
Quantitative Spectrochip-Coupled Lateral Flow Immunoassay Demonstrates Clinical Potential for Overcoming Coronavirus Disease 2019 Pandemic Screening Challenges

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
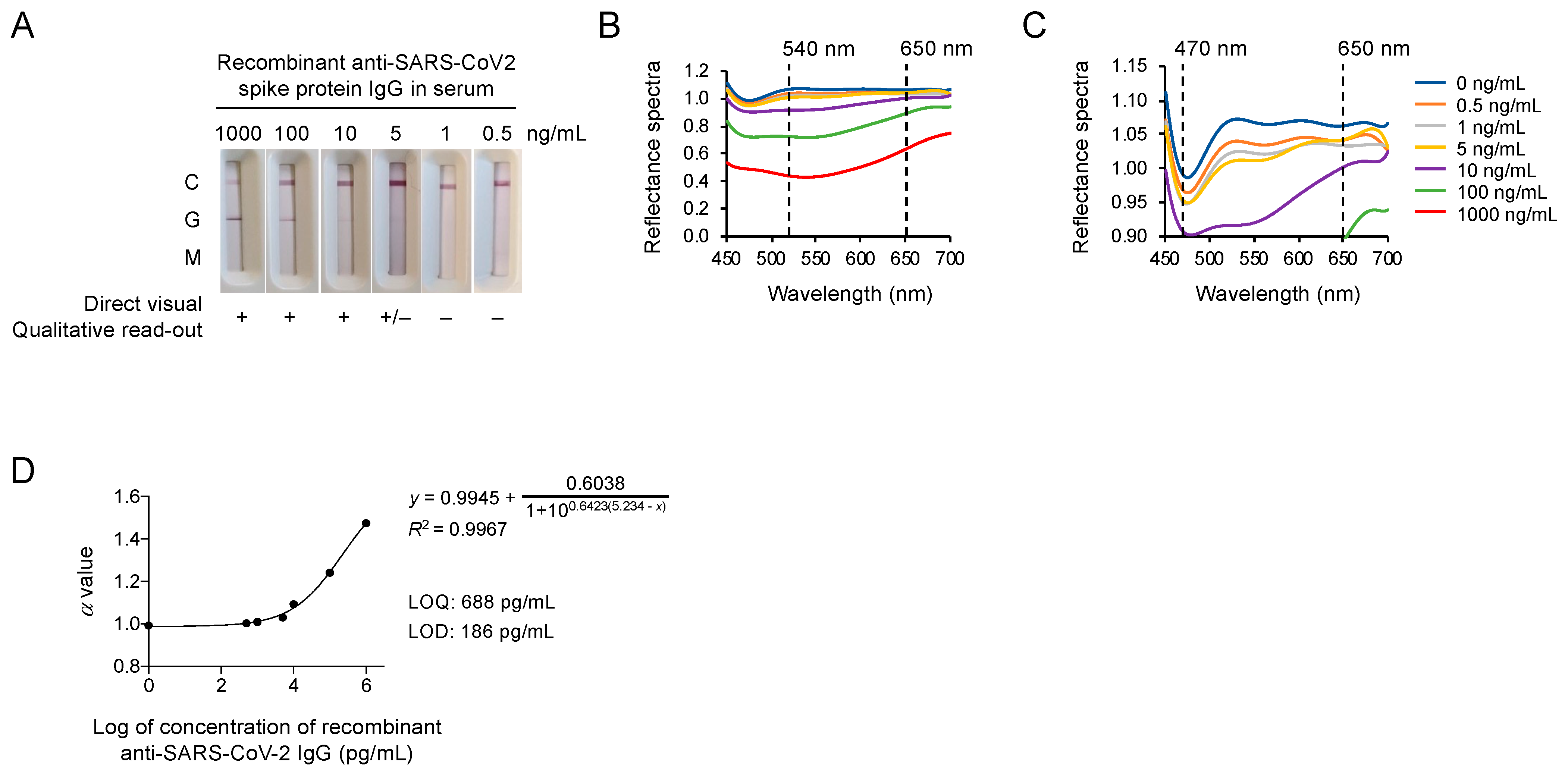
2.1. The Spectrum Analyzer System Provides High-Performance Spectral Analysis for the COVID-19 IgM/IgG Test Strip
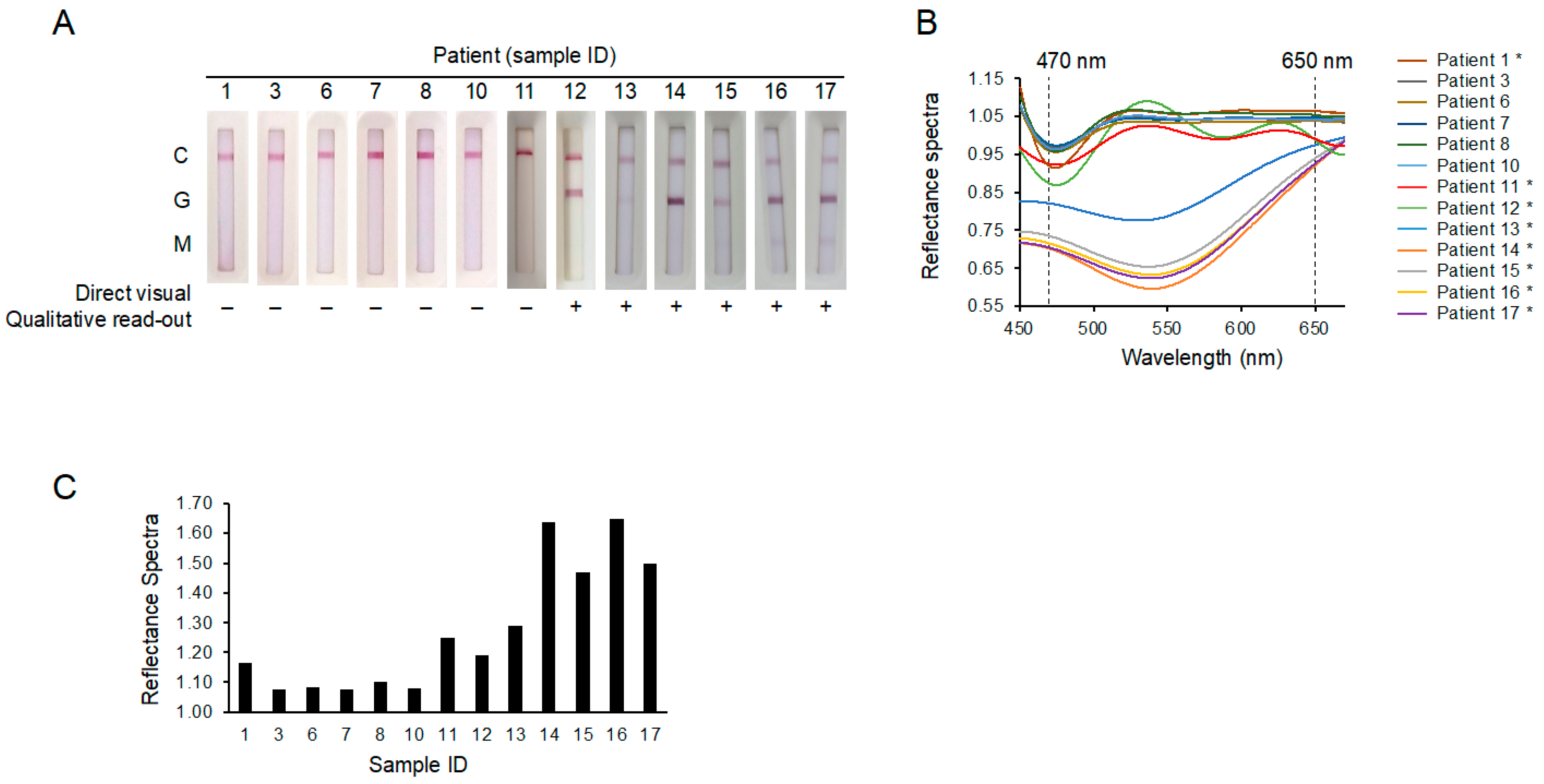
2.2. The New Spectrum Analyzer System May Enable the Identification of Patients That Would Otherwise Produce False Negative Test Results
3. Discussion
4. Methods
4.1. Patients and Samples
4.2. Statement
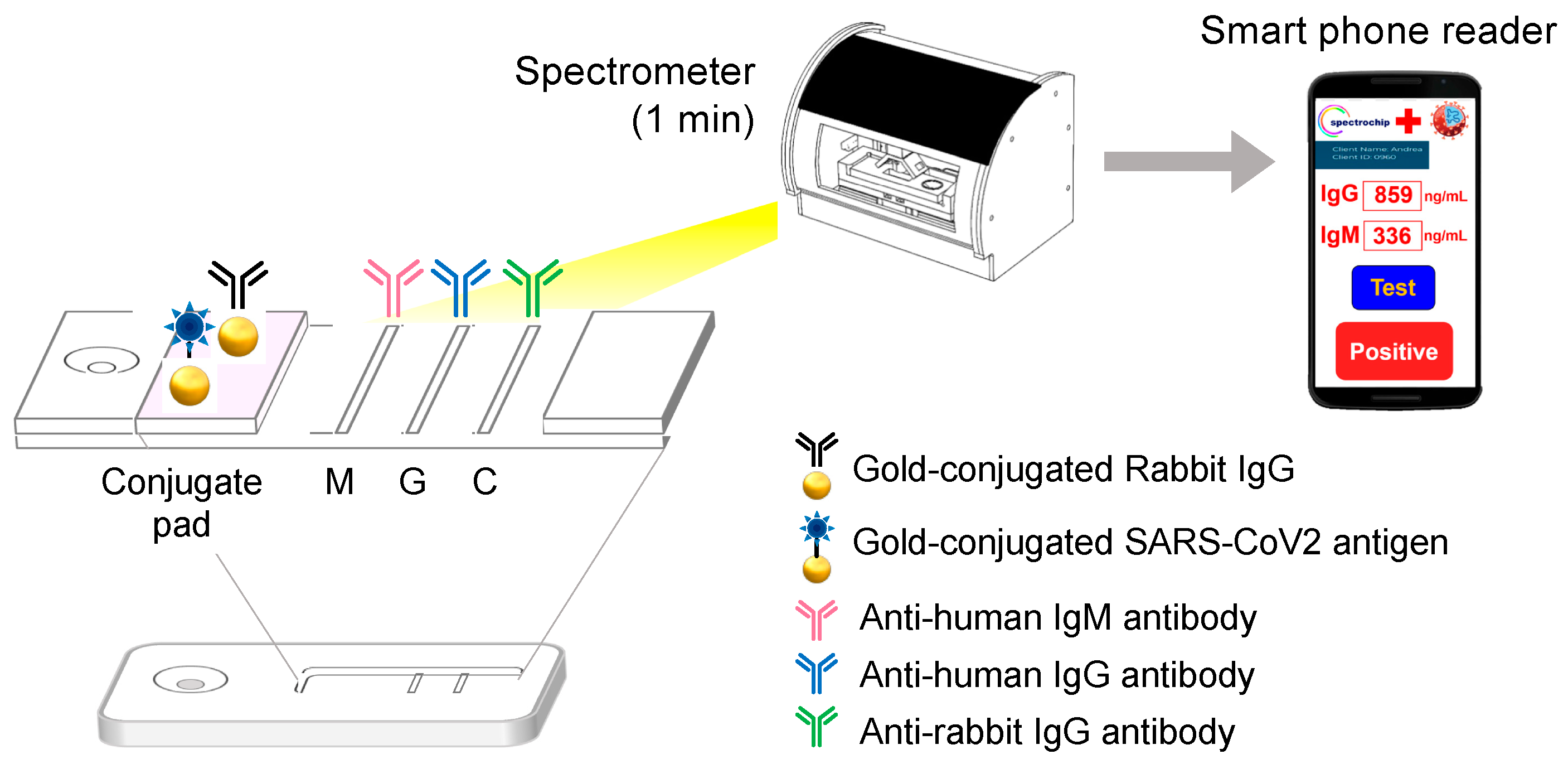
4.3. Lateral Flow Immunoassays
4.4. Reflectance Spectral Analysis
4.5. Limit of Detection and Limit of Quantification
LOQ = Blank (mean) + 10 × Blank (standard deviation) → Fit to the Figure D equation
Author Contributions
Funding
Conflicts of Interest
References
- Cui, J.; Li, F.; Shi, Z.L. Origin and evolution of pathogenic coronaviruses. Nat. Rev. Microbiol. 2019, 17, 181–192. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 7 February 2021).
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Perez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Moderna Press release: Moderna’s COVID-19 Vaccine Candidate Meets its Primary Efficacy Endpoint in the First Interim Analysis of the Phase 3 COVE Study. 2020. Available online: https://investors.modernatx.com/news-releases/news-release-details/modernas-covid-19-vaccine-candidate-meets-its-primary-efficacy/ (accessed on 17 March 2021).
- BioNTech Press release: Pfizer and BioNTech Announce Vaccine Candidate Against COVID-19 Achieved Success in First Interim Analysis from Phase 3 Study. 2020. Available online: https://www.pfizer.com/news/press-release/press-release-detail/pfizer-and-biontech-announce-vaccine-candidate-against (accessed on 9 November 2020).
- Sethuraman, N.; Jeremiah, S.S.; Ryo, A. Interpreting Diagnostic Tests for SARS-CoV-2. JAMA 2020. [Google Scholar] [CrossRef] [PubMed]
- Spellberg, B.; Haddix, M.; Lee, R.; Butler-Wu, S.; Holtom, P.; Yee, H.; Gounder, P. Community Prevalence of SARS-CoV-2 Among Patients with Influenzalike Illnesses Presenting to a Los Angeles Medical Center in March 2020. JAMA 2020. [Google Scholar] [CrossRef] [PubMed]
- To, K.K.; Tsang, O.T.; Leung, W.S.; Tam, A.R.; Wu, T.C.; Lung, D.C.; Yip, C.C.; Cai, J.P.; Chan, J.M.; Chik, T.S.; et al. Temporal profiles of viral load in posterior oropharyngeal saliva samples and serum antibody responses during infection by SARS-CoV-2: An observational cohort study. Lancet Infect. Dis. 2020, 20, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Carter, L.J.; Garner, L.V.; Smoot, J.W.; Li, Y.; Zhou, Q.; Saveson, C.J.; Sasso, J.M.; Gregg, A.C.; Soares, D.J.; Beskid, T.R.; et al. Assay Techniques and Test Development for COVID-19 Diagnosis. ACS Cent. Sci. 2020, 6, 591–605. [Google Scholar] [CrossRef]
- Younes, N.; Al-Sadeq, D.W.; Al-Jighefee, H.; Younes, S.; Al-Jamal, O.; Daas, H.I.; Yassine, H.M.; Nasrallah, G.K. Challenges in Laboratory Diagnosis of the Novel Coronavirus SARS-CoV-2. Viruses 2020, 12, 582. [Google Scholar] [CrossRef]
- Chan, J.F.; Yip, C.C.; To, K.K.; Tang, T.H.; Wong, S.C.; Leung, K.H.; Fung, A.Y.; Ng, A.C.; Zou, Z.; Tsoi, H.W.; et al. Improved Molecular Diagnosis of COVID-19 by the Novel, Highly Sensitive and Specific COVID-19-RdRp/Hel Real-Time Reverse Transcription-PCR Assay Validated In Vitro and with Clinical Specimens. J. Clin. Microbiol. 2020, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.; Ai, J.; Loeffelholz, M.J.; Tang, Y.W.; Zhang, W. Meta-analysis of Diagnostic Performance of Serology Tests for COVID-19: Impact of Assay Design and Post-symptom-onset Intervals. Emerg. Microbes Infect. 2020, 9, 2200–2211. [Google Scholar] [CrossRef]
- Hung, I.F.; Cheng, V.C.; Li, X.; Tam, A.R.; Hung, D.L.; Chiu, K.H.; Yip, C.C.; Cai, J.P.; Ho, D.T.; Wong, S.C.; et al. SARS-CoV-2 shedding and seroconversion among passengers quarantined after disembarking a cruise ship: A case series. Lancet Infect. Dis. 2020, 20, 1051–1060. [Google Scholar] [CrossRef]
- Lou, B.; Li, T.D.; Zheng, S.F.; Su, Y.Y.; Li, Z.Y.; Liu, W.; Yu, F.; Ge, S.X.; Zou, Q.D.; Yuan, Q.; et al. Serology characteristics of SARS-CoV-2 infection after exposure and post-symptom onset. Eur. Respir. J. 2020, 56. [Google Scholar] [CrossRef]
- Wu, L.P.; Wang, N.C.; Chang, Y.H.; Tian, X.Y.; Na, D.Y.; Zhang, L.Y.; Zheng, L.; Lan, T.; Wang, L.F.; Liang, G.D. Duration of antibody responses after severe acute respiratory syndrome. Emerg. Infect. Dis. 2007, 13, 1562–1564. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.Y.; Lin, R.T.P.; Renia, L.; Ng, L.F.P. Serological Approaches for COVID-19: Epidemiologic Perspective on Surveillance and Control. Front. Immunol. 2020, 11, 879. [Google Scholar] [CrossRef]
- Long, Q.X.; Liu, B.Z.; Deng, H.J.; Wu, G.C.; Deng, K.; Chen, Y.K.; Liao, P.; Qiu, J.F.; Lin, Y.; Cai, X.F.; et al. Antibody responses to SARS-CoV-2 in patients with COVID-19. Nat. Med. 2020, 26, 845–848. [Google Scholar] [CrossRef] [PubMed]
- Xiang, F.; Wang, X.; He, X.; Peng, Z.; Yang, B.; Zhang, J.; Zhou, Q.; Ye, H.; Ma, Y.; Li, H.; et al. Antibody Detection and Dynamic Characteristics in Patients with COVID-19. Clin. Infect. Dis. 2020, 71, 1930–1934. [Google Scholar] [CrossRef] [PubMed]
- Zhao, R.; Li, M.; Song, H.; Chen, J.; Ren, W.; Feng, Y.; Gao, G.F.; Song, J.; Peng, Y.; Su, B.; et al. Early detection of SARS-CoV-2 antibodies in COVID-19 patients as a serologic marker of infection. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Van der Heide, V. Neutralizing antibody response in mild COVID-19. Nat. Rev. Immunol. 2020, 20, 352. [Google Scholar] [CrossRef]
- Udugama, B.; Kadhiresan, P.; Kozlowski, H.N.; Malekjahani, A.; Osborne, M.; Li, V.Y.C.; Chen, H.; Mubareka, S.; Gubbay, J.B.; Chan, W.C.W. Diagnosing COVID-19: The Disease and Tools for Detection. ACS Nano 2020, 14, 3822–3835. [Google Scholar] [CrossRef] [Green Version]
- Montesinos, I.; Gruson, D.; Kabamba, B.; Dahma, H.; Van den Wijngaert, S.; Reza, S.; Carbone, V.; Vandenberg, O.; Gulbis, B.; Wolff, F.; et al. Evaluation of two automated and three rapid lateral flow immunoassays for the detection of anti-SARS-CoV-2 antibodies. J. Clin. Virol. 2020, 128, 104413. [Google Scholar] [CrossRef]
- Arons, M.M.; Hatfield, K.M.; Reddy, S.C.; Kimball, A.; James, A.; Jacobs, J.R.; Taylor, J.; Spicer, K.; Bardossy, A.C.; Oakley, L.P.; et al. Presymptomatic SARS-CoV-2 Infections and Transmission in a Skilled Nursing Facility. N. Engl. J. Med. 2020, 382, 2081–2090. [Google Scholar] [CrossRef]
- Hoehl, S.; Rabenau, H.; Berger, A.; Kortenbusch, M.; Cinatl, J.; Bojkova, D.; Behrens, P.; Boddinghaus, B.; Gotsch, U.; Naujoks, F.; et al. Evidence of SARS-CoV-2 Infection in Returning Travelers from Wuhan, China. N. Engl. J. Med. 2020, 382, 1278–1280. [Google Scholar] [CrossRef] [PubMed]
- Nalla, A.K.; Casto, A.M.; Huang, M.W.; Perchetti, G.A.; Sampoleo, R.; Shrestha, L.; Wei, Y.; Zhu, H.; Jerome, K.R.; Greninger, A.L. Comparative Performance of SARS-CoV-2 Detection Assays Using Seven Different Primer-Probe Sets and One Assay Kit. J. Clin. Microbiol. 2020, 58. [Google Scholar] [CrossRef] [Green Version]
- Meschi, S.; Colavita, F.; Bordi, L.; Matusali, G.; Lapa, D.; Amendola, A.; Vairo, F.; Ippolito, G.; Capobianchi, M.R.; Castilletti, C.; et al. Performance evaluation of Abbott ARCHITECT SARS-CoV-2 IgG immunoassay in comparison with indirect immunofluorescence and virus microneutralization test. J. Clin. Virol. 2020, 129, 104539. [Google Scholar] [CrossRef]
- Tre-Hardy, M.; Wilmet, A.; Beukinga, I.; Favresse, J.; Dogne, J.M.; Douxfils, J.; Blairon, L. Analytical and clinical validation of an ELISA for specific SARS-CoV-2 IgG, IgA, and IgM antibodies. J. Med. Virol. 2020, 93, 803–811. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Bundschuh, C.; Wiesinger, K.; Gabriel, C.; Clodi, M.; Mueller, T.; Dieplinger, B. Comparison of the Elecsys(R) Anti-SARS-CoV-2 immunoassay with the EDI enzyme linked immunosorbent assays for the detection of SARS-CoV-2 antibodies in human plasma. Clin. Chim. Acta 2020, 509, 18–21. [Google Scholar] [CrossRef]
- Bryan, A.; Pepper, G.; Wener, M.H.; Fink, S.L.; Morishima, C.; Chaudhary, A.; Jerome, K.R.; Mathias, P.C.; Greninger, A.L. Performance Characteristics of the Abbott Architect SARS-CoV-2 IgG Assay and Seroprevalence in Boise, Idaho. J. Clin. Microbiol. 2020, 58. [Google Scholar] [CrossRef] [PubMed]
- Abbott, “SARS-CoV-2 IgG assay”, US FAD-EUA, 2020, 04, 26. Available online: https://www.fda.gov/media/137384/download (accessed on 26 April 2020).
- BIO-RAD, “Platelia SARS-CoV-2 Total Ab assay”, US FAD-EUA, 2020, 04, 29. Available online: https://www.fda.gov/media/137494/download (accessed on 29 April 2020).
- Roche Diagnostics, “Elecsys Anti-SARS-CoV-2”, US FAD-EUA, 2020, 05, 02. Available online: https://www.fda.gov/media/137602/download (accessed on 2 May 2020).




{kind=link}
{kind=link}
{kind=link}
| Sample ID | Days from Onset to PCR | Spectrochip Direct Visual Read-Out | Spectrochip Quantitative Estimate (pg/mL) | Spectrochip Results | PCR Results |
|---|---|---|---|---|---|
| 1 | 3 | Negative | 191 | Weakly positive | Positive |
| 3 | 0 | Negative | 162 | Negative | Negative |
| 6 | 1 | Negative | 165 | Negative | Negative |
| 7 | 12 | Negative | 162 | Negative | Negative |
| 8 | 5 | Negative | 170 | Negative | Negative |
| 10 | 15 | Negative | 164 | Negative | Negative |
| 11 | 18 | Negative | 379 | Positive | Positive |
| 12 | 10 | Positive | 499 | Positive | Positive |
| 13 | 24 | Positive | 578 | Positive | Positive |
| 14 | 13 | Positive | 1263 | Positive | Positive |
| 15 | 10 | Positive | 952 | Positive | Positive |
| 16 | 33 | Positive | 1282 | Positive | Positive |
| 17 | 43 | Positive | 2481 | Positive | Positive |
| Sample ID | Age | Gender | Date of Symptom Onset | Symptoms | Date of PCR Test | PCR Result | Date of Blood Draw | Date of Spectrochip Test |
|---|---|---|---|---|---|---|---|---|
| 1 | 31 | M | 14/3/2020 | Stuffy running nose, cough, sore throat | 17/3/2020 | Confirmed | 17/3/2020 | 8/4/2020 |
| 3 | 35 | M | 10/3/2020 | Sore throat | 10/3/2020 | Negative | 10/3/2020 | 8/4/2020 |
| 6 | 23 | F | 11/3/2020 | Fever, headache, sore throat | 12/3/2020 | Negative | 12/3/2020 | 8/4/2020 |
| 7 | 55 | F | 29/2/2020 | Cough, sore throat | 12/3/2020 | Negative | 12/3/2020 | 8/4/2020 |
| 8 | 41 | F | 9/3/2020 | Headache, fever, body aches and rash | 14/3/2020 | Negative | 16/3/2020 | 8/4/2020 |
| 10 | 48 | M | 12/3/2020 | Chest pain, chest tightness, short of breath | 27/3/2020 | Negative | 30/3/2020 | 8/4/2020 |
| 11 | 31 | M | 14/3/2020 | Stuffy running nose, cough, sore throat | 24/3/2020 | Confirmed | 1/4/2020 | 8/4/2020 |
| 12 | 31 | M | 14/3/2020 | Stuffy running nose, cough, sore throat | 1/4/2020 | Confirmed | 24/3/2020 | 8/4/2020 |
| 13 | 27 | F | 6/3/2020 | Fever, cough, abnormal taste/smell, rhinorrhea | 18/3/2020 | Confirmed | 30/3/2020 | 1/9/2020 |
| 14 | 50 | F | 24/3/2020 | Fever, abnormal taste, chills | 31/3/2020 | Confirmed | 6/4/2020 | 1/9/2020 |
| 15 | 23 | F | 27/3/2020 | Abnormal smell, rhinorrhea | 27/3/2020 | Confirmed | 6/4/2020 | 1/9/2020 |
| 16 | 21 | F | 19/3/2020 | Fever, cough, abnormal taste/smell, diarrhea, chest pain | 24/3/2020 | Confirmed | 21/4/2020 | 1/9/2020 |
| 17 | 34 | M | 10/3/2020 | Fever, cough, abnormal taste/smell | 18/3/2020 | Confirmed | 21/4/2020 | 1/9/2020 |
| COVID-19 Molecular Diagnostics Provider | New Spectrum Analyzer Platform | Abbott CMIA | Bio-Rad ELISA | Roche ECLIA |
|---|---|---|---|---|
| Platform | LFA | Laboratory-based inventories | Laboratory-based inventories | Laboratory-based inventories |
| Spectral analysis | Reflection spectra (α light intensity) (300–1000 nm) Resolution = 5 nm | Luminescence COI (300–800 nm) | Filter (titer) (OD = 450 nm, ref = 650 nm) | Relative light unit (specific 300–650 nm) Resolution = 15 nm |
| Sensitivity (confirmed cases/test positive cases) | 100% (8/8) | 89% (109/122) [30] | 98% (49/50) [31] | 82% (409/496) [32] |
| Sample preparation | No | Yes | Yes | Yes |
| Specimen | Whole blood, Serum, plasma | Serum, plasma | Serum, plasma | Serum, plasma |
| Calculation | Index (α) | Index (S/C) | Information not available | Information not available |
| Turnaround time | 5–10 min | 10–15 min | 1 h | 1 h |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hung, K.-F.; Hung, C.-H.; Hong, C.; Chen, S.-C.; Sun, Y.-C.; Wen, J.-W.; Kuo, C.-H.; Ko, C.-H.; Cheng, C.-M. Quantitative Spectrochip-Coupled Lateral Flow Immunoassay Demonstrates Clinical Potential for Overcoming Coronavirus Disease 2019 Pandemic Screening Challenges. Micromachines 2021, 12, 321. https://doi.org/10.3390/mi12030321
Hung K-F, Hung C-H, Hong C, Chen S-C, Sun Y-C, Wen J-W, Kuo C-H, Ko C-H, Cheng C-M. Quantitative Spectrochip-Coupled Lateral Flow Immunoassay Demonstrates Clinical Potential for Overcoming Coronavirus Disease 2019 Pandemic Screening Challenges. Micromachines. 2021; 12(3):321. https://doi.org/10.3390/mi12030321
Chicago/Turabian StyleHung, Kai-Feng, Chih-Hsing Hung, Chitsung Hong, Szu-Chia Chen, Yi-Chen Sun, Jyun-Wei Wen, Chao-Hung Kuo, Cheng-Hao Ko, and Chao-Min Cheng. 2021. "Quantitative Spectrochip-Coupled Lateral Flow Immunoassay Demonstrates Clinical Potential for Overcoming Coronavirus Disease 2019 Pandemic Screening Challenges" Micromachines 12, no. 3: 321. https://doi.org/10.3390/mi12030321