Inflammatory Profile Associated with Secondary Infection from Bothrops atrox Snakebites in the Brazilian Amazon

 , , , ,
, , , ,  , , , ,
, , , ,  ,
,
Abstract
:1. Introduction
2. Results
2.1. Factors Associated to Secondary Infections
2.2. Local Clinical Manifestations Analysis
2.3. Laboratory Parameters
2.4. Soluble Immunological Molecules Profile
3. Discussion
4. Conclusions
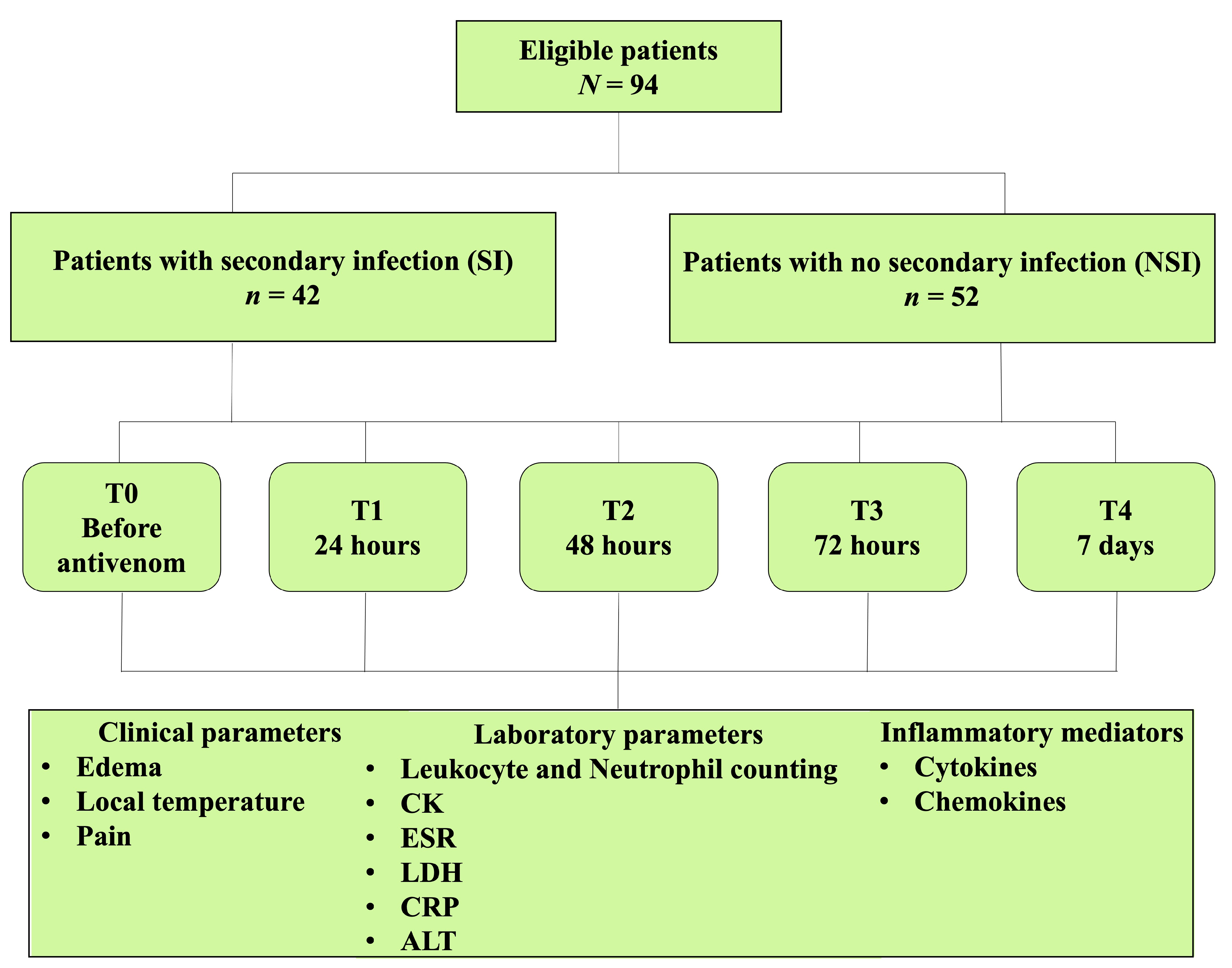
5. Materials and Methods
5.1. Study Design, Participants and Ethical Aspects
5.2. Admission and Follow-Up Procedures
5.3. Secondary Infection Diagnosis
5.4. Clinical Parameters
5.4.1. Edema
5.4.2. Local Temperature
5.4.3. Pain
5.5. Laboratory Parameters
5.6. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gutiérrez, J.M.; Calvete, J.J.; Habib, A.G.; Harrison, R.A.; Williams, D.J.; Warrell, D.A. Snakebite envenoming. Nat. Rev. Dis. Prim. 2017, 3, 17063. [Google Scholar] [CrossRef]
- Seifert, S.A.; Armitage, J.O.; Sanchez, E.E. Snake Envenomation. N. Engl. J. Med. 2022, 386, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Bhaumik, S.; Beri, D.; Lassi, Z.S.; Jagnoor, J. Interventions for the management of snakebite envenoming: An overview of systematic reviews. PLoS Negl. Trop. Dis. 2020, 14, e0008727. [Google Scholar] [CrossRef] [PubMed]
- Ralph, R.; Faiz, M.A.; Sharma, S.K.; Ribeiro, I.; Chappuis, F. Managing snakebite. BMJ 2022, 376, e057926. [Google Scholar] [CrossRef] [PubMed]
- Roriz, K.R.P.S.; Zaqueo, K.D.; Setubal, S.S.; Katsuragawa, T.H.; Silva, R.R.D.; Fernandes, C.F.C.; Cardoso, L.A.P.; Rodrigues, M.M.S.; Soares, A.M.; Stábeli, R.G.; et al. Epidemiological study of snakebite cases in Brazilian Western Amazonia. Rev. Da. Soc. Bras. De Med. Trop. 2018, 51, 338–346. [Google Scholar] [CrossRef]
- Souza, T.C.; Farias, B.E.S.; Bernarde, P.S.; Chiaravalotti Neto, F.; Frade, D.D.R.; Brilhante, A.F.; Melchior, L.A.K. Temporal trend and epidemiological profile of accidents involving venomous animals in Brazil, 2007–2019. Epidemiol. Serv. Saude 2022, 31, e2022025. [Google Scholar] [CrossRef] [PubMed]
- Chippaux, J.P. Incidence and mortality due to snakebite in the Americas. PLoS Negl. Trop. Dis. 2017, 11, e0005662. [Google Scholar] [CrossRef]
- Magalhães, S.F.V.; Peixoto, H.M.; Moura, N.; Monteiro, W.M.; de Oliveira, M.R.F. Snakebite envenomation in the Brazilian Amazon: A descriptive study. Trans. R. Soc. Trop. Med. Hyg. 2019, 113, 143–151. [Google Scholar] [CrossRef]
- Monteiro, W.M.; Contreras-Bernal, J.C.; Bisneto, P.F.; Sachett, J.; Mendonça da Silva, I.; Lacerda, M.; Guimarães da Costa, A.; Val, F.; Brasileiro, L.; Sartim, M.A.; et al. Bothrops atrox, the most important snake involved in human envenomings in the amazon: How venomics contributes to the knowledge of snake biology and clinical toxinology. Toxicon X 2020, 6, 100037. [Google Scholar] [CrossRef]
- Rucavado, A.; Nicolau, C.A.; Escalante, T.; Kim, J.; Herrera, C.; Gutiérrez, J.M.; Fox, J.W. Viperid Envenomation Wound Exudate Contributes to Increased Vascular Permeability via a DAMPs/TLR-4 Mediated Pathway. Toxins 2016, 8, 349. [Google Scholar] [CrossRef]
- Rucavado, A.; Escalante, T.; Kalogeropoulos, K.; Camacho, E.; Gutiérrez, J.M.; Fox, J.W. Analysis of wound exudates reveals differences in the patterns of tissue damage and inflammation induced by the venoms of Daboia russelii and Bothrops asper in mice. Toxicon 2020, 186, 94–104. [Google Scholar] [CrossRef]
- Zychar, B.C.; Clissa, P.B.; Carvalho, E.; Alves, A.S.; Baldo, C.; Faquim-Mauro, E.L.; Gonçalves, L.R.C. Modulation of Adhesion Molecules Expression by Different Metalloproteases Isolated from Bothrops Snakes. Toxins 2021, 13, 803. [Google Scholar] [CrossRef]
- Moreira, V.; Dos-Santos, M.C.; Nascimento, N.G.; Borges da Silva, H.; Fernandes, C.M.; D'Império Lima, M.R.; Teixeira, C. Local inflammatory events induced by Bothrops atrox snake venom and the release of distinct classes of inflammatory mediators. Toxicon 2012, 60, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Sachett, J.A.G.; da Silva, I.M.; Alves, E.C.; Oliveira, S.S.; Sampaio, V.S.; do Vale, F.F.; Romero, G.A.S.; Dos Santos, M.C.; Marques, H.O.; Colombini, M.; et al. Poor efficacy of preemptive amoxicillin clavulanate for preventing secondary infection from Bothrops snakebites in the Brazilian Amazon: A randomized controlled clinical trial. PLoS Negl. Trop. Dis. 2017, 11, e0005745. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.W.; Wang, J.D.; Huang, J.A.; Hu, S.Y.; Wang, L.M.; Tsan, Y.T. Wound infections secondary to snakebite in central Taiwan. J. Venom. Anim. Toxins Incl. Trop. Dis. 2012, 18, 1129–1135. [Google Scholar] [CrossRef]
- Sadeghi, M.; Barazandeh, M.; Zakariaei, Z.; Davoodi, L.; Tabaripour, R.; Fakhar, M.; Zakariaei, A. Massive cutaneous complications due to snakebite: A case report and literature review. Clin. Case Rep. 2021, 9, e04129. [Google Scholar] [CrossRef]
- Garg, A.; Sujatha, S.; Garg, J.; Acharya, N.S.; Chandra Parija, S. Wound infections secondary to snakebite. J. Infect. Dev. Ctries. 2009, 3, 221–223. [Google Scholar] [CrossRef] [PubMed]
- Mao, Y.C.; Liu, P.Y.; Hung, D.Z.; Lai, W.C.; Huang, S.T.; Hung, Y.M.; Yang, C.C. Bacteriology of Naja atra Snakebite Wound and Its Implications for Antibiotic Therapy. Am. J. Trop. Med. Hyg. 2016, 94, 1129–1135. [Google Scholar] [CrossRef] [PubMed]
- Resiere, D.; Gutiérrez, J.M.; Névière, R.; Cabié, A.; Hossein, M.; Kallel, H. Antibiotic therapy for snakebite envenoming. J. Venom. Anim. Toxins Incl. Trop. Dis. 2020, 26, e20190098. [Google Scholar] [CrossRef] [PubMed]
- Mendes, V.K.D.G.; Pereira, H.D.S.; Elias, I.C.; Soares, G.S.; Santos, M.; Talhari, C.; Cordeiro-Santos, M.; Monteiro, W.M.; Sachett, J.A.G. Secondary infection profile after snakebite treated at a tertiary referral center in the Brazilian Amazon. Rev. Soc. Bras. Med. Trop. 2022, 55, e0244. [Google Scholar] [CrossRef]
- Dantas, A.P.C.; Sifuentes, D.N.; Wen, F.H.; Dourado, F.S.; de Lima Junior, F.E.F.; França, F.O.S.; Reckziegel, G.C.; Pereira, L.R.M.; Santalucia, M.; Wada, M.Y.; et al. Acidente ofídico. In Guia de Vigilância em Saúde Secretaria de Vigilância em Saúde, 5th ed.; de Medeiros, A.C., Ed.; Ministério da Saúde: Brasília, Brasil, 2021; p. 1019. [Google Scholar]
- Sandoz, H. An overview of the prevention and management of wound infection. Nurs. Stand. 2022, 37, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Mamede, C.C.N.; de Sousa Simamoto, B.B.; da Cunha Pereira, D.F.; de Oliveira Costa, J.; Ribeiro, M.S.M.; de Oliveira, F. Edema, hyperalgesia and myonecrosis induced by Brazilian bothropic venoms: Overview of the last decade. Toxicon 2020, 187, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Maciel Salazar, G.K.; Saturnino Cristino, J.; Vilhena Silva-Neto, A.; Seabra Farias, A.; Alcântara, J.A.; Azevedo Machado, V.; Murta, F.; Souza Sampaio, V.; Val, F.; Sachett, A.; et al. Snakebites in “Invisible Populations”: A cross-sectional survey in riverine populations in the remote western Brazilian Amazon. PLoS Negl. Trop. Dis. 2021, 15, e0009758. [Google Scholar] [CrossRef] [PubMed]
- Ibiapina, H.N.S.; Costa, A.G.; Sachett, J.A.G.; Silva, I.M.; Tarragô, A.M.; Neves, J.C.F.; Kerr, M.W.A.; Santana, M.F.; Martins-Filho, O.A.; Lacerda, M.V.G.; et al. An Immunological Stairway to Severe Tissue Complication Assembly in Bothrops atrox Snakebites. Front. Immunol. 2019, 10, 1882. [Google Scholar] [CrossRef]
- Moreira, V.; Teixeira, C.; Borges da Silva, H.; D'Império Lima, M.R.; Dos-Santos, M.C. The role of TLR2 in the acute inflammatory response induced by Bothrops atrox snake venom. Toxicon 2016, 118, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Leonel, T.B.; Gabrili, J.J.M.; Squaiella-Baptistão, C.C.; Woodruff, T.M.; Lambris, J.D.; Tambourgi, D.V. Bothrops jararaca Snake Venom Inflammation Induced in Human Whole Blood: Role of the Complement System. Front. Immunol. 2022, 13, 885223. [Google Scholar] [CrossRef]
- Raziyeva, K.; Kim, Y.; Zharkinbekov, Z.; Kassymbek, K.; Jimi, S.; Saparov, A. Immunology of Acute and Chronic Wound Healing. Biomolecules 2021, 11, 700. [Google Scholar] [CrossRef]
- Malone, M.; Schultz, G. Challenges in the diagnosis and management of wound infection. Br. J. Dermatol. 2022, 187, 159–166. [Google Scholar] [CrossRef]
- Alangode, A.; Rajan, K.; Nair, B.G. Snake antivenom: Challenges and alternate approaches. Biochem. Pharmacol. 2020, 181, 114135. [Google Scholar] [CrossRef]
- Rojnuckarin, P.; Chanthawibun, W.; Noiphrom, J.; Pakmanee, N.; Intragumtornchai, T. A randomized, double-blind, placebo-controlled trial of antivenom for local effects of green pit viper bites. Trans. R. Soc. Trop. Med. Hyg. 2006, 100, 879–884.2. [Google Scholar] [CrossRef]
- Santoro, M.L.; Sano-Martins, I.S.; Fan, H.W. Haematological evaluation of patients bitten by the jararaca, Bothrops jararaca, in Brazil. Toxicon 2008, 51, 1440–1448. [Google Scholar] [CrossRef]
- Luyendyk, J.P.; Schoenecker, J.G.; Flick, M.J. The multifaceted role of fibrinogen in tissue injury and inflammation. Blood 2019, 133, 511–520. [Google Scholar] [CrossRef] [PubMed]
- Sachetto, A.T.A.; Jensen, J.R.; Santoro, M.L. Liver gene regulation of hemostasis-related factors is altered by experimental snake envenomation in mice. PLoS Negl. Trop. Dis. 2020, 14, e0008379. [Google Scholar] [CrossRef] [PubMed]
- Larréché, S.; Chippaux, J.P.; Chevillard, L.; Mathé, S.; Résière, D.; Siguret, V.; Mégarbane, B. Bleeding and Thrombosis: Insights into Pathophysiology of Bothrops Venom-Related Hemostasis Disorders. Int. J. Mol. Sci. 2021, 22, 9643. [Google Scholar] [CrossRef]
- Resiere, D.; Mehdaoui, H.; Neviere, R. Inflammation and Oxidative Stress in Snakebite Envenomation: A Brief Descriptive Review and Clinical Implications. Toxins 2022, 14, 802. [Google Scholar] [CrossRef]
- Escocard, R.d.C.; Kanashiro, M.M.; Petretski, J.H.; Azevedo-Silva, J.; Queiroz de Carvalho, E.C.; Dias da Silva, W.; Kipnis, T.L. Neutrophils regulate the expression of cytokines, chemokines and nitric oxide synthase/nitric oxide in mice injected with Bothrops atrox venom. Immunobiology 2006, 211, 37–46. [Google Scholar] [PubMed]
- Ambrosch, A.; Lobmann, R.; Pott, A.; Preissler, J. Interleukin-6 concentrations in wound fluids rather than serological markers are useful in assessing bacterial triggers of ulcer inflammation. Int. Wound. J. 2008, 5, 99–106. [Google Scholar] [CrossRef]
- Al-Jebouri, M.; Al-Mahmood, B. Estimation of Cytokines Involved in Acute-Phase Wound Infection with Reference to Residence Time of Patients in Hospitals. Mod. Res. Inflamm. 2019, 8, 1–10. [Google Scholar] [CrossRef]
- Ridiandries, A.; Tan, J.T.M.; Bursill, C.A. The Role of Chemokines in Wound Healing. Int. J. Mol. Sci. 2018, 19, 3217. [Google Scholar] [CrossRef]
- Davalos, D.; Akassoglou, K. Fibrinogen as a key regulator of inflammation in disease. Semin. Immunopathol. 2012, 34, 43–62. [Google Scholar] [CrossRef]
- Cavalcante, J.S.; Brito, I.M.D.C.; De Oliveira, L.A.; De Barros, L.C.; Almeida, C.; Rossini, B.C.; Sousa, D.L.; Alves, R.S.; Jorge, R.J.B.; Santos, L.D.D. Experimental Bothrops atrox Envenomation: Blood Plasma Proteome Effects after Local Tissue Damage and Perspectives on Thromboinflammation. Toxins 2022, 14, 613. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, C.; Fernandes, C.M.; Leiguez, E.; Chudzinski-Tavassi, A.M. Inflammation Induced by Platelet-Activating Viperid Snake Venoms: Perspectives on Thromboinflammation. Front. Immunol. 2019, 10, 2082. [Google Scholar] [CrossRef] [PubMed]
- Wellmann, I.A.M.; Ibiapina, H.N.S.; Sachett, J.A.G.; Sartim, M.A.; Silva, I.M.; Oliveira, S.S.; Tarragô, A.M.; Moura-da-Silva, A.M.; Lacerda, M.V.G.; Ferreira, L.C.L.; et al. Correlating Fibrinogen Consumption and Profiles of Inflammatory Molecules in Human Envenomation's by Bothrops atrox in the Brazilian Amazon. Front. Immunol. 2020, 11, 1874. [Google Scholar] [CrossRef] [PubMed]
- Pardal, P.P.; Souza, S.M.; Monteiro, M.R.; Fan, H.W.; Cardoso, J.L.; França, F.O.; Tomy, S.C.; Sano-Martins, I.S.; de Sousa-e-Silva, M.C.; Colombini, M.; et al. Clinical trial of two antivenoms for the treatment of Bothrops and Lachesis bites in the north eastern Amazon region of Brazil. Trans. R. Soc. Trop. Med. Hyg. 2004, 98, 28–42. [Google Scholar] [CrossRef]
- Huskisson, E.C. Measurement of pain. J. Rheumatol. 1982, 9, 768–769. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total (%) N = 94 | SI (%) n = 42 | NSI (%) n = 52 | OR | CI 95% | p Value |
|---|---|---|---|---|---|---|
| Gender | ||||||
| Female | 14 (14.9) | 6 (14.3) | 8 (15.4) | 0.92 | 0.29–2.89 | 0.882 |
| Male | 80 (85.1) | 36 (85.7) | 44 (84.6) | 1 | - | - |
| Age (years) | ||||||
| 0–10 | 5 (5.4) | 4 (9.5) | 1 (2.0) | 1 | - | - |
| 11–20 | 11 (11.8) | 5 (11.9) | 6 (11.8) | 0.21 | 0.02–2.52 | 0.217 |
| 21–40 | 36 (39.8) | 16 (38.1) | 21 (41.2) | 0.19 | 0.02–1.87 | 0.155 |
| 41–60 | 27 (29.0) | 13 (31.0) | 14 (27.5) | 0.23 | 0.02–2.36 | 0.217 |
| >60 | 13 (14.0) | 4 (9.5) | 9 (17.7) | 0.11 | 0.01–1.34 | 0.083 |
| Area of occurrence | ||||||
| Urban | 7 (7.5) | 3 (7.1) | 4 (7.8) | 1 | - | - |
| Rural | 86 (92.5) | 39 (92.9) | 47 (92.2) | 1.11 | 0.23–5.24 | 0.899 |
| Bite site | ||||||
| Lower limbs | 18 (19.4) | 10 (23.8) | 8 (15.7) | 1 | - | - |
| Upper limbs | 2 (2.2) | 0 (0.0) | 2 (3.9) | - | - | - |
| Hand | 15 (16.1) | 3 (7.1) | 12 (23.5) | 0.20 | 0.04–0.96 | 0.045 * |
| Foot | 58 (62.4) | 29 (69.1) | 29 (56.9) | 0.80 | 0.28–2.32 | 0.681 |
| Work-related bite | 44 (47.3) | 18 (42.9) | 26 (51.0) | 0.72 | 0.32–1.64 | 0.435 |
| Time to assistance (hours) | ||||||
| 0–3 | 58 (61.7) | 23 (54.7) | 35 (67.3) | 1 | - | - |
| 4–6 | 17 (17.0) | 10 (23.8) | 7 (13.4) | 1.96 | 0.64–5.99 | 0.240 |
| >6 | 19 (21.3) | 9 (21.4) | 10 (19.2) | 1.52 | 0.55–4.23 | 0.421 |
| Previous snakebite history | 13 (14.0) | 6 (14.3) | 7 (13.7) | 0.95 | 0.29–3.09 | 0.938 |
| Use of topical medicines | 35 (37.6) | 14 (33.3) | 21 (41.2) | 0.71 | 0.31–1.67 | 0.438 |
| Use of oral medicines | 31 (33.3) | 13 (31.0) | 18 (35.3) | 0.84 | 0.37–2.02 | 0.8261 |
| Use of tourniquet | 22 (23.7) | 11 (26.2) | 11 (21.6) | 1.29 | 0.50–3.36 | 0.602 |
| Snakebite clinical classification | ||||||
| Mild | 36 (38.7) | 11 (26.2) | 25 (49.0) | 1 | - | - |
| Moderate | 48 (51.6) | 26 (61.9) | 22 (43.1) | 2.69 | 1.08–6.66 | 0.033 * |
| Severe | 9 (9.7) | 5 (11.9) | 4 (7.8) | 2.84 | 0.64–12.65 | 0.171 |
| Antivenom vials administrated | ||||||
| 2–4 | 15 (15.9) | 4 (9.5) | 11 (21.1) | 1 | - | - |
| 5–8 | 59 (62.7) | 27 (64.2) | 32 (61.5) | 2.32 | 0.66–8.13 | 0.188 |
| 9–12 | 19 (20.2) | 11 (26.1) | 8 (15.3) | 3.36 | 0.79–14.25 | 0.100 |
| Comorbidities % | 8 (8.51) | 3 (7.14) | 5 (9.62) | 0.72 | 0.16–3.22 | 0.670 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cavalcante, T.T.A.; de Souza, M.B.S.; Neves, J.C.F.; Ibiapina, H.N.S.; Barbosa, F.B.A.; Bentes, K.O.; Alves, E.C.; Marques, H.O.; Colombini, M.; Sampaio, S.V.; et al. Inflammatory Profile Associated with Secondary Infection from Bothrops atrox Snakebites in the Brazilian Amazon. Toxins 2023, 15, 524. https://doi.org/10.3390/toxins15090524
Cavalcante TTA, de Souza MBS, Neves JCF, Ibiapina HNS, Barbosa FBA, Bentes KO, Alves EC, Marques HO, Colombini M, Sampaio SV, et al. Inflammatory Profile Associated with Secondary Infection from Bothrops atrox Snakebites in the Brazilian Amazon. Toxins. 2023; 15(9):524. https://doi.org/10.3390/toxins15090524
Chicago/Turabian StyleCavalcante, Távila Tatiane Amorim, Márcia Beatriz Silva de Souza, Juliana Costa Ferreira Neves, Hiochelson Najibe Santos Ibiapina, Fabiane Bianca Albuquerque Barbosa, Karolaine Oliveira Bentes, Eliane Campos Alves, Hedylamar Oliveira Marques, Monica Colombini, Suely Vilela Sampaio, and et al. 2023. "Inflammatory Profile Associated with Secondary Infection from Bothrops atrox Snakebites in the Brazilian Amazon" Toxins 15, no. 9: 524. https://doi.org/10.3390/toxins15090524