

Citrulline, Intestinal Fatty Acid-Binding Protein and the Acute Gastrointestinal Injury Score as Predictors of Gastrointestinal Failure in Patients with Sepsis and Septic Shock
 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Data Collection
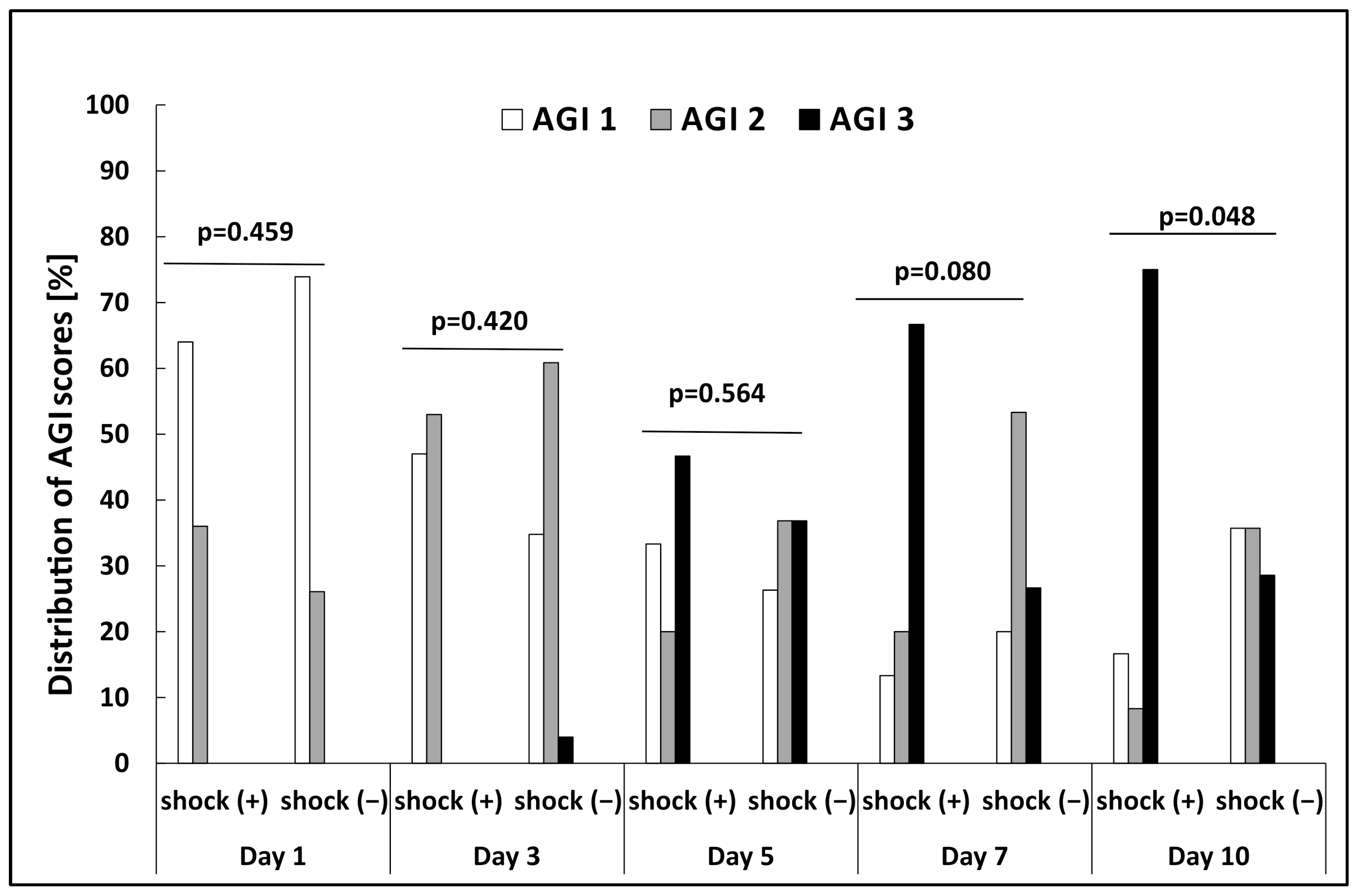
- AGI score I: (the patient is at risk of developing GI dysfunction) the function of the digestive tract is partially impaired; GI symptoms are associated with a known cause and transient;
- AGI score II: (the patient developed GI dysfunction) the GI tract is unable to function properly to meet patient’s needs for nutrients and fluids;
- AGI score III: (the patient developed GI failure) severe GI damage which does not respond to normal treatment and the general condition of the patient is not improving;
- AGI score IV: (the patient developed GI failure with severe impact on distant organ function) persistent, long-term damage, resulting in worsening of multi-organ dysfunction syndrome or shock; life-threatening and requiring surgical intervention.
2.2. Control Group
2.3. Sample Collection and Measurement of the Biomarkers
2.4. Statistical Analysis
3. Results
3.1. Levels of Citrulline and I-FABP in Septic Patients with and without Shock
3.2. The Relationship between AGI Score and Biomarker Levels
3.3. Biomarker Levels as a Tool for Predicting the Development of GI Failure
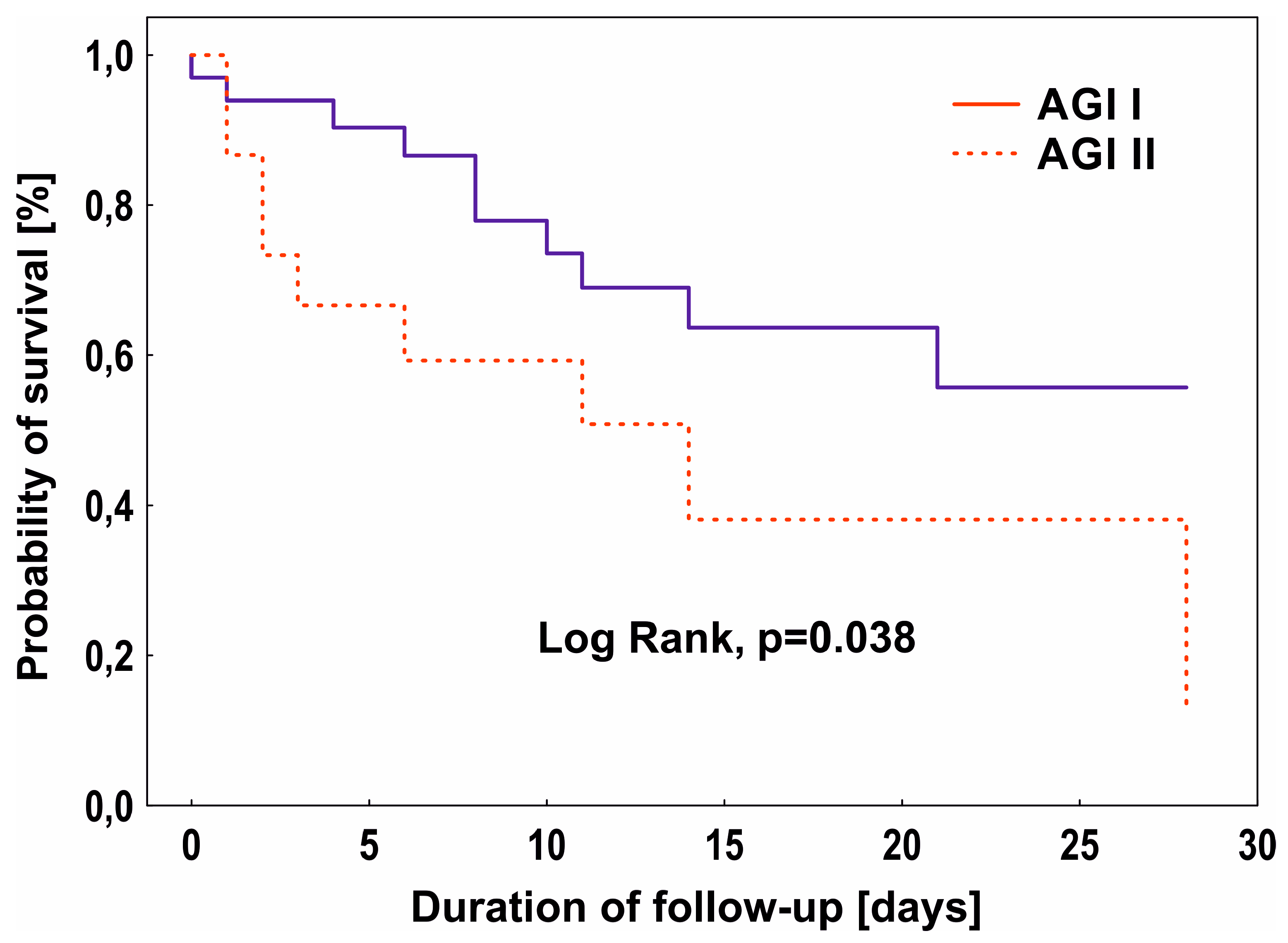
3.4. AGI Score, Biomarkers, and 28-Day Mortality
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Singer, M.; Deutschman, C.S.; Seymour, C.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Hu, B.; Sun, R.; Wu, A.; Ni, Y.; Liu, J.; Guo, F.; Ying, L.; Ge, G.; Ding, A.; Shi, Y.; et al. Severity of Acute Gastrointestinal Injury Grade Is a Predictor of All-Cause Mortality in Critically Ill Patients: A Multicenter, Prospective, Observational Study. Crit. Care 2017, 21, 188. [Google Scholar] [CrossRef] [PubMed]
- Adelman, M.W.; Woodworth, M.H.; Langelier, C.; Busch, L.M.; Kempker, J.A.; Kraft, C.S.; Kraft, C.S.; Martin, G.S.; Martin, G.S. The Gut Microbiome’s Role in the Development, Maintenance, and Outcomes of Sepsis. Crit. Care 2020, 24, 278. [Google Scholar] [CrossRef] [PubMed]
- Fay, K.T.; Klingensmith, N.J.; Chen, C.W.; Zhang, W.; Sun, Y.; Morrow, K.N.; Liang, Z.; Burd, E.M.; Ford, M.L.; Coopersmith, C.M. The Gut Microbiome Alters Immunophenotype and Survival from Sepsis. FASEB J. 2019, 33, 11258–11269. [Google Scholar] [CrossRef] [PubMed]
- Adamik, B.; Gozdzik, W.; Jakubczyk, D.; Welna, M.; Kübler, A. Coagulation Abnormalities Identified by Thromboelastometry in Patients with Severe Sepsis: The Relationship to Endotoxemia and Mortality. Blood Coagul. Fibrinolysis 2017, 28, 163–170. [Google Scholar] [CrossRef]
- Bray, M.A.; Sartain, S.E.; Gollamudi, J.; Rumbaut, R.E. Microvascular Thrombosis: Experimental and Clinical Implications. Transl. Res. 2020, 225, 105–130. [Google Scholar] [CrossRef]
- Dempfle, C.E. Coagulopathy of Sepsis. Thromb. Haemost. 2004, 91, 213–224. [Google Scholar] [CrossRef]
- de Backer, D.; Creteur, J.; Preiser, J.C.; Dubois, M.J.; Vincent, J.L. Microvascular Blood Flow Is Altered in Patients with Sepsis. Am. J. Respir. Crit. Care Med. 2002, 166, 98–104. [Google Scholar] [CrossRef]
- Ellis, C.G.; Jagger, J.; Sharpe, M. The Microcirculation as a Functional System. Crit. Care 2005, 9, S3–S8. [Google Scholar] [CrossRef]
- Altshuler, A.E.; Lamadrid, I.; Li, D.; Ma, S.R.; Kurre, L.; Schmid-Schönbein, G.W.; Penn, A.H. Transmural Intestinal Wall Permeability in Severe Ischemia after Enteral Protease Inhibition. PLoS ONE 2014, 9, e96655. [Google Scholar] [CrossRef]
- Jiang, L.-Y.; Zhang, M.; Zhou, T.-E.; Yang, Z.-F.; Wen, L.-Q.; Chang, J.-X. Changes of the Immunological Barrier of Intestinal Mucosa in Rats with Sepsis. World J. Emerg. Med. 2010, 1, 138–143. [Google Scholar] [PubMed]
- Reintam Blaser, A.; Preiser, J.C.; Fruhwald, S.; Wilmer, A.; Wernerman, J.; Benstoem, C.; Casaer, M.P.; Starkopf, J.; van Zanten, A.; Rooyackers, O.; et al. Gastrointestinal Dysfunction in the Critically Ill: A Systematic Scoping Review and Research Agenda Proposed by the Section of Metabolism, Endocrinology and Nutrition of the European Society of Intensive Care Medicine. Crit. Care 2020, 24, 224. [Google Scholar] [CrossRef]
- Doudakmanis, C.; Bouliaris, K.; Kolla, C.; Efthimiou, M.; Koukoulis, G.D. Bacterial Translocation in Patients Undergoing Major Gastrointestinal Surgery and Its Role in Postoperative Sepsis. World J. Gastrointest. Pathophysiol. 2021, 12, 106–114. [Google Scholar] [CrossRef]
- Crapser, J.; Ritzel, R.; Verma, R.; Venna, V.R.; Liu, F.; Chauhan, A.; Koellhoffer, E.; Patel, A.; Ricker, A.; Maas, K.; et al. Ischemic Stroke Induces Gut Permeability and Enhances Bacterial Translocation Leading to Sepsis in Aged Mice. Aging 2016, 8, 1049–1063. [Google Scholar] [CrossRef]
- Blaser, A.R.; Malbrain, M.L.N.G.; Starkopf, J.; Fruhwald, S.; Jakob, S.M.; de Waele, J.; Braun, J.P.; Poeze, M.; Spies, C. Gastrointestinal Function in Intensive Care Patients: Terminology, Definitions and Management. Recommendations of the ESICM Working Group on Abdominal Problems. Intensive Care Med. 2012, 38, 384–394. [Google Scholar] [CrossRef]
- Reintam Blaser, A.; Padar, M.; Mändul, M.; Elke, G.; Engel, C.; Fischer, K.; Giabicani, M.; Gold, T.; Hess, B.; Hiesmayr, M.; et al. Development of the Gastrointestinal Dysfunction Score (GIDS) for Critically Ill Patients—A Prospective Multicenter Observational Study (ISOFA Study). Clin. Nutr. 2021, 40, 4932–4940. [Google Scholar] [CrossRef]
- Curis, E.; Nicolis, I.; Moinard, C.; Osowska, S.; Zerrouk, N.; Bénazeth, S.; Cynober, L. Almost All about Citrulline in Mammals. Amino Acids 2005, 29, 177–205. [Google Scholar] [CrossRef]
- Noordally, S.O.; Sohawon, S.; Semlali, H.; Michely, D.; Devriendt, J.; Gottignies, P. Is There a Correlation between Circulating Levels of Citrulline and Intestinal Dysfunction in the Critically Ill? Nutr. Clin. Pract. 2012, 27, 527–532. [Google Scholar] [CrossRef] [PubMed]
- Fagoni, N.; Piva, S.; Marino, R.; Chiarini, G.; Ferrari, D.; Grespi, E.; Bertuetti, R.; Barbieri, S.; Latronico, N.; Rasulo, F. The IN-PANCIA Study: Clinical Evaluation of Gastrointestinal Dysfunction and Failure, Multiple Organ Failure, and Levels of Citrulline in Critically Ill Patients. J. Intensive Care Med. 2020, 35, 279–283. [Google Scholar] [CrossRef]
- Crenn, P.; Neveux, N.; Chevret, S.; Jaffray, P.; Cynober, L.; Melchior, J.C.; Annane, D. Plasma L-Citrulline Concentrations and Its Relationship with Inflammation at the Onset of Septic Shock: A Pilot Study. J. Crit. Care 2014, 29, 315.e1–315.e6. [Google Scholar] [CrossRef] [PubMed]
- Piton, G.; Manzon, C.; Monnet, E.; Cypriani, B.; Barbot, O.; Navellou, J.C.; Carbonnel, F.; Capellier, G. Plasma Citrulline Kinetics and Prognostic Value in Critically Ill Patients. Intensive Care Med. 2010, 36, 702–706. [Google Scholar] [CrossRef] [PubMed]
- Luiking, Y.C.; Poeze, M.; Ramsay, G.; Deutz, N.E.P. Reduced Citrulline Production in Sepsis Is Related to Diminished de Novo Arginine and Nitric Oxide Production. Am. J. Clin. Nutr. 2009, 89, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Kanda, T.; Fujii, H.; Tani, T.; Murakami, H.; Suda, T.; Sakai, Y.; Ono, T.; Hatakeyama, K. Intestinal Fatty Acid-Binding Protein Is a Useful Diagnostic Marker for Mesenteric Infarction in Humans. Gastroenterology 1996, 110, 339–343. [Google Scholar] [CrossRef]
- Derikx, J.P.M.; Poeze, M.; van Bijnen, A.A.; Buurman, W.A.; Heineman, E. Evidence for Intestinal and Liver Epithelial Cell Injury in the Early Phase of Sepsis. Shock 2007, 28, 544–548. [Google Scholar] [CrossRef] [PubMed]
- Padar, M.; Starkopf, J.; Starkopf, L.; Forbes, A.; Hiesmayr, M.; Jakob, S.M.; Rooijackers, O.; Wernerman, J.; Ojavee, S.E.; Reintam Blaser, A. Enteral Nutrition and Dynamics of Citrulline and Intestinal Fatty Acid-Binding Protein in Adult ICU Patients. Clin. Nutr. ESPEN 2021, 45, 322–332. [Google Scholar] [CrossRef] [PubMed]
- Sekino, M.; Funaoka, H.; Sato, S.; Okada, K.; Inoue, H.; Yano, R.; Matsumoto, S.; Ichinomiya, T.; Higashijima, U.; Matsumoto, S.; et al. Intestinal Fatty Acid-Binding Protein Level as a Predictor of 28-Day Mortality and Bowel Ischemia in Patients with Septic Shock: A Preliminary Study. J. Crit. Care 2017, 42, 92–100. [Google Scholar] [CrossRef]
- Tyszko, M.; Lipińska-Gediga, M.; Lemańska-Perek, A.; Kobylińska, K.; Gozdzik, W.; Adamik, B. Intestinal Fatty Acid Binding Protein (I-FABP) as a Prognostic Marker in Critically Ill COVID-19 Patients. Pathogens 2022, 11, 1526. [Google Scholar] [CrossRef]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017, 43, 304–377. [Google Scholar] [CrossRef]
- Piton, G.; Capellier, G. Biomarkers of Gut Barrier Failure in the ICU. Curr. Opin. Crit. Care 2016, 22, 152–160. [Google Scholar] [CrossRef]
- Jenkins, B.; Calder, P.C.; Marino, L.V. A Scoping Review Considering Potential Biomarkers or Functional Measures of Gastrointestinal Dysfunction and Enteral Feeding Intolerance in Critically Ill Adults. Clin. Nutr. ESPEN 2022, 52, 331–339. [Google Scholar] [CrossRef]
- Li, H.; Chen, Y.; Huo, F.; Wang, Y.; Zhang, D. Association between Acute Gastrointestinal Injury and Biomarkers of Intestinal Barrier Function in Critically Ill Patients. BMC Gastroenterol. 2017, 17, 45. [Google Scholar] [CrossRef] [PubMed]
- Pelsers, M.M.A.L.; Namiot, Z.; Kisielewski, W.; Namiot, A.; Januszkiewicz, M.; Hermens, W.T.; Glatz, J.F.C. Intestinal-Type and Liver-Type Fatty Acid-Binding Protein in the Intestine. Tissue Distribution and Clinical Utility. Clin. Biochem. 2003, 36, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Lieberman, J.M.; Sacchettini, J.; Marks, C.; Marks, W.H. Human Intestinal Fatty Acid Binding Protein: Report of an Assay with Studies in Normal Volunteers and Intestinal Ischemia. Surgery 1997, 121, 335–342. [Google Scholar] [CrossRef]
- Heida, F.H.; Hulscher, J.B.F.; Schurink, M.; Timmer, A.; Kooi, E.M.W.; Bos, A.F.; Bruggink, J.L.M.; Kasper, D.C.; Pones, M.; Benkoe, T. Intestinal Fatty Acid-Binding Protein Levels in Necrotizing Enterocolitis Correlate with Extent of Necrotic Bowel: Results from a Multicenter Study. J. Pediatr. Surg. 2015, 50, 1115–1118. [Google Scholar] [CrossRef] [PubMed]
- Kanda, T.; Tsukahara, A.; Ueki, K.; Sakai, Y.; Tani, T.; Nishimura, A.; Yamazaki, T.; Tamiya, Y.; Tada, T.; Hirota, M.; et al. Diagnosis of Ischemic Small Bowel Disease by Measurement of Serum Intestinal Fatty Acid-Binding Protein in Patients with Acute Abdomen: A Multicenter, Observer-Blinded Validation Study. J. Gastroenterol. 2011, 46, 492–500. [Google Scholar] [CrossRef] [PubMed]
- Voth, M.; Duchene, M.; Auner, B.; Lustenberger, T.; Relja, B.; Marzi, I. I-FABP Is a Novel Marker for the Detection of Intestinal Injury in Severely Injured Trauma Patients. World J. Surg. 2017, 41, 3120–3127. [Google Scholar] [CrossRef]
- Crenn, P.; Coudray-Lucas, C.; Thuillier, F.; Cynober, L.; Messing, B. Postabsorptive Plasma Citrulline Concentration Is a Marker of Absorptive Enterocyte Mass and Intestinal Failure in Humans. Gastroenterology 2000, 119, 1496–1505. [Google Scholar] [CrossRef]
- Elkhatib, I.; Buchman, A.L. Plasma Citrulline Concentration as a Marker for Disease Activity in Patients With Crohn’s Disease. J. Clin. Gastroenterol. 2012, 46, 308–310. [Google Scholar] [CrossRef]
- Shen, L.J.; Guan, Y.Y.; Wu, X.P.; Wang, Q.; Wang, L.; Xiao, T.; Wu, H.R.; Wang, J.G. Serum Citrulline as a Diagnostic Marker of Sepsis-Induced Intestinal Dysfunction. Clin. Res. Hepatol. Gastroenterol. 2015, 39, 230–236. [Google Scholar] [CrossRef]
- Blasco-Alonso, J.; Sánchezyáñez, P.; Rosa Camacho, V.; Camacho Alonso, J.M.; Yahyaoui Macías, R.; Gil-Gómez, R.; Milano Manso, G. Citrulline and Arginine Kinetics and Its Value as a Prognostic Factor in Pediatric Critically Ill Patients. An. Pediatría 2015, 83, 257–263. [Google Scholar] [CrossRef]
- Sarikaya, M.; Ergül, B.; Doğan, Z.; Filik, L.; Can, M.; Arslan, L. Intestinal Fatty Acid Binding Protein (I-FABP) as a Promising Test for Crohn’s Disease: A Preliminary Study. Clin. Lab. 2015, 61, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Ockner, R.K.; Manning, J.A. Fatty Acid Binding Protein in Small Intestine. Identification, Isolation, and Evidence for Its Role in Cellular Fatty Acid Transport. J. Clin. Investig. 1974, 54, 326–338. [Google Scholar] [CrossRef]
- Pelsers, M.M.A.L.; Hermens, W.T.; Glatz, J.F.C. Fatty Acid-Binding Proteins as Plasma Markers of Tissue Injury. Clin. Chim. Acta 2005, 352, 15–35. [Google Scholar] [CrossRef]
- de Haan, J.J.; Lubbers, T.; Derikx, J.P.; Relja, B.; Henrich, D.; Greve, J.W.; Marzi, I.; Buurman, W.A. Rapid Development of Intestinal Cell Damage Following Severe Trauma: A Prospective Observational Cohort Study. Crit. Care 2009, 13, R86. [Google Scholar] [CrossRef] [PubMed]
- Piton, G.; Belon, F.; Cypriani, B.; Regnard, J.; Puyraveau, M.; Manzon, C.; Navellou, J.C.; Capellier, G. Enterocyte Damage in Critically Ill Patients Is Associated with Shock Condition and 28-Day Mortality. Crit. Care Med. 2013, 41, 2169–2176. [Google Scholar] [CrossRef]
- Zhang, D.; Li, H.; Li, Y.; Qu, L. Gut Rest Strategy and Trophic Feeding in the Acute Phase of Critical Illness with Acute Gastrointestinal Injury. Nutr. Res. Rev. 2019, 32, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.K.; Liu, Y.; Zou, L.; Zhang, W.H.; Wang, Y.; Kan, X.H.; Chen, J.D.; Li, J.J.; Shi, Q.K.; Yuan, S.T. Acute Gastrointestinal Injury in Critically Ill Patients with COVID-19 in Wuhan, China. World J. Gastroenterol. 2020, 26, 6087–6097. [Google Scholar] [CrossRef]
- Drakos, P.; Volteas, P.; Cleri, N.A.; Alkadaa, L.N.; Asencio, A.A.; Oganov, A.; Pryor, A.; Talamini, M.; Rubano, J.; Bannazadeh, M.; et al. Acute Gastrointestinal Injury and Feeding Intolerance as Prognostic Factors in Critically Ill COVID-19 Patients. J. Gastrointest. Surg. 2022, 26, 181–190. [Google Scholar] [CrossRef]
- Ahn, J.W.; Scallan Walter, E.; White, A.E.; McQueen, R.B.; Hoffmann, S. Identifying Sepsis From Foodborne Hospitalization: Incidence and Hospitalization Cost by Pathogen. Clin. Infect. Dis. 2022, 75, 857–866. [Google Scholar] [CrossRef]
- Zhang, Z.; Li, Q.; Jiang, L.; Xie, B.; Ji, X.; Lu, J.; Jiang, R.; Lei, S.; Mao, S.; Ying, L.; et al. Effectiveness of Enteral Feeding Protocol on Clinical Outcomes in Critically Ill Patients: A Study Protocol for before-and-after Design. Ann. Transl. Med. 2016, 4, 308. [Google Scholar] [CrossRef]
- Teng, J.; Xiang, L.; Long, H.; Gao, C.; Lei, L.; Zhang, Y. The Serum Citrulline and D-Lactate Are Associated with Gastrointestinal Dysfunction and Failure in Critically Ill Patients. Int. J. Gen. Med. 2021, 14, 4125–4134. [Google Scholar] [CrossRef] [PubMed]
- Klanovicz, T.M.; Franzosi, O.S.; Nunes, D.S.L.; Loss, S.H.; Batassini, É.; Turra, E.E.; Teixeira, C.; Vieira, S.R.R. Acute Gastrointestinal Failure Is Associated with Worse Hemodynamic and Perfusion Parameters over 48 h after Admission in Patients with Septic Shock: Retrospective Cohort Study. Nutr. Clin. Pract. 2022. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Li, Y.; Ding, L.; Fu, Y.; Dong, X.; Li, H. Prevalence and Outcome of Acute Gastrointestinal Injury in Critically Ill Patients: A Systematic Review and Meta-Analysis. Medicine 2018, 97, e12970. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Control | Septic Patients | ||
|---|---|---|---|---|
| N = 10 | Shock (+), N = 30 | Shock (−), N = 28 | p * | |
| Age, years | 67.5 (61.0–70.0) | 66.0 (60.0–73.0) | 61.5 (55.5–72.5) | 0.198 |
| Male, n (%) | 7.0 (70.0) | 18.0 (60.0) | 16.0 (57.0) | 0.825 |
| BMI, kg/m2 | 27.0 (24.0– 29.1) | 27.8 (25.2–30.9) | 26.1 (24.3–29.7) | 0.171 |
| APACHE II score | 10.5 (10–11) | 28.0 (24.0–32.0) | 24 (18–28) | 0.046 |
| SOFA score | 2 (1–3) | 10 (8.0–13.0) | 9 (8–12) | 0.388 |
| ICU admission n (%): | 0.360 | |||
| Medical | 0.0 | 18.0 (60.0) | 20.0 (71.0) | |
| Surgical | 10.0 (100.0) | 12.0 (40.0) | 8.0 (29) | |
| Lactate [mmol/L] | 0.9 (0.7–1.1) | 4.6 (2.6–8.2) | 1.7 (1.2–1.8) | <0.001 |
| PLT [103/uL] | 159.0 (137.0–181.0) | 210.0 (124.0–309.0) | 174.5 (120.0–364.5) | 0.803 |
| Fibrinogen [g/L] | 2.9 (3.6–6.5) | 4.6 (3.6–6.0) | 5.6 (3.7–6.6) | 0.481 |
| D-dimer [mg/L] | 0.7 (0.4–2.1) | 6.2 (3.9–15.7) | 6.2 (2.7–10.1) | 0.395 |
| WBC [103/uL] | 12.6 (11.2–16.1) | 17.1 (11.3–27.6) | 13.3 (9.1–21.1) | 0.543 |
| CRP [mg/L] | 61.6 (35.5–106.7) | 194.6 (104.1–328.4) | 255.6 (164.5–344.5) | 0.358 |
| PCT [ng/mL] | 0.1 (0.0–0.1) | 10.6 (3.6–34.2) | 8.7 (3.5–23.4) | 0.528 |
| Treatment n (%): | ||||
| CRRT | 0.0 | 12.0 (40.0) | 6.0 (21.0) | 0.126 |
| Mechanical ventilation | 10.0 (100) | 19.0 (63.0) | 22.0 (79.0) | 0.202 |
| ICU LOS [day] | 2.0 (2.0–3.0) | 7.5 (2.0–17.5) | 11 (5.0–21.0) | 0.093 |
| Mortality, 28 days (%) | 0.0 | 50.0 | 25.0 | 0.049 |
| Day 1 | Day 3 | Day 5 | Day 7 | Day 10 | |
|---|---|---|---|---|---|
| Citrulline [nmol/mL] | |||||
| AGI I | 27.36 | 25.03 | 26.72 | 24.11 | 33.81 |
| (13.36–30.58) | (23.30–30.92) | (23.63–46.54) | (23.42–24.40) | (27.55–35.22) | |
| AGI II | 31.00 | 27.56 | 32.66 | 29.20 | 29.40 |
| (27.26–33.30) | (25.62–36.87) | (25.62–36.87) | (21.33–31.45) | (23.84–47.95) | |
| AGI III | 24.59 | 23.42 | 22.14 | 21.50 | 18.46 |
| (12.30–26.85) | (12.64–27.47) | (9.92–26.81) | (10.32–25.88) | (8.88–26.33) | |
| * p | 0.244 | 0.197 | 0.053 | 0.205 | 0.037 |
| # p | <0.001 | 0.018 | 0.005 | 0.027 | 0.022 |
| I-FABP [pg/mL] | |||||
| AGI I | 476.61 | 400.71 | 546.00 | 493.21 | 2125.36 |
| (146.33–1095.36) | (303.84–812.14) | (155.27–1633.57) | (484.00–610.67) | (694.00–3204.29) | |
| AGI II | 956.33 | 414.67 | 421.33 | 1146.33 | 937.87 |
| (429.67–2191.00) | (254.67–1002.54) | (286.33–2432.86) | (431.00–1443.00) | (373.00–1139.67) | |
| AGI III | 832.57 | 283.76 | 416.78 | 550.35 | 698.10 |
| (125.80–1148.27) | (198.17–831.07) | (173.33–690.00) | (322.33–1673.00) | (225.71–1479.29) | |
| * p | 0.693 | 0.424 | 0.793 | 0.753 | 0.231 |
| # p | 0.293 | 0.447 | 0.451 | 0.887 | 0.650 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tyszko, M.; Lemańska-Perek, A.; Śmiechowicz, J.; Tomaszewska, P.; Biecek, P.; Gozdzik, W.; Adamik, B. Citrulline, Intestinal Fatty Acid-Binding Protein and the Acute Gastrointestinal Injury Score as Predictors of Gastrointestinal Failure in Patients with Sepsis and Septic Shock. Nutrients 2023, 15, 2100. https://doi.org/10.3390/nu15092100
Tyszko M, Lemańska-Perek A, Śmiechowicz J, Tomaszewska P, Biecek P, Gozdzik W, Adamik B. Citrulline, Intestinal Fatty Acid-Binding Protein and the Acute Gastrointestinal Injury Score as Predictors of Gastrointestinal Failure in Patients with Sepsis and Septic Shock. Nutrients. 2023; 15(9):2100. https://doi.org/10.3390/nu15092100
Chicago/Turabian StyleTyszko, Maciej, Anna Lemańska-Perek, Jakub Śmiechowicz, Paulina Tomaszewska, Przemyslaw Biecek, Waldemar Gozdzik, and Barbara Adamik. 2023. "Citrulline, Intestinal Fatty Acid-Binding Protein and the Acute Gastrointestinal Injury Score as Predictors of Gastrointestinal Failure in Patients with Sepsis and Septic Shock" Nutrients 15, no. 9: 2100. https://doi.org/10.3390/nu15092100