

Plasma Trimethylamine N-Oxide Levels Are Associated with Poor Kidney Function in People with Type 2 Diabetes
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Markers of Diabetes, Renal Function, and Systemic Inflammation
2.3. Quantification of Trimethylamine N-Oxide (TMAO) Levels in Plasma
2.4. Statistical Analysis
3. Results
3.1. Subject Characteristics and and Metabolic Parameters
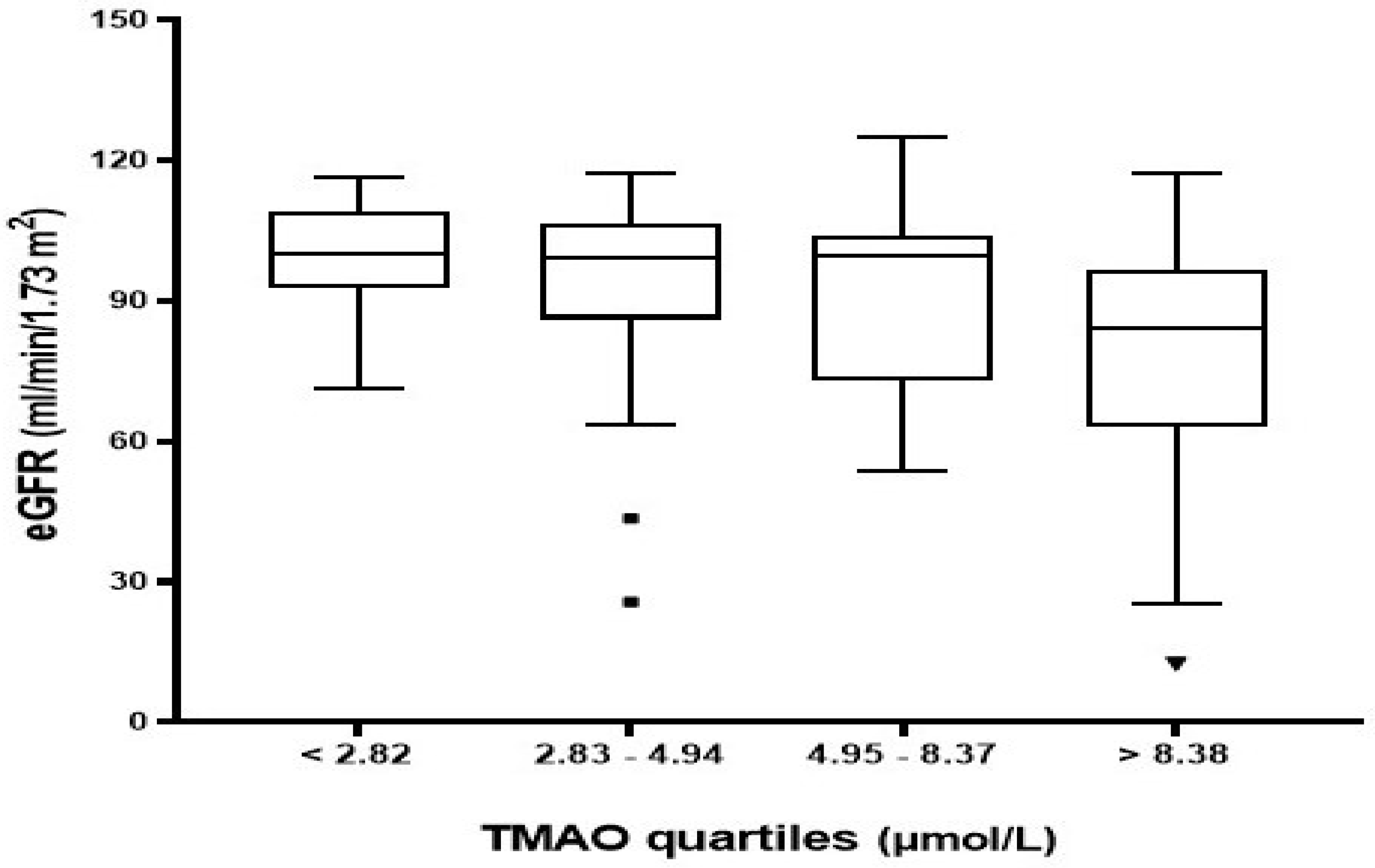
3.2. Plasma TMAO Levels and Markers of Kidney Disease
3.2.1. Correlation between Plasma TMAO Levels and Biomarkers of Kidney Disease
3.2.2. Association between Plasma TMAO Levels and CKD
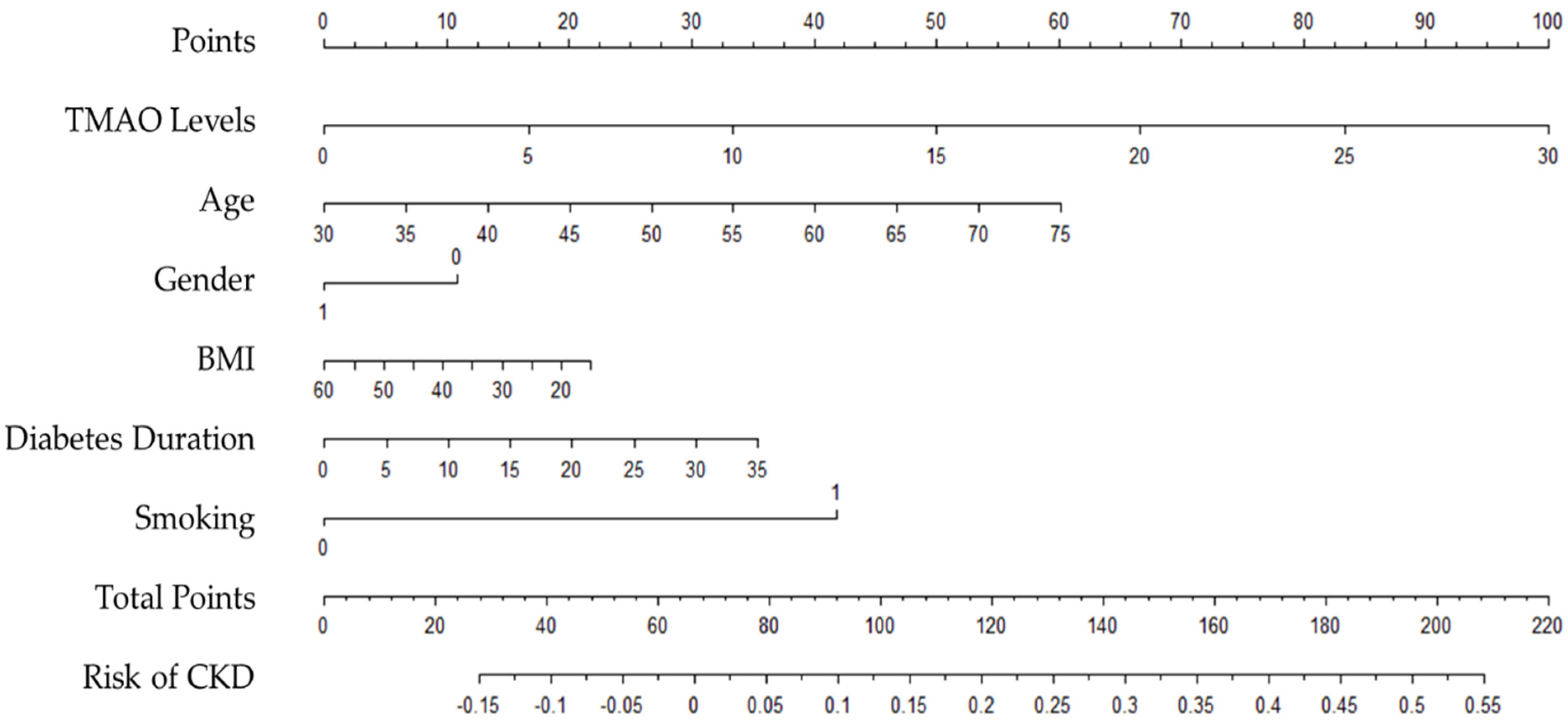
3.2.3. CKD Risk Prediction Nomogram
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A.; et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef] [PubMed]
- Wu, B.; Bell, K.; Stanford, A.; Kern, D.M.; Tunceli, O.; Vupputuri, S.; Kalsekar, I.; Willey, V. Understanding CKD among patients with T2DM: Prevalence, temporal trends, and treatment patterns—NHANES 2007–2012. BMJ Open Diabetes Res. Care 2016, 4, e000154. [Google Scholar] [CrossRef]
- Soldatos, G.; Cooper, M.E. Diabetic nephropathy: Important pathophysiologic mechanisms. Diabetes Res. Clin. Pract. 2008, 82, S75–S79. [Google Scholar] [CrossRef]
- Ninomiya, T.; Perkovic, V.; de Galan, B.E.; Zoungas, S.; Pillai, A.; Jardine, M.; Patel, A.; Cass, A.; Neal, B.; Poulter, N.; et al. Albuminuria and kidney function independently predict cardiovascular and renal outcomes in diabetes. J. Am. Soc. Nephrol. JASN 2009, 20, 1813–1821. [Google Scholar] [CrossRef]
- Pálsson, R.; Patel, U.D. Cardiovascular complications of diabetic kidney disease. Adv. Chronic. Kidney Dis. 2014, 21, 273–280. [Google Scholar] [CrossRef]
- Duran-Salgado, M.B.; Rubio-Guerra, A.F. Diabetic nephropathy and inflammation. World J. Diabetes 2014, 5, 393–398. [Google Scholar] [CrossRef]
- Shikata, K.; Makino, H. Microinflammation in the pathogenesis of diabetic nephropathy. J. Diabetes Investig. 2013, 4, 142–149. [Google Scholar] [CrossRef]
- Sekirov, I.; Russell, S.L.; Antunes, L.C.M.; Finlay, B.B. Gut microbiota in health and disease. Physiol. Rev. 2010, 90, 859–904. [Google Scholar] [CrossRef]
- Wang, Z.; Klipfell, E.; Bennett, B.J.; Koeth, R.; Levison, B.S.; DuGar, B.; Feldstein, A.E.; Britt, E.B.; Fu, X.; Chung, Y.-M. Gut flora metabolism of phosphatidylcholine promotes cardiovascular disease. Nature 2011, 472, 57. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Alcoholado, L.; Castellano-Castillo, D.; Jordán-Martínez, L.; Moreno-Indias, I.; Cardila-Cruz, P.; Elena, D.; Muñoz-Garcia, A.J.; Queipo-Ortuño, M.I.; Jimenez-Navarro, M. Role of gut microbiota on cardio-metabolic parameters and immunity in coronary artery disease patients with and without type-2 diabetes mellitus. Front. Microbiol. 2017, 8, 1936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shan, Z.; Sun, T.; Huang, H.; Chen, S.; Chen, L.; Luo, C.; Yang, W.; Yang, X.; Yao, P.; Cheng, J.; et al. Association between microbiota-dependent metabolite trimethylamine-N-oxide and type 2 diabetes. Am. J. Clin. Nutr. 2017, 106, 888–894. [Google Scholar] [CrossRef] [PubMed]
- Dambrova, M.; Latkovskis, G.; Kuka, J.; Strele, I.; Konrade, I.; Grinberga, S.; Hartmane, D.; Pugovics, O.; Erglis, A.; Liepinsh, E. Diabetes is associated with higher trimethylamine N-oxide plasma levels. Exp. Clin. Endocrinol. Diabetes 2016, 124, 251–256. [Google Scholar] [CrossRef]
- Zhuang, R.; Ge, X.; Han, L.; Yu, P.; Gong, X.; Meng, Q.; Zhang, Y.; Fan, H.; Zheng, L.; Liu, Z. Gut microbe–generated metabolite trimethylamine N-oxide and the risk of diabetes: A systematic review and dose-response meta-analysis. Obes. Rev. 2019, 20, 883–894. [Google Scholar] [CrossRef] [PubMed]
- Lever, M.; George, P.M.; Slow, S.; Bellamy, D.; Young, J.M.; Ho, M.; McEntyre, C.J.; Elmslie, J.L.; Atkinson, W.; Molyneux, S.L. Betaine and trimethylamine-N-oxide as predictors of cardiovascular outcomes show different patterns in diabetes mellitus: An observational study. PloS ONE 2014, 9, e114969. [Google Scholar] [CrossRef] [PubMed]
- Obeid, R.; Awwad, H.M.; Rabagny, Y.; Graeber, S.; Herrmann, W.; Geisel, J. Plasma trimethylamine N-oxide concentration is associated with choline, phospholipids, and methyl metabolism. Am. J. Clin. Nutr. 2016, 103, 703–711. [Google Scholar] [CrossRef]
- Tang, W.H.; Wang, Z.; Kennedy, D.J.; Wu, Y.; Buffa, J.A.; Agatisa-Boyle, B.; Li, X.S.; Levison, B.S.; Hazen, S.L. Gut microbiota-dependent trimethylamine N-oxide (TMAO) pathway contributes to both development of renal insufficiency and mortality risk in chronic kidney disease. Circ. Res. 2015, 116, 448–455. [Google Scholar] [CrossRef] [PubMed]
- Åkesson, B.; Vinge, E.; Skerfving, S. Pharmacokinetics of triethylamine and triethylamine-N-oxide in man. Toxicol. Appl. Pharmacol. 1989, 100, 529–538. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Y.; Guo, M.; Fang, X.; Teng, F.; Tan, X.; Li, X.; Wang, M.; Long, Y.; Xu, Y. Gut microbiota-derived trimethylamine N-oxide and kidney function: A systematic review and meta-Analysis. Adv. Nutr. 2021, 12, 1286–1304. [Google Scholar] [CrossRef]
- Stubbs, J.R.; House, J.A.; Ocque, A.J.; Zhang, S.; Johnson, C.; Kimber, C.; Schmidt, K.; Gupta, A.; Wetmore, J.B.; Nolin, T.D.; et al. Serum trimethylamine-N-oxide is elevated in CKD and correlates with coronary atherosclerosis burden. J. Am. Soc. Nephrol. JASN 2016, 27, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Missailidis, C.; Hällqvist, J.; Qureshi, A.R.; Barany, P.; Heimbürger, O.; Lindholm, B.; Stenvinkel, P.; Bergman, P. Serum trimethylamine-N-oxide is strongly related to renal function and predicts outcome in chronic kidney disease. PloS ONE 2016, 11, e0141738. [Google Scholar] [CrossRef] [Green Version]
- Xu, K.-Y.; Xia, G.-H.; Lu, J.-Q.; Chen, M.-X.; Zhen, X.; Wang, S.; You, C.; Nie, J.; Zhou, H.-W.; Yin, J. Impaired renal function and dysbiosis of gut microbiota contribute to increased trimethylamine-N-oxide in chronic kidney disease patients. Sci. Rep. 2017, 7, 1445. [Google Scholar] [CrossRef]
- Pelletier, C.C.; Croyal, M.; Ene, L.; Aguesse, A.; Billon-Crossouard, S.; Krempf, M.; Lemoine, S.; Guebre-Egziabher, F.; Juillard, L.; Soulage, C.O. Elevation of trimethylamine-N-oxide in chronic kidney disease: Contribution of decreased glomerular filtration rate. Toxins 2019, 11, 635. [Google Scholar] [CrossRef] [PubMed]
- Mueller, D.M.; Allenspach, M.; Othman, A.; Saely, C.H.; Muendlein, A.; Vonbank, A.; Drexel, H.; von Eckardstein, A. Plasma levels of trimethylamine-N-oxide are confounded by impaired kidney function and poor metabolic control. Atherosclerosis 2015, 243, 638–644. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Heaney, L.M.; Bhandari, S.S.; Jones, D.J.; Ng, L.L. Trimethylamine N-oxide and prognosis in acute heart failure. Heart 2016, 102, 841–848. [Google Scholar] [CrossRef]
- Roncal, C.; Martínez-Aguilar, E.; Orbe, J.; Ravassa, S.; Fernandez-Montero, A.; Saenz-Pipaon, G.; Ugarte, A.; Estella-Hermoso de Mendoza, A.; Rodriguez, J.A.; Fernández-Alonso, S. Trimethylamine-N-oxide (TMAO) predicts cardiovascular mortality in peripheral artery disease. Sci. Rep. 2019, 9, 15580. [Google Scholar] [CrossRef] [PubMed]
- Trøseid, M.; Ueland, T.; Hov, J.R.; Svardal, A.; Gregersen, I.; Dahl, C.P.; Aakhus, S.; Gude, E.; Bjørndal, B.; Halvorsen, B.; et al. Microbiota-dependent metabolite trimethylamine-N-oxide is associated with disease severity and survival of patients with chronic heart failure. J. Intern. Med. 2015, 277, 717–726. [Google Scholar] [CrossRef]
- Mafune, A.; Iwamoto, T.; Tsutsumi, Y.; Nakashima, A.; Yamamoto, I.; Yokoyama, K.; Yokoo, T.; Urashima, M. Associations among serum trimethylamine-N-oxide (TMAO) levels, kidney function and infarcted coronary artery number in patients undergoing cardiovascular surgery: A cross-sectional study. Clin. Exp. Nephrol. 2016, 20, 731–739. [Google Scholar] [CrossRef]
- Kim, R.B.; Morse, B.L.; Djurdjev, O.; Tang, M.; Muirhead, N.; Barrett, B.; Holmes, D.T.; Madore, F.; Clase, C.M.; Rigatto, C. Advanced chronic kidney disease populations have elevated trimethylamine N-oxide levels associated with increased cardiovascular events. Kidney Int. 2016, 89, 1144–1152. [Google Scholar] [CrossRef]
- Al-Obaide, M.A.; Singh, R.; Datta, P.; Rewers-Felkins, K.A.; Salguero, M.V.; Al-Obaidi, I.; Kottapalli, K.R.; Vasylyeva, T.L. Gut microbiota-dependent trimethylamine-N-oxide and serum biomarkers in patients with T2DM and advanced CKD. J. Clin. Med. 2017, 6, 86. [Google Scholar] [CrossRef]
- Kaysen, G.A.; Johansen, K.L.; Chertow, G.M.; Dalrymple, L.S.; Kornak, J.; Grimes, B.; Dwyer, T.; Chassy, A.W.; Fiehn, O. Associations of trimethylamine N-oxide with nutritional and inflammatory biomarkers and cardiovascular outcomes in patients new to dialysis. J. Ren. Nutr. 2015, 25, 351–356. [Google Scholar] [CrossRef] [Green Version]
- Tanase, D.M.; Gosav, E.M.; Neculae, E.; Costea, C.F.; Ciocoiu, M.; Hurjui, L.L.; Tarniceriu, C.C.; Maranduca, M.A.; Lacatusu, C.M.; Floria, M.; et al. Role of gut microbiota on onset and progression of microvascular complications of type 2 diabetes (T2DM). Nutrients 2020, 12, 3719. [Google Scholar] [CrossRef]
- Winther, S.A.; Øllgaard, J.C.; Hansen, T.W.; von Scholten, B.J.; Reinhard, H.; Ahluwalia, T.S.; Wang, Z.; Gæde, P.; Parving, H.-H.; Hazen, S.; et al. Plasma trimethylamine N-oxide and its metabolic precursors and risk of mortality, cardiovascular and renal disease in individuals with type 2-diabetes and albuminuria. PLoS ONE 2021, 16, e0244402. [Google Scholar] [CrossRef] [PubMed]
- Kalagi, N.A.; Thota, R.N.; Stojanovski, E.; Alburikan, K.A.; Garg, M.L. Association between plasma trimethylamine N-oxide levels and type 2 diabetes: A case control study. Nutrients 2022, 14, 2093. [Google Scholar] [CrossRef]
- Al-Wakeel Jamal, S. Accuracy and precision of the CKD-EPI and MDRD predictive equations compared with glomerular filtration rate measured by inulin clearance in a Saudi population. Ann. Saudi Med. 2016, 36, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Stevens, L.A.; Schmid, C.H.; Greene, T.; Zhang, Y.L.; Beck, G.J.; Froissart, M.; Hamm, L.L.; Lewis, J.B.; Mauer, M.; Navis, G.J.; et al. Comparative performance of the CKD Epidemiology Collaboration (CKD-EPI) and the Modification of Diet in Renal Disease (MDRD) Study equations for estimating GFR levels above 60 mL/min/1.73 m2. Am. J. Kidney Dis. 2010, 56, 486–495. [Google Scholar] [CrossRef]
- Awwad, H.M.; Geisel, J.; Obeid, R. Determination of trimethylamine, trimethylamine N-oxide, and taurine in human plasma and urine by UHPLC–MS/MS technique. J. Chromatogr. B 2016, 1038, 12–18. [Google Scholar] [CrossRef]
- Lai, Y.; Tang, H.; Zhang, X.; Zhou, Z.; Zhou, M.; Hu, Z.; Zhu, F.; Zhang, L.; Nie, J. Trimethylamine-N-Oxide Aggravates Kidney Injury via Activation of p38/MAPK Signaling and Upregulation of HuR. Kidney Blood Press. Res. 2022, 47, 61–71. [Google Scholar] [CrossRef] [PubMed]
- Sabatino, A.; Regolisti, G.; Brusasco, I.; Cabassi, A.; Morabito, S.; Fiaccadori, E. Alterations of intestinal barrier and microbiota in chronic kidney disease. Nephrol. Dial. Transplant. 2015, 30, 924–933. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Cai, R.; Sun, J.; Dong, X.; Huang, R.; Tian, S.; Wang, S. Diabetes mellitus as a risk factor for incident chronic kidney disease and end-stage renal disease in women compared with men: A systematic review and meta-analysis. Endocrine 2017, 55, 66–76. [Google Scholar] [CrossRef]
- Hai, X.; Landeras, V.; Dobre, M.A.; DeOreo, P.; Meyer, T.W.; Hostetter, T.H. Mechanism of prominent trimethylamine oxide (TMAO) accumulation in hemodialysis patients. PLoS ONE 2015, 10, e0143731. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Type 2 Diabetes | ||
|---|---|---|---|
| without CKD (n = 121) | with CKD (n = 12) | p-Value * | |
| Demographics | |||
| Age (years) a | 55 ± 9 | 63 ± 8 | 0.020 |
| Gender, No. (%) | 0.262 | ||
| Male | 23 (19) | 4 (33) | |
| Female | 98 (81) | 8 (66.7) | |
| BMI (kg/m2) b | 30.96 (28.31–34.81) | 31.52 (26.91–36.52) | 0.956 |
| Smoking (yes), No. (%) | 9 (7.4) | 3 (25) | 0.043 |
| Medical History | |||
| Diabetes duration (years) b | 11 (6–20) | 20 (15–20) | 0.007 |
| Laboratory Parameters | |||
| FPG, mmol/L b | 7.82 (8.00–10.00) | 9.25 (8.16–12.58) | 0.051 |
| HbA1C, % b | 8.2 (7.2–9.4) | 9.3 (8.7–10.1) | 0.036 |
| Haemoglobin, gm/L a | 132 ± 13 | 122 ± 17 | 0.021 |
| Serum creatinine, µmol/L b | 60 (51–73) | 128 (94–168) | <0.0001 |
| BUN, mmol/L b | 4.20 (3.30–5.30) | 9.75 (6.35–13.65) | <0.0001 |
| GFR, mL/min/1.73 m2 b | 98.75 (84.83–105.59) | 47.49 (30.51–55.22) | <0.0001 |
| Albumin, gm/L a | 36.86 ± 2.98 | 34.77 ± 3.45 | 0.024 |
| Alkaline phosphatase, unit/L b | 89 (64–108) | 97 (74–143) | 0.212 |
| K, mmol/L a | 4.49 ± 0.43 | 4.82 ± 0.50 | 0.015 |
| Na, mmol/L b | 140 (138–141) | 137 (135–140) | 0.005 |
| Ca+, mmol/L b | 2.34 (2.25–2.42) | 2.36 (2.30–2.42) | 0.574 |
| Phosphorous, mmol/L b | 1.24 (1.11–1.36) | 1.38 (1.20–1.48) | 0.073 |
| GGT, unit/L b | 24 (18–35) | 52 (36–96) | 0.001 |
| Total Bilirubin, µmol b | 6.55 (5.48–8.41) | 6.61 (5.68–10.82) | 0.572 |
| UACR, mg/gm b | 12.80 (6.68–32.11) | 154.07 (5.10–446) | 0.064 |
| Microalbuminuria, No. (%) | 23 (19) | 3 (25) | 0.702 |
| Macroalbuminuria, No. (%) | 5 (4.13) | 4 (33.3) | 0.004 |
| Urine creatinine, µmol/L b | 7149 (3885–9509) | 3637 (2836–7170) | 0.069 |
| Hs-CRP, mg/L b | 3.9 (1.3–8.3) | 1.6 (1.2–7.7) | 0.591 |
| TMAO, µmol/L b | 4.69 (2.62–7.76) | 10.16 (5.86–17.45) | 0.002 |
| Quartiles of TMAO | ||||||
|---|---|---|---|---|---|---|
| n | Q1 (n = 32) | Q2 (n = 34) | Q3 (n = 34) | Q4 (n = 33) | p-Value c | |
| TMAO, µmol/L | < 2.82 | 2.83–4.94 | 4.95–8.37 | > 8.38 | ||
| Demographics | ||||||
| Age (years) a | 133 | 54 ± 8 | 53 ± 10 | 55 ± 10 | 60 ± 8 2 | 0.011 |
| Gender, No. (%) | 0.531 | |||||
| Male | 27 | 5 (15.6) | 9 (26.5) | 5 (14.7) | 8 (24.2) | |
| Female | 106 | 27 (84.4) | 25 (73.5) | 29 (85.3) | 25 (75.8) | |
| BMI (kg/m2) b | 133 | 30.8 (28.58–33.17) | 31.24 (28.21–36.45) | 31.80 (29.50–37.53) | 30.78 (27.48–34.00) | 0.425 |
| Smoking (yes), No. (%) | 12 | 3 (9.4) | 4 (11.7) | 2 (5.9) | 3 (9.1) | 0.867 |
| Medical History | ||||||
| Kidney disease (yes), No. % | 12 | 0 | 2 (5.9) | 2 (5.9) | 8 (24.2) 1,2,3 | 0.004 |
| Diabetes duration | 133 | 15 (8–21) | 10 (8–15) | 11 (5–20) | 15 (8–20) | 0.437 |
| Laboratory Parameters | 133 | |||||
| FPG, mmol/L b | 8.25 (7.11–10.86) | 7.4 (6.25–10.04) | 8.24 (5.50–10.30) | 7.2 (5.31–9.35) | 0.488 | |
| HbA1C, % b | 8.5 (7.85–9.45) | 8.2 (7.20–9.60) | 8.6 (7.20–10) | 8.2 (7.20–9.30) | 0.770 | |
| Haemoglobin, gm/L a | 134 ± 12 | 132 ± 14 | 130 ± 15 | 127 ± 14 | 0.139 | |
| Serum creatinine, µmol/L b | 54 (50–69) | 63 (54–80) | 61 (49–82) | 71 (60–90) 1 | 0.016 | |
| BUN, mmol/L b | 3.6 (3.2–4.4) | 4.7 (3.4–5.4) | 4.5 (3.7–5.7) | 5.6 (3.7–7.2) 1 | 0.002 | |
| GFR, mL/min/1.73 m2 b | 99.96 (93.02–108.94) | 99.10 (86.15–105.86) | 99.48 (73.72–104.06) | 84.10 (65.94–94.35) 1,2 | 0.001 | |
| Albumin, gm/L a | 36.44 ± 2.61 | 37.41 ± 3.34 | 36.45 ± 3.16 | 36.36 ± 3.13 | 0.455 | |
| Alkaline phosphatase, unit/L b | 89.5 (67.50–114) | 81.5 (59–108) | 93 (67–108) | 94 (76–113) | 0.424 | |
| K, mmol/L a | 4.4 ± 0.5 | 4.5 ± 0.4 | 4.6 ± 0.4 | 4.6 ± 0.5 | 0.196 | |
| Na, mmol/L b | 139 (138–141) | 140 (138–141) | 140 (138–142) | 140 (138–141) | 0.780 | |
| Ca+, mmol/L b | 2.39 (2.30–2.43) | 2.34 (2.25–2.39) | 2.35 (2.28–2.42) | 2.34 (2.35–2.39) | 0.558 | |
| Phosphorous, mmol/L b | 1.25 (1.10–1.37) | 1.23 (1.09–1.35) | 1.27 (1.12–1.38) | 1.27 (1.16–1.48) | 0.443 | |
| Total Bilirubin, µmol b | 6.87 (6.44–8.70) | 6.30 (4.82–8.32) | 6.61 (5.26–8.41) | 6.55 (5.55–9.67) | 0.228 | |
| UACR, mg/gm b | 9.12 (5.91–32.95) | 11.28 (5.90–17.43) | 15.47 (8.13–78.25) | 22.25 (7.60–159.86) | 0.154 | |
| Urine creatinine, µmol/L b | 7403 (3979–10475) | 6832 (3637–8506) | 6622 (4569–9843) | 4638 (2648–9202) | 0.614 | |
| Hs-CRP, mg/L b | 3.6 (2.4–7.8) | 2.2 (0.9–8.8) | 4.1 (1.1–6.0) | 2.9 (1.2–7.2) | 0.399 | |
| Variables | rs | p-Value * |
|---|---|---|
| Age | 0.198 | 0.023 |
| BMI | −0.037 | 0.672 |
| Diabetes duration | 0.018 | 0.841 |
| Serum creatinine | 0.266 | 0.002 |
| BUN | 0.324 | <0.0001 |
| Albumin | −0.043 | 0.623 |
| Alkaline phosphatase | 0.079 | 0.367 |
| Total Bilirubin | −0.048 | 0.581 |
| K | 0.122 | 0.161 |
| Na | 0.081 | 0.356 |
| Ca | −0.007 | 0.376 |
| Phosphorous | 0.113 | 0.196 |
| GGT | −0.107 | 0.220 |
| UACR | 0.183 | 0.046 |
| Urine creatinine | −0.088 | 0.342 |
| Hs-CRP | −0.100 | 0.404 |
| Outcome—CKD | TMAO Levels, µmol/L | ||
|---|---|---|---|
| β | p-Value | 95% CI | |
| Model 1 (Unadjusted) | 0.015 | <0.0001 * | 0.007, 0.024 |
| Model 2 | 0.014 | 0.001 * | 0.005, 0.022 |
| Model 3 | 0.008 | 0.063 | 0.000, 0.016 |
| Model 4 | 0.001 | 0.706 | −0.005, 0.008 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kalagi, N.A.; Thota, R.N.; Stojanovski, E.; Alburikan, K.A.; Garg, M.L. Plasma Trimethylamine N-Oxide Levels Are Associated with Poor Kidney Function in People with Type 2 Diabetes. Nutrients 2023, 15, 812. https://doi.org/10.3390/nu15040812
Kalagi NA, Thota RN, Stojanovski E, Alburikan KA, Garg ML. Plasma Trimethylamine N-Oxide Levels Are Associated with Poor Kidney Function in People with Type 2 Diabetes. Nutrients. 2023; 15(4):812. https://doi.org/10.3390/nu15040812
Chicago/Turabian StyleKalagi, Nora A., Rohith N. Thota, Elizabeth Stojanovski, Khalid A. Alburikan, and Manohar L. Garg. 2023. "Plasma Trimethylamine N-Oxide Levels Are Associated with Poor Kidney Function in People with Type 2 Diabetes" Nutrients 15, no. 4: 812. https://doi.org/10.3390/nu15040812