
Comparison of Weight Reduction, Change in Parameters and Safety of a Very Low Carbohydrate Diet in Comparison to a Low Carbohydrate Diet in Obese Japanese Subjects with Metabolic Disorders
 , ,
, ,
Abstract
:1. Introduction
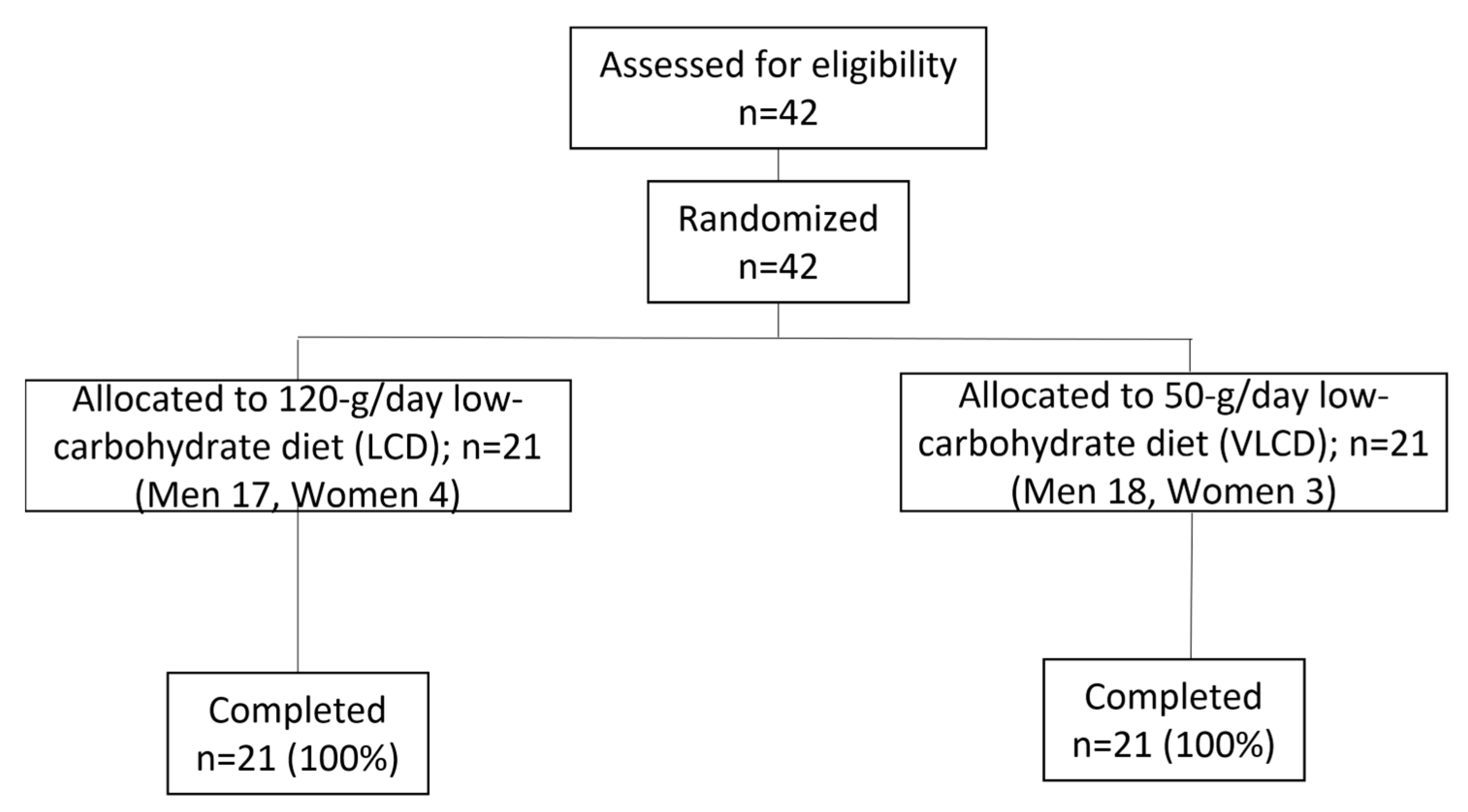
2. Materials and Methods
Statistical Analysis
3. Results
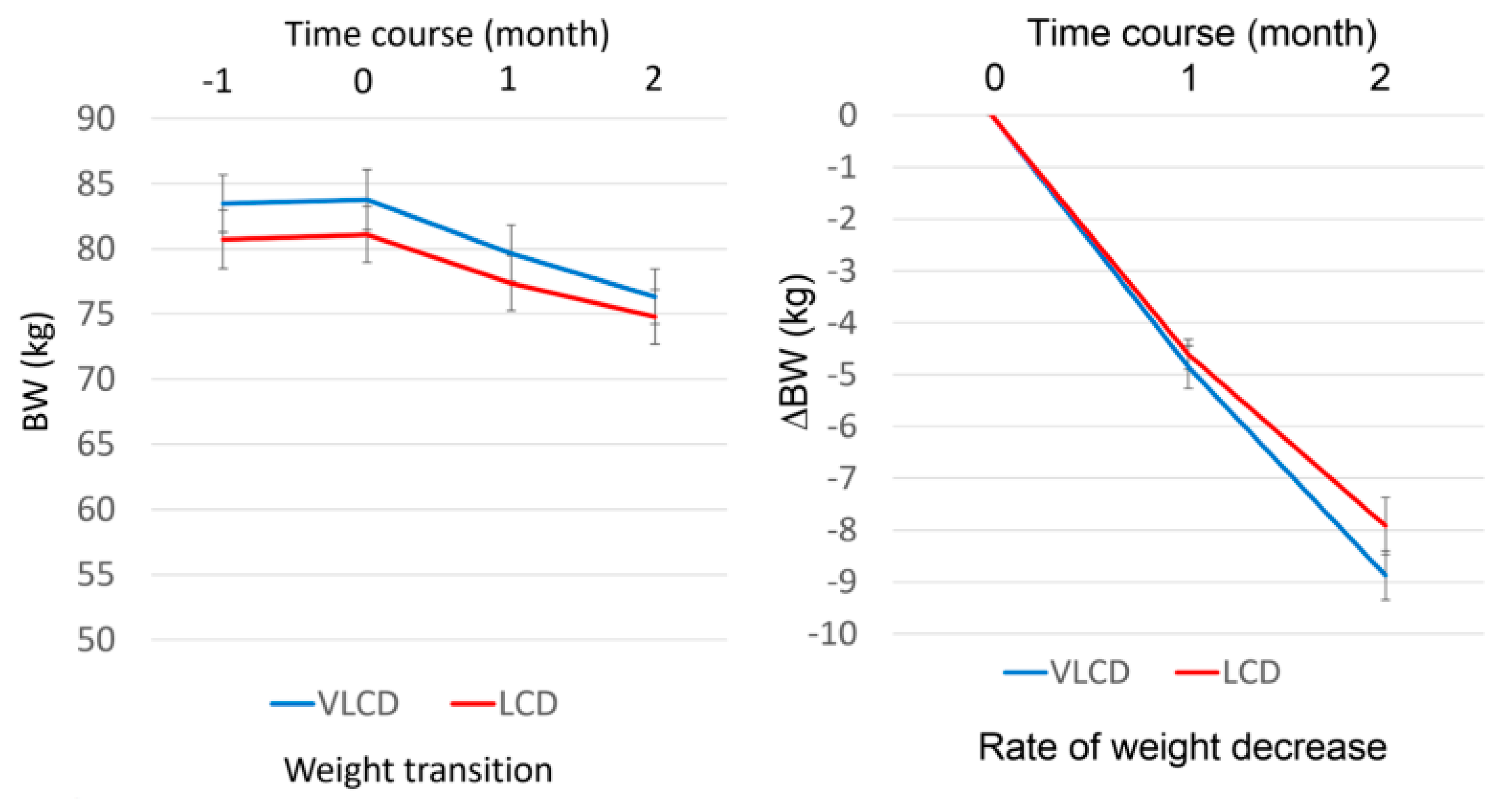
3.1. The LCD and VLCD Groups Showed an Equal Decrease in BW and Other Body Composition Parameters
3.2. Lipid Profile
3.3. Liver Function
3.4. Glucose Metabolism
3.5. Ketone Bodies
3.6. Other Parameters
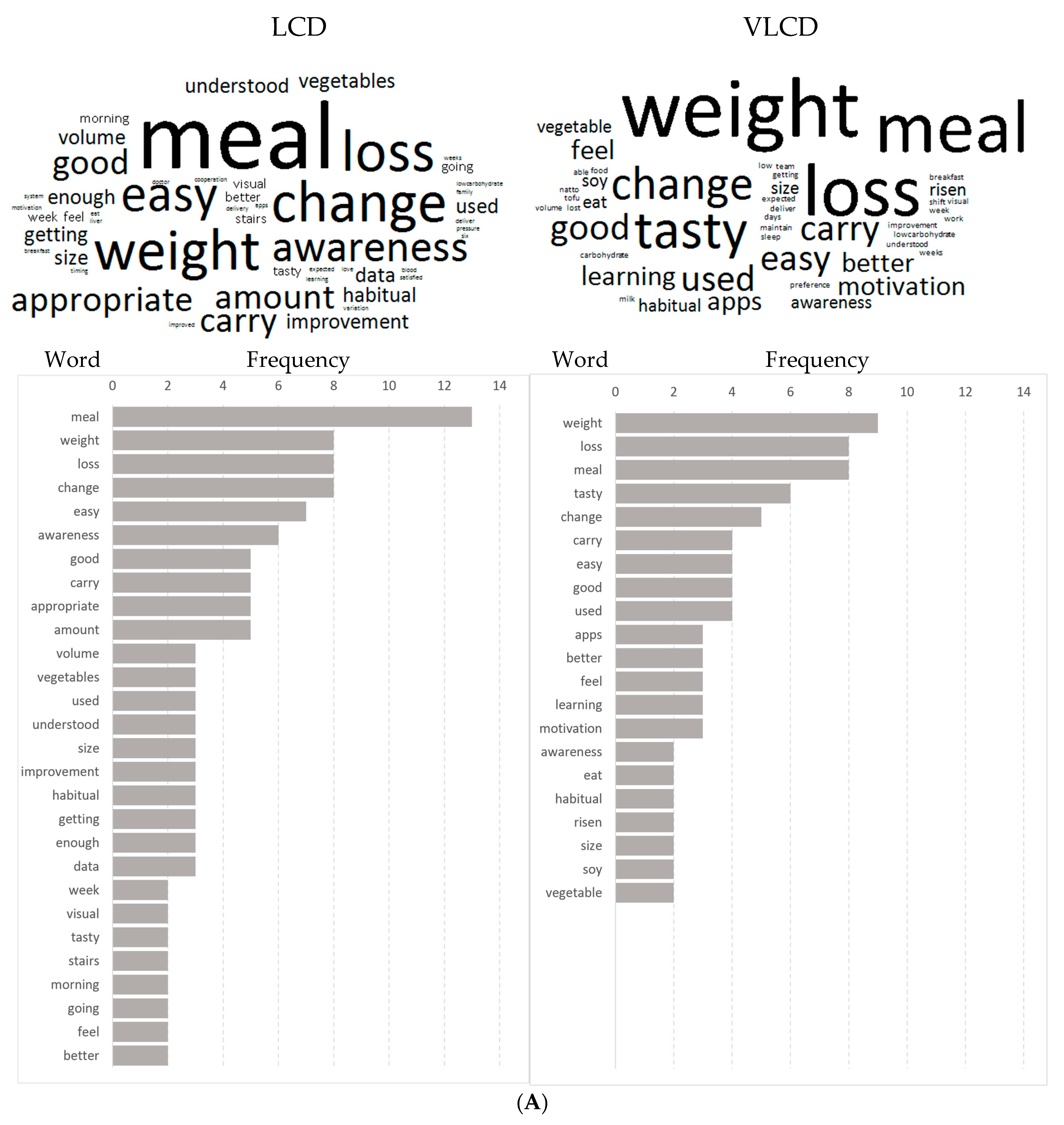
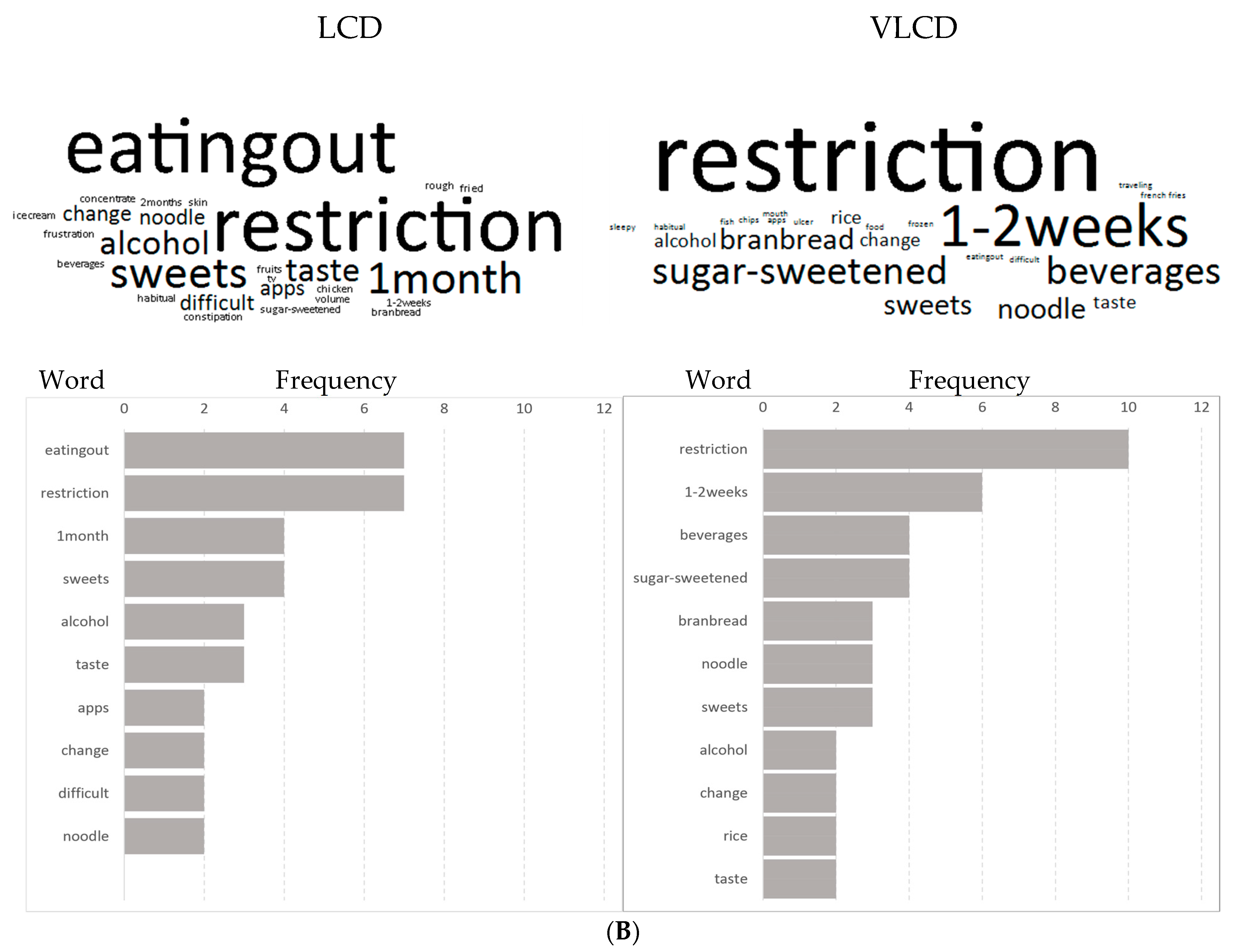
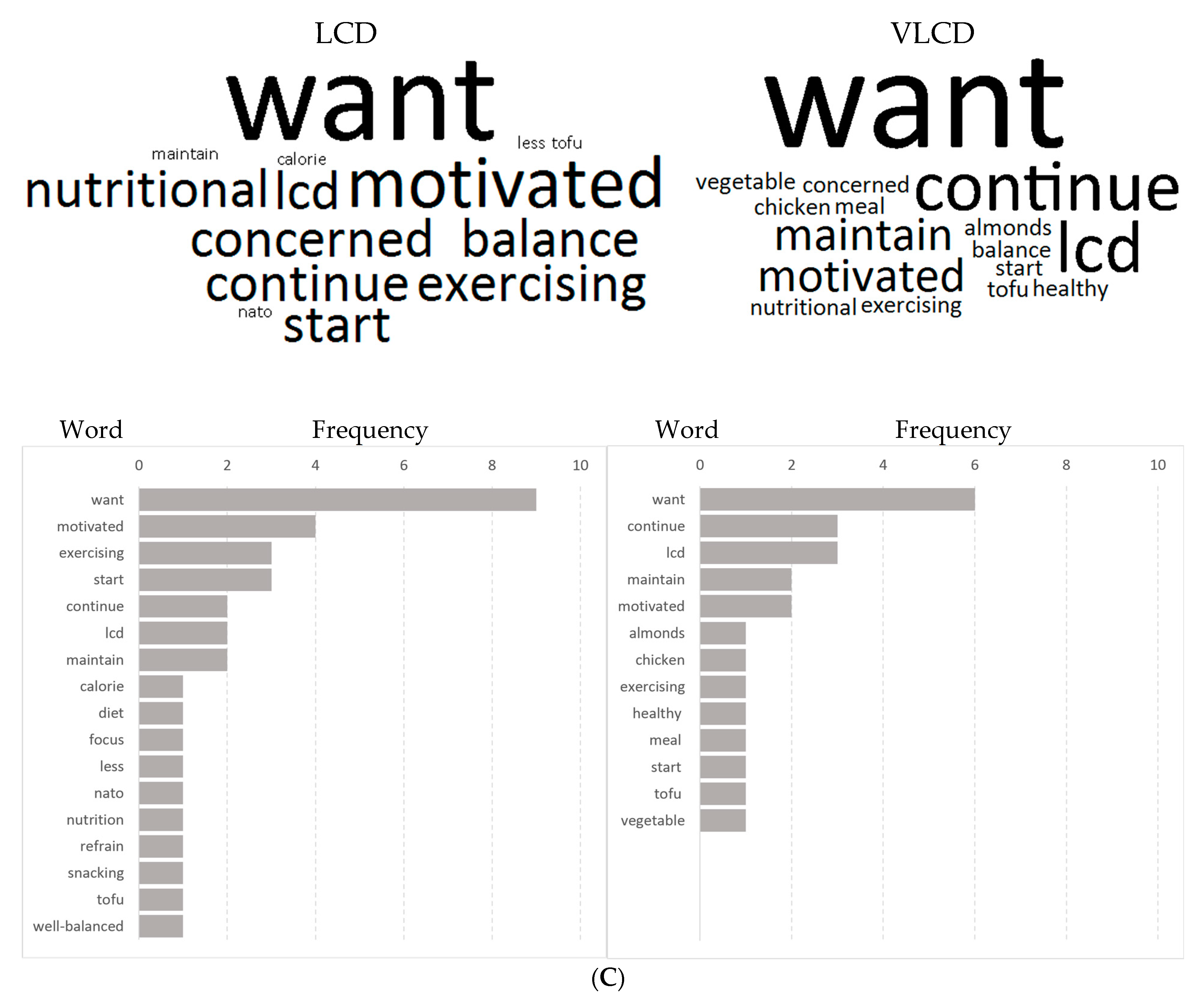
3.7. Questionnaire Survey after the Study
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.N.; Mbanya, J.C.; et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef] [PubMed]
- Shai, I.; Jiang, R.; Manson, J.E.; Stampfer, M.J.; Willett, W.C.; Colditz, G.A.; Hu, F.B. Ethnicity, obesity, and risk of type 2 diabetes in women: A 20-year follow-up study. Diabetes Care 2006, 29, 1585–1590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kushiyama, A.; Yoshida, Y.; Kikuchi, T.; Suzawa, N.; Yamamoto, M.; Tanaka, K.; Okayasu, M.; Tahara, T.; Takao, T.; Onishi, Y.; et al. Twenty-year trend of increasing obesity in young patients with poorly controlled type 2 diabetes at first diagnosis in urban Japan. J. Diabetes Investig. 2013, 4, 540–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association Professional Practice Committee. 8. Obesity and Weight Management for the Prevention and Treatment of Type 2 Diabetes: Standards of Medical Care in Diabetes-2022. Diabetes Care 2022, 45, S113–S124. [Google Scholar] [CrossRef]
- Accurso, A.; Bernstein, R.K.; Dahlqvist, A.; Draznin, B.; Feinman, R.D.; Fine, E.J.; Gleed, A.; Jacobs, D.B.; Larson, G.; Lustig, R.H.; et al. Dietary carbohydrate restriction in type 2 diabetes mellitus and metabolic syndrome: Time for a critical appraisal. Nutr. Metab. 2008, 5, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamada, Y.; Uchida, J.; Izumi, H.; Tsukamoto, Y.; Inoue, G.; Watanabe, Y.; Irie, J.; Yamada, S. A non-calorie-restricted low-carbohydrate diet is effective as an alternative therapy for patients with type 2 diabetes. Intern. Med. 2014, 53, 13–19. [Google Scholar] [CrossRef] [Green Version]
- Sato, J.; Kanazawa, A.; Makita, S.; Hatae, C.; Komiya, K.; Shimizu, T.; Ikeda, F.; Tamura, Y.; Ogihara, T.; Mita, T.; et al. A randomized controlled trial of 130 g/day low-carbohydrate diet in type 2 diabetes with poor glycemic control. Clin. Nutr. 2017, 36, 992–1000. [Google Scholar] [CrossRef]
- Shai, I.; Schwarzfuchs, D.; Henkin, Y.; Shahar, D.R.; Witkow, S.; Greenberg, I.; Golan, R.; Fraser, D.; Bolotin, A.; Vardi, H.; et al. Weight loss with a low-carbohydrate, Mediterranean, or low-fat diet. N. Engl. J. Med. 2008, 359, 229–241. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. 4. Comprehensive Medical Evaluation and Assessment of Comorbidities: Standards of Medical Care in Diabetes-2019. Diabetes Care 2019, 42, S34–S45. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. 5. Lifestyle Management: Standards of Medical Care in Diabetes-2019. Diabetes Care 2019, 42, S46–S60. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. 7. Diabetes Technology: Standards of Medical Care in Diabetes-2019. Diabetes Care 2019, 42, S71–S80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association. 8. Obesity Management for the Treatment of Type 2 Diabetes: Standards of Medical Care in Diabetes-2019. Diabetes Care 2019, 42, S81–S89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association. 12. Older Adults: Standards of Medical Care in Diabetes-2019. Diabetes Care 2019, 42, S139–S147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association. 15. Diabetes Care in the Hospital: Standards of Medical Care in Diabetes-2019. Diabetes Care 2019, 42, S173–S181. [Google Scholar] [CrossRef] [Green Version]
- Buren, J.; Ericsson, M.; Damasceno, N.R.T.; Sjodin, A. A Ketogenic Low-Carbohydrate High-Fat Diet Increases LDL Cholesterol in Healthy, Young, Normal-Weight Women: A Randomized Controlled Feeding Trial. Nutrients 2021, 13, 814. [Google Scholar] [CrossRef]
- Cox, P.J.; Kirk, T.; Ashmore, T.; Willerton, K.; Evans, R.; Smith, A.; Murray, A.J.; Stubbs, B.; West, J.; McLure, S.W.; et al. Nutritional Ketosis Alters Fuel Preference and Thereby Endurance Performance in Athletes. Cell Metab. 2016, 24, 256–268. [Google Scholar] [CrossRef] [Green Version]
- Han, J.H.; Oh, T.J.; Lee, G.; Maeng, H.J.; Lee, D.H.; Kim, K.M.; Choi, S.H.; Jang, H.C.; Lee, H.S.; Park, K.S.; et al. The beneficial effects of empagliflozin, an SGLT2 inhibitor, on atherosclerosis in ApoE−/− mice fed a western diet. Diabetologia 2017, 60, 364–376. [Google Scholar] [CrossRef] [Green Version]
- Tomita, I.; Kume, S.; Sugahara, S.; Osawa, N.; Yamahara, K.; Yasuda-Yamahara, M.; Takeda, N.; Chin-Kanasaki, M.; Kaneko, T.; Mayoux, E.; et al. SGLT2 Inhibition Mediates Protection from Diabetic Kidney Disease by Promoting Ketone Body-Induced mTORC1 Inhibition. Cell Metab. 2020, 32, 404–419.E6. [Google Scholar] [CrossRef]
- Tay, J.; Luscombe-Marsh, N.D.; Thompson, C.H.; Noakes, M.; Buckley, J.D.; Wittert, G.A.; Yancy, W.S., Jr.; Brinkworth, G.D. A very low-carbohydrate, low-saturated fat diet for type 2 diabetes management: A randomized trial. Diabetes Care 2014, 37, 2909–2918. [Google Scholar] [CrossRef] [Green Version]
- Pearl, R.L.; Wadden, T.A.; Tronieri, J.S.; Berkowitz, R.I.; Chao, A.M.; Alamuddin, N.; Leonard, S.M.; Carvajal, R.; Bakizada, Z.M.; Pinkasavage, E.; et al. Short- and Long-Term Changes in Health-Related Quality of Life with Weight Loss: Results from a Randomized Controlled Trial. Obesity 2018, 26, 985–991. [Google Scholar] [CrossRef] [Green Version]
- Langan, A.; Bader, A.; Goedkoop, S.; Cummings, S.; Tsikitas, M.; Nogueira, I.; Campoverde Reyes, K.J.; Stanford, F.C. A longitudinal study to investigate the effects of a 12-week comprehensive lifestyle weight management program on body weight and quality of life. Clin. Nutr. ESPEN 2020, 40, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Gualtieri, P.; Marchetti, M.; Frank, G.; Cianci, R.; Bigioni, G.; Colica, C.; Soldati, L.; Moia, A.; De Lorenzo, A.; Di Renzo, L. Exploring the Sustainable Benefits of Adherence to the Mediterranean Diet during the COVID-19 Pandemic in Italy. Nutrients 2022, 15, 110. [Google Scholar] [CrossRef] [PubMed]
- Jospe, M.R.; Haszard, J.J.; Taylor, R.W.; Freedhoff, Y. A tool for assessing the satisfaction of a diet: Development and preliminary validation of the Diet Satisfaction Score. Nutr. Diet. 2020, 77, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Nakata, Y.; Sasai, H.; Gosho, M.; Kobayashi, H.; Shi, Y.; Ohigashi, T.; Mizuno, S.; Murayama, C.; Kobayashi, S.; Sasaki, Y. A Smartphone Healthcare Application, CALO mama Plus, to Promote Weight Loss: A Randomized Controlled Trial. Nutrients 2022, 14, 4608. [Google Scholar] [CrossRef]
- Koeryaman, M.T.; Pallikadavath, S.; Ryder, I.H.; Kandala, N. The Effectiveness of a Web-Based Application for a Balanced Diet and Healthy Weight Among Indonesian Pregnant Women: Randomized Controlled Trial. JMIR Form. Res. 2023, 7, e38378. [Google Scholar] [CrossRef]
- Hinchliffe, N.; Capehorn, M.S.; Bewick, M.; Feenie, J. The Potential Role of Digital Health in Obesity Care. Adv. Ther. 2022, 39, 4397–4412. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| LCD | VLCD | p Value * | |
|---|---|---|---|
| n | 21 | 21 | N/A |
| Gender (male/female) | 17/4 | 18/3 | NS |
| Age (Years) | 44 ± 2 | 41 ± 2 | NS |
| Height (cm) | 166.4 ± 1.7 | 170.8 ± 1.6 | NS |
| Body weight (kg) | 79.2 [75.1–85.1] | 83.2 [76.8–91] | NS |
| Body mass index (kg/m2) | 29 [27.4–31] | 27.6 [26.3–31.5] | NS |
| Waist (cm) | 98 [91.6–103.4] | 96.5 [90.8–108] | NS |
| Body fat (%) | 30 [24.2–32.5] | 28.1 [25.3–35.6] | NS |
| SBP (mmHg) | 131 [121.5–139] | 133 [121–141] | NS |
| DBP (mmHg) | 81 [75–88.5] | 77 [70.5–86.5] | NS |
| AST (GOT) (U/L) | 25 [20–40.5] | 28 [21–37.5] | NS |
| ALT (GPT) (U/L) | 38 [28–57] | 45 [24–72] | NS |
| γ-GTP (U/L) | 46 [26–70] | 51 [37–78] | NS |
| UA (mg/dL) | 6.4 [5.3–7.5] | 7 [6.5–7.9] | NS |
| Cr (mg/dL) | 0.8 [0.7–0.9] | 0.8 [0.7–1] | NS |
| eGFR (mL/min/1.73 m2) | 79 [74.4–91.9] | 77.1 [70.4–92.9] | NS |
| TG (mg/dL) | 203 [146–259.5] | 156 [114–253.5] | NS |
| T-Cho (mg/dL) | 218 [196–251] | 214 [190.5–237.5] | NS |
| HDL-C (mg/dL) | 45 [38.5–54] | 46 [42.5–54] | NS |
| LDL-C (mg/dL) | 130 [120–157] | 135 [118–149.5] | NS |
| CRP (mg/dL) | 0.1 [0.1–0.2] | 0.1 [0.1–0.2] | NS |
| C peptide (ng/mL) | 2.5 [1.9–3.3] | 2.2 [1.7–3] | NS |
| FPG (mg/dL) | 92 [87–112] | 94 [89.5–97.5] | NS |
| HbA1c (%) | 5.6 [5.4–5.8] | 5.6 [5.4–5.8] | NS |
| Total ketone (µmol/L) | 50 [37.5, 82] | 63 [50, 113.5] | NS |
| 3OHBA (µmol/L) | 32 [22.5, 54.5] | 40 [28.5, 74] | NS |
| Acetylacetic acid (µmol/L) | 19 [15.5, 19] | 26 [18, 39.5] | NS |
| Antidiabetic drug N (%) | 2 (9.5) | 1 (4.8) | NS |
| Antihypertensive agents N (%) | 3 (14.3) | 2 (9.5) | NS |
| Lipid-lowering agents N (%) | 0 (0) | 1 (4.8) | NS |
| Uric acid treatment N (%) | 1(4.8) | 1(4.8) | NS |
| Smoking (Never/Ex/Current) N | 7/4/10 | 3/7/11 | NS |
| LCD | VLCD | p Value * | |
|---|---|---|---|
| ∆Body weight (kg) | −5.4 [−8.8, −4.7]) | −8 [−8.7, −6.1] | NS |
| ∆Body mass index (kg/m2) | −2.1 [−3.1, −1.7] | −2.6 [−2.9, −2] | NS |
| ∆Waist (cm) | −6.8 [−8.9, −4.3] | −8.5 [−10.3, −6.5] | NS |
| ∆Body fat (%) | −2.6 [−3.9, −1.5] | −2.8 [−4, −2.4] | NS |
| ∆SBP (mmHg) | −4 [−9.5, −2] | −8 [−17.5, −1.5] | NS |
| ∆DBP (mmHg) | −6 [−13, −1.5] | −5 [–11, –1] | NS |
| ∆AST (U/L) | −6 [–15, –2] | −7 [–15, –3] | NS |
| ∆ALT (U/L) | −12 [−24.5, −2] | −16 [-35.5, −5.5] | NS |
| ∆γ-GTP (U/L) | −14 [−40, −7.5] | −28 [-52.5, −13] | NS |
| ∆UA (mg/dL) | −0.3 [−0.7, 0.8] | −0.5 [−0.9, 0.1] | NS |
| ∆Cr (mg/dL) | −0.01 [−0.04, 0.02] | −0.07 [−0.1, −0.02] | p = 0.008 |
| ∆eGFR (mL/min/1.73 m2) | 1 [−1.8, 4.1] | 6.9 [1.8, 11] | p = 0.01 |
| ∆TG (mg/dL) | −103 [−161.5, −75.5] | −98 [−145, −47.5] | NS |
| ∆HDL-C (mg/dL) | 5 [0.5, 8] | 4 [1.5, 9] | NS |
| ∆LDL-C (mg/dL) | −2 [−17, 6] | 8 [−17.5, 22.5] | NS |
| ∆CRP (mg/dL) | −0.02 [−0.06, 0.02] | −0.01 [-0.03, 0.15] | NS |
| ∆C peptide (ng/mL) | −0.6 [−1.6, −0.4] | −0.8 [−1.2, −0.5] | NS |
| ∆FPG (mg/dL) | −6 [−21.5, 0] | −7 [−11, 1] | NS |
| ∆HbA1c (%) | −0.1 [−0.3, 0.1] | −0.2 [−0.4, 0] | NS |
| ∆Total ketone (µmol/L) | 140 [67, 485.5] | 538 [187.5, 810.5] | p = 0.04 |
| ∆3OHBA (µmol/L) | 98 [49.5, 373.5] | 390 [142, 608.5] | p = 0.045 |
| ∆Acetylacetic acid (µmol/L) | 42 [20, 112] | 538 [187.5, 810.5] | p = 0.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kikuchi, T.; Kushiyama, A.; Yanai, M.; Kashiwado, C.; Seto, T.; Kasuga, M. Comparison of Weight Reduction, Change in Parameters and Safety of a Very Low Carbohydrate Diet in Comparison to a Low Carbohydrate Diet in Obese Japanese Subjects with Metabolic Disorders. Nutrients 2023, 15, 1342. https://doi.org/10.3390/nu15061342
Kikuchi T, Kushiyama A, Yanai M, Kashiwado C, Seto T, Kasuga M. Comparison of Weight Reduction, Change in Parameters and Safety of a Very Low Carbohydrate Diet in Comparison to a Low Carbohydrate Diet in Obese Japanese Subjects with Metabolic Disorders. Nutrients. 2023; 15(6):1342. https://doi.org/10.3390/nu15061342
Chicago/Turabian StyleKikuchi, Takako, Akifumi Kushiyama, Miho Yanai, Chieko Kashiwado, Takeshi Seto, and Masato Kasuga. 2023. "Comparison of Weight Reduction, Change in Parameters and Safety of a Very Low Carbohydrate Diet in Comparison to a Low Carbohydrate Diet in Obese Japanese Subjects with Metabolic Disorders" Nutrients 15, no. 6: 1342. https://doi.org/10.3390/nu15061342