

The NUTRIC Score as a Tool to Predict Mortality and Increased Resource Utilization in Intensive Care Patients with Sepsis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Ethics
2.3. Patient Management and Data Collection
2.4. Statistical Analysis
3. Results
3.1. Study Sample
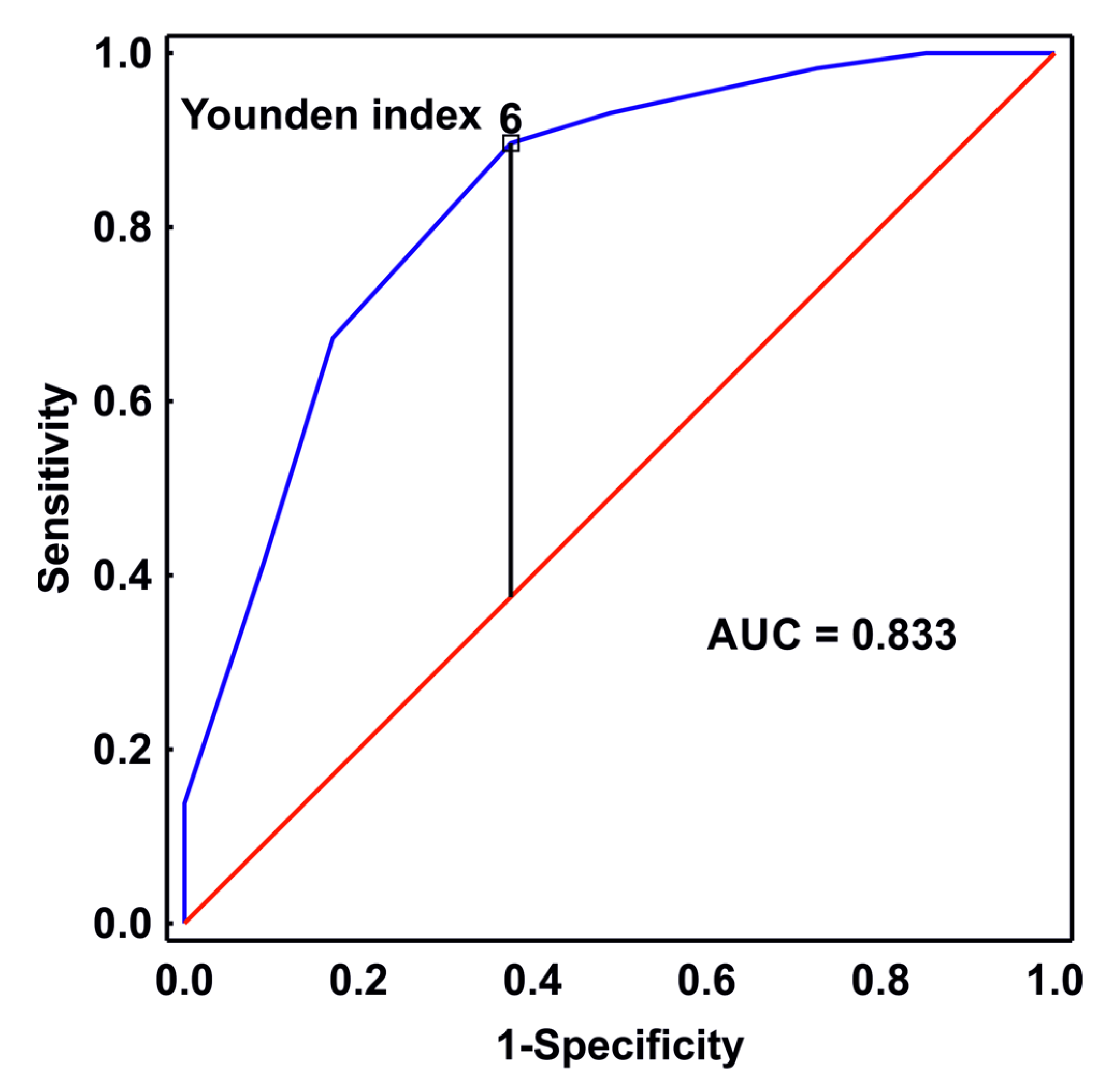
3.2. The Optimal Cut-Off Point for mNUTRIC
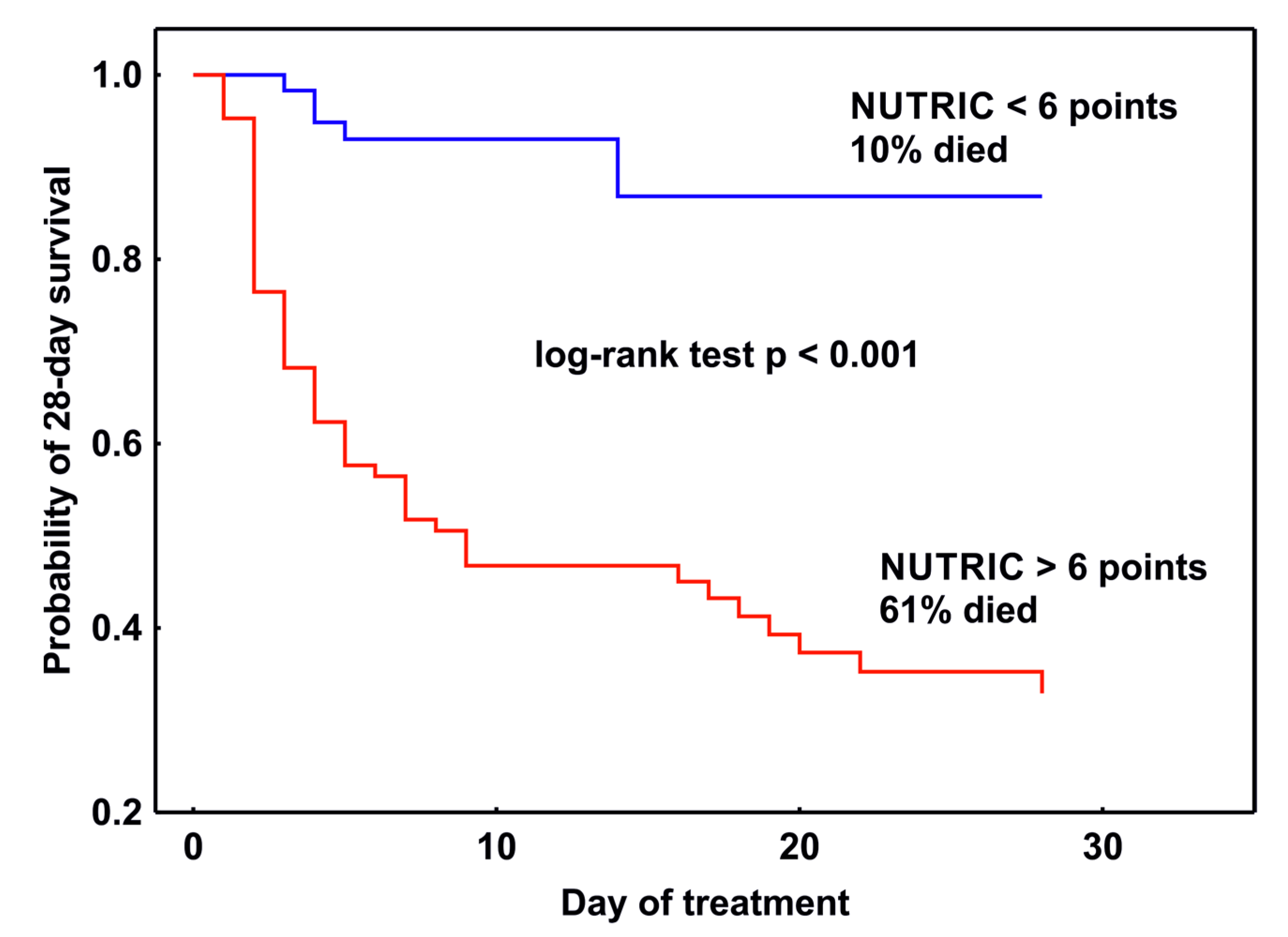
3.3. mNUTRIC Predictive Power
3.4. Characterization of Groups of Patients According to the Optimal Cut-Off Point for the mNUTRIC Score
3.5. Patient Management
3.6. Patient Management
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Heyland, D.K.; Dhaliwal, R.; Jiang, X.; Day, A.G. Identifying Critically Ill Patients Who Benefit the Most from Nutrition Therapy: The Development and Initial Validation of a Novel Risk Assessment Tool. Crit. Care 2011, 15, R268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, P.; He, Z.; Yu, G.; Peng, D.; Feng, Y.; Ling, J.; Wang, Y.; Li, S.; Bian, Y. The Modified NUTRIC Score Can Be Used for Nutritional Risk Assessment as Well as Prognosis Prediction in Critically Ill COVID-19 Patients. Clin. Nutr. 2021, 40, 534–541. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.; Kumar, A.; Kumar, A.; Pattanayak, A.; Singh, K.; Singh, P. NUTRIC Score as a Predictor of Outcome in COVID-19 ARDS Patients: A Retrospective Observational Study. Indian J. Anaesth. 2021, 65, 669. [Google Scholar] [CrossRef] [PubMed]
- Renuka, M.K.; Arunkumar, A.S. Use of Nutrition Risk in Critically Ill (NUTRIC) Score to Assess Nutritional Risk in Mechanically Ventilated Patients: A Prospective Observational Study. Indian J. Crit. Care Med. 2017, 21, 253–256. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.-Y.; Yen, Y.-T.; Lam, C.-T.; Li, K.-C.; Lu, M.-J.; Hsu, H.-S. Use of Modified-NUTRIC Score to Assess Nutritional Risk in Surgical Intensive Care Unit. J. Chin. Med. Assoc. 2021, 84, 860–864. [Google Scholar] [CrossRef]
- Zheng, C.; Xie, K.; Li, X.; Wang, G.; Luo, J.; Zhang, C.; Jiang, Z.; Wang, Y.; Luo, C.; Qiang, Y.; et al. The Prognostic Value of Modified NUTRIC Score for Patients in Cardiothoracic Surgery Recovery Unit: A Retrospective Cohort Study. J. Hum. Nutr. Diet 2021, 34, 926–934. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.-C.; Tu, C.-Y.; Chen, C.-H.; Wang, Y.-T.; Chen, W.-C.; Fu, P.-K.; Chen, C.-M.; Lai, C.-C.; Kuo, L.-K.; Ku, S.-C.; et al. Significance of the Modified NUTRIC Score for Predicting Clinical Outcomes in Patients with Severe Community-Acquired Pneumonia. Nutrients 2021, 14, 198. [Google Scholar] [CrossRef]
- Rahman, A.; Hasan, R.M.; Agarwala, R.; Martin, C.; Day, A.G.; Heyland, D.K. Identifying Critically-Ill Patients Who Will Benefit Most from Nutritional Therapy: Further Validation of the “Modified NUTRIC” Nutritional Risk Assessment Tool. Clin. Nutr. 2016, 35, 158–162. [Google Scholar] [CrossRef]
- Jeong, D.H.; Hong, S.-B.; Lim, C.-M.; Koh, Y.; Seo, J.; Kim, Y.; Min, J.-Y.; Huh, J.W. Relationship between Nutrition Intake and 28-Day Mortality Using Modified NUTRIC Score in Patients with Sepsis. Nutrients 2019, 11, 1906. [Google Scholar] [CrossRef] [Green Version]
- Mukhopadhyay, A.; Henry, J.; Ong, V.; Leong, C.S.-F.; Teh, A.L.; van Dam, R.M.; Kowitlawakul, Y. Association of Modified NUTRIC Score with 28-Day Mortality in Critically Ill Patients. Clin. Nutr. 2017, 36, 1143–1148. [Google Scholar] [CrossRef]
- Villacrs, C.Q.; Ochoa, G.S.; Sarmiento-Bobadilla, M.; Hilbron, A.S.; Garcia, C.; Cuenca, J. 376: Assessing the nutric score 28-day mortality prediction in critically ill cancer patients. Crit. Care Med. 2020, 48, 170. [Google Scholar] [CrossRef]
- de Vries, M.C.; Koekkoek, W.; Opdam, M.H.; van Blokland, D.; van Zanten, A.R. Nutritional Assessment of Critically Ill Patients: Validation of the Modified NUTRIC Score. Eur. J. Clin. Nutr. 2018, 72, 428–435. [Google Scholar] [CrossRef] [Green Version]
- van den Berg, M.; van Beuningen, F.E.; ter Maaten, J.C.; Bouma, H.R. Hospital-Related Costs of Sepsis around the World: A Systematic Review Exploring the Economic Burden of Sepsis. J. Crit. Care 2022, 71, 154096. [Google Scholar] [CrossRef]
- Lasater, K.B.; McHugh, M.D.; Rosenbaum, P.R.; Aiken, L.H.; Smith, H.L.; Reiter, J.G.; Niknam, B.A.; Hill, A.S.; Hochman, L.L.; Jain, S.; et al. Evaluating the Costs and Outcomes of Hospital Nursing Resources: A Matched Cohort Study of Patients with Common Medical Conditions. J. Gen. Intern. Med. 2021, 36, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Jones, S.L.; Ashton, C.M.; Kiehne, L.B.; Nicolas, J.C.; Rose, A.L.; Shirkey, B.A.; Masud, F.; Wray, N.P. Outcomes and Resource Use of Sepsis-Associated Stays by Presence on Admission, Severity, and Hospital Type. Med. Care 2016, 54, 303–310. [Google Scholar] [CrossRef] [Green Version]
- Al-Saad, N.A.; Nortje, J. Principles of Resource Allocation in Critical Care. BJA Educ. 2017, 17, 6. [Google Scholar] [CrossRef] [Green Version]
- Dellinger, R.P.; Levy, M.M.; Rhodes, A.; Annane, D.; Gerlach, H.; Opal, S.M.; Sevransky, J.E.; Sprung, C.L.; Douglas, I.S.; Jaeschke, R.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock, 2012. Intensive Care Med. 2013, 39, 165–228. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A Severity of Disease Classification System. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef]
- Vincent, J.-L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonça, A.; Bruining, H.; Reinhart, C.K.; Suter, P.; Thijs, L.G. The SOFA (Sepsis-Related Organ Failure Assessment) Score to Describe Organ Dysfunction/Failure. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef]
- Miranda, D.R.; de Rijk, A.; Schaufeli, W. Simplified Therapeutic Intervention Scoring System: The TISS-28 Items--Results from a Multicenter Study. Crit. Care Med. 1996, 24, 64–73. [Google Scholar] [CrossRef] [PubMed]
- Jensen, G.L.; Mirtallo, J.; Compher, C.; Dhaliwal, R.; Forbes, A.; Grijalba, R.F.; Hardy, G.; Kondrup, J.; Labadarios, D.; Nyulasi, I.; et al. Adult Starvation and Disease-Related Malnutrition: A Proposal for Etiology-Based Diagnosis in the Clinical Practice Setting from the International Consensus Guideline Committee. Clin. Nutr. 2010, 29, 151–153. [Google Scholar] [CrossRef]
- Malnutrition Advisory Group. A Consistent and Reliable Tool for Malnutrition Screening. Nurs. Times 2003, 99, 26–27. [Google Scholar]
- Lim, S.-L.; Tong, C.-Y.; Ang, E.; Lee, E.J.-C.; Loke, W.-C.; Chen, Y.; Ferguson, M.; Daniels, L. Development and Validation of 3-Minute Nutrition Screening (3-MinNS) Tool for Acute Hospital Patients in Singapore. Asia Pac. J. Clin. Nutr. 2009, 18, 395–403. [Google Scholar]
- Kruizenga, H.M.; Seidell, J.C.; de Vet, H.C.W.; Wierdsma, N.J.; van Bokhorst-de van der Schueren, M.A.E. Development and Validation of a Hospital Screening Tool for Malnutrition: The Short Nutritional Assessment Questionnaire (SNAQ). Clin. Nutr. 2005, 24, 75–82. [Google Scholar] [CrossRef]
- Ferguson, M.; Capra, S.; Bauer, J.; Banks, M. Development of a Valid and Reliable Malnutrition Screening Tool for Adult Acute Hospital Patients. Nutrition 1999, 15, 458–464. [Google Scholar] [CrossRef] [PubMed]
- Anthony, P.S. Nutrition Screening Tools for Hospitalized Patients. Nutr. Clin. Pract. 2008, 23, 373–382. [Google Scholar] [CrossRef]
- Kondrup, J.; Rasmussen, H.H.; Hamberg, O.; Stanga, Z. Ad Hoc ESPEN Working Group Nutritional Risk Screening (NRS 2002): A New Method Based on an Analysis of Controlled Clinical Trials. Clin. Nutr. 2003, 22, 321–336. [Google Scholar] [CrossRef]
- Detsky, A.S.; McLaughlin, J.R.; Baker, J.P.; Johnston, N.; Whittaker, S.; Mendelson, R.A.; Jeejeebhoy, K.N. What Is Subjective Global Assessment of Nutritional Status? JPEN J. Parenter. Enteral Nutr. 1987, 11, 8–13. [Google Scholar] [CrossRef] [Green Version]
- Fu, P.-K.; Wang, C.-Y.; Wang, W.-N.; Hsu, C.-Y.; Lin, S.-P.; Kuo, C.-T. Energy Achievement Rate Is an Independent Factor Associated with Intensive Care Unit Mortality in High-Nutritional-Risk Patients with Acute Respiratory Distress Syndrome Requiring Prolonged Prone Positioning Therapy. Nutrients 2021, 13, 3176. [Google Scholar] [CrossRef]
- dos Reis, A.M.; Fructhenicht, A.V.G.; Moreira, L.F. NUTRIC Score Use around the World: A Systematic Review. Rev. Bras. Ter. Intensiv. 2019, 31, 379–385. [Google Scholar] [CrossRef]
- Moretti, D. Estudio de dos variantes de la puntuación de riesgo nutricional. Nutr. Hosp. 2014, 166–172. [Google Scholar] [CrossRef]
- Mendes, R.; Policarpo, S.; Fortuna, P.; Alves, M.; Virella, D.; Heyland, D.K. Nutritional Risk Assessment and Cultural Validation of the Modified NUTRIC Score in Critically Ill Patients—A Multicenter Prospective Cohort Study. J. Crit. Care 2017, 37, 45–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lew, C.C.H.; Cheung, K.P.; Chong, M.F.F.; Chua, A.P.; Fraser, R.J.L.; Miller, M. Combining 2 Commonly Adopted Nutrition Instruments in the Critical Care Setting Is Superior to Administering Either One Alone. JPEN J. Parenter. Enteral Nutr. 2017, 45, 872–876. [Google Scholar] [CrossRef] [PubMed]
- Heyland, D.; Muscedere, J.; Wischmeyer, P.E.; Cook, D.; Jones, G.; Albert, M.; Elke, G.; Berger, M.M.; Day, A.G. A Randomized Trial of Glutamine and Antioxidants in Critically Ill Patients. N. Engl. J. Med. 2013, 368, 1489–1497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lew, C.C.H.; Yandell, R.; Fraser, R.J.L.; Chua, A.P.; Chong, M.F.F.; Miller, M. Association Between Malnutrition and Clinical Outcomes in the Intensive Care Unit: A Systematic Review. JPEN J. Parenter. Enteral Nutr. 2017, 41, 744–758. [Google Scholar] [CrossRef]
- Hamers, L.; Kox, M.; Pickkers, P. Sepsis-Induced Immunoparalysis: Mechanisms, Markers, and Treatment Options. Minerva Anestesiol 2015, 81, 426–439. [Google Scholar]
- Villet, S.; Chiolero, R.L.; Bollmann, M.D.; Revelly, J.-P.; Cayeux RN, M.-C.; Delarue, J.; Berger, M.M. Negative Impact of Hypocaloric Feeding and Energy Balance on Clinical Outcome in ICU Patients. Clin. Nutr. 2005, 24, 502–509. [Google Scholar] [CrossRef]
- Bodolea, C.; Nemes, A.; Avram, L.; Craciun, R.; Coman, M.; Ene-Cocis, M.; Ciobanu, C.; Crisan, D. Nutritional Risk Assessment Scores Effectively Predict Mortality in Critically Ill Patients with Severe COVID-19. Nutrients 2022, 14, 2105. [Google Scholar] [CrossRef]
- Hung, K.-Y.; Chen, Y.-M.; Wang, C.-C.; Wang, Y.-H.; Lin, C.-Y.; Chang, Y.-T.; Huang, K.-T.; Lin, M.-C.; Fang, W.-F. Insufficient Nutrition and Mortality Risk in Septic Patients Admitted to ICU with a Focus on Immune Dysfunction. Nutrients 2019, 11, 367. [Google Scholar] [CrossRef] [Green Version]
- Zusman, O.; Theilla, M.; Cohen, J.; Kagan, I.; Bendavid, I.; Singer, P. Resting Energy Expenditure, Calorie and Protein Consumption in Critically Ill Patients: A Retrospective Cohort Study. Crit. Care 2016, 20, 367. [Google Scholar] [CrossRef] [Green Version]
- The TARGET Investigators, for the ANZICS Clinical Trials Group. Energy-Dense versus Routine Enteral Nutrition in the Critically Ill. N. Engl. J. Med. 2018, 379, 1823–1834. [Google Scholar] [CrossRef] [PubMed]
- Rudd, K.E.; Johnson, S.C.; Agesa, K.M.; Shackelford, K.A.; Tsoi, D.; Kievlan, D.R.; Colombara, D.V.; Ikuta, K.S.; Kissoon, N.; Finfer, S.; et al. Global, Regional, and National Sepsis Incidence and Mortality, 1990–2017: Analysis for the Global Burden of Disease Study. Lancet 2020, 395, 200–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verburg, I.W.M.; Atashi, A.; Eslami, S.; Holman, R.; Abu-Hanna, A.; de Jonge, E.; Peek, N.; de Keizer, N.F. Which Models Can I Use to Predict Adult ICU Length of Stay? A Systematic Review. Crit. Care Med. 2017, 45, e222–e231. [Google Scholar] [CrossRef]
- Lisboa, T.; Diaz, E.; Sa-Borges, M.; Socias, A.; Sole-Violan, J.; Rodríguez, A.; Rello, J. The Ventilator-Associated Pneumonia PIRO Score. Chest 2008, 134, 1208–1216. [Google Scholar] [CrossRef]
- Sukmark, T.; Lumlertgul, N.; Praditpornsilpa, K.; Tungsanga, K.; Eiam-Ong, S.; Srisawat, N. SEA-MAKE Score as a Tool for Predicting Major Adverse Kidney Events in Critically Ill Patients with Acute Kidney Injury: Results from the SEA-AKI Study. Ann. Intensive Care 2020, 10, 42. [Google Scholar] [CrossRef] [Green Version]
- Kwak, G.H.; Ling, L.; Hui, P. Predicting the Need for Vasopressors in the Intensive Care Unit Using an Attention Based Deep Learning Model. Shock 2020. Publish Ahead of Print. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, J.M.; Fialho, A.S.; Vieira, S.M.; Mendonca, L.F.; Sousa, J.M.C. Data Mining and Modeling to Predict the Necessity of Vasopressors for ICU Patients. In Proceedings of the 2013 IEEE International Conference on Fuzzy Systems (FUZZ-IEEE), Hyderabad, India, 7–10 July 2013; IEEE: Hyderabad, India, 2013; pp. 1–6. [Google Scholar]
- Liu, R.; Greenstein, J.L.; Granite, S.J.; Fackler, J.C.; Bembea, M.M.; Sarma, S.V.; Winslow, R.L. Data-Driven Discovery of a Novel Sepsis Pre-Shock State Predicts Impending Septic Shock in the ICU. Sci. Rep. 2019, 9, 6145. [Google Scholar] [CrossRef] [Green Version]
- Johnson, A.E.W.; Pollard, T.J.; Shen, L.; Lehman, L.H.; Feng, M.; Ghassemi, M.; Moody, B.; Szolovits, P.; Anthony Celi, L.; Mark, R.G. MIMIC-III, a Freely Accessible Critical Care Database. Sci. Data 2016, 3, 160035. [Google Scholar] [CrossRef] [Green Version]
- Siu, B.M.K.; Kwak, G.H.; Ling, L.; Hui, P. Predicting the Need for Intubation in the First 24 h after Critical Care Admission Using Machine Learning Approaches. Sci. Rep. 2020, 10, 20931. [Google Scholar] [CrossRef]
- Buswell, L.; Hayes, A.; Baombe, J. BET 2: Predicting the Need for Endotracheal Intubation in Poisoned Patients. Emerg. Med. J. 2019, 36, 573–575. [Google Scholar] [CrossRef] [PubMed]
- Onishi, S.; Osuka, A.; Kuroki, Y.; Ueyama, M. Indications of Early Intubation for Patients with Inhalation Injury. Acute Med. Surg. 2017, 4, 278–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variable | Range | Points |
|---|---|---|
| Age (years) | Below 50 | 0 |
| From 50 to 74 | 1 | |
| 75 and more | 2 | |
| APACHE II (points) | Below 15 | 0 |
| From 15 to 19 | 1 | |
| From 20 to 27 | 2 | |
| 28 and more | 3 | |
| SOFA (points) | Below 6 | 0 |
| From 6 to 9 | 1 | |
| 10 and more | 2 | |
| Co-morbidities (n) | 0, 1 | 0 |
| 2 and more | 1 | |
| Days before ICU admission | 0 | 0 |
| 1 and more | 1 |
| mNUTRIC ≥ 6 pts | mNUTRIC < 6 pts | p-Value | |
|---|---|---|---|
| (n = 85) | (n = 61) | ||
| Age (years) | 69 (63–80) | 61 (50–78) | <0.001 |
| Male/Female | 56 (/29) | (39/22) | 0.807 |
| APACHE II | 24 (21–30) | 14 (11–18) | <0.001 |
| SOFA | 12 (10–15) | 8 (6–10) | <0.001 |
| Source of infection (%) | |||
| Lungs | 49 | 48 | 0.823 |
| Abdominal cavity | 31 | 30 | 0.888 |
| Urinary tract | 4 | 11 | 0.062 |
| Other * | 16 | 11 | 0.396 |
| Co-morbidities (%) | |||
| Chronic circulatory failure | 39 | 15 | 0.001 |
| Liver disease | 11 | 3 | 0.088 |
| Hematological diseases | 5 | 6 | 0.446 |
| Hypertention | 52 | 36 | 0.060 |
| Diabetes | 25 | 21 | 0.632 |
| Copd | 9 | 2 | 0.051 |
| Chronic kindey disease | 22 | 11 | 0.090 |
| Malignancies | 13 | 10 | 0.564 |
| Procalcitonin (ng/mL) | 6.2 (2.75–28.6) | 4.54 (0.89–8.75) | 0.174 |
| Lactate (mmol/L) | 3.96 (1.87–7.88) | 1.69 (1.16–3.2) | <0.001 |
| LOS before ICU (day) | 3 (1–8) | 2 (0–13) | 0.112 |
| LOS in the ICU (day) | 8 (3–18) | 13 (7–29) | 0.003 |
| LOS in the hospital (day) | 16 (6–43) | 43 (28–65) | <0.001 |
| 28-day mortality (%) | 61 | 10 | <0.001 |
| mNUTRIC ≥ 6 pts | mNUTRIC < 6 pts | p-Value | |
|---|---|---|---|
| (n = 85) | (n = 61) | ||
| Age (years) | 69 (63–80) | 61 (50–78) | <0.001 |
| APACHE II | 24 (21–30) | 14 (11–18) | <0.001 |
| 1st day SOFA | 12 (10–15) | 8 (6–10) | <0.001 |
| LOS before ICU admission | 3 (1–8) | 2 (0–13) | 0.112 |
| Number of comorbidities | 2 (1–3) | 1 (1–2) | <0.001 |
| Parameter | NUTRIC ≥ 6 | NUTRIC < 6 | p-Value |
|---|---|---|---|
| Fluid resuscitation n (%) | 73 (86) | 46 (75) | 0.154 |
| Vasopressors n (%) | 83 (98) | 50 (82) | 0.001 |
| Mechanical Ventilation n (%) | 84 (99) | 53 (87) | 0.018 |
| RRT n (%) | 46 (54) | 16 (26) | 0.001 |
| Steroids n (%) | 58 (68) | 19 (31) | 0.001 |
| Nutrition Theraphy n (%) | 48 (56) | 45 (74) | 0.021 |
| Enteral n (%) | 31 (36) | 28 (46) | 0.252 |
| Parenteral n (%) | 17 (19) | 17 (26) | 0.286 |
| Insulin n (%) | 50 (59) | 38 (62) | 0.643 |
| Thromboprohylaxis n (%) | 67 (79) | 58 (95) | 0.001 |
| Blood products n (%) | 51 (60) | 26 (43) | 0.038 |
| Surgery during ICU stay n (%) | 29 (34) | 20 (33) | 0.866 |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| Parameter | Odds Ratio | 95%CI | p-Value | Odds Ratio | 95%CI | p-Value |
| mNUTRIC score | 2.24 | 1.71–2.95 | <0.001 | 1.86 | 1.36–2.54 | <0.001 |
| Septic shock | 8.24 | 3.59–8.89 | <0.001 | 4.19 | 1.38–12.73 | 0.011 |
| Lactate level | 1.52 | 1.27–1.82 | <0.001 | 1.32 | 1.08 –1.59 | 0.005 |
| Gender | 0.65 | 0.32–1.33 | 0.248 | |||
| Procalcitonin level | 1.00 | 0.99–1.01 | 0.990 | |||
| RRT | 3.47 | 1.72–7.01 | <0.001 | |||
| Respiratory support | 1.78 | 0.32–0.22 | 0.521 | |||
| Positive blood culture | 1.02 | 0.48–2.15 | 0.949 | |||
| Time to antibiotic administration | 1.00 | 0.99–1.00 | 0.572 | |||
| Co-morbidities: | ||||||
| Chronic circulatory failure | 2.07 | 0.10–4.30 | 0.048 | |||
| Liver disease | 1.91 | 0.55–6.59 | 0.302 | |||
| Hematological diseases | 0.91 | 0.20–3.94 | 0.894 | |||
| Hypertention | 1.37 | 0.71–2.68 | 0.345 | |||
| Diabetes | 1.08 | 0.49–2.36 | 0.843 | |||
| Copd | 2.67 | 0.61–11.64 | 0.191 | |||
| Chronic kindey disease | 2.01 | 0.85–4.74 | 0.108 | |||
| Malignancies | 1.60 | 0.56–4.53 | 0.376 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wełna, M.; Adamik, B.; Kübler, A.; Goździk, W. The NUTRIC Score as a Tool to Predict Mortality and Increased Resource Utilization in Intensive Care Patients with Sepsis. Nutrients 2023, 15, 1648. https://doi.org/10.3390/nu15071648
Wełna M, Adamik B, Kübler A, Goździk W. The NUTRIC Score as a Tool to Predict Mortality and Increased Resource Utilization in Intensive Care Patients with Sepsis. Nutrients. 2023; 15(7):1648. https://doi.org/10.3390/nu15071648
Chicago/Turabian StyleWełna, Marek, Barbara Adamik, Andrzej Kübler, and Waldemar Goździk. 2023. "The NUTRIC Score as a Tool to Predict Mortality and Increased Resource Utilization in Intensive Care Patients with Sepsis" Nutrients 15, no. 7: 1648. https://doi.org/10.3390/nu15071648