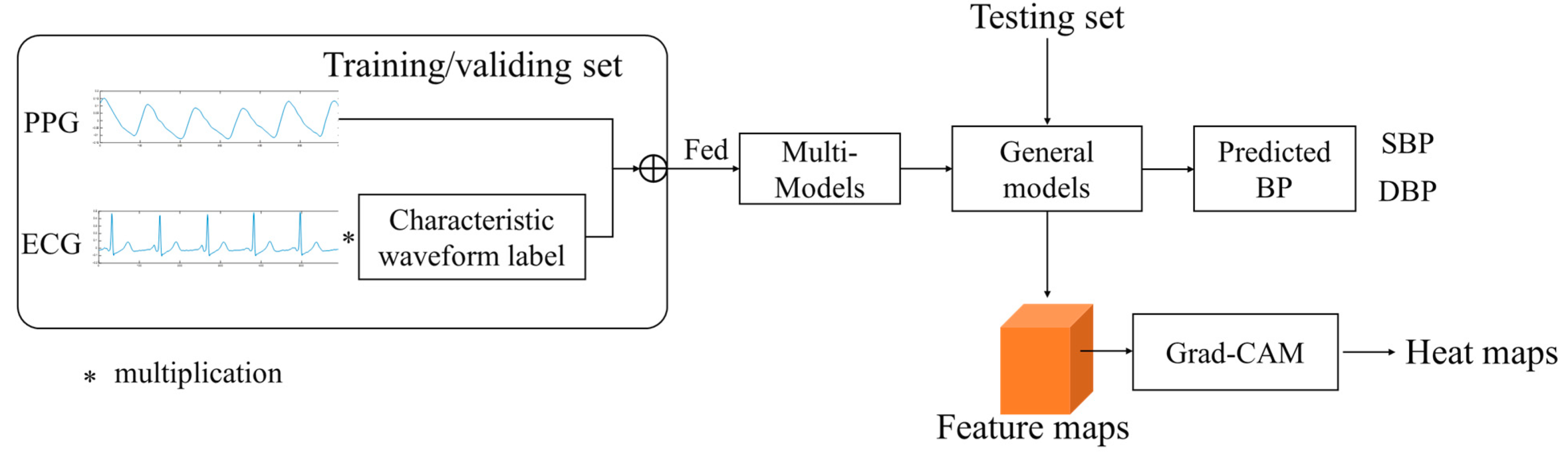
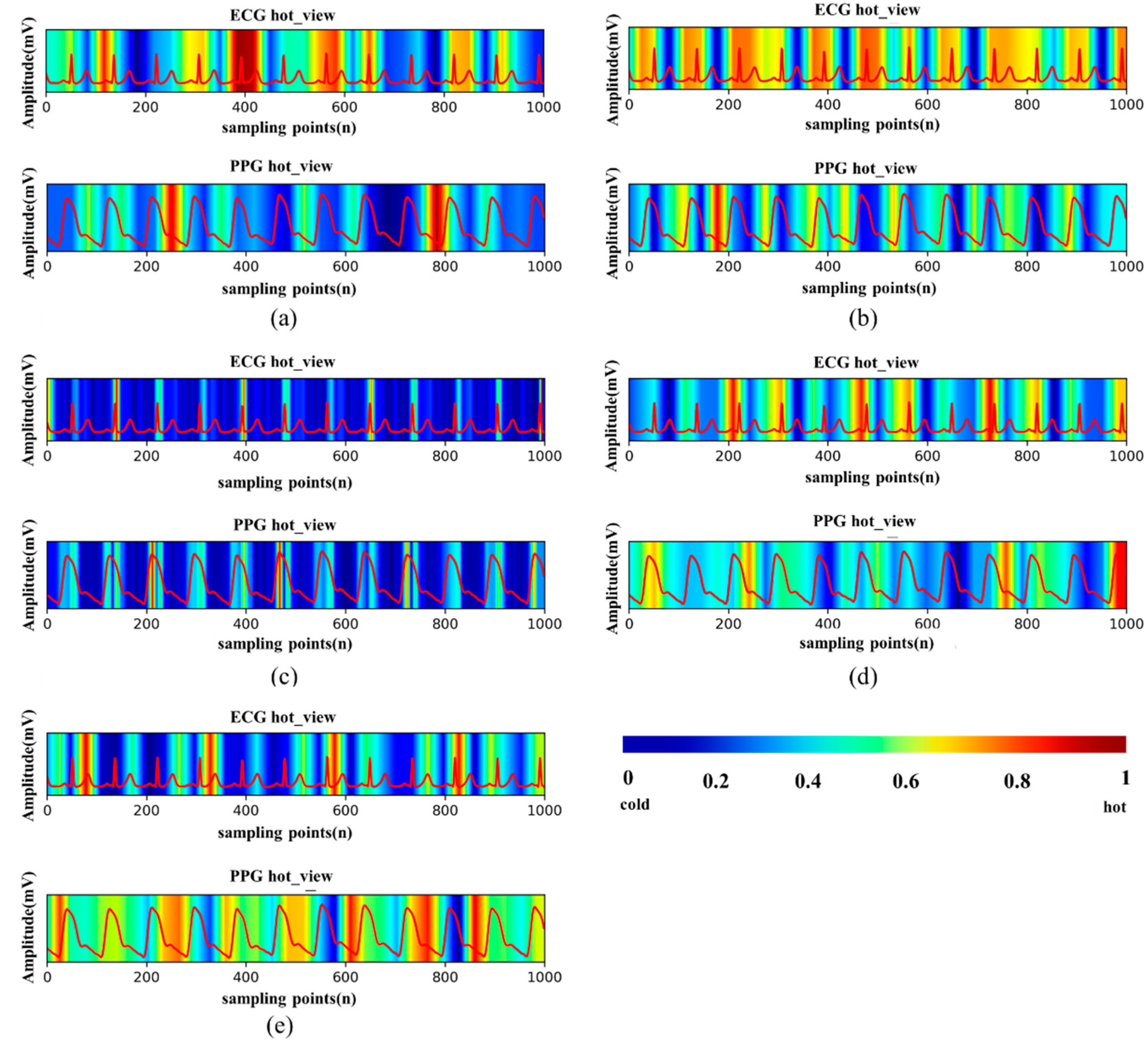
- This paper introduces Grad-CAM into a BP regression model so that we can more clearly understand which features of physiological signals will receive more attention or be ignored in the model, so as to provide a reference for artificial feature extraction or modification of the network model. Meanwhile, the visualization results further corroborate with (1), which strongly illustrate the different characteristics that ECG signals and PPG signals provide in the model.
2. Materials and Methods
2.1. Dataset
2.2. Preprocessing
2.2.1. Signal Selection and Filtering
2.2.2. ECG Detection
2.3. Multiple Regression Models
- (1)
- AlexNet [38]: was one of the classic CNN networks in the past decade, which has laid an important foundation for the network and proved the effectiveness of CNN in complex models.
- (2)
- GoogLeNet [39]: multiple convolutions or pooling operations were assembled into an inception module, and the network structure was constructed with this module. Then the network was concentrated in feature dimension, which reduced the number of parameters and further improved the network performance.
- (3)
- ResNet18 [40]: proposed in 2015. It established the “shortcut connection” between the front and the back layer, which is useful for the back-propagation of gradients in the training process and deepens the number of layers.
- (4)
- DenseNet121 [41]: established a dense connection between all previous layers and the back layer and realizes feature reuse by connecting features on the channel.
- (5)
- DPN68 [42]: combined the fundamental ideas of ResNet and DenseNet. ResNet was the main framework to ensure low redundancy of features and a DenseNet branch was added to generate new features.
2.4. Visualization with Grad-CAM
3. Results
3.1. Metrics
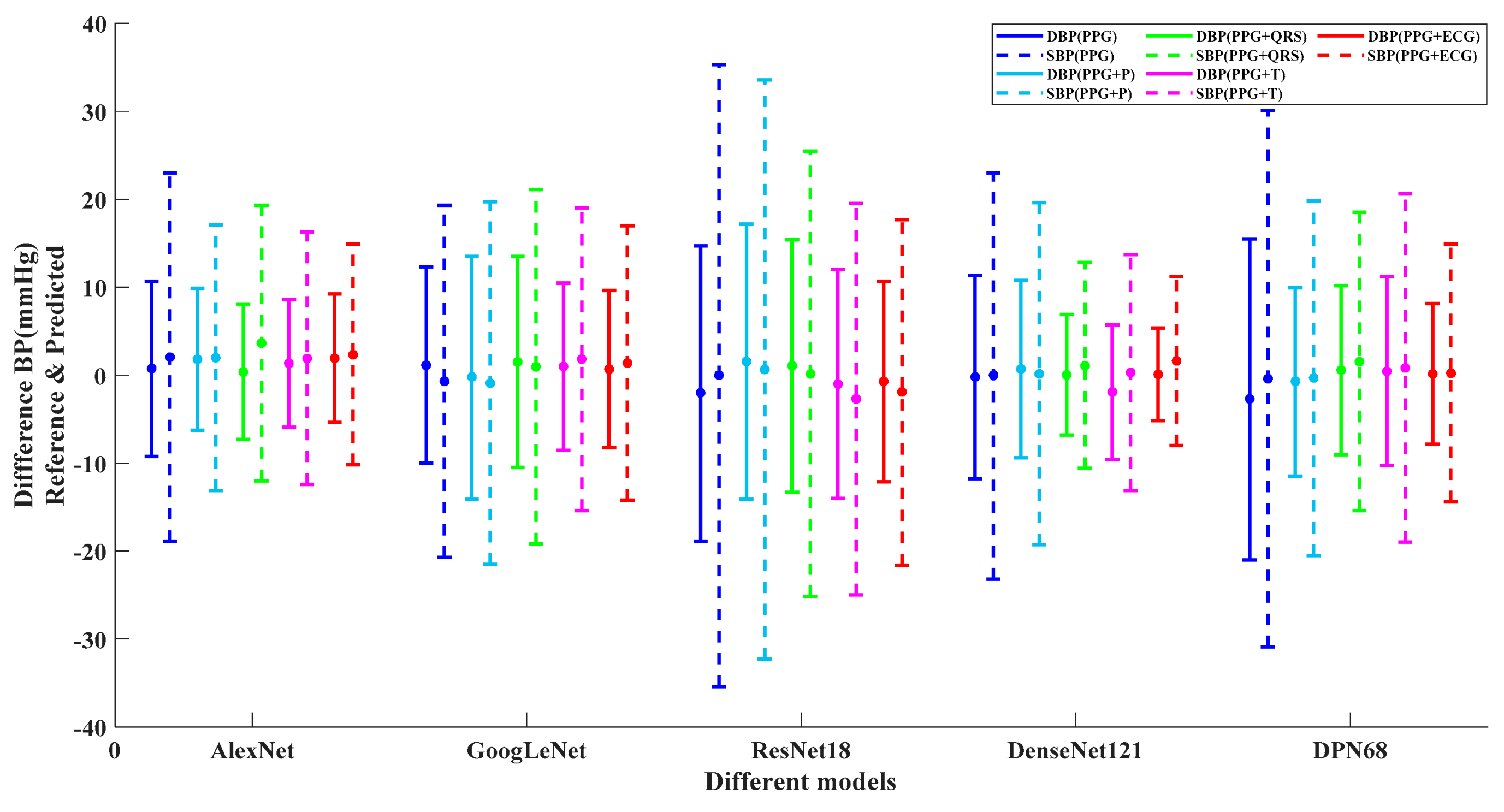
3.2. Analysis of Error Distribution
3.3. Performance of Visualization
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Kannel, W.B. Blood Pressure as a Cardiovascular Risk Factor. JAMA 1996, 275, 1571–1576. [Google Scholar] [CrossRef] [PubMed]
- Sharifi, I.; Goudarzi, S.; Khodabakhshi, M.B. A novel dynamical approach in continuous cuffless blood pressure estimation based on ECG and PPG signals. Artif. Intell. Med. 2019, 97, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Zhou, B.; Carrillo-Larco, R.M.; Danaei, G.; Riley, L.M.; Paciorek, C.J.; Stevens, G.A.; Gregg, E.W.; Bennett, J.E.; Solomon, B.; Singleton, R.K.; et al. Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: A pooled analysis of 1201 population-representative studies with 104 million participants. Lancet 2021, 398, 957–980. [Google Scholar] [CrossRef]
- Fischer, C.; Penzel, T. Continuous non-invasive determination of nocturnal blood pressure variation using photoplethysmographic pulse wave signals: Comparison of pulse propagation time, pulse transit time and RR-interval. Physiol. Meas. 2019, 40, 014001. [Google Scholar] [CrossRef] [PubMed]
- Bugarini, A.; Young, A.J.; Griessenauer, C.J.; Dalal, S.S.; Schirmer, C.M.; Vaughan, S.; Goren, O. Perioperative Continuous Noninvasive Arterial Pressure Monitoring for Neuroendovascular Interventions: Prospective Study for Evaluation of the Vascular Unloading Technique. World Neurosurg. 2021, 153, e195–e203. [Google Scholar] [CrossRef] [PubMed]
- Heydari, F.; Ebrahim, M.P.; Redoute, J.-M.; Joe, K.; Walker, K.; Yuce, M.R. A chest-based continuous cuffless blood pressure method: Estimation and evaluation using multiple body sensors. Inf. Fusion 2020, 54, 119–127. [Google Scholar] [CrossRef]
- Guo, Y.; Liu, X.; Peng, S.; Jiang, X.; Xu, K.; Chen, C.; Wang, Z.; Dai, C.; Chen, W. A review of wearable and unobtrusive sensing technologies for chronic disease management. Comput. Biol. Med. 2021, 129, 104163. [Google Scholar] [CrossRef]
- Geddes, L.A.; Voelz, M.H.; Babbs, C.F.; Bourland, J.D.; Tacker, W.A. Pulse Transit Time as an Indicator of Arterial Blood Pressure. Psychophysiology 1981, 18, 71–74. [Google Scholar] [CrossRef]
- Park, Y.-S.; Kim, S.-H.; Lee, Y.S.; Choi, S.-H.; Ku, S.-W.; Hwang, G.-S. Real-Time Monitoring of Blood Pressure Using Digitalized Pulse Arrival Time Calculation Technology for Prompt Detection of Sudden Hypertensive Episodes During Laryngeal Microsurgery: Retrospective Observational Study. J. Med. Internet Res. 2020, 22, e13156. [Google Scholar] [CrossRef]
- Najjar, S.S.; Scuteri, A.; Shetty, V.; Wright, J.G.; Muller, D.C.; Fleg, J.L.; Spurgeon, H.P.; Ferrucci, L.; Lakatta, E.G. Pulse wave velocity is an independent predictor of the longitudinal increase in systolic blood pressure and of incident hypertension in the Baltimore Longitudinal Study of Aging. J. Am. Coll. Cardiol. 2008, 51, 1377–1383. [Google Scholar] [CrossRef] [Green Version]
- Sharma, M.; Barbosa, K.; Ho, V.; Griggs, D.; Ghirmai, T.; Krishnan, S.K.; Hsiai, T.K.; Chiao, J.-C.; Cao, H. Cuff-Less and Continuous Blood Pressure Monitoring: A Methodological Review. Technologies 2017, 5, 21. [Google Scholar] [CrossRef]
- Awad, A.A.; Haddadin, A.S.; Tantawy, H.; Badr, T.M.; Stout, R.G.; Silverman, D.G.; Shelley, K.H. The relationship between the photoplethysmographic waveform and systemic vascular resistance. J. Clin. Monit. Comput. 2007, 21, 365–372. [Google Scholar] [CrossRef]
- Ding, X.-R.; Zhang, Y.-T.; Liu, J.; Dai, W.-X.; Tsang, H.K. Continuous Cuffless Blood Pressure Estimation Using Pulse Transit Time and Photoplethysmogram Intensity Ratio. IEEE Trans. Biomed. Eng. 2016, 63, 964–972. [Google Scholar] [CrossRef]
- Tan, X.; Ji, Z.; Zhang, Y. Non-invasive continuous blood pressure measurement based on mean impact value method, BP neural network, and genetic algorithm. Technol. Health Care 2018, 26, 87–101. [Google Scholar] [CrossRef]
- Kurylyak, Y.; Lamonaca, F.; Grimaldi, D. A Neural Network-based method for continuous blood pressure estimation from a PPG signal. In Proceedings of the 2013 IEEE International Instrumentation and Measurement Technology Conference (I2MTC), Minneapolis, MN, USA, 6–9 May 2013; pp. 280–283. [Google Scholar]
- Liu, M.; Po, L.-M.; Fu, H. Cuffless Blood Pressure Estimation Based on Photoplethysmography Signal and Its Second Derivative. Int. J. Comput. Theory Eng. 2017, 9, 202–206. [Google Scholar] [CrossRef]
- Yin, S.; Li, G.; Luo, Y.; Lin, L. Cuff-less continuous blood pressure measurement based on multiple types of information fusion. Biomed. Signal Process. Control 2021, 68, 102549. [Google Scholar] [CrossRef]
- Lin, W.-H.; Wang, H.; Samuel, O.W.; Liu, G.; Huang, Z.; Li, G. New photoplethysmogram indicators for improving cuffless and continuous blood pressure estimation accuracy. Physiol. Meas. 2018, 39, 025005. [Google Scholar] [CrossRef]
- Chowdhury, M.H.; Shuzan, N.I.; Chowdhury, M.E.; Mahbub, Z.B.; Uddin, M.M.; Khandakar, A.; Reaz, M.B.I. Estimating Blood Pressure from the Photoplethysmogram Signal and Demographic Features Using Machine Learning Techniques. Sensors 2020, 20, 3127. [Google Scholar] [CrossRef]
- Esmaelpoor, J.; Moradi, M.H.; Kadkhodamohammadi, A. Cuffless blood pressure estimation methods: Physiological model parameters versus machine-learned features. Physiol. Meas. 2021, 42, 035006. [Google Scholar] [CrossRef]
- Thambiraj, G.; Gandhi, U.; Mangalanathan, U.; Jose, V.J.M.; Anand, M. Investigation on the effect of Womersley number, ECG and PPG features for cuff less blood pressure estimation using machine learning. Biomed. Signal Process. Control 2020, 60, 101942. [Google Scholar] [CrossRef]
- Panwar, M.; Gautam, A.; Biswas, D.; Acharyya, A. PP-Net: A Deep Learning Framework for PPG-Based Blood Pressure and Heart Rate Estimation. IEEE Sens. J. 2020, 20, 10000–10011. [Google Scholar] [CrossRef]
- Su, P.; Ding, X.R.; Zhang, Y.T.; Liu, J.; Miao, F.; Zhao, N. Long-term blood pressure prediction with deep recurrent neural networks. In Proceedings of the 2018 IEEE EMBS International Conference on Biomedical & Health Informatics (BHI), Las Vegas, NV, USA, 4–7 March 2018; pp. 323–328. [Google Scholar]
- Tanveer, M.S.; Hasan, M.K. Cuffless blood pressure estimation from electrocardiogram and photoplethysmogram using waveform based ANN-LSTM network. Biomed. Signal Process. Control 2019, 51, 382–392. [Google Scholar] [CrossRef]
- Yu, M.; Huang, Z.; Zhu, Y.; Zhou, P.; Zhu, J. Attention-based residual improved U-Net model for continuous blood pressure monitoring by using photoplethysmography signal. Biomed. Signal Process. Control 2022, 75, 103581. [Google Scholar] [CrossRef]
- Rong, M.; Li, K. A multi-type features fusion neural network for blood pressure prediction based on photoplethysmography. Biomed. Signal Process. Control 2021, 68, 102772. [Google Scholar] [CrossRef]
- Selvaraju, R.R.; Cogswell, M.; Das, A.; Vedantam, R.; Parikh, D.; Batra, D. Grad-CAM: Visual Explanations from Deep Networks via Gradient-Based Localization. In Proceedings of the 2017 IEEE International Conference on Computer Vision (ICCV), Venice, Italy, 22–29 October 2017. [Google Scholar]
- Zhou, B.; Khosla, A.; Lapedriza, A.; Oliva, A.; Torralba, A. Learning deep features for discriminative localization. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 2921–2929. [Google Scholar]
- Li, Y.; Yang, H.; Li, J.; Chen, D.; Du, M. EEG-based intention recognition with deep recurrent-convolution neural network: Performance and channel selection by Grad-CAM. Neurocomputing 2020, 415, 225–233. [Google Scholar] [CrossRef]
- Kim, J.-K.; Jung, S.; Park, J.; Han, S.W. Arrhythmia detection model using modified DenseNet for comprehensible Grad-CAM visualization. Biomed. Signal Process. Control 2022, 73, 103408. [Google Scholar] [CrossRef]
- Johnson, A.; Pollard, T.; Mark, R. MIMIC-III Clinical Database (version 1.4). PhysioNet 2016. [Google Scholar] [CrossRef]
- Johnson, A.E.W.; Pollard, T.J.; Shen, L.; Lehman, L.-W.H.; Feng, M.; Ghassemi, M.; Moody, B.; Szolovits, P.; Celi, L.A.; Mark, R.G. MIMIC-III, a freely accessible critical care database. Sci. Data 2016, 3, 160035. [Google Scholar] [CrossRef]
- Slapničar, G.; Mlakar, N.; Luštrek, M. Blood Pressure Estimation from Photoplethysmogram Using a Spectro-Temporal Deep Neural Network. Sensors 2019, 19, 3420. [Google Scholar] [CrossRef]
- Harfiya, L.; Chang, C.-C.; Li, Y.-H. Continuous Blood Pressure Estimation Using Exclusively Photopletysmography by LSTM-Based Signal-to-Signal Translation. Sensors 2021, 21, 2952. [Google Scholar] [CrossRef]
- Lin, W.-H.; Chen, F.; Geng, Y.; Ji, N.; Fang, P.; Li, G. Towards accurate estimation of cuffless and continuous blood pressure using multi-order derivative and multivariate photoplethysmogram features. Biomed. Signal Process. Control 2021, 63, 102198. [Google Scholar] [CrossRef]
- Jimenez-Perez, G.; Alcaine, A.; Camara, O. Delineation of the electrocardiogram with a mixed-quality-annotations dataset using convolutional neural networks. Sci. Rep. 2021, 11, 863. [Google Scholar] [CrossRef]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation. In Medical Image Computing and Computer-Assisted Intervention 2015; Navab, N., Hornegger, J., Wells, W.M., Frangi, A.F., Eds.; Springer International Publishing: Cham, Switzerland, 2015; pp. 234–241. [Google Scholar]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. Imagenet classification with deep convolutional neural networks. NIPS 2012, 25, 84–90. [Google Scholar] [CrossRef]
- Szegedy, C.; Liu, W.; Jia, Y.; Sermanet, P.; Reed, S.; Anguelov, D.; Erhan, D.; Vanhoucke, V.; Rabinovich, A. Going deeper with convolutions. In Proceedings of the 2015 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Boston, MA, USA, 7–12 June 2015; pp. 1–9. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition, Seattle, WA, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]
- Chen, Y.; Li, J.; Xiao, H.; Jin, X.; Yan, S.; Feng, J. Dual path networks. Adv. Neural Inf. Process. Syst. 2017, 30, 9. [Google Scholar]
- Qin, K.; Huang, W.; Zhang, T. Deep generative model with domain adversarial training for predicting arterial blood pressure waveform from photoplethysmogram signal. Biomed. Signal Process. Control 2021, 70, 102972. [Google Scholar] [CrossRef]
- Attia, Z.I.; Kapa, S.; Lopez-Jimenez, F.; McKie, P.M.; Ladewig, D.J.; Satam, G.; Pellikka, P.A.; Enriquez-Sarano, M.; Noseworthy, P.A.; Munger, T.M.; et al. Screening for cardiac contractile dysfunction using an artificial intelligence-enabled electrocardiogram. Nat. Med. 2019, 25, 70–74. [Google Scholar] [CrossRef]
- Cheffer, A.; Savi, M.A.; Pereira, T.L.; de Paula, A.S. Heart rhythm analysis using a nonlinear dynamics perspective. Appl. Math. Model. 2021, 96, 152–176. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Models | AlexNet | GoogLeNet | ResNet18 | |||||||||
| SBP/mmHg | DBP/mmHg | SBP/mmHg | DBP/mmHg | SBP/mmHg | DBP/mmHg | |||||||
| MAE | RMSE | MAE | RMSE | MAE | RMSE | MAE | RMSE | MAE | RMSE | MAE | RMSE | |
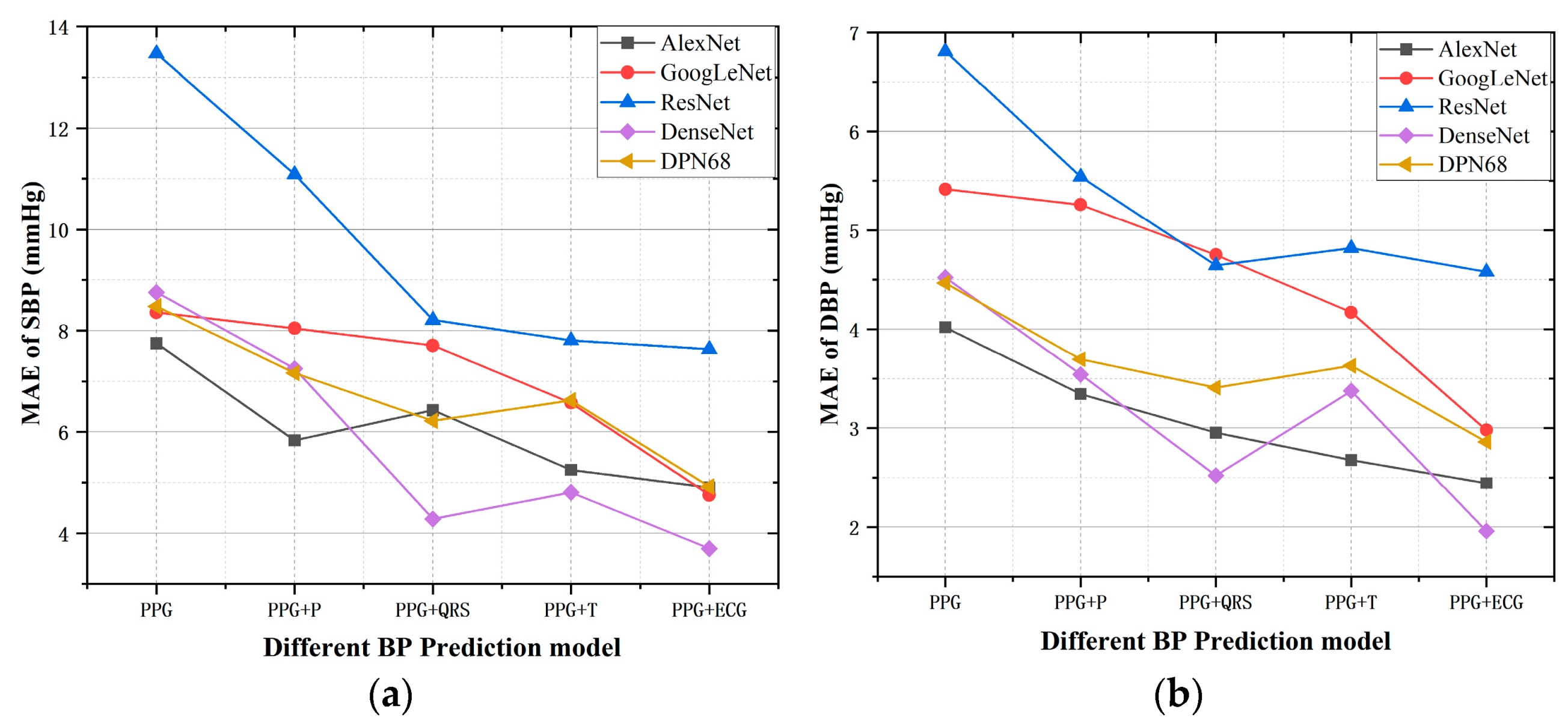
| PPG | 7.74 | 10.53 | 4.02 | 5.19 | 8.35 | 11.15 | 5.25 | 6.71 | 13.46 | 17.53 | 6.81 | 8.47 |
| PPG + P wave | 5.83 | 7.98 | 3.34 | 4.50 | 8.04 | 10.57 | 5.41 | 7.06 | 11.08 | 14.35 | 5.54 | 7.16 |
| PPG + QRS wave | 6.42 | 8.80 | 2.95 | 3.95 | 7.70 | 10.33 | 4.75 | 6.34 | 8.21 | 10.74 | 4.64 | 5.91 |
| PPG + T wave | 5.25 | 6.96 | 2.67 | 3.47 | 6.57 | 8.68 | 4.17 | 5.38 | 7.80 | 10.39 | 4.81 | 5.87 |
| PPG + ECG | 4.93 | 6.2 | 2.44 | 4.19 | 4.75 | 6.44 | 2.97 | 3.97 | 7.63 | 10.26 | 4.58 | 6.21 |
| Models | DenseNet121 | DPN68 | ||||||||||
| SBP/mmHg | DBP/mmHg | SBP/mmHg | DBP/mmHg | |||||||||
| MAE | RMSE | MAE | RMSE | MAE | RMSE | MAE | RMSE | |||||
| PPG | 8.75 | 11.81 | 4.52 | 5.91 | 8.48 | 11.41 | 4.46 | 5.98 | ||||
| PPG + P wave | 7.25 | 9.80 | 3.54 | 4.71 | 7.16 | 9.64 | 3.69 | 4.95 | ||||
| PPG + QRS wave | 7.70 | 10.33 | 4.75 | 6.34 | 6.22 | 8.50 | 3.40 | 4.55 | ||||
| PPG + T wave | 4.80 | 6.87 | 3.37 | 4.35 | 6.62 | 9.14 | 3.62 | 4.90 | ||||
| PPG + ECG | 3.69 | 5.18 | 1.95 | 2.71 | 4.92 | 6.86 | 2.86 | 3.97 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, G.; Chen, Y.; Zhu, W.; Zheng, L.; Tang, H.; Yu, Y.; Wang, L. Evaluating and Visualizing the Contribution of ECG Characteristic Waveforms for PPG-Based Blood Pressure Estimation. Micromachines 2022, 13, 1438. https://doi.org/10.3390/mi13091438
Ma G, Chen Y, Zhu W, Zheng L, Tang H, Yu Y, Wang L. Evaluating and Visualizing the Contribution of ECG Characteristic Waveforms for PPG-Based Blood Pressure Estimation. Micromachines. 2022; 13(9):1438. https://doi.org/10.3390/mi13091438
Chicago/Turabian StyleMa, Gang, Yuhang Chen, Wenliang Zhu, Lesong Zheng, Hui Tang, Yong Yu, and Lirong Wang. 2022. "Evaluating and Visualizing the Contribution of ECG Characteristic Waveforms for PPG-Based Blood Pressure Estimation" Micromachines 13, no. 9: 1438. https://doi.org/10.3390/mi13091438