
The Effect of Prior Creatine Intake for 28 Days on Accelerated Recovery from Exercise-Induced Muscle Damage: A Double-Blind, Randomized, Placebo-Controlled Trial
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
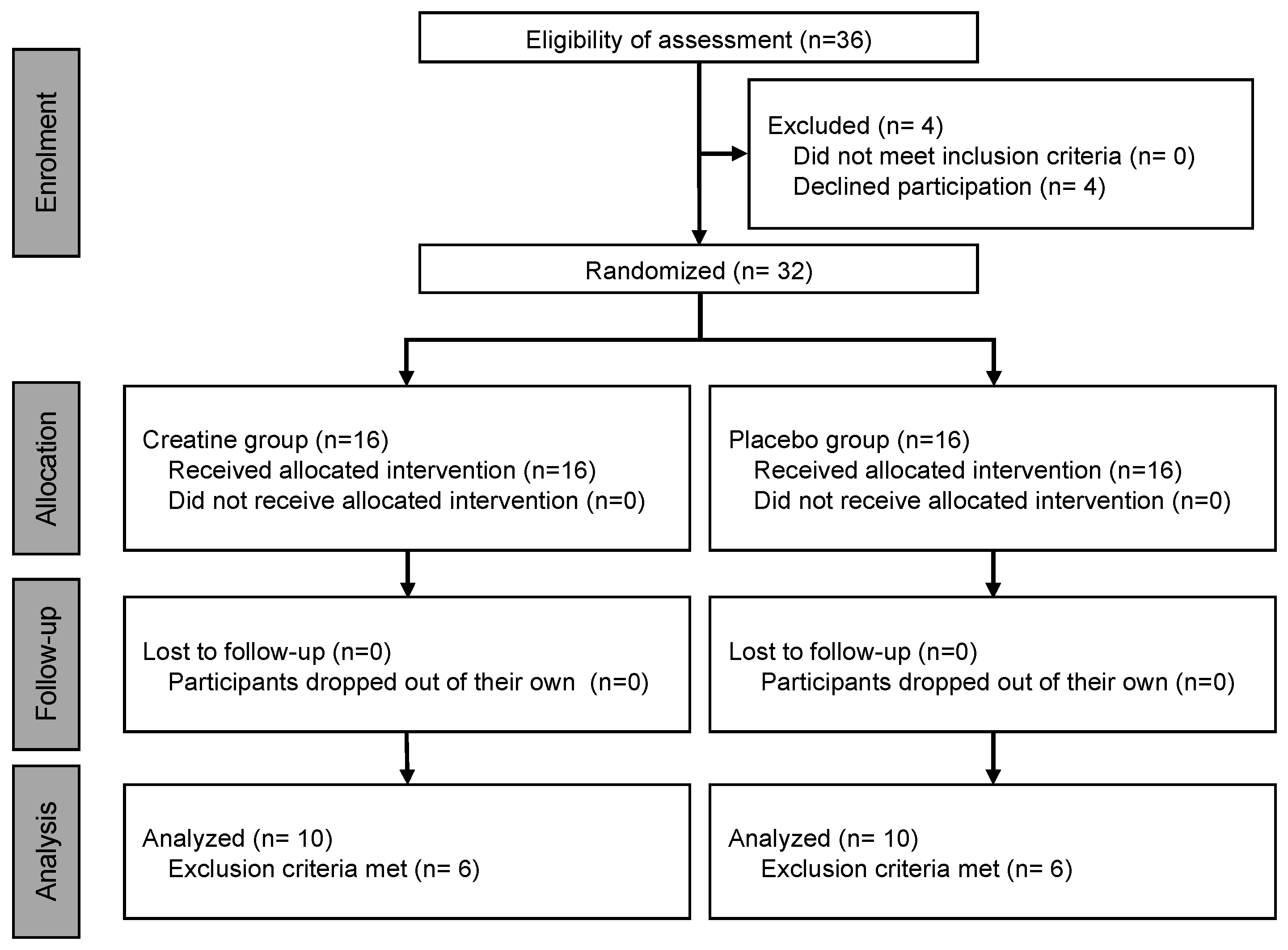
2.1. Participants
2.2. Experimental Design
2.3. Eccentric Exercise
2.4. Maximum Voluntary Contraction Evaluation
2.5. Active Range of Motion
2.6. Subjective Evaluation
2.7. Circumference
2.8. Muscle Shear Modulus
2.9. Titin N-Terminal Fragment Excretion Assay
2.10. Statistical Analysis
3. Results
EIMD Indices
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fridén, J.; Lieber, R.L. Structural and mechanical basis of exercise-induced muscle injury. Med. Sci. Sports Exerc. 1992, 24, 521–530. [Google Scholar] [CrossRef] [PubMed]
- Inami, T.; Yamaguchi, S.; Ishida, H.; Kohtake, N.; Morito, A.; Yamada, S.; Shimomasuda, M.; Haramoto, M.; Nagata, N.; Murayama, M. Changes in muscle shear modulus and urinary titin N-terminal fragment after eccentric exercise. J. Sports Sci. Med. 2022, 21, 536–544. [Google Scholar] [CrossRef] [PubMed]
- Nosaka, K.; Newton, M. Concentric or eccentric training effect on eccentric exercise-induced muscle damage. Med. Sci. Sports Exerc. 2002, 34, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Nosaka, K.; Sakamoto, K.; Newton, M.; Sacco, P. How long does the protective effect on eccentric exercise-induced muscle damage last? Med. Sci. Sports Exerc. 2001, 33, 1490–1495. [Google Scholar] [CrossRef]
- Iguchi, J.; Hojo, T.; Fujisawa, Y.; Kuzuhara, K.; Yanase, K.; Hirono, T.; Koyama, Y.; Tateuchi, H.; Ichihashi, N. Synergistic dominance induced by hip extension exercise alters biomechanics and muscular activity during sprinting and suggests a potential link to hamstring strain. J. Strength Cond. Res. 2023, 37, 1770–1776. [Google Scholar] [CrossRef] [PubMed]
- Tanabe, Y.; Maeda, S.; Akazawa, N.; Zempo-Miyaki, A.; Choi, Y.; Ra, S.G.; Imaizumi, A.; Otsuka, Y.; Nosaka, K. Attenuation of indirect markers of eccentric exercise-induced muscle damage by curcumin. Eur. J. Appl. Physiol. 2015, 115, 1949–1957. [Google Scholar] [CrossRef] [PubMed]
- Tanabe, Y.; Fujii, N.; Suzuki, K. Dietary supplementation for attenuating exercise-induced muscle damage and delayed-onset muscle soreness in humans. Nutrients 2021, 14, 70. [Google Scholar] [CrossRef]
- Kreider, R.B.; Stout, J.R. Creatine in health and disease. Nutrients 2021, 13, 447. [Google Scholar] [CrossRef]
- Brosnan, M.E.; Brosnan, J.T. The role of dietary creatine. Amino Acids 2016, 48, 1785–1791. [Google Scholar] [CrossRef]
- Dolan, E.; Gualano, B.; Rawson, E.S. Beyond muscle: The effects of creatine supplementation on brain creatine, cognitive processing, and traumatic brain injury. Eur. J. Sport. Sci. 2019, 19, 1–14. [Google Scholar] [CrossRef]
- Busanello, E.N.B.; Marques, A.C.; Lander, N.; de Oliveira, D.N.; Catharino, R.R.; Oliveira, H.C.F.; Vercesi, A.E. Pravastatin chronic treatment sensitizes hypercholesterolemic mice muscle to mitochondrial permeability transition: Protection by creatine or coenzyme Q10. Front. Pharmacol. 2017, 8, 185. [Google Scholar] [CrossRef]
- Wang, C.C.; Fang, C.C.; Lee, Y.H.; Yang, M.T.; Chan, K.H. Effects of 4-week creatine supplementation combined with complex training on muscle damage and sport performance. Nutrients 2018, 10, 1640. [Google Scholar] [CrossRef]
- Rosene, J.; Matthews, T.; Ryan, C.; Belmore, K.; Bergsten, A.; Blaisdell, J.; Gaylord, J.; Love, R.; Marrone, M.; Ward, K.; et al. Short and longer-term effects of creatine supplementation on exercise induced muscle damage. J. Sports Sci. Med. 2009, 8, 89–96. [Google Scholar] [PubMed]
- Northeast, B.; Clifford, T. The effect of creatine supplementation on markers of exercise-induced muscle damage: A systematic review and meta-analysis of human intervention trials. Int. J. Sport. Nutr. Exerc. Metab. 2021, 31, 276–291. [Google Scholar] [CrossRef] [PubMed]
- Evans, R.K.; Knight, K.L.; Draper, D.O.; Parcell, A.C. Effects of warm-up before eccentric exercise on indirect markers of muscle damage. Med. Sci. Sports Exerc. 2002, 34, 1892–1899. [Google Scholar] [CrossRef] [PubMed]
- Markus, I.; Constantini, K.; Hoffman, J.R.; Bartolomei, S.; Gepner, Y. Exercise-induced muscle damage: Mechanism, assessment and nutritional factors to accelerate recovery. Eur. J. Appl. Physiol. 2021, 121, 969–992. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, S.; Suzuki, K.; Kanda, K.; Okada, J. N-terminal fragments of titin in urine as a biomarker for eccentric exercise-induced muscle damage. J. Phys. Fit. Sports Med. 2020, 9, 21–29. [Google Scholar] [CrossRef]
- Nosaka, K.; Newton, M. Repeated eccentric exercise bouts do not exacerbate muscle damage and repair. J. Strength Cond. Res. 2002, 16, 117–122. [Google Scholar] [CrossRef]
- Yamaguchi, S.; Suzuki, K.; Kanda, K.; Inami, T.; Okada, J. Changes in urinary titin N-terminal fragments as a biomarker of exercise-induced muscle damage in the repeated bout effect. J. Sci. Med. Sport. 2020, 23, 536–540. [Google Scholar] [CrossRef]
- Nosaka, K.; Clarkson, P.M. Changes in indicators of inflammation after eccentric exercise of the elbow flexors. Med. Sci. Sports Exerc. 1996, 28, 953–961. [Google Scholar] [CrossRef]
- Maruyama, N.; Asai, T.; Abe, C.; Inada, A.; Kawauchi, T.; Miyashita, K.; Maeda, M.; Matsuo, M.; Nabeshima, Y.I. Establishment of a highly sensitive sandwich ELISA for the N-terminal fragment of titin in urine. Sci. Rep. 2016, 6, 39375. [Google Scholar] [CrossRef]
- Yamaguchi, S.; Suzuki, K.; Inami, T.; Kanda, K.; Hanye, Z.; Okada, J. Changes in urinary titin N-terminal fragment concentration after concentric and eccentric exercise. J. Sports Sci. Med. 2020, 19, 121–129. [Google Scholar]
- Doma, K.; Ramachandran, A.K.; Boullosa, D.; Connor, J. The paradoxical effect of creatine monohydrate on muscle damage markers: A systematic review and meta-analysis. Sports Med. 2022, 52, 1623–1645. [Google Scholar] [CrossRef] [PubMed]
- Cooke, M.B.; Rybalka, E.; Williams, A.D.; Cribb, P.J.; Hayes, A. Creatine supplementation enhances muscle force recovery after eccentrically-induced muscle damage in healthy individuals. J. Int. Soc. Sports Nutr. 2009, 6, 13. [Google Scholar] [CrossRef] [PubMed]
- Deldicque, L.; Louis, M.; Theisen, D.; Nielens, H.; Dehoux, M.; Thissen, J.P.; Rennie, M.J.; Francaux, M. Increased IGF mRNA in human skeletal muscle after creatine supplementation. Med. Sci. Sports Exerc. 2005, 37, 731–736. [Google Scholar] [CrossRef] [PubMed]
- Close, G.L.; Ashton, T.; Cable, T.; Doran, D.; MacLaren, D.P.M. Eccentric exercise, isokinetic muscle torque and delayed onset muscle soreness: The role of reactive oxygen species. Eur. J. Appl. Physiol. 2004, 91, 615–621. [Google Scholar] [CrossRef] [PubMed]
- Hyldahl, R.D.; Hubal, M.J. Lengthening our perspective: Morphological, cellular, and molecular responses to eccentric exercise. Muscle Nerve 2014, 49, 155–170. [Google Scholar] [CrossRef]
- Lawler, J.M.; Barnes, W.S.; Wu, G.; Song, W.; Demaree, S. Direct antioxidant properties of creatine. Biochem. Biophys. Res. Commun. 2002, 290, 47–52. [Google Scholar] [CrossRef]
- Sestili, P.; Martinelli, C.; Bravi, G.; Piccoli, G.; Curci, R.; Battistelli, M.; Falcieri, E.; Agostini, D.; Gioacchini, A.M.; Stocchi, V. Creatine supplementation affords cytoprotection in oxidatively injured cultured mammalian cells via direct antioxidant activity. Free Radic. Biol. Med. 2006, 40, 837–849. [Google Scholar] [CrossRef]
- Bassit, R.A.; Curi, R.; Costa Rosa, L.F.B.P. Creatine supplementation reduces plasma levels of pro-inflammatory cytokines and PGE2 after a half-ironman competition. Amino Acids 2008, 35, 425–431. [Google Scholar] [CrossRef]
- Santos, R.V.T.; Bassit, R.A.; Caperuto, E.C.; Costa Rosa, L.F.B.P. The effect of creatine supplementation upon inflammatory and muscle soreness markers after a 30 km race. Life Sci. 2004, 75, 1917–1924. [Google Scholar] [CrossRef] [PubMed]
- Nomura, A.; Zhang, M.; Sakamoto, T.; Ishii, Y.; Morishima, Y.; Mochizuki, M.; Kimura, T.; Uchida, Y.; Sekizawa, K. Anti-inflammatory activity of creatine supplementation in endothelial cells in vitro. Br. J. Pharmacol. 2003, 139, 715–720. [Google Scholar] [CrossRef] [PubMed]
- Enoka, R.M.; Duchateau, J. Muscle fatigue: What, why and how it influences muscle function. J. Physiol. 2008, 586, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Allen, D.G.; Whitehead, N.P.; Yeung, E.W. Mechanisms of stretch-induced muscle damage in normal and dystrophic muscle: Role of ionic changes. J. Physiol. 2005, 567, 723–735. [Google Scholar] [CrossRef] [PubMed]
- Casey, A.; Greenhaff, P.L. Does dietary creatine supplementation play a role in skeletal muscle metabolism and performance? Am. J. Clin. Nutr. 2000, 72 (Suppl. 2), 607S–617S. [Google Scholar] [CrossRef] [PubMed]
- Korge, P.; Byrd, S.K.; Campbell, K.B. Functional coupling between sarcoplasmic-reticulum-bound creatine kinase and Ca2+-ATPase. Eur. J. Biochem. 1993, 213, 973–980. [Google Scholar] [CrossRef] [PubMed]
- Rawson, E.S.; Gunn, B.; Clarkson, P.M. The effects of creatine supplementation on exercise-induced muscle damage. J. Strength Cond. Res. 2001, 15, 178–184. [Google Scholar] [CrossRef]
- Yokota, Y.; Yamada, S.; Yamamoto, D.; Kato, K.; Morito, A.; Takaoka, A. Creatine supplementation alleviates fatigue after exercise through anti-inflammatory action in skeletal muscle and brain. Nutraceuticals 2023, 3, 234–249. [Google Scholar] [CrossRef]
- Chino, K.; Takahashi, H. Measurement of gastrocnemius muscle elasticity by shear wave elastography: Association with passive ankle joint stiffness and sex differences. Eur. J. Appl. Physiol. 2016, 116, 823–830. [Google Scholar] [CrossRef]
- Hill, A.V. The heat of shortening and the dynamic constants of muscle. Proc. R. Soc. Lond. B 1938, 126, 136–195. [Google Scholar] [CrossRef]
- Hicks, K.M.; Onambele-Pearson, G.L.; Winwood, K.; Morse, C.I. Muscle-tendon unit properties during eccentric exercise correlate with the creatine kinase response. Front. Physiol. 2017, 8, 657. [Google Scholar] [CrossRef]
- Doma, K.; Gahreman, D.; Connor, J. Fruit supplementation reduces indices of exercise-induced muscle damage: A systematic review and meta-analysis. Eur. J. Sport. Sci. 2021, 21, 562–579. [Google Scholar] [CrossRef] [PubMed]
- Doma, K.; Devantier-Thomas, B.; Gahreman, D.; Connor, J. Selected root plant supplementation reduces indices of exercise-induced muscle damage: A systematic review and meta-analysis. Int. J. Vitam. Nutr. Res. 2022, 92, 448–468. [Google Scholar] [CrossRef]
- Romero-Parra, N.; Cupeiro, R.; Alfaro-Magallanes, V.M.; Rael, B.; Rubio-Arias, J.Á.; Peinado, A.B.; Benito, P.J.; IronFEMME Study Group. Exercise-induced muscle damage during the menstrual cycle: A systematic review and meta-analysis. J. Strength Cond. Res. 2021, 35, 549–561. [Google Scholar] [CrossRef]
- Wax, B.; Kerksick, C.M.; Jagim, A.R.; Mayo, J.J.; Lyons, B.C.; Kreider, R.B. Creatine for Exercise and Sports Performance, with Recovery Considerations for Healthy Populations. Nutrients 2021, 13, 1915. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Levene’s Test | Independent t-Test | ||||||
|---|---|---|---|---|---|---|---|
| PLA | CRE | F-Value | p-Value | t-Value | p-Value | t-Test | |
| Age (years) | 23.9 ± 1.9 | 23.5 ± 4.1 | 1.390 | 0.252 | 0.753 | 0.460 | n.s. |
| Body Mass (kg) | 72.1 ± 11.2 | 70.4 ± 9.9 | 0.276 | 0.605 | 0.293 | 0.773 | n.s. |
| Body Fat (%) | 19.7 ± 4.2 | 17.5 ± 4.3 | 0.000 | 0.995 | 1.084 | 0.291 | n.s. |
| SLM (kg) | 54.2 ± 6.9 | 54.5 ± 6.2 | 0.003 | 0.959 | −0.084 | 0.934 | n.s. |
| ROM (deg) | 123.0 ± 5.3 | 120.2 ± 2.9 | 0.002 | 0.964 | 0.188 | 0.852 | n.s. |
| MVC (kgf) | 21.6 ± 2.8 | 21.6 ± 2.2 | 0.795 | 0.383 | 0.070 | 0.945 | n.s. |
| CIR (cm) | 28.6 ± 2.5 | 27.6 ± 1.8 | 0.726 | 0.404 | 0.703 | 0.490 | n.s. |
| SM (kPa) | 41.4 ± 6.7 | 45.6 ± 10.3 | 0.750 | 0.397 | −0.813 | 0.426 | n.s. |
| UTF/USG | 208.8 ± 161.9 | 313.1 ± 387.3 | 1.147 | 0.297 | −0.786 | 0.441 | n.s. |
| SOR (mm) | 0.0 ± 0.0 | 0.0 ± 0.0 | − | − | − | − | n.s. |
| MF (mm) | 0.0 ± 0.0 | 0.3 ± 0.8 | 5.833 | 0.027 | −1.176 | 0.255 | n.s. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamaguchi, S.; Inami, T.; Ishida, H.; Morito, A.; Yamada, S.; Nagata, N.; Murayama, M. The Effect of Prior Creatine Intake for 28 Days on Accelerated Recovery from Exercise-Induced Muscle Damage: A Double-Blind, Randomized, Placebo-Controlled Trial. Nutrients 2024, 16, 896. https://doi.org/10.3390/nu16060896
Yamaguchi S, Inami T, Ishida H, Morito A, Yamada S, Nagata N, Murayama M. The Effect of Prior Creatine Intake for 28 Days on Accelerated Recovery from Exercise-Induced Muscle Damage: A Double-Blind, Randomized, Placebo-Controlled Trial. Nutrients. 2024; 16(6):896. https://doi.org/10.3390/nu16060896
Chicago/Turabian StyleYamaguchi, Shota, Takayuki Inami, Hiroyuki Ishida, Akihisa Morito, Satoshi Yamada, Naoya Nagata, and Mitsuyoshi Murayama. 2024. "The Effect of Prior Creatine Intake for 28 Days on Accelerated Recovery from Exercise-Induced Muscle Damage: A Double-Blind, Randomized, Placebo-Controlled Trial" Nutrients 16, no. 6: 896. https://doi.org/10.3390/nu16060896