
Mediterranean Diet and Lung Function in Adults Current Smokers: A Cross-Sectional Analysis in the MEDISTAR Project
 , , , ,
, , , ,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
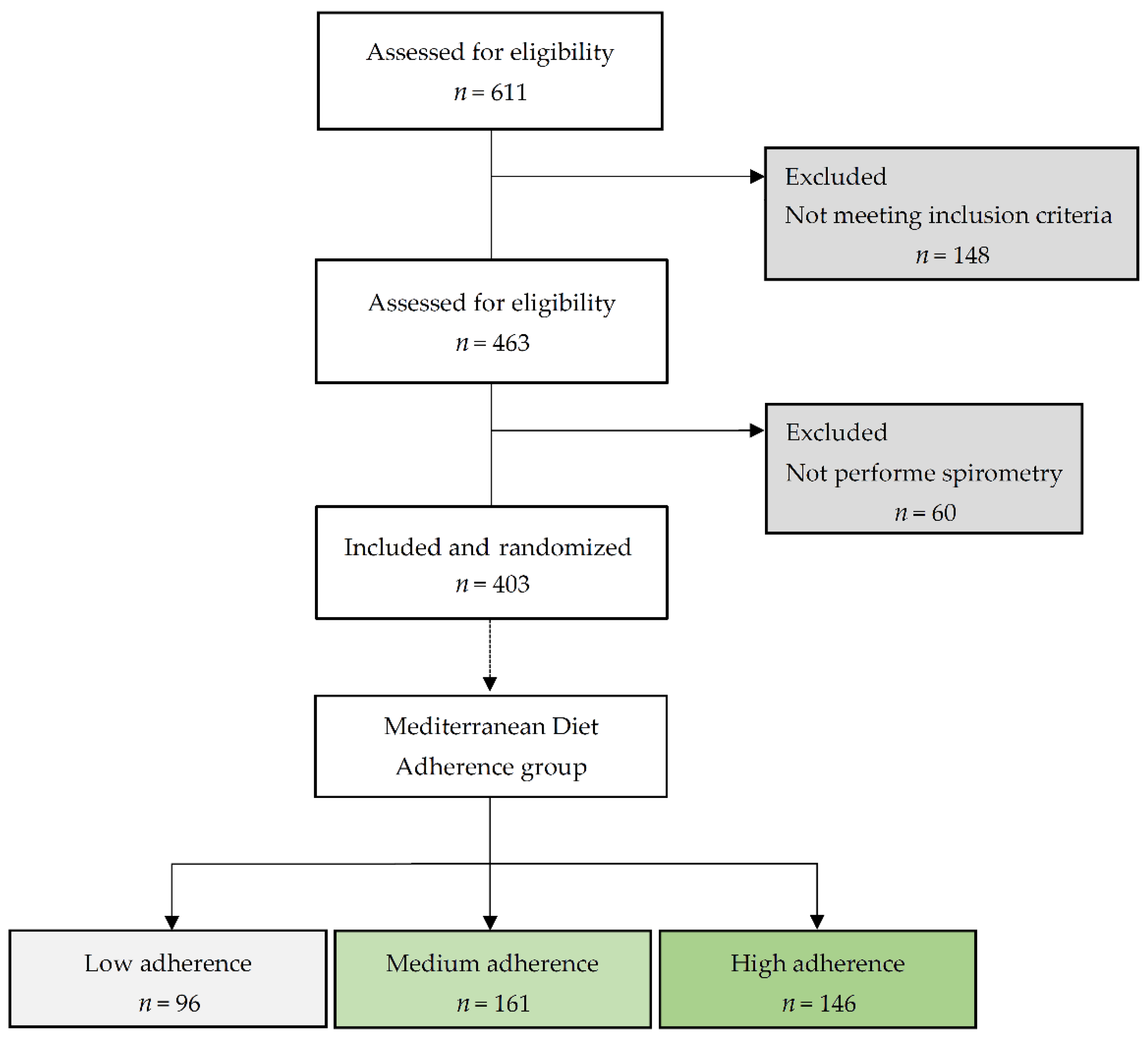
2.1. Study Design
2.2. Selection of Participants and Obtaining the Sample
2.3. Study Variables
2.4. Statistical Analysis
2.5. Ethical Approval
3. Results
4. Discussion
Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Singh, D.; Agusti, A.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Celli, B.R.; Criner, G.J.; Frith, P.; Halpin, D.M.G.; Han, M.; et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease: The GOLD science committee report 2019. Eur. Respir. J. 2019, 53, 1900164. [Google Scholar] [CrossRef]
- Reddel, H.K.; Bacharier, L.B.; Bateman, E.D.; Brightling, C.E.; Brusselle, G.G.; Buhl, R.; Cruz, A.A.; Duijts, L.; Drazen, J.M.; FitzGerald, J.M.; et al. Global Initiative for Asthma Strategy 2021: Executive summary and rationale for key changes. Eur. Respir. J. 2021, 59, 2102730. [Google Scholar] [CrossRef] [PubMed]
- Scoditti, E.; Massaro, M.; Garbarino, S.; Toraldo, D.M. Role of Diet in Chronic Obstructive Pulmonary Disease Prevention and Treatment. Nutrients 2019, 11, 1357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lange, P.; Celli, B.; Agustí, A.; Boje Jensen, G.; Divo, M.; Faner, R.; Guerra, S.; Marott, J.L.; Martinez, F.D.; Martinez-Camblor, P.; et al. Lung-function trajectories leading to chronic obstructive pulmonary disease. N. Engl. J. Med. 2015, 373, 111–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agustí, A.; Melen, E.; DeMeo, D.L.; Breyer-Kohansal, R.; Faner, R. Pathogenesis of chronic obstructive pulmonary disease: Understanding the contributions of gene-environment interactions across the lifespan. Lancet Respir. Med. 2022, 10, 512–524. [Google Scholar] [CrossRef] [PubMed]
- Townend, J.; Minelli, C.; Mortimer, K.; Obaseki, D.O.; Al Ghobain, M.; Cherkaski, H.; Denguezli, M.; Gunesekera, K.; Hafizi, H.; Koul, P.A.; et al. The association between chronic airflow obstruction and poverty in 12 sites of the multinational BOLD study. Eur. Respir. J. 2017, 49, 1601880. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Larsen, V.; Amigo, H.; Bustos, P.; Bakolis, I.; Rona, R.J. Ventilatory Function in Young Adults and Dietary Antioxidant Intake. Nutrients 2015, 7, 2879–2896. [Google Scholar] [CrossRef] [Green Version]
- Varraso, R.; Camargo, C.A. Processed meat consumption and lung health: More evidence for harm. Eur. Respir. J. 2014, 43, 943–946. [Google Scholar] [CrossRef] [Green Version]
- Mehta, A.J.; Guidot, D.M. Alcohol and the lung. Alcohol Res. 2017, 38, 243–254. [Google Scholar] [PubMed]
- Garcia-Larsen, V.; Potts, J.F.; Omenaas, E.; Heinrich, J.; Svanes, C.; Garcia-Aymerich, J.; Burney, P.G.; Jarvis, D.L. Dietary antioxidants and 10-year lung function decline in adults from the ECRHS survey. Eur. Respir. J. 2017, 50, 1602286. [Google Scholar] [CrossRef] [Green Version]
- Brigham, E.P.; Steffen, L.M.; London, S.J.; Boyce, D.; Diette, G.B.; Hansel, N.N.; Rice, J.; McCormack, M.C. Diet Pattern and Respiratory Morbidity in the Atherosclerosis Risk in Communities Study. Ann. Am. Thorac. Soc. 2018, 15, 675–682. [Google Scholar] [CrossRef] [PubMed]
- Parvizian, M.K.; Dhaliwal, M.; Li, J.; Satia, I.; Kurmi, O.P. Relationship between dietary patterns and COPD: A systematic review and meta-analysis. ERJ Open Res. 2020, 6, 00168–2019. [Google Scholar] [CrossRef] [PubMed]
- Zheng, P.F.; Shu, L.; Si, C.J.; Zhang, X.Y.; Yu, X.L.; Gao, W. Dietary Patterns and Chronic Obstructive Pulmonary Disease: A Meta-analysis. COPD 2016, 13, 515–522. [Google Scholar] [CrossRef]
- Guilleminault, L.; Williams, E.J.; Scott, H.A.; Berthon, B.S.; Jensen, M.; Wood, L.G. Diet and Asthma: Is It Time to Adapt Our Message? Nutrients 2017, 9, 1227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gantenbein, K.V.; Kanaka-Gantenbein, C. Mediterranean Diet as an Antioxidant: The Impact on Metabolic Health and Overall Wellbeing. Nutrients 2021, 13, 1951. [Google Scholar] [CrossRef]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean diet and multiple health outcomes: An umbrella review of meta-analyses of observational studies and randomised trials. Eur. J. Clin. Nutr. 2018, 72, 30–43. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef]
- Martín-Luján, F.; Catalin, R.E.; Salamanca-González, P.; Sorlí-Aguilar, M.; Santigosa-Ayala, A.; Valls-Zamora, R.M.; Martín-Vergara, N.; Canela-Armengol, T.; Arija-Val, V.; Solà-Alberich, R. A clinical trial to evaluate the effect of the Mediterranean diet on smokers lung function. NPJ Prim. Care Respir. Med. 2019, 29, 40. [Google Scholar] [CrossRef] [Green Version]
- Schröder, H.; Fitó, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.; Ros, E.; Salaverría, I.; Fiol, M.; et al. A short screener is valid for assessing Mediterranean diet adherence among older Spanish men and women. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef] [Green Version]
- Graham, B.L.; Steenbruggen, I.; Miller, M.R.; Barjaktarevic, I.Z.; Cooper, B.G.; Hall, G.L.; Hallstrand, T.S.; Kaminsky, D.A.; McCarthy, K.; McCormack, M.C.; et al. Standardization of Spirometry 2019 Update. An Official American Thoracic Society and European Respiratory Society Technical Statement. Am. J. Respir. Crit. Care Med. 2019, 200, e70–e88. [Google Scholar] [CrossRef]
- Spanish Ministry of Health. Low Risk Alcohol Consumption Thresholds. Update on the Risks Related to Alcohol Consumption Levels, Consumption Patterns, and Type of Alcoholic Drink; Spanish Ministry of Health: Madrid, Spain, 2020; Available online: https://www.sanidad.gob.es/profesionales/saludPublica/prevPromocion/Prevencion/alcohol/docs/Low_Risk_Alcohol_Consumption_Thresholds_Part1.pdf (accessed on 15 February 2023).
- Sember, V.; Meh, K.; Sorić, M.; Starc, G.; Rocha, P.; Jurak, G. Validity and Reliability of International Physical Activity Questionnaires for Adults across EU Countries: Systematic Review and Meta Analysis. Int. J. Environ Res. Public Health 2020, 17, 7161. [Google Scholar] [CrossRef] [PubMed]
- van Iersel, L.E.J.; Beijers, R.J.H.C.G.; Gosker, H.R.; Schols, A.M.W.J. Nutrition as a modifiable factor in the onset and progression of pulmonary function impairment in COPD: A systematic review. Nutr. Rev. 2022, 80, 1434–1444. [Google Scholar] [CrossRef] [PubMed]
- Sorli-Aguilar, M.; Martin-Lujan, F.; Flores-Mateo, G.; Arija-Val, V.; Basora-Gallisa, J.; Sola-Alberich, R.; RESET Study Group Investigators. Dietary patterns are associated with lung function among Spanish smokers without respiratory disease. BMC Pulm Med. 2016, 16, 162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varraso, R.; Fung, T.T.; Hu, F.B.; Willett, W.; Camargo, C.A. Prospective study of dietary patterns and chronic obstructive pulmonary disease among US men. Thorax 2007, 62, 786–791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varraso, R.; Fung, T.T.; Barr, R.G.; Hu, F.B.; Willett, W.; Camargo, C.A., Jr. Prospective study of dietary patterns and chronic obstructive pulmonary disease among US women. Am. J. Clin. Nutr. 2007, 86, 488–495. [Google Scholar] [CrossRef] [Green Version]
- Shaheen, S.O.; Jameson, K.A.; Syddall, H.E.; Aihie Sayer, A.; Dennison, E.M.; Cooper, C.; Robinson, S.M.; Hertfordshire Cohort Study Group. The relationship of dietary patterns with adult lung function and COPD. Eur. Respir. J. 2010, 36, 277–284. [Google Scholar] [CrossRef] [Green Version]
- McKeever, T.M.; Lewis, S.A.; Cassano, P.A.; Ocké, M.; Burney, P.; Britton, J.; Smit, H.A. Patterns of dietary intake and relation to respiratory disease, forced expiratory volume in 1 s, and decline in 5-y forced expiratory volume. Am. J. Clin. Nutr. 2010, 92, 408–415. [Google Scholar] [CrossRef] [Green Version]
- Shin, M.K.; Kwak, S.H.; Park, Y.; Jung, J.Y.; Kim, Y.S.; Kang, Y.A. Association between Dietary Patterns and Chronic Obstructive Pulmonary Disease in Korean Adults: The Korean Genome and Epidemiology Study. Nutrients 2021, 13, 4348. [Google Scholar] [CrossRef]
- Papamichael, M.M.; Itsiopoulos, C.; Susanto, N.H.; Erbas, B. Does adherence to the Mediterranean dietary pattern reduce asthma symptoms in children? A systematic review of observational studies. Public Health Nutr. 2017, 20, 2722–2734. [Google Scholar] [CrossRef] [Green Version]
- Andrianasolo, R.M.; Kesse-Guyot, E.; Adjibade, M.; Hercberg, S.; Galan, P.; Varraso, R. Associations between dietary scores with asthma symptoms and asthma control in adults. Eur. Respir. J. 2018, 52, 1702572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulze, M.B.; Martínez-González, M.A.; Fung, T.T.; Lichtenstein, A.H.; Forouhi, N.G. Food based dietary patterns and chronic disease prevention. BMJ 2018, 361, k2396. [Google Scholar] [CrossRef] [Green Version]
- Rabe, K.F.; Watz, H. Chronic obstructive pulmonary disease. Lancet 2017, 389, 1931–1940. [Google Scholar] [CrossRef]
- Marín-Hinojosa, C.; Eraso, C.C.; Sanchez-Lopez, V.; Hernández, L.C.; Otero-Candelera, R.; Lopez-Campos, J.L. Nutriepigenomics and chronic obstructive pulmonary disease: Potential role of dietary and epigenetics factors in disease development and management. Am. J. Clin. Nutr. 2021, 114, 1894–1906. [Google Scholar] [CrossRef] [PubMed]
- Du, H.; Cao, T.; Lu, X.; Zhang, T.; Luo, B.; Li, Z. Mediterranean Diet Patterns in Relation to Lung Cancer Risk: A Meta-Analysis. Front. Nutr. 2022, 9, 844382. [Google Scholar] [CrossRef] [PubMed]
- Fischer, A.; Johansson, I.; Blomberg, A.; Sundström, B. Adherence to a Mediterranean-like Diet as a Protective Factor Against COPD: A Nested Case-Control Study. COPD 2019, 16, 272–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papassotiriou, I.; Shariful Islam, S.M. Adherence to Mediterranean Diet Is Associated With Lung Function in Older Adults: Data From the Health and Retirement Study. J. Am. Coll. Nutr. 2021, 40, 119–124. [Google Scholar] [CrossRef]
- Salamanca-González, P.; Valls-Zamora, R.M.; Pedret-Figuerola, A.; Sorlí-Aguilar, M.; Santigosa-Ayala, A.; Catalin, R.-E.; Pallejà-Millán, M.; Solà-Alberich, R.; Martin-Lujan, F.; The Cenit Research Group Investigators. Effectiveness of a Motivational Nutritional Intervention through Social Networks 2.0 to Increase Adherence to the Mediterranean Diet and Improve Lung Function in Active Smokers: The DIET Study, a Randomized, Controlled and Parallel Clinical Trial in Primary Care. Nutrients 2021, 13, 3597. [Google Scholar] [CrossRef]
- Fischer, B.M.; Voynow, J.A.; Ghio, A.J. COPD: Balancing oxidants and antioxidants. Int. J. Chron. Obstruct. Pulmon. Dis. 2015, 10, 261–276. [Google Scholar] [CrossRef] [Green Version]
- Schneider, J.L.; Rowe, J.H.; Garcia-de-Alba, C.; Kim, C.F.; Sharpe, A.H.; Haigis, M.C. The aging lung: Physiology, disease, and immunity. Cell 2021, 184, 1990–2019. [Google Scholar] [CrossRef]
- Bentley, A.R.; Kritchevsky, S.B.; Harris, T.B.; Holvoet, P.; Jensen, R.L.; Newman, A.B.; Lee, J.S.; Yende, S.; Bauer, D.; Cassano, P.A.; et al. Dietary antioxidants and forced expiratory volume in 1 s decline: The Health, Aging and Body Composition study. Eur. Respir. J. 2012, 39, 979–984. [Google Scholar] [CrossRef] [Green Version]
- Djuricic, I.; Calder, P.C. Beneficial Outcomes of Omega-6 and Omega-3 Polyunsaturated Fatty Acids on Human Health: An Update for 2021. Nutrients 2021, 13, 2421. [Google Scholar] [CrossRef]
- Cornell, K.; Alam, M.; Lyden, E.; Wood, L.; LeVan, T.D.; Nordgren, T.M.; Bailey, K.; Hanson, C. Saturated Fat Intake Is Associated with Lung Function in Individuals with Airflow Obstruction: Results from NHANES 2007–2012. Nutrients 2019, 11, 317. [Google Scholar] [CrossRef] [Green Version]
- Hooper, L.; Abdelhamid, A.; Brainard, J.; Deane, K.H.O.; Song, F.; PUFAH Group. Creation of a database to assess effects of omega-3, omega-6 and total polyunsaturated fats on health: Methodology for a set of systematic reviews. BMJ Open 2019, 9, e029554. [Google Scholar] [CrossRef] [Green Version]
- Ng, R.; Sutradhar, R.; Yao, Z.; Wodchis, W.P.; Rosella, L.C. Smoking, drinking, diet and physical activity-modifiable lifestyle risk factors and their associations with age to first chronic disease. Int. J. Epidemiol. 2020, 49, 113–130. [Google Scholar] [CrossRef] [Green Version]
- Zaninotto, P.; Head, J.; Steptoe, A. Behavioural risk factors and healthy life expectancy: Evidence from two longitudinal studies of ageing in England and the US. Sci. Rep. 2020, 10, 6955. [Google Scholar] [CrossRef] [Green Version]
- Gutiérrez-Carrasquilla, L.; Sánchez, E.; Hernández, M.; Polanco, D.; Salas-Salvadó, J.; Betriu, À.; Gaeta, A.M.; Carmona, P.; Purroy, F.; Pamplona, R.; et al. Effects of Mediterranean Diet and Physical Activity on Pulmonary Function: A Cross-Sectional Analysis in the ILERVAS Project. Nutrients 2019, 11, 329. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Aymerich, J.; Lange, P.; Serra, I.; Schnohr, P.; Antó, J.M. Time-dependent confounding in the study of the effects of regular physical activity in chronic obstructive pulmonary disease: An application of the marginal structural model. Ann. Epidemiol. 2008, 18, 775–783. [Google Scholar] [CrossRef]
- Kantorowski, A.; Wan, E.S.; Homsy, D.; Kadri, R.; Richardson, C.R.; Moy, M.L. Determinants and outcomes of change in physical activity in COPD. ERJ Open Res. 2018, 4, 00054–2018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lounassalo, I.; Salin, K.; Kankaanpää, A.; Hirvensalo, M.; Palomäki, S.; Tolvanen, A.; Yang, X.; Tammelin, T.H. Distinct trajectories of physical activity and related factors during the life course in the general population: A systematic review. BMC Public Health 2019, 19, 271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bédard, A.; Carsin, A.E.; Fuertes, E.; Accordini, S.; Dharmage, S.C.; Garcia-Larsen, V.; Heinrich, J.; Janson, C.; Johannessen, A.; Leynaert, B.; et al. Physical activity and lung function-Cause or consequence? PLoS ONE 2020, 15, e0237769. [Google Scholar] [CrossRef] [PubMed]
- Rowe, A.; Hernandez, P.; Kuhle, S.; Kirkland, S. The association between anthropometric measures and lung function in a population-based study of Canadian adults. Respir. Med. 2017, 131, 199–204. [Google Scholar] [CrossRef] [Green Version]
- Peters, U.; Suratt, B.T.; Bates, J.H.T.; Dixon, A.E. Beyond BMI: Obesity and Lung Disease. Chest 2018, 153, 702–709. [Google Scholar] [CrossRef] [PubMed]
- Carreras-Torres, R.; Johansson, M.; Haycock, P.C.; Relton, C.L.; Davey Smith, G.; Brennan, P.; Martin, R.M. Role of obesity in smoking behaviour: Mendelian randomisation study in UK Biobank. BMJ 2018, 361, k1767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, Y.; Milne, S.; Jaw, J.E.; Yang, C.X.; Xu, F.; Li, X.; Obeidat, M.; Sin, D.D. BMI is associated with FEV1 decline in chronic obstructive pulmonary disease: A meta-analysis of clinical trials. Respir. Res. 2019, 20, 236. [Google Scholar] [CrossRef] [Green Version]
- Sorlí-Aguilar, M.; Martín-Luján, F.; Flores-Mateo, G.; Jardí-Piñana, C.; Aparicio-Llopis, E.; Basora-Gallisà, J.; Solà-Alberich, R. Adiposity markers and lung function in smokers: A cross-sectional study in a Mediterranean population. BMC Pulm. Med. 2016, 16, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.Y.; Yang, H.K.; Song, H.J.; Chang, H.J.; Kang, J.Y.; Lee, S.H.; Han, S.; Kim, Y.K. Metabolic health is more closely associated with decrease in lung function than obesity. PLoS ONE 2019, 14, e0209575. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Kwon, D.; Lee, Y.; Jung, I.; Hyun, D.; Lee, H.; Ahn, Y.S. Hypertension Is Associated with Increased Risk of Diabetic Lung. Int. J. Environ. Res. Public Health 2020, 17, 7513. [Google Scholar] [CrossRef]
- Wang, Y.; Li, Z.; Li, F. Nonlinear relationship between visceral adiposity index and lung function: A population-based study. Respir. Res. 2021, 22, 161. [Google Scholar] [CrossRef] [PubMed]
- Primeau, V.; Coderre, L.; Karelis, A.D.; Brochu, M.; Lavoie, M.E.; Messier, V.; Sladek, R.; Rabasa-Lhoret, R. Characterizing the profile of obese patients who are metabolically healthy. Int. J. Obes. 2011, 90, 971–981. [Google Scholar] [CrossRef] [Green Version]
- Steinemann, N.; Grize, L.; Pons, M.; Rothe, T.; Stolz, D.; Turk, A.; Schindler, C.; Brombach, C.; Probst-Hensch, N. Associations between Dietary Patterns and Post-Bronchodilation Lung Function in the SAPALDIA Cohort. Respiration 2018, 95, 454–463. [Google Scholar] [CrossRef]
- Thomas, E.T.; Guppy, M.; Straus, S.E.; Bell, K.J.L.; Glasziou, P. Rate of normal lung function decline in ageing adults: A systematic review of prospective cohort studies. BMJ Open 2019, 9, e028150. [Google Scholar] [CrossRef] [PubMed]
- Fenger, R.V.; Gonzalez-Quintela, A.; Vidal, C.; Husemoen, L.L.; Skaaby, T.; Thuesen, B.H.; Aadahl, M.; Madsen, F.; Linneberg, A. The longitudinal relationship of changes of adiposity to changes in pulmonary function and risk of asthma in a general adult population. BMC Pulm. Med. 2014, 14, 208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.A.; Joshi, P.; Kim, Y.; Kang, D.; Kim, W.J. The Association of Dietary Macronutrients with Lung Function in Healthy Adults Using the Ansan-Ansung Cohort Study. Nutrients 2020, 12, 2688. [Google Scholar] [CrossRef] [PubMed]
- Okubo, H.; Shaheen, S.O.; Ntani, G.; Jameson, K.A.; Syddall, H.E.; Sayer, A.A.; Dennison, E.M.; Cooper, C.; Robinson, S.M.; Hertfordshire Cohort Study Group. Processed meat consumption and lung function: Modification by antioxidants and smoking. Eur. Respir. J. 2014, 43, 972–982. [Google Scholar] [CrossRef] [Green Version]
- Rocha, V.; Fraga, S.; Moreira, C.; Carmeli, C.; Lenoir, A.; Steptoe, A.; Giles, G.; Goldberg, M.; Zins, M.; Kivimäki, M.; et al. Life-course socioeconomic disadvantage and lung function: A multicohort study of 70,496 individuals. Eur. Respir. J. 2021, 57, 2001600. [Google Scholar] [CrossRef]
- Rocha, V.; Stringhini, S.; Henriques, A.; Falcão, H.; Barros, H.; Fraga, S. Life-course socioeconomic status and lung function in adulthood: A study in the EPIPorto cohort. J. Epidemiol. Community Health 2020, 74, 290–297. [Google Scholar] [CrossRef]
- Cespedes, E.M.; Hu, F.B. Dietary patterns: From nutritional epidemiologic analysis to national guidelines. Am. J. Clin. Nutr. 2015, 101, 899–900. [Google Scholar] [CrossRef] [Green Version]
- Leng, S.; Picchi, M.A.; Tesfaigzi, Y.; Wu, G.; Gauderman, W.J.; Xu, F.; Gilliland, F.D.; Belinsky, S.A. Dietary nutrients associated with preservation of lung function in Hispanic and non-Hispanic white smokers from New Mexico. Int. J. Chron. Obstruct. Pulm. Dis. 2017, 12, 3171–3181. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Total | Low Adherence | Medium Adherence | High Adherence | p Value | |
|---|---|---|---|---|---|
| (n = 403) | (n = 96) | (n = 161) | (n = 146) | ||
| Socio-demographics | |||||
| Sex, woman | 266 (66.0%) | 64 (66.7%) | 105 (65.2%) | 97 (66.4%) | 0.9603 |
| Age | 51.1 (10.1) | 49.8 (10.4) | 51 (10.3) | 52.2 (9.66) | 0.188 |
| Employment status | 0.593 | ||||
| Working | 256 (64.2%) | 57 (59.4%) | 104 (65.4%) | 95 (66.0%) | |
| Unemployed | 33 (8.3%) | 8 (8.3%) | 17 (10.7%) | 8 (5.5%) | |
| Working at home | 72 (18.0%) | 21 (21.9%) | 24 (15.1%) | 27 (18.8%) | |
| Student | 38 (9.5%) | 10 (10.4%) | 14 (8.8%) | 14 (9.7%) | |
| Marital status | 0.484 | ||||
| Single | 87 (21.6%) | 19 (19.8%) | 42 (26.1%) | 26 (17.8%) | |
| Married | 271 (67.2%) | 66 (68.8%) | 103 (64.0%) | 102 (69.9%) | |
| Divorced/Windowed | 45 (11.2%) | 11 (11.5%) | 16 (9.9%) | 18 (12.3%) | |
| Education level | 0.068 | ||||
| Doesn’t know to read or write | 75 (18.7%) | 14 (14.6%) | 34 (21.1%) | 27 (18.6%) | |
| Primary Studies | 142 (35.3%) | 45 (46.9%) | 51 (31.7%) | 46 (31.7%) | |
| Secondary Studies | 141 (35.1%) | 28 (29.2%) | 53 (32.9%) | 60 (41.4%) | |
| University Studies | 44 (10.9%) | 9 (9.3%) | 23 (14.3%) | 12 (8.2%) | |
| Health Habits | |||||
| Smoking age, years | 17 [15.0; 20.0] | 17 [15.0; 20.0] | 16 [15.0; 19.0] | 16 [15.0; 20.0] | 0.548 |
| Current consumption, cigarettes/day | 23.0 [15.0; 34.0] | 20,3 [12.9; 34.0] | 25 [15.0; 34.0] | 21.5 [15.0; 34.0] | 0.150 |
| Accumulated consumption, packs-year | 23.0 [15.0; 34.0] | 20.3 [12.9; 34.0] | 25 [15.0; 34.0] | 21.5 [15.0; 34.0] | 0.150 |
| Alcohol consumption, | 58.6% | 52.1% | 55.3% | 66.4% | 0.048 |
| Alcohol intake, SDU/week | 4.88 (6.8) | 4.28 (6.7) | 4.96 (8.1) | 5.11 (5.6) | 0.780 |
| Physical activity, IPAQ categorization | 0.185 | ||||
| Inactive | 33 (8.2%) | 10 (10.4%) | 12 (7.4%) | 11 (7.5%) | |
| Low | 142 (35.2%) | 42 (43.8%) | 50 (31.1%) | 50 (34.2%) | |
| Moderate | 204 (50.6%) | 41 (42.7%) | 85 (52.8%) | 78 (53.5%) | |
| High | 24 (6.0%) | 3 (3.1%) | 14 (8.7%) | 7 (4.8%) | |
| Pathological history | |||||
| Cardiovascular disease | 18 (4.4%) | 6 (6.2%) | 6 (3.7%) | 6 (4.1%) | 0.052 |
| Oncologic disease | 25 (6.2%) | 12 (12.5%) | 8 (4.9%) | 5 (3.4%) | 0.012 |
| Circulatory disease | 59 (14.6%) | 20 (20.8%) | 24 (14.9%) | 15 (10.3%) | 0.075 |
| Endocrinological disease | 91 (22.6%) | 30 (31.2%) | 33 (20.5%) | 28 (19.2%) | 0.064 |
| Exploratory parameters | |||||
| Weight, kg | 70 [61.0; 82.0] | 68 [59.0; 80.2] | 69 [59.0; 83.0] | 72 [63.0; 83.0] | 0.222 |
| BMI, Kg/m2 | 27.0 (5.1) | 26.9 (4.6) | 26.6 (5.3) | 27.6 (5.2) | 0.187 |
| WC, cm | 90.9 (15.3) | 91.1 (14.5) | 89.2 (14.8) | 92.5 (16.2) | 0.244 |
| SBP, mmHg | 125 (15.3) | 123 (14.5) | 124 (14.7) | 127 (16.4) | 0.147 |
| DBP, mmHg | 77.5 (9.4) | 76.7 (10.3) | 77.5 (8.8) | 78 (9.6) | 0.658 |
| Laboratory data | |||||
| Glucose, mg/dL | 87.3 [80.0; 102.0] | 86.0 [80.0; 102.0] | 88.3 [80.0; 106.0] | 87.4 [81.0; 99.0] | 0.512 |
| Total cholesterol, mg/dL | 213 (45.6) | 208 (41.8) | 219 (47.5) | 209 (45.4) | 0.088 |
| LDL Cholesterol, mg/dL | 127 (35.4) | 124 (35.8) | 133 (34.5) | 123 (35.6) | 0.035 |
| HDL Cholesterol, mg/dL | 61.8 (17.6) | 60.8 (16.0) | 62 (18.0) | 62.1 (18.2) | 0.835 |
| Triglycerides, mg/dL | 128 [98.0; 179.0] | 118 [91.5; 156.0] | 146 [105.0; 189.0] | 126 [99.9; 173.0] | 0.070 |
| Haemoglobin, g/dL | 14.0 [12.9; 14.8] | 14.2 [12.9; 14.8] | 14.2 [13.0; 14.8] | 13.8 [12.9; 14.8] | 0.532 |
| Haematocrit, % | 42.1 [39.2; 44.7] | 42.3 [39.2; 45.2] | 42.3 [39.7; 44.8] | 41.8 [39.0; 44.0] | 0.168 |
| Erythrocytes, 106/mm3 | 4.4 [4.2; 4.6] | 4.4 [4.2; 4.6] | 4.4 [4.3:4.6] | 4.4 [4.2; 4.5] | 0.173 |
| Total | Low Adherence | Medium Adherence | High Adherence | p Value | |
|---|---|---|---|---|---|
| (n = 403) | (n = 96) | (n = 161) | (n = 146) | ||
| Pulmonary values | |||||
| FEV1, L | 2.7 (0.7) | 2.7 (0.7) | 2.7 (0.7) | 2.7 (0.7) | 0.982 |
| FEV1, %predicted | 92.6 (17.4) | 90.8 (17.6) | 93.7 (17.7) | 92.6 (17.0) | 0.433 |
| FVC, L | 3.5 (0.9) | 3.5 (0.9) | 3.5 (0.8) | 3.51 (0.9) | 0.973 |
| FVC, %predicted | 90.3 (16.0) | 88.2 (15.8) | 91.5 (15.9) | 90.4 (16.2) | 0.270 |
| Impaired lung function (a) | |||||
| Impaired FEV1 | 85 (21.1%) | 27 (28.1%) | 30 (18.6%) | 28 (19.2%) | 0.153 |
| Impaired FVC | 105 (26.1%) | 33 (34.4%) | 33 (20.5%) | 39 (26.7%) | 0.048 |
| Impaired FEV1 and/or FVC | 116 (28.8%) | 37 (38.5%) | 39 (24.2%) | 40 (27.4%) | 0.044 |
| Types of ventilatory patterns (b) | |||||
| Normal spirometry | 287 (71.2%) | 59 (61.5%) | 122 (75.8%) | 106 (72.6%) | 0.044 |
| Spirometric abnormality pattern | 0.906 | ||||
| Obstructive | 50 (12.4%) | 17 (17.7%) | 16 (9.9%) | 17 (11.6%) | |
| Non-obstructive | 66 (16.4%) | 20 (20.8%) | 23 (14.3%) | 23 (15.8%) | |
| Impaired FEV1 | Impaired FVC | Impaired FEV1 and/or FVC | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | p Value | OR (95% CI) | p Value | OR (95% CI) | p Value | |
| Unadjusted model | ||||||
| Mediterranean Diet Adherence * | ||||||
| low | reference | reference | reference | |||
| medium | 0.585 (0.322–1.062) | 0.078 | 0.492 (0.279–0.869) | 0.015 | 0.510 (0.416–0.946) | 0.016 |
| high | 0.606 (0.331–1.112) | 0.106 | 0.696 (0.398–1.216) | 0.203 | 0.602 (0.348–1.042) | 0.070 |
| Age/sex adjusted model | ||||||
| Mediterranean Diet Adherence * | ||||||
| low | reference | reference | reference | |||
| medium | 0.565 (0.309–1.031) | 0.063 | 0.465 (0.261–0.831) | 0.010 | 0.477 (0.273–0.835) | 0.009 |
| high | 0.575 (0.311–1.063) | 0.078 | 0.648 (0.366–1.146) | 0.136 | 0.550 (0.313–0.968) | 0.038 |
| Sex (women) | 0.644 (0.392–1.057) | 0.082 | 0.572 (0.359–0.912) | 0.019 | 0.554 (0.351–0.872) | 0.011 |
| Age (years) | 1.019 (0.994–1.043) | 0.134 | 1.025 (1.002–1.048) | 0.135 | 1.029 (1.006–1.052) | 0.013 |
| Multivariable adjusted model | ||||||
| Mediterranean Diet Adherence * | ||||||
| low | reference | reference | reference | |||
| medium | 0.582 (0.316–1.074) | 0.083 | 0.475 (0.265–0.851) | 0.012 | 0.487 (0.277–0.856) | 0.012 |
| high | 0.590 (0.317–1.097) | 0.095 | 0.643 (0.363–1.141) | 0.131 | 0.556 (0.315–0.979) | 0.042 |
| Sex (women) | 0.648 (0.390–1.078) | 0.095 | 0.587 (0.366–0.940) | 0.027 | 0.565 (0.356–0.896) | 0.015 |
| Age (years) | 1.017 (0.993–1.042) | 0.172 | 1.023 (1.000–1.047) | 0.048 | 1.027 (1.004–1.050) | 0.019 |
| BMI (kg/m2) | 1.002 (0.954–1.051) | 0.950 | 1.020 (0.976–1.067) | 0.383 | 1.011 (0.968–1.056) | 0.616 |
| Smoking current consumption | ||||||
| Daily consumption (min, 10] cigarettes | reference | reference | reference | |||
| Daily consumption (10, 20] cigarettes | 0.764 (0.449–1.301) | 0.322 | 0.900 (0.552–1.469) | 0.674 | 0.886 (0.548–1.432) | 0.621 |
| Daily consumption (20, max] cigarettes | 2.051 (0.936–4.495) | 0.073 | 1.044 (0.461–2.365) | 0.917 | 1.532 (0.709–3.310) | 0.278 |
| FEV1% Predicted Value | FVC% Predicted Value | |||
|---|---|---|---|---|
| β Regression Coefficient (95% CI) | p Value | β Regression Coefficient (95% CI) | p Value | |
| Unadjusted Model | ||||
| Mediterranean Diet Adherence * | ||||
| low | reference | reference | ||
| medium | 2.906 (−1.507; 7.319) | 0.196 | 3.332 (−0.716; 7.379) | 0.106 |
| high | 1.873 (−2.623; 6.370) | 0.413 | 2.239 (−1.885; 6.364) | 0.286 |
| Age/sex adjusted model | ||||
| Mediterranean Diet Adherence * | ||||
| low | reference | reference | ||
| medium | 3.044 (−1.139; 7.427) | 0.173 | 3.629 (−0.341; 7.599) | 0.073 |
| high | 2.005 (−2.474; 6.484) | 0.379 | 2.651 (−1.407; 6.708) | 0.200 |
| Sex (women) | 5.142 (1.566; 8.718) | 0.005 | 6.029 (2.789; 9.268) | <0.001 |
| Age (years) | −0.050 (−0.218; 0.119) | 0.564 | −0.165 (−0.317; −0.012) | 0.035 |
| Multivariable adjusted model | ||||
| Mediterranean Diet Adherence * | ||||
| low | reference | reference | ||
| medium | 3.203 (−1.133; 7.540) | 0.145 | 3.660 (−0.285; 7.605) | 0.069 |
| high | 1.481 (−2.955; 5.918) | 0.487 | 2.239 (−1.786; 6.264) | 0.275 |
| Sex (women) | 5.870 (2.212; 9.529) | 0.002 | 6.220 (2.893; 9.546) | 0.000 |
| Smoking cumulative consumption (pack-year) | −0.142 (−0.272; −0.038) | 0.008 | −0.143 (−0.239; −0.048) | 0.003 |
| BMI (Kg/m2) | 0.975 | −0.193 (−0.494; 0.109) | 0.209 | |
| Alcohol intake (SDU/week) | 0.374 (0.074; 0.675) | 0.013 | 0.244 (−0.028; 0.517) | 0.079 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Catalin, R.-E.; Martin-Lujan, F.; Salamanca-Gonzalez, P.; Palleja-Millan, M.; Villalobos, F.; Santigosa-Ayala, A.; Pedret, A.; Valls-Zamora, R.M.; Sola, R.; on behalf of the MEDISTAR Research Group Investigators. Mediterranean Diet and Lung Function in Adults Current Smokers: A Cross-Sectional Analysis in the MEDISTAR Project. Nutrients 2023, 15, 1272. https://doi.org/10.3390/nu15051272
Catalin R-E, Martin-Lujan F, Salamanca-Gonzalez P, Palleja-Millan M, Villalobos F, Santigosa-Ayala A, Pedret A, Valls-Zamora RM, Sola R, on behalf of the MEDISTAR Research Group Investigators. Mediterranean Diet and Lung Function in Adults Current Smokers: A Cross-Sectional Analysis in the MEDISTAR Project. Nutrients. 2023; 15(5):1272. https://doi.org/10.3390/nu15051272
Chicago/Turabian StyleCatalin, Roxana-Elena, Francisco Martin-Lujan, Patricia Salamanca-Gonzalez, Meritxell Palleja-Millan, Felipe Villalobos, Antoni Santigosa-Ayala, Anna Pedret, Rosa M. Valls-Zamora, Rosa Sola, and on behalf of the MEDISTAR Research Group Investigators. 2023. "Mediterranean Diet and Lung Function in Adults Current Smokers: A Cross-Sectional Analysis in the MEDISTAR Project" Nutrients 15, no. 5: 1272. https://doi.org/10.3390/nu15051272