
Dietary Fibers in Healthy Children and in Pediatric Gastrointestinal Disorders: A Practical Guide

 and
and
Abstract
:1. Introduction
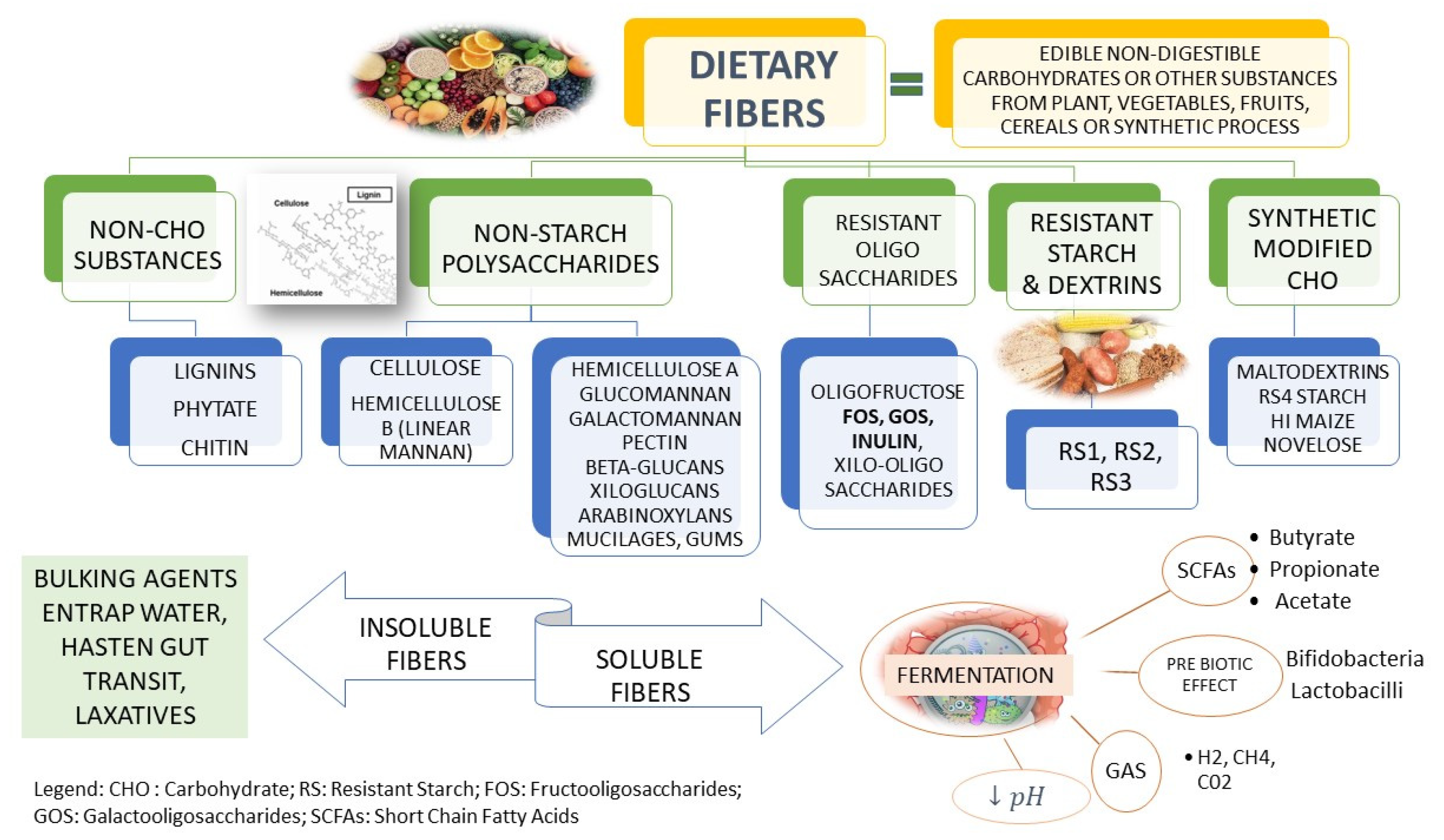
2. Definition and Type of Fibers
3. Fiber Requirement in Children
4. Fibers in Functional Gastrointestinal Disorders in Children
5. Fibers in Constipation
6. Fibers in Functional Abdominal Pain
7. Fibers in Irritable Bowel Syndrome
8. Fibers in Other Functional Gastrointestinal Disorders
9. Fibers in Inflammatory Bowel Disease (IBD)
10. Adverse Effects of Fibers
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Kranz, S.; Brauchla, M.; Slavin, J.L.; Miller, K.B. What do we know about dietary fiber intake in children and health? The effects of fiber intake on constipation, obesity, and diabetes in children. Adv. Nutr. 2012, 3, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Slavin, J. Fiber and prebiotics: Mechanisms and health benefits. Nutrients 2013, 5, 1417–1435. [Google Scholar] [CrossRef] [PubMed]
- Korczak, R.; Kamil, A.; Fleige, L.; Donovan, S.M.; Slavin, J.L. Dietary fiber and digestive health in children. Nutr. Rev. 2017, 75, 241–259. [Google Scholar] [CrossRef] [PubMed]
- Rajindrajith, S.; Devanarayana, N.M.; Benninga, M.A. Childhood constipation: Current status, challenges, and future perspectives. World J. Clin. Pediatr. 2022, 11, 385–404. [Google Scholar] [CrossRef]
- Augustin, L.S.A.; Aas, A.-M.; Astrup, A.; Atkinson, F.S.; Baer-Sinnott, S.; Barclay, A.W.; Brand-Miller, J.C.; Brighenti, F.; Bullo, M.; Buyken, A.E.; et al. Dietary fibre consensus from the International carbohydrate quality Consortium (ICQC). Nutrients 2020, 12, 2553. [Google Scholar] [CrossRef]
- Hojsak, I.; Benninga, M.A.; Hauser, B.; Kansu, A.; Kelly, V.B.; Stephen, A.M.; Morais Lopez, A.; Slavin, J.; Tuohy, K. Benefits of dietary fibre for children in health and disease. Arch. Dis. Child. 2022, 107, 973–979. [Google Scholar] [CrossRef]
- Burkitt, D.P. Some diseases characteristic of modern Western civilization. Br. Med. J. 1973, 1, 274–278. [Google Scholar] [CrossRef]
- Hipsley, E.H. Dietary “fibre” and pregnancy toxaemia. Br. Med. J. 1953, 2, 420–422. [Google Scholar] [CrossRef]
- Joint FAO/WHO Food Standards Programme, Secretariat of the CODEX Alimentarius Commission. CODEX Alimentarius (CODEX) Guidelines on Nutrition Labeling CAC/GL 2–1985 as Last Amended 2010; FAO: Rome, Italy, 2010. [Google Scholar]
- Stephen, A.M.; Champ, M.M.; Cloran, S.J.; Fleith, M.; van Lieshout, L.; Mejborn, H.; Burley, V.J. Dietary fibre in Europe: Current state of knowledge on definitions, sources, recommendations, intakes and relationships to health. Nutr. Res. Rev. 2017, 30, 149–190. [Google Scholar] [CrossRef]
- Scholz-Ahrens, K.E.; Ade, P.; Marten, B.; Weber, P.; Timm, W.; Asil, Y.; Glüer, C.-C.; Schrezenmeir, J. Prebiotics, probiotics, and synbiotics affect mineral absorption, bone mineral content, and bone structure. J. Nutr. 2007, 137, 838S–846S. [Google Scholar] [CrossRef]
- Whisner, C.M.; Castillo, L.F. Prebiotics, Bone and Mineral Metabolism. Calcif. Tissue Int. 2018, 102, 443–479. [Google Scholar] [CrossRef] [PubMed]
- Trumbo, P.; Schlicker, S.; Yates, A.A.; Poos, M.; Food and Nutrition Board of the Institute of Medicine; The National Academies. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein and amino acids. J. Am. Diet. Assoc. 2002, 102, 1621–1630. [Google Scholar] [CrossRef] [PubMed]
- Gibson, G.R.; Hutkins, R.; Sanders, M.E.; Prescott, S.L.; Reimer, R.A.; Salminen, S.J.; Scott, K.; Stanton, C.; Swanson, K.S.; Cani, P.D.; et al. Expert consensus document: The International Scientific Association for Probiotics and Prebiotics (ISAPP) consensus statement on the definition and scope of prebiotics. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 491–502. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.C.; Prosky, L.; DeVries, J.W. Determination of total, soluble and insoluble dietary fiber in foodsenzymatic-gravimetric method, MES-tris buffer: Collaborative study. JAOAC Int. 1992, 75, 395–416. [Google Scholar] [CrossRef]
- Dhingra, D.R.; Michael, M.; Rajput, H.; Patil, R.T. Dietary fibre in foods: A review. J. Food Sci. Technol. 2012, 49, 255–266. [Google Scholar] [CrossRef]
- Tosh, S.M. Review of human studies investigating the post-prandial blood-glucose lowering ability of oat and barley food products. Eur. J. Clin. Nutr. 2013, 67, 310–317. [Google Scholar] [CrossRef]
- Coppa, G.V.; Bruni, S.; Morelli, L.; Soldi, S.; Gabrielli, O. The first prebiotics in humans: Human milk oligosaccharides. J. Clin. Gastroenterol. 2004, 38, S80–S83. [Google Scholar] [CrossRef]
- Bode, L. Human milk oligosaccharides: Prebiotics and beyond. Nutr. Rev. 2009, 67, S183–S191. [Google Scholar] [CrossRef]
- Mei, Z.; Yuan, J.; Li, D. Biological activity of galacto-oligosaccharides: A review. Front. Microbiol. 2022, 13, 993052. [Google Scholar] [CrossRef]
- Kelly, G. Inulin-type p.rebiotics—A review: Part 1. Altern. Med. Rev. J. Clin. Ther. 2008, 13, 315–329. [Google Scholar]
- François, I.E.; Lescroart, O.; Veraverbeke, W.S.; Marzorati, M.; Possemiers, S.; Hamer, H.; Windey, K.; Welling, G.W.; Delcour, J.A.; Courtin, C.M.; et al. Effects of wheat bran extract containing arabinoxylan oligosaccharides on gastrointestinal parameters in healthy preadolescent children. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 647–653. [Google Scholar] [CrossRef] [PubMed]
- Moro, G.; Minoli, I.; Mosca, M.; Fanaro, S.; Jelinek, J.; Stahl, B. Dosage-related bifidogenic effects of galacto- and fructooligosaccharides in formula-fed term infants. J. Pediatr. Gastroenterol. Nutr. 2002, 34, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Boehm, G.; Lidestri, M.; Casetta, P.; Jelinek, J.; Negretti, F.; Stahl, B.; Marini, A. Supplementation of a bovine milk formula with an oligosaccharide mixture increases counts of faecal bifidobacteria in preterm infants. Arch. Dis. Childhood. Fetal Neonatal Ed. 2002, 86, F178–F181. [Google Scholar] [CrossRef] [PubMed]
- Knol, J.; Scholtens, P.; Kafka, C.; Steenbakkers, J.; Gro, S.; Helm, K.; Klarczyk, M.; Schöpfer, H.; Böckler, H.-M.; Wells, J. Colon microflora in infants fed formula with galacto- and fructo-oligosaccharides: More like breast-fed infants. J. Pediatr. Gastroenterol. Nutr. 2005, 40, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Horvath, A.; Dziechciarz, P.; Szajewska, H. Glucomannan for abdominal pain-related functional gastrointestinal disorders in children: A randomized trial. World J. Gastroenterol. 2013, 19, 3062–3068. [Google Scholar] [CrossRef]
- Tabbers, M.M.; DiLorenzo, C.; Berger, Y.M.; Faure, C.; Langendam, W.M.; Nurko, S.; Staiano, A.; Vandenplas, Y.; Benninga, A.M. Evaluation and treatment of functional constipation in infants and children: Evidence-based recommendations from ESPGHAN and NASPGHAN. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 258–274. [Google Scholar] [CrossRef] [PubMed]
- Axelrod, C.H.; Saps, M. The Role of Fiber in the Treatment of Functional Gastrointestinal Disorders in Children. Nutrients 2018, 10, 1650. [Google Scholar] [CrossRef]
- Lattimer, J.M.; Haub, M.D. Effects of dietary fiber and its components on metabolic health. Nutrients 2010, 2, 1266–1289. [Google Scholar] [CrossRef]
- Sabater-Molina, M.; Larque, E.; Torrella, F.; Zamora, S. Dietary fructooligosaccharides and potential benefits on health. J. Physiol. Biochem. 2009, 65, 315–328. [Google Scholar] [CrossRef]
- Niittynen, L.; Kajander, K.; Korpela, R. Galacto-oligosaccharides and bowel function. Scand. J. Food Nutr. 2007, 51, 62–66. [Google Scholar] [CrossRef]
- Gibson, G.R.; Beatty, E.R.; Wang, X.; Cummings, J.H. Selective stimulation of bifidobacteria in the human colon by oligofructose and inulin. Gastroenterology 1995, 108, 975–982. [Google Scholar] [CrossRef]
- Williams, C.L.; Bollella, M.; Wynder, E.L. A new recommendation for dietary fiber in childhood. Pediatrics. 1995, 96 Pt 2, 985–988. [Google Scholar] [CrossRef]
- Kamar, M.; Evans, C.; Hugh-Jones, S. Factors influencing adolescent whole grain intake: A theory-based qualitative study. Appetite 2016, 101, 125–133. [Google Scholar] [CrossRef]
- Larson, N.I.; Neumark-Sztainer, D.; Story, M.; Burgess-Champoux, T. Whole-grain intake correlates among adolescents and young adults: Findings from Project EAT. J. Am. Diet. Assoc. 2010, 110, 230–237. [Google Scholar] [CrossRef]
- Newlove-Delgado, T.V.; Martin, A.E.; Abbott, R.A.; Bethel, A.; Thompson-Coon, J.; Whear, R.; Logan, S. Dietary interventions for recurrent abdominal pain in childhood. Cochrane Database Syst. Rev. 2017, 3, CD010972. [Google Scholar] [CrossRef] [PubMed]
- Connor, F.; Salvatore, S.; D’Auria, E.; Baldassarre, M.E.; Acunzo, M.; Di Bella, G.; Farella, I.; Sestito, S.; Pensabene, L. Cows’ Milk Allergy-Associated Constipation: When to Look for It? A Narrative Review. Nutrients 2022, 14, 1317. [Google Scholar] [CrossRef] [PubMed]
- Maffei Leoni, H.V.; Vicentini, A.P. Prospective evaluation of dietary treatment in childhood constipation: High dietary fiber and wheat bran intake are associated with constipation amelioration. J. Pediatr. Gastroenterol. Nutr. 2011, 52, 55–59. [Google Scholar] [CrossRef]
- Southwell, B.R. Treatment of childhood constipation: A synthesis of systematic reviews and meta-analyses. Expert Rev. Gastroenterol. Hepatol. 2020, 14, 163–174. [Google Scholar] [CrossRef]
- Wegh, C.A.M.; Baaleman, D.F.; Tabbers, M.M.; Smidt, H.; Benninga, M.A. Nonpharmacologic Treatment for Children with Functional Constipation: A Systematic Review and Meta-analysis. J. Pediatr. 2022, 240, 136–149.e5. [Google Scholar] [CrossRef] [PubMed]
- Castillejo, G.; Bullo, M.; Anguera, A.; Escribano, J.; Salas-Salvado, J. A controlled, randomized, double-blind trial to evaluate the effect of a supplement of cocoa husk that is rich in dietary fiber on colonic transit in constipated pediatric patients. Pediatrics 2006, 118, e641–e648. [Google Scholar] [CrossRef]
- Loening-Baucke, V.; Miele, E.; Staiano, A. Fiber (glucomannan) is beneficial in the treatment of childhood constipation. Pediatrics 2004, 113, e259–e264. [Google Scholar] [CrossRef] [PubMed]
- Staiano, A.; Simeone, D.; Del Giudice, E.; Miele, E.; Tozzi, A.; Toraldo, C. Effect of the dietary fiber glucomannan on chronic constipation in neurologically impaired children. J. Pediatr. 2000, 136, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Chmielewska, A.; Horvath, A.; Dziechciarz, P.; Szajewska, H. Glucomannan is not effective for the treatment of functional constipation in children: A double-blind, placebo-controlled, randomized trial. Clin. Nutr. 2011, 30, 462–468. [Google Scholar] [CrossRef]
- Üstündağ, G.; Kuloğlu, Z.; Kirbaş, N.; Kansu, A. Can partially hydrolyzed guar gum be an alternative to lactulose in treatment of childhood constipation? Turk. J. Gastroenterol. Off. J. Turk. Soc. Gastroenterol. 2010, 21, 360–364. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarpur, S.A.; Naseri, M.; Esmaeilidooki, M.R.; Kamalinejad, M.; Bijani, A. The effect of cassia fistula emulsion on pediatric functional constipation in comparison with mineral oil: A randomized, clinical trial. Daru J. Fac. Pharm. Tehran Univ. Med. Sci. 2012, 20, 83. [Google Scholar] [CrossRef]
- Nimrouzi, M.; Zarshenas, M.M. Functional constipation in children: Non-pharmacological approach. J. Integr. Med. 2015, 25, 69–71. [Google Scholar] [CrossRef]
- Beleli, C.A.V.; Antonio, M.A.; dos Santos, R.; Pastore, G.M.; Lomazi, E.A. Effect of 4’galactooligosaccharide on constipation symptoms. J. Pediatr. 2015, 91, 567–573. [Google Scholar] [CrossRef]
- Kokke, F.T.; Scholtens, P.A.; Alles, M.S.; Decates, T.S.; Fiselier, T.J.; Tolboom, J.J.; Kimpen, J.L.; Benninga, M.A. A dietary fiber mixture versus lactulose in the treatment of childhood constipation: A double-blind randomized controlled trial. J. Pediatr. Gastroenterol. Nutr. 2008, 47, 592–597. [Google Scholar] [CrossRef]
- Quitadamo, P.; Coccorullo, P.; Giannetti, E.; Romano, C.; Chiaro, A.; Campanozzi, A.; Poli, E.; Cucchiara, S.; Di Nardo, G.; Staiano, A. A randomized, prospective, comparison study of a mixture of acacia fiber, psyllium fiber, and fructose vs. polyethylene glycol 3350 with electrolytes for the treatment of chronic functional constipation in childhood. J. Pediatr. 2012, 161, 710–715.e1. [Google Scholar] [CrossRef]
- Weber, T.K.; Toporovski, M.S.; Tahan, S.; Neufeld, C.B.; de Morais, M.B. Dietary fiber mixture in pediatric patients with controlled chronic constipation. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 297–302. [Google Scholar] [CrossRef]
- Piccoli de Mello, P.; Eifer, D.A.; Daniel de Mello, E. Use of fibers in childhood constipation treatment: Systematic review with meta-analysis. J. Pediatr. 2018, 94, 460–470. [Google Scholar] [CrossRef] [PubMed]
- Souza, D.D.S.; Tahan, S.; Weber, T.K.; Araujo-Filho, H.B.; De Morais, M.B. Randomized, Double-Blind, Placebo-Controlled Parallel Clinical Trial Assessing the Effect of Fructooligosaccharides in Infants with Constipation. Nutrients 2018, 10, 1602. [Google Scholar] [CrossRef] [PubMed]
- Toporovski, M.S.; de Morais, M.B.; Abuhab, A.; Crippa, J.M.A. Effect of Polydextrose/Fructooligosaccharide Mixture on Constipation Symptoms in Children Aged 4 to 8 Years. Nutrients 2021, 13, 1634. [Google Scholar] [CrossRef] [PubMed]
- Huo, J.; Wu, L.; Lv, J.; Cao, H.; Gao, Q. Effect of fruit intake on functional constipation: A systematic review and meta-analysis of randomized and crossover studies. Front. Nutr. 2022, 9, 1018502. [Google Scholar] [CrossRef]
- Bongers, M.E.; de Lorijn, F.; Reitsma, J.B.; Groeneweg, M.; Taminiau, J.A.; Benninga, M.A. The clinical effect of a new infant formula in term infants with constipation: A double-blind, randomized cross-over trial. Nutr. J. 2007, 6, 8. [Google Scholar] [CrossRef]
- Vivatvakin, B.; Mahayosnond, A.; Theamboonlers, A.; Steenhout, P.G.; Conus, N.J. Effect of a whey-predominant starter formula containing LCPUFAs and oligosaccharides (FOS/GOS) on gastrointestinal comfort in infants. Asia Pac. J. Clin. Nutr. 2010, 19, 473–480. [Google Scholar]
- Vandenplas, Y.; Benninga, M.; Broekaert, I.; Falconer, J.; Gottrand, F.; Guarino, A.; Lifschitz, C.; Lionetti, P.; Orel, R.; Papadopoulou, A.; et al. Functional gastro-intestinal disorder algorithms focus on early recognition, parental reassurance and nutritional strategies. Acta Paediatr. 2016, 105, 244–252. [Google Scholar] [CrossRef]
- Vandenplas, Y.; Gerlier, L.; Caekelbergh, K.; Nan-Study-Group; Possner, M. An Observational Real-Life Study with a New Infant Formula in Infants with Functional Gastro-Intestinal Disorders. Nutrients 2021, 13, 3336. [Google Scholar] [CrossRef]
- Ben, X.M.; Li, J.; Feng, Z.T.; Shi, S.Y.; Lu, Y.D.; Chen, R.; Zhou, X.Y. Low level of galacto-oligosaccharide in infant formula stimulates growth of intestinal Bifidobacteria and Lactobacilli. World J. Gastroenterol. 2008, 14, 6564–6568. [Google Scholar] [CrossRef]
- Salvatore, S. Nutritional options for infant constipation. Nutrition 2007, 23, 615–616. [Google Scholar] [CrossRef]
- Salvatore, S.; Abkari, A.; Cai, W.; Catto-Smith, A.; Cruchet, S.; Gottrand, F.; Hegar, B.; Lifschitz, C.; Ludwig, T.; Shah, N.; et al. Review shows that parental reassurance and nutritional advice help to optimise the management of functional gastrointestinal disorders in infants. Acta Paediatr. 2018, 107, 1512–1520. [Google Scholar] [CrossRef] [PubMed]
- Feldman, W.; McGrath, P.; Hodgson, C.; Ritter, H.; Shipman, R.T. The use of dietary fiber in the management of simple, childhood, idiopathic, recurrent, abdominal pain. Results in a prospective, double-blind, randomized, controlled trial. Am. J. Dis. Child. 1985, 139, 1216–1218. [Google Scholar] [CrossRef] [PubMed]
- Romano, C.; Comito, D.; Famiani, A.; Calamara, S.; Loddo, I. Partially hydrolyzed guar gum in pediatric functional abdominal pain. World J. Gastroenterol. 2013, 19, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Shulman, R.J.; Hollister, E.B.; Cain, K.; Czyzewski, D.I.; Self, M.M.; Weidler, E.M.; Devaraj, S.; Luna, R.A.; Versalovic, J.; Heitkemper, M. Psyllium Fiber Reduces Abdominal Pain in Children With Irritable Bowel Syndrome in a Randomized, Double-Blind Trial. Clin. Gastroenterol. Hepatol. 2017, 15, 712–719.e4. [Google Scholar] [CrossRef]
- de Bruijn, C.M.; Rexwinkel, R.; Gordon, M.; Sinopoulou, V.; Benninga, M.A.; Tabbers, M.M. Dietary interventions for functional abdominal pain disorders in children: A systematic review and meta-analysis. Expert Rev. Gastroenterol. Hepatol. 2022, 16, 359–371. [Google Scholar] [CrossRef]
- Grimaldi, R.; Gibson, G.R.; Vulevic, J.; Giallourou, N.; Castro-Mejia, J.L.; Hansen, L.H.; Gibson, E.L.; Nielsen, D.S.; Costabile, A. A prebiotic intervention study in children with autism spectrum disorders (ASDs). Microbiome 2018, 6, 133. [Google Scholar] [CrossRef]
- Basturk, A.; Artan, R.; Yilmaz, A. Efficacy of synbiotic, probiotic, and prebiotic treatments for irritable bowel syndrome in children: A randomized controlled trial. Turk. J. Gastroenterol. 2016, 27, 439–443. [Google Scholar] [CrossRef]
- Menon, J.; Thapa, B.R.; Kumari, R.; Puttaiah Kadyada, S.; Rana, S.; Lal, S.B. Efficacy of Oral Psyllium in Pediatric Irritable Bowel Syndrome: A Double-Blind Randomized Control Trial. J. Pediatr. Gastroenterol. Nutr. 2023, 76, 14–19. [Google Scholar] [CrossRef]
- Salvatore, S.; Savino, F.; Singendonk, M.; Tabbers, M.; Benninga, M.A.; Staiano, A.; Vandenplas, Y. Thickened infant formula: What to know. Nutrition 2018, 49, 51–56. [Google Scholar] [CrossRef]
- Savino, F.; Palumeri, E.; Castagno, E.; Cresi, F.; Dalmasso, P.; Cavallo, F. Reduction of crying episodes owing to infantile colic: A randomized controlled study on the efficacy of a new infant formula. Eur. J. Clin. Nutr. 2006, 60, 1304–1310. [Google Scholar] [CrossRef]
- Vandenplas, Y.; Ludwig, T.; Bouritius, H. The combination of scGOS/lcFOS with fermented infant formula reduces the incidence of colic in 4 week old infants. Arch. Dis. Child. 2014, 99 (Suppl. S2), A91–A92. [Google Scholar]
- Gordon, M.; Biagioli, E.; Sorrenti, M.; Lingua, C.; Moja, L.; Banks, S.S.; Ceratto, S.; Savino, F. Dietary modifications for infantile colic. Cochrane Database Syst. Rev. 2018, 10, CD011029. [Google Scholar] [CrossRef]
- Haskey, N.; Gold, S.L.; Faith, J.J.; Raman, M. To Fiber or Not to Fiber: The Swinging Pendulum of Fiber Supplementation in Patients with Inflammatory Bowel Disease. Nutrients 2023, 15, 1080. [Google Scholar] [CrossRef]
- Healey, G.R.; Celiberto, L.S.; Lee, S.M.; Jacobson, K. Fiber and Prebiotic Interventions in Pediatric Inflammatory Bowel Disease: What Role Does the Gut Microbiome Play? Nutrients 2020, 12, 3204. [Google Scholar] [CrossRef]
- Miele, E.; Shamir, R.; Aloi, M.; Assa, A.; Braegger, C.; Bronsky, J.; de Ridder, L.; Escher, J.C.; Hojsak, I.; Kolaček, S.; et al. Nutrition in Pediatric Inflammatory Bowel Disease: A Position Paper on Behalf of the Porto Inflammatory Bowel Disease Group of the European Society of Pediatric Gastroenterology, Hepatology and Nutrition. J. Pediatr. Gastroenterol. Nutr. 2018, 66, 687–708. [Google Scholar] [CrossRef]
- Peters, V.; Dijkstra, G.; Campmans-Kuijpers, M.J.E. Are all dietary fibers equal for patients with inflammatory bowel disease? A systematic review of randomized controlled trials. Nutr. Rev. 2022, 80, 1179–1193. [Google Scholar] [CrossRef]
- Giorgio, V.; Margiotta, G.; Stella, G.; Di Cicco, F.; Leoni, C.; Proli, F.; Zampino, G.; Gasbarrini, A.; Onesimo, R. Intestinal Permeability in Children with Functional Gastrointestinal Disorders: The Effects of Diet. Nutrients 2022, 14, 1578. [Google Scholar] [CrossRef]
- Turco, R.; Salvatore, S.; Miele, E.; Romano, C.; Marseglia, G.L.; Staiano, A. Does a low FODMAPsdiet reduce symptoms of functional abdominal pain disorders? A systematic review in adult and paediatric population, on behalf of Italian Society of Pediatrics. Ital. J. Pediatr. 2018, 44, 53. [Google Scholar] [CrossRef] [PubMed]
- Pensabene, L.; Salvatore, S.; Turco, R.; Tarsitano, F.; Concolino, D.; Baldassarre, M.E.; Borrelli, O.; Thapar, N.; Vandenplas, Y.; Staiano, A.; et al. Low FODMAPs diet for functional abdominal pain disorders in children: Critical review of current knowledge. J. Pediatr. 2019, 95, 642–656. [Google Scholar] [CrossRef]
- Boradyn, K.M.; Przybylowicz, K.E.; Jarocka-Cyrta, E. Low.FODMAP diet is not effective in children with functional abdominal pain: A randomized controlled trial. Ann. Nutr. Metab. 2020, 76, 334–344. [Google Scholar] [CrossRef]
- Nurko, S.; Benninga, M.A.; Solari, T.; Chumpitazi, B.P. Pediatric Aspects of Nutrition Interventions for Disorders of Gut-Brain Interaction. Am. J. Gastroenterol. 2022, 117, 995–1009. [Google Scholar] [CrossRef] [PubMed]
- Morreale, C.; Bresesti, I.; Bosi, A.; Baj, A.; Giaroni, C.; Agosti, M.; Salvatore, S. Microbiota and Pain: Save Your Gut Feeling. Cells 2022, 11, 971. [Google Scholar] [CrossRef] [PubMed]
- Hambidge, K.M. Micronutrient bioavailability: Dietary Reference Intakes and a future perspective. Am. J. Clin. Nutr. 2010, 91, 1430S–1432S. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| A. Content of fibers in common fruits, vegetables and nuts | |||||||
FOOD | Total Fibers g/100 g | Soluble Fiber g/100 g | Insoluble Fiber g/100 g | FOOD | Total Fibers g/100 g | Soluble Fiber g/100 g | Insoluble Fiber g/100 g |
| FRUITS | VEGETABLES | ||||||
| Apple (with skin) | 2.6 | 0.73 | 1.84 | Artichoke (frozen) | 5.0 | 3.04 | 1.93 |
| Apple (without skin) | 2.0 | 1.55 | 0.44 | Asparagus | 3.5 | 2.6 | 0.9 |
| Apricot | 1.5 | 0.71 | 0.83 | Aubergine | 2.5 | 0.6 | 1.9 |
| Avocado | 6.7 | 4.7 | 2.0 | Beetroot | 7.8 | 2.4 | 5.4 |
| Banana | 1.8 | 0.62 | 1.19 | Broccoli | 2.4 | 0 | 2.4 |
| Blueberry (bilberry) | 3.3 | 0.7 | 2.6 | Brussels sprouts | 4.4 | 2.8 | 1.6 |
| Cherry | 1.3 | 0.49 | 0.8 | Cabbage (green) | 2.6 | 0.32 | 2.26 |
| Coconut | 9 | 0.5 | 8.5 | Cabbage (red) | 2.5 | 1.4 | 1.1 |
| Grape (black) | 1.6 | 0.25 | 1.33 | Cabbage (savoy) | 2.9 | 0.35 | 2.53 |
| Grape (white) | 1.4 | 0.16 | 1.2 | Carrot | 3.1 | 0.41 | 2.7 |
| Grapefruit | 1.6 | 0.54 | 1.06 | Cauliflower | 1.9 | 1.4 | 0.5 |
| Kiwi | 2.2 | 0.78 | 1.43 | Celeriac | 2.9 | 0.9 | 2.0 |
| Lemon | 2.8 | 1.6 | 1.2 | Celery | 1.6 | 0.18 | 1.41 |
| Mandarin | 1.9 | 0.9 | 1.0 | Cucumber | 0.8 | 0.21 | 0.54 |
| Mango | 2.0 | 1.0 | 1.0 | Eggplant | 6.6 | 1.3 | 5.3 |
| Melon (cantaloupe) | 0.8 | 0.3 | 0.5 | Fennel | 2.2 | 0.25 | 1.97 |
| Melon (honeydew) | 0.8 | 0.4 | 0.4 | Green beans | 2.9 | 0.71 | 2.14 |
| Olive (in oil) | 4.4 | 1.8 | 2.6 | Italian chicory | 3.0 | 0.59 | 2.37 |
| Orange (generic) | 1.6 | 0.6 | 1.0 | Lettuce | 1.5 | 0.13 | 1.33 |
| Peach (with skin) | 1.9 | 0.78 | 1.19 | Mushrooms (boletus) | 1.9 | 0.1 | 1.8 |
| Peach (without skin) | 1.6 | 0.87 | 0.71 | Mushrooms (field) | 2.3 | 0.11 | 2.14 |
| Pear (with skin) | 4.3 | 4.0 | 0.3 | Mushrooms (pleurotes) | 2.4 | 0.25 | 2.15 |
| Pear (without skin) | 3.8 | 1.29 | 2.56 | Onion | 1.0 | 0.16 | 0.88 |
| Pineapple | 1.0 | 0.15 | 0.83 | Pepper | 1.9 | 0.43 | 1.47 |
| Plum (red) | 1.6 | 0.67 | 0.91 | Potato (boiled—with skin) | 1.6 | 0.71 | 0.85 |
| Plum (yellow) | 1.4 | 0.57 | 0.83 | Potato (raw—with skin) | 1.8 | 0.8 | 0.96 |
| Raspberry | 3.7 | 0.4 | 3.3 | Potato (raw) | 1.3 | 0.3 | 1.0 |
| Strawberry | 1.6 | 0.45 | 1.13 | Pumpkin | 2.0 | 0.6 | 1.4 |
| Tangerine | 1.7 | 0.67 | 1.03 | Radish | 1.3 | 0.07 | 1.23 |
| Watermelon | 0.2 | 0.02 | 0.2 | Spinach (fresh—raw) | 2.6 | 0.5 | 2.1 |
| NUTS | Spinach (frozen) | 1.3 | 0.4 | 0.9 | |||
| Almond | 11.2 | 1.1 | 10.1 | Sweetcorn (boiled) | 3.5 | 0.3 | 3.2 |
| Brazil Nut | 6.5 | 5.1 | 1.4 | Sweetcorn (kernels) | 3.7 | 0.3 | 3.4 |
| Cashew Nut | 3.5 | 1.6 | 1.9 | Tomato (canned) | 1.9 | 1.7 | 0.2 |
| Hazelnut (dried) | 17.5 | 11.8 | 5.7 | Tomato (fresh) | 1.0 | 0.24 | 0.77 |
| Peanut (roasted) | 10.9 | 1 | 9.9 | Tomato (puree) | 1.0 | 0.6 | 0.4 |
| Pecan nuts | 9.4 | 0.3 | 9.1 | Turnip | 2.6 | 0.29 | 2.32 |
| Pine nuts | 4.6 | 0.8 | 3.8 | ||||
| Walnuts | 6.7 | 1.7 | 5.0 | ||||
| Chestnut | 4.7 | 0.4 | 4.3 | ||||
| B. Content of fibers in grains and legumes | |||||||
FOOD | Total Fibers g/100 g | Soluble Fiber g/100 g | Insoluble Fiber g/100 g | FOOD | Total Fibers g/100 g | Soluble Fiber g/100 g | Insoluble Fiber g/100 g |
| GRAINS | GRAINS | ||||||
| Barley (pearled) | 9.2 | 4.41 | 4.83 | Rice (brown) | 4.0 | 0.1 | 3.9 |
| Biscuits (for children) | 1.3 | 0.3 | 1.0 | Rice (generic) | 1.3 | 0.3 | 1.0 |
| Biscuits (dried) | 2.6 | 1.32 | 1.32 | Rice (white—long grain—parboiled) | 1.7 | 0.7 | 1.0 |
| Biscuits (whole wheat) | 6.0 | 0.94 | 5.07 | Rice cake | 7.4 | 1.1 | 6.3 |
| Bread (flour type 00) | 3.1 | 1.46 | 1.63 | Rusks | 3.5 | 0.8 | 2.7 |
| Bread (whole wheat) | 6.5 | 1.15 | 5.36 | Rusks (whole wheat) | 4.3 | 0.8 | 3.5 |
| Corn flakes | 2.7 | 1.0 | 1.7 | Semolina | 3.5 | 0.9 | 2.6 |
| Corn flakes (sugar coated) | 1.8 | 0.7 | 1.1 | Spelt | 6.5 | 0.96 | 5.5 |
| Cornflour | 3.1 | 0.35 | 2.76 | Maize | 12.8 | 1.6 | 11.2 |
| Cornstarch | 0 | 0 | 0 | Quality Protein Maize (QPM) | 14.9 | 1.1 | 13.8 |
| Couscous | 5.0 | 2.4 | 2.6 | LEGUMES | |||
| Crackers (salted) | 2.7 | 0.7 | 2.0 | Beans (cannellini—cooked) | 7.8 | 1.05 | 6.78 |
| Crackers (wholewheat) | 10.0 | 1.2 | 8.8 | Beans (cannellini—dry weight) | 17.6 | 2.3 | 15.25 |
| Egg pasta (fresh) (f) | 3.6 | 1.7 | 1.9 | Beans (generic—cooked) | 7.8 | 1.05 | 6.78 |
| Flour (wheat type 0) | 2.9 | 1.07 | 1.86 | Beans (generic—dry weight) | 17.5 | 2.34 | 15.14 |
| Flour (wheat type 00) | 2.2 | 0.84 | 1.41 | Beans (pinto—cooked) | 6.9 | 0.81 | 6.28 |
| Flour (wheat whole wheat) | 8.4 | 1.92 | 6.51 | Beans (pinto—dry weight) | 17.3 | 1.54 | 15.71 |
| Millet (flour) | 3.2 | 0.6 | 2.6 | Chickpeas (dry weight) | 13.6 | 1.13 | 12.45 |
| Muesli | 8.7 | 3.3 | 5.4 | Chickpeas (cooked) | 5.8 | 0.47 | 5.29 |
| Oat flakes | 8.3 | 3.3 | 4.99 | Fava beans (shelled—cooked) | 3.0 | 0.24 | 2.89 |
| Oat flour | 9.0 | 4.4 | 4.6 | Fava beans (shelled—dry weight) | 7.0 | 0.36 | 6.64 |
| Pasta (durum wheat flour) | 1.7 | 0.72 | 0.98 | Lentils (cooked) | 8.3 | 0.53 | 7.74 |
| Pasta (whole wheat, durum wheat) | 7.1 | 1.53 | 5.57 | Lentils (dry weight) | 13.8 | 0.92 | 12.91 |
| Quinoa (cooked) | 2.8 | 2.8 | 0 | Peas (cooked) | 6.4 | 0.64 | 5.73 |
| Rice (white) | 2.3 | 0.2 | 2.1 | Peas (frozen) | 3.5 | 0.3 | 3.2 |
| Rice (whole grain) | 7.4 | 1.1 | 6.3 | Soybeans (dry weight) | 15.7 | 6.4 | 9.3 |
| FIBER | TYPE | SOURCE | COMPONENTS | PREBIOTIC EFFECT | Reference |
|---|---|---|---|---|---|
| Glucomannan | Soluble | Japanese konjac plant | Polysaccharide of 1,4-d-glucose and d-mannose | YES | [26] |
| Acacia/Arabic gum | Soluble | Acacia trees (Leguminosae) | Anionic polysaccharide: l-arabinose, l-rhamnose, and d-glucuronic acid and 1,3-linked β-d-galactopyranosyl units | YES | [2,3] |
| Arabinoxylan | Soluble | Whole grains (endosperm and bran) | Hemicellulose, polymers of two pentose sugars: arabinose and 1,4-linked xylose units | YES | [3,29] |
| Beta-glucan | Soluble | endosperm of barley and oats | Glucose polysaccharide with Beta (1–4) (1–3) linkages ± branch points | YES | [3,12,17] |
| Bran | Soluble (oat bran); insoluble (wheat, rice, corn, bran) | outermost layer cereal grains | Non-starch polysaccharides, cellulose, hemicellulose, lignin | YES, as source of arabinoxylan-oligosaccharides (i.e., wheat bran) | [2,3] |
| Fructo-oligosaccharides (FOSs) | Soluble | many plants (i.e., garlic, chicory, onion, artichoke, and banana | Linear chains of fructose units linked by beta bonds. The number of fructose units ranges from 2 to 60 and often ends in a terminal glucose unit. | YES (>>Bifidobacteria) | [3,23,30] |
| Galactooligosaccharides (GOS) | Soluble | Dairy products, beans, certain root vegetables | They are produced commercially from lactose by β-galactosidase | YES | [2,20,23,24,31] |
| Inulin | Soluble | Chicory roots, artichokes, bananas, onion, garlic, and wheat | Fructose polymers (ranging from 2 to >60) that are linked by beta bonds and that terminate with a glucose unit | YES | [29,32] |
| Partially hydrolyzed guar gum | Soluble | Extracted from guar beans from the Cyamopsis tetragonolobus plant | High-molecular-weight polysaccharide: galactomannans of a linear chain of (1-4)-linked β-d-mannopyranosyl units with (1-6)-linked α-d-galactopyranosyl residues as side chains. The mannose: galactose ratio is approximately 2:1. | YES | [2,3,10] |
| Resistant starch | Soluble | Grains, starch or chemically modified starch | High-molecular carbohydrate: linear (amylose) and branched (amylopectin) chains of glucose residues. RS1 is a physically protected form of starch found in whole or partly milled grains; RS2 is present as raw granules; RS3 is retrograded starch, composed of crystallized starches produced via unique cooking and cooling processes; and RS4 is a chemically modified starch. | YES | [2,3,29] |
| Dextrin | Soluble | Any starch source (corn, wheat, potatoes). There are as follows: white dextrin, yellow or canary dextrin, or British gums | Saccharide polymer linked primarily by alpha-(1 --> 4) d-glucose units and prepared by partial hydrolysis of starch | YES | [2] |
| Psyllium | Soluble | Seeds of the plant genus Plantago | Highly branched arabinoxylan | YES | [2] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salvatore, S.; Battigaglia, M.S.; Murone, E.; Dozio, E.; Pensabene, L.; Agosti, M. Dietary Fibers in Healthy Children and in Pediatric Gastrointestinal Disorders: A Practical Guide. Nutrients 2023, 15, 2208. https://doi.org/10.3390/nu15092208
Salvatore S, Battigaglia MS, Murone E, Dozio E, Pensabene L, Agosti M. Dietary Fibers in Healthy Children and in Pediatric Gastrointestinal Disorders: A Practical Guide. Nutrients. 2023; 15(9):2208. https://doi.org/10.3390/nu15092208
Chicago/Turabian StyleSalvatore, Silvia, Maria Serena Battigaglia, Elena Murone, Eugenia Dozio, Licia Pensabene, and Massimo Agosti. 2023. "Dietary Fibers in Healthy Children and in Pediatric Gastrointestinal Disorders: A Practical Guide" Nutrients 15, no. 9: 2208. https://doi.org/10.3390/nu15092208