
Gender Differences in Vitamin D Status and Determinants of Vitamin D Insufficiency in Patients with Chronic Obstructive Pulmonary Disease

Abstract
:1. Introduction
2. Materials and Methods
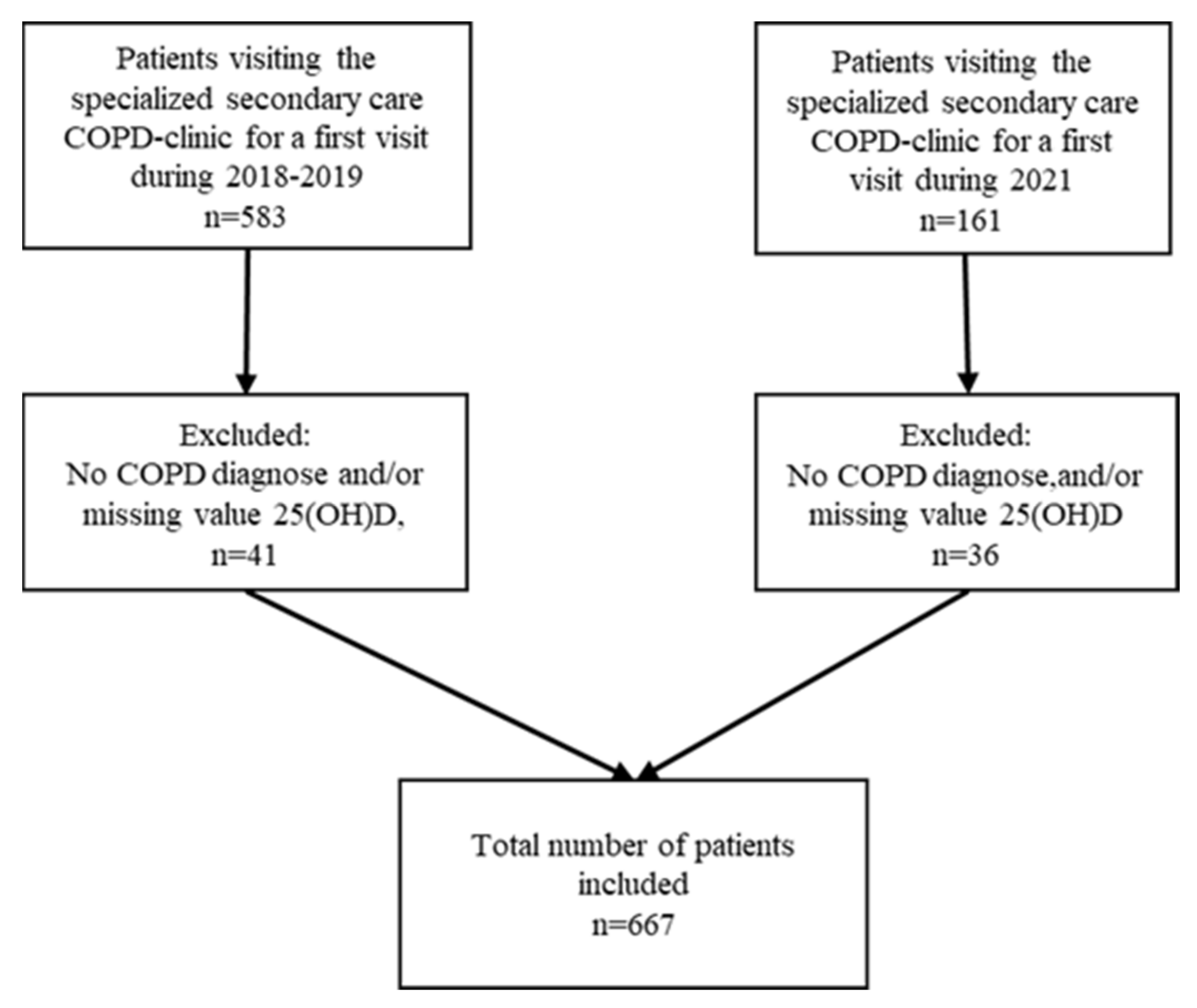
2.1. Enrollment and Data Collection
2.2. Statistical Analyses
3. Results
3.1. Patient Characteristics
3.2. Vitamin D Supplementation
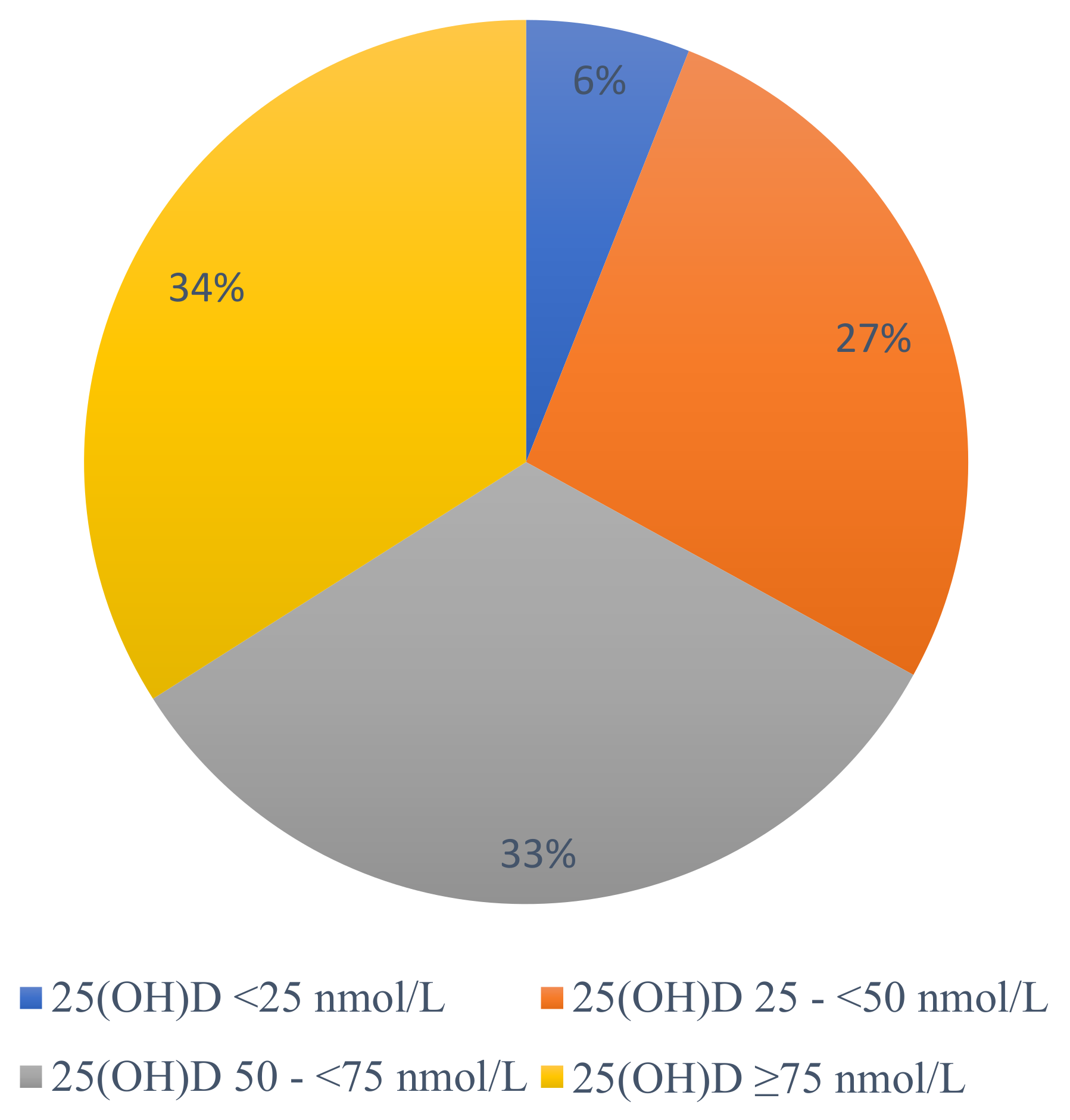
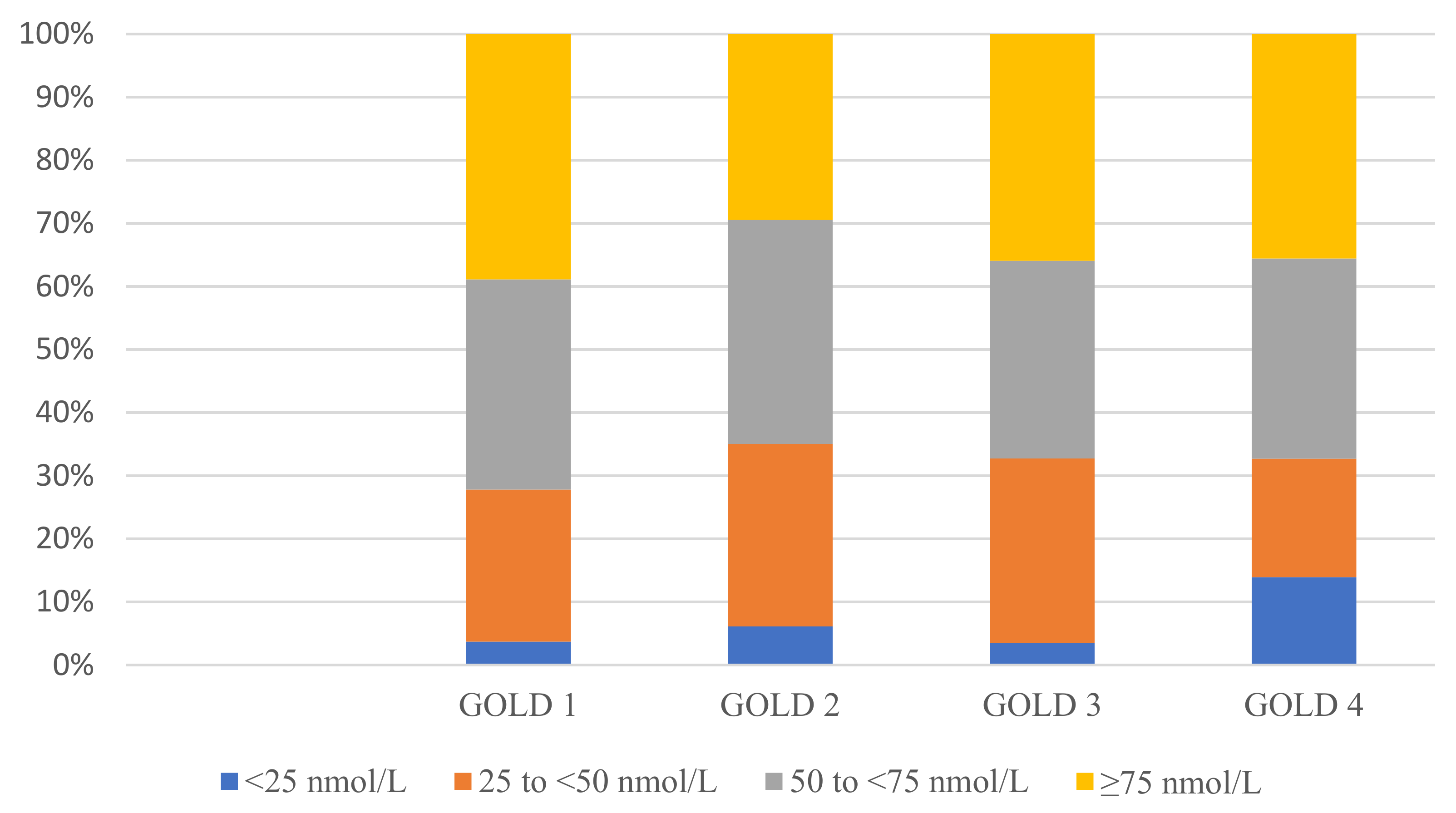
3.3. Vitamin D Status
3.4. Seasonal Variations
3.5. Factors Associated with Vitamin D Insufficiency
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Manegement, and Prevention of Chronic Obstructive Pulmonary Disease (2022 Report). Available online: https://goldcopd.org/2022-gold-reports-2/ (accessed on 11 February 2022).
- Varmaghani, M.; Dehghani, M.; Heidari, E.; Sharifi, F.; Moghaddam, S.S.; Farzadfar, F. Global prevalence of chronic obstructive pulmonary disease: Systematic review and meta-analysis. East. Mediterr. Health J. 2019, 25, 47–57. [Google Scholar] [CrossRef] [PubMed]
- Vanfleteren, L.; Spruit, M.A.; Wouters, E.F.M.; Franssen, F.M.E. Management of chronic obstructive pulmonary disease beyond the lungs. Lancet Respir Med. 2016, 4, 911–924. [Google Scholar] [CrossRef] [PubMed]
- Vanfleteren, L.E.; Spruit, M.A.; Groenen, M.; Gaffron, S.; van Empel, V.P.; Bruijnzeel, P.L.; Rutten, E.P.; Op ’t Roodt, J.; Wouters, E.F.; Franssen, F.M. Clusters of comorbidities based on validated objective measurements and systemic inflammation in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2013, 187, 728–735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carson, E.L.; Pourshahidi, L.K.; Madigan, S.M.; Baldrick, F.R.; Kelly, M.G.; Laird, E.; Healy, M.; Strain, J.J.; Mulhern, M.S. Vitamin D status is associated with muscle strength and quality of life in patients with COPD: A seasonal prospective observation study. Int. J. Chron. Obstruct. Pulmon. Dis. 2018, 13, 2613–2622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graumam, R.Q.; Pinheiro, M.M.; Nery, L.E.; Castro, C.H.M. Increased rate of osteoporosis, low lean mass, and fragility fractures in COPD patients: Association with disease severity. Osteoporos. Int. 2018, 29, 1457–1468. [Google Scholar] [CrossRef] [PubMed]
- Mete, B.; Pehlivan, E.; Gülbaş, G.; Günen, H. Prevalence of malnutrition in COPD and its relationship with the parameters related to disease severity. Int. J. Chron. Obstruct. Pulmon. Dis. 2018, 13, 3307–3312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, M.; Wang, T.; Wang, C.; Ji, Y. The association between vitamin D and COPD risk, severity, and exacerbation: An updated systematic review and meta-analysis. Int. J. Chron. Obstruct. Pulmon. Dis. 2016, 11, 2597–2607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jolliffe, D.A.; James, W.Y.; Hooper, R.L.; Barnes, N.C.; Greiller, C.L.; Islam, K.; Bhowmik, A.; Timms, P.M.; Rajakulasingam, R.K.; Choudhury, A.B.; et al. Prevalence, determinants and clinical correlates of vitamin D deficiency in patients with Chronic Obstructive Pulmonary Disease in London, UK. J. Steroid Biochem. Mol. Biol. 2018, 175, 138–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jorde, I.; Stegemann-Koniszewski, S.; Papra, K.; Föllner, S.; Lux, A.; Schreiber, J.; Lücke, E. Association of serum vitamin D levels with disease severity, systemic inflammation, prior lung function loss and exacerbations in a cohort of patients with chronic obstructive pulmonary disease (COPD). J. Thorac. Dis. 2021, 13, 3597–3609. [Google Scholar] [CrossRef]
- Holmgaard, D.B.; Mygind, L.H.; Titlestad, I.L.; Madsen, H.; Fruekilde, P.B.; Pedersen, S.S.; Pedersen, C. Serum vitamin D in patients with chronic obstructive lung disease does not correlate with mortality—Results from a 10-year prospective cohort study. PLoS ONE 2013, 8, e53670. [Google Scholar] [CrossRef] [PubMed]
- Persson, L.J.; Aanerud, M.; Hiemstra, P.S.; Hardie, J.A.; Bakke, P.S.; Eagan, T.M. Chronic obstructive pulmonary disease is associated with low levels of vitamin D. PLoS ONE 2012, 7, e38934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Måhlin, C.; von Sydow, H.; Osmancevic, A.; Emtner, M.; Grönberg, A.M.; Larsson, S.; Slinde, F. Vitamin D status and dietary intake in a Swedish COPD population. Clin. Respir. J. 2014, 8, 24–32. [Google Scholar] [CrossRef]
- Janssens, W.; Bouillon, R.; Claes, B.; Carremans, C.; Lehouck, A.; Buysschaert, I.; Coolen, J.; Mathieu, C.; Decramer, M.; Lambrechts, D. Vitamin D deficiency is highly prevalent in COPD and correlates with variants in the vitamin D-binding gene. Thorax 2010, 65, 215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burkes, R.M.; Ceppe, A.S.; Doerschuk, C.M.; Couper, D.; Hoffman, E.A.; Comellas, A.P.; Barr, R.G.; Krishnan, J.A.; Cooper, C.; Labaki, W.W.; et al. Associations Among 25-Hydroxyvitamin D Levels, Lung Function, and Exacerbation Outcomes in COPD: An Analysis of the SPIROMICS Cohort. Chest 2020, 157, 856–865. [Google Scholar] [CrossRef] [PubMed]
- Charoenngam, N.; Holick, M.F. Immunologic Effects of Vitamin D on Human Health and Disease. Nutrients 2020, 12, 2097. [Google Scholar] [CrossRef] [PubMed]
- Herr, C.; Greulich, T.; Koczulla, R.A.; Meyer, S.; Zakharkina, T.; Branscheidt, M.; Eschmann, R.; Bals, R. The role of vitamin D in pulmonary disease: COPD, asthma, infection, and cancer. Respir. Res. 2011, 12, 31. [Google Scholar] [CrossRef] [Green Version]
- Black, P.N.; Scragg, R. Relationship Between Serum 25-Hydroxyvitamin D and Pulmonary Function in the Third National Health and Nutrition Examination Survey. Chest 2005, 128, 3792–3798. [Google Scholar] [CrossRef] [Green Version]
- Ginde, A.A.; Mansbach, J.M.; Camargo, C.A., Jr. Association between serum 25-hydroxyvitamin D level and upper respiratory tract infection in the Third National Health and Nutrition Examination Survey. Arch. Intern. Med. 2009, 169, 384–390. [Google Scholar] [CrossRef] [Green Version]
- Monlezun, D.J.; Bittner, E.A.; Christopher, K.B.; Camargo, C.A.; Quraishi, S.A. Vitamin D Status and Acute Respiratory Infection: Cross Sectional Results from the United States National Health and Nutrition Examination Survey, 2001–2006. Nutrients 2015, 7, 1933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallelli, L.; Mannino, G.C.; Luciani, F.; de Sire, A.; Mancuso, E.; Gangemi, P.; Cosco, L.; Monea, G.; Averta, C.; Minchella, P.; et al. Vitamin D Serum Levels in Subjects Tested for SARS-CoV-2: What Are the Differences among Acute, Healed, and Negative COVID-19 Patients? A Multicenter Real-Practice Study. Nutrients 2021, 13, 3932. [Google Scholar] [CrossRef] [PubMed]
- Ulucoban, H.; Dirol, H.; Ozdemir, T. The Effect of Vitamin D Deficiency in Chronic Obstructive Pulmonary Disease. Turk. Thorac. J. 2021, 22, 242–246. [Google Scholar] [CrossRef] [PubMed]
- Janssens, W.; Lehouck, A.; Carremans, C.; Bouillon, R.; Mathieu, C.; Decramer, M. Vitamin D beyond bones in chronic obstructive pulmonary disease: Time to act. Am. J. Respir. Crit. Care Med. 2009, 179, 630–636. [Google Scholar] [CrossRef] [Green Version]
- Charoenngam, N.; Shirvani, A.; Holick, M.F. Vitamin D for skeletal and non-skeletal health: What we should know. J. Clin. Orthop. Trauma 2019, 10, 1082–1093. [Google Scholar] [CrossRef] [PubMed]
- Nordic Council of Ministers. Nordic Nutrition Recommendations 2012, Integrating Nutrition and Physical Activity; Nordisk Ministerråd: Copenhagen, Denmark, 2014; Volume 5, pp. 349–356. [Google Scholar]
- WHO. A Healthy Lifestyle—WHO Recommendations. Available online: https://www.who.int/europe/news-room/fact-sheets/item/a-healthy-lifestyle---who-recommendations (accessed on 1 October 2022).
- Norden, J.; Gronberg, A.; Slinde, F. Utveckling av verktyget för bedömning av risk för undernäring hos patienter med KOL. Lung Allergiforum 2013, 2, 13–16. [Google Scholar]
- Jones, P.W.; Harding, G.; Berry, P.; Wiklund, I.; Chen, W.H.; Kline Leidy, N. Development and first validation of the COPD Assessment Test. Eur. Respir. J. 2009, 34, 648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hedenström, H.; Malmberg, P.; Agarwal, K. Reference values for lung function tests in females. Regression equations with smoking variables. Bull. Eur. Physiopathol. Respir. 1985, 21, 551–557. [Google Scholar] [PubMed]
- Hedenström, H.; Malmberg, P.; Fridriksson, H.V. Reference values for lung function tests in men: Regression equations with smoking variables. Ups J. Med. Sci. 1986, 91, 299–310. [Google Scholar] [CrossRef] [Green Version]
- Jones, P.W.; Brusselle, G.; Dal Negro, R.W.; Ferrer, M.; Kardos, P.; Levy, M.L.; Perez, T.; Soler Cataluña, J.J.; van der Molen, T.; Adamek, L.; et al. Properties of the COPD assessment test in a cross-sectional European study. Eur. Respir. J. 2011, 38, 29. [Google Scholar] [CrossRef] [Green Version]
- Lips, P.; Cashman, K.D.; Lamberg-Allardt, C.; Bischoff-Ferrari, H.A.; Obermayer-Pietsch, B.; Bianchi, M.L.; Stepan, J.; El-Hajj Fuleihan, G.; Bouillon, R. Current vitamin D status in European and Middle East countries and strategies to prevent vitamin D deficiency: A position statement of the European Calcified Tissue Society. Eur. J. Endocrinol. 2019, 180, P23–P54. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.Y.; Shin, S.H.; Choi, H.S.; Im, Y.; Kim, B.G.; Song, J.Y.; Lee, D.; Park, H.Y.; Lim, J.H. Association Between Vitamin D Level and Respiratory Symptoms in Patients with Stable Chronic Obstructive Pulmonary Disease. Int. J. Chron. Obstruct. Pulmon. Dis. 2022, 17, 579–590. [Google Scholar] [CrossRef]
- Melhus, H.; Snellman, G.; Gedeborg, R.; Byberg, L.; Berglund, L.; Mallmin, H.; Hellman, P.; Blomhoff, R.; Hagström, E.; Arnlöv, J.; et al. Plasma 25-hydroxyvitamin D levels and fracture risk in a community-based cohort of elderly men in Sweden. J. Clin. Endocrinol. Metab. 2010, 95, 2637–2645. [Google Scholar] [CrossRef] [PubMed]
- Livsmedelsverket. D-Vitamin. Available online: https://www.livsmedelsverket.se/livsmedel-och-innehall/naringsamne/vitaminer-och-antioxidanter/d-vitamin (accessed on 7 October 2022).
- Livsmedelsverket. LIVSFS 2018:5. Available online: https://kontrollwiki.livsmedelsverket.se/lagstiftning/402/livsfs-2018-5 (accessed on 13 October 2022).
- Kentson, M.; Leanderson, P.; Jacobson, P.; Persson, H.L. The influence of disease severity and lifestyle factors on the peak annual 25(OH)D value of COPD patients. Int. J. Chron. Obstruct. Pulmon. Dis. 2018, 13, 1389–1398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Martinis, M.; Sirufo, M.M.; Polsinelli, M.; Placidi, G.; Di Silvestre, D.; Ginaldi, L. Gender Differences in Osteoporosis: A Single-Center Observational Study. World J. Mens Health 2021, 39, 750–759. [Google Scholar] [CrossRef] [PubMed]
- De Sire, A.; Lippi, L.; Aprile, V.; Calafiore, D.; Folli, A.; D’Abrosca, F.; Moalli, S.; Lucchi, M.; Ammendolia, A.; Invernizzi, M. Pharmacological, Nutritional, and Rehabilitative Interventions to Improve the Complex Management of Osteoporosis in Patients with Chronic Obstructive Pulmonary Disease: A Narrative Review. J. Pers. Med. 2022, 12, 1626. [Google Scholar] [CrossRef]
- Lippi, L.; Folli, A.; Curci, C.; D’Abrosca, F.; Moalli, S.; Mezian, K.; de Sire, A.; Invernizzi, M. Osteosarcopenia in Patients with Chronic Obstructive Pulmonary Diseases: Which Pathophysiologic Implications for Rehabilitation? Int. J. Environ. Res. Public Health 2022, 19, 14314. [Google Scholar] [CrossRef] [PubMed]
- Pitta, F.; Troosters, T.; Spruit, M.A.; Probst, V.S.; Decramer, M.; Gosselink, R. Characteristics of physical activities in daily life in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2005, 171, 972–977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scoditti, E.; Massaro, M.; Garbarino, S.; Toraldo, D.M. Role of Diet in Chronic Obstructive Pulmonary Disease Prevention and Treatment. Nutrients 2019, 11, 1357. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total | Women | Men | p-Value | Vitamin D Insufficiency | Vitamin D Sufficiency | p-Value | |
|---|---|---|---|---|---|---|---|
| Patients, n (%) | 667 | 394 (59) | 273 (41) | 221 (33) | 446 (67) | ||
| Sex, n (%) | |||||||
| Male | 273 (41) | 113 (51) | 160 (36) | < 0.001 * | |||
| Age, median (Q1–Q3) | 73 (66–79) | 73 (67–79) | 72 (66–78) | 0.520 2 | 73 (66–79) | 73 (67–79) | 0.757 2 |
| BMI, kg/m2, median (Q1–Q3) | 25.7 (21.9–30) | 25.6 (21.4–30.4) | 26 (22.5–29.4) | 0.306 2 | 26 (22.6–30.7) | 25.5 (21.6–29.8) | 0.118 2 |
| Current smoking, n (%) | 189 (28) | 107 (57) | 82 (43) | 0.395 1 | 73 (33) | 116 (26) | 0.055 1 |
| FEV1 % predicted, n = 632 | |||||||
| median (Q1–Q3) | 47 (36–62) | 47 (36–61) | 49 (35–63) | 0.569 2 | 48 (36–60) | 47 (36–62) | 0.866 2 |
| GOLD grade, n (%) | |||||||
| 1 | 54 (8) | 28 (7) | 26 (10) | 0.439 1 | 15 (7) | 39 (9) | 0.772 1 |
| 2 | 228 (34) | 134 (34) | 94 (34) | 80 (36) | 148 (33) | ||
| 3 | 284 (43) | 176 (45) | 108 (40) | 93 (42) | 191 (43) | ||
| 4 | 101 (15) | 56 (14) | 45 (16) | 33 (15) | 68 (15) | ||
| CAT score, | |||||||
| median (Q1–Q3) | 20 (14–25) | 21 (15–25) | 19 (14–25) | 0.085 2 | 21 (15–26) | 20 (14–25) | 0.096 2 |
| Risk of malnutrition, n (%) | 209 (34) | 136 (37) | 73 (29) | 0.036 1 | 61 (30) | 148 (36) | 0.143 1 |
| 25(OH)D, nmol/L, | |||||||
| median (Q1–Q3) | 62 (43.5–83.1) | 65.3 (47.3–87.6) | 55 (40.7–77.7) | < 0.001 2* | 36.7 (29.7–43.4) | 75 (62–94.3) | < 0.001 2* |
| Documented vitamin D | |||||||
| supplementation, n (%) | 169 (26) | 132 (34) | 37 (14) | < 0.001 1* | 22 (10) | 147 (33) | < 0.001 1* |
| Season, n (%) | |||||||
| Summer | 345 (52) | 199 (58) | 146 (42) | 0.450 1 | 91 (41) | 254 (57) | < 0.001 1* |
| Winter | 322 (48) | 195 (61) | 127 (39) | 130 (59) | 192 (43) |
| Coefficient | OR | 95% CI | p-Value |
|---|---|---|---|
| Age | 1.01 | 0.99–1.03 | 0.201 |
| Gender | 1.64 | 1.14–2.35 | 0.007 * |
| BMI | 1.01 | 0.98–1.04 | 0.448 |
| FEV1 % predicted | 1.00 | 0.99–1.01 | 0.570 |
| Smoking | 1.53 | 1.02–2.31 | 0.040 * |
| Season | 2.08 | 1.45–2.42 | < 0.001 * |
| Supplementation containing vitamin D | 4.11 | 2.42–6.98 | < 0.001 * |
| n= 623 | |||
| Nagelkerke’s R2 = 0.152 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minter, M.; Augustin, H.; van Odijk, J.; Vanfleteren, L.E.G.W. Gender Differences in Vitamin D Status and Determinants of Vitamin D Insufficiency in Patients with Chronic Obstructive Pulmonary Disease. Nutrients 2023, 15, 426. https://doi.org/10.3390/nu15020426
Minter M, Augustin H, van Odijk J, Vanfleteren LEGW. Gender Differences in Vitamin D Status and Determinants of Vitamin D Insufficiency in Patients with Chronic Obstructive Pulmonary Disease. Nutrients. 2023; 15(2):426. https://doi.org/10.3390/nu15020426
Chicago/Turabian StyleMinter, Maria, Hanna Augustin, Jenny van Odijk, and Lowie E. G. W. Vanfleteren. 2023. "Gender Differences in Vitamin D Status and Determinants of Vitamin D Insufficiency in Patients with Chronic Obstructive Pulmonary Disease" Nutrients 15, no. 2: 426. https://doi.org/10.3390/nu15020426