
Association between Masticatory Performance, Nutritional Intake, and Frailty in Japanese Older Adults
 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
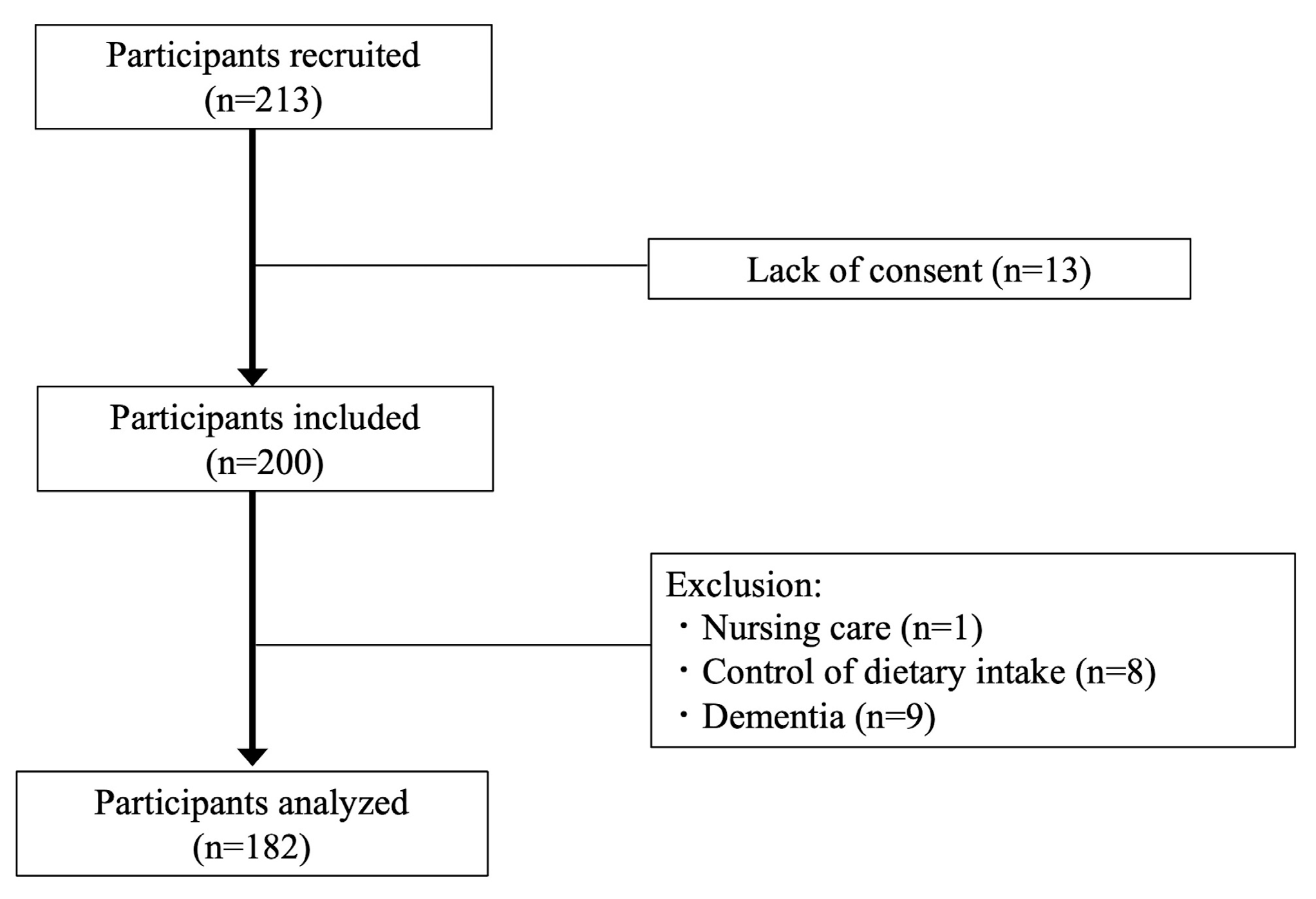
2.2. Participants
2.3. Measurement/Questionnaire
2.3.1. Masticatory Performance
2.3.2. Nutrients
2.3.3. Frailty
2.3.4. Other Measurements
2.4. Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cabinet Office. Annual Report on the Ageing Society. 2023. Available online: https://www8.cao.go.jp/kourei/whitepaper/w-2022/html/zenbun/index.html (accessed on 29 July 2023).
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- The Japan Geriatrics Society in 2014. Available online: https://www.jpn-geriat-soc.or.jp/info/topics/pdf/20140513_01_01.pdf (accessed on 1 December 2023).
- Morley, J.E. Frailty and sarcopenia in elderly. Wien Klin. Wochenschr. 2016, 128 (Suppl. S7), 439–445. [Google Scholar] [CrossRef]
- Coelho-Junior, H.J.; Marzetti, E.; Picca, A.; Cesari, M.; Uchida, M.C.; Calvani, R. Protein intake and frailty: A matter of quantity, quality, and timing. Nutrients 2020, 12, 2915. [Google Scholar] [CrossRef]
- Coelho-Júnior, H.J.; Rodrigues, B.; Uchida, M.; Marzetti, E. Low protein intake is associated with frailty in older adults: A systematic review and meta-analysis of observational studies. Nutrients 2018, 10, 1334. [Google Scholar] [CrossRef]
- Morley, J.E.; Vellas, B.; van Kan, G.A.; Anker, S.D.; Bauer, J.M.; Bernabei, R.; Cesari, M.; Chumlea, W.C.; Doehner, W.; Evans, J.; et al. Frailty consensus: A call to action. J. Am. Med. Dir. Assoc. 2013, 14, 392–397. [Google Scholar] [CrossRef]
- Artaza-Artabe, I.; Sáez-López, P.; Sánchez-Hernández, N.; Fernández-Gutierrez, N.; Malafarina, V. The relationship between nutrition and frailty: Effects of protein intake, nutritional supplementation, vitamin D and exercise on muscle metabolism in the elderly. A systematic review. Maturitas 2016, 93, 89–99. [Google Scholar] [CrossRef]
- Shimizu, Y.; Kim, H.; Yoshida, H.; Shimada, H.; Suzuki, T. Serum 25-hydroxyvitamin D level and risk of falls in Japanese community-dwelling elderly women: A 1-year follow-up study. Osteoporos. Int. 2015, 26, 2185–2192. [Google Scholar] [CrossRef]
- Iwasaki, M.; Kimura, Y.; Sasiwongsaroj, K.; Kettratad-Pruksapong, M.; Suksudaj, S.; Ishimoto, Y.; Chang, N.Y.; Sakamoto, R.; Matsubayashi, K.; Songpaisan, Y.; et al. Association between objectively measured chewing ability and frailty: A cross-sectional study in central Thailand. Geriatr. Gerontol. Int. 2018, 18, 860–866. [Google Scholar] [CrossRef]
- Watanabe, D.; Yoshida, T.; Yokoyama, K.; Yoshinaka, Y.; Watanabe, Y.; Kikutani, T.; Yoshida, M.; Yamada, Y.; Kimura, M.; Study, K.-K. Association between mixing ability of masticatory functions measured using color-changing chewing gum and frailty among Japanese older adults: The kyoto-kameoka study. Int. J. Environ. Res. Public Health 2020, 17, 4555. [Google Scholar] [CrossRef]
- Murakami, M.; Hirano, H.; Watanabe, Y.; Sakai, K.; Kim, H.; Katakura, A. Relationship between chewing ability and sarcopenia in Japanese community-dwelling older adults. Geriatr. Gerontol. Int. 2015, 15, 1007–1012. [Google Scholar] [CrossRef]
- Özsürekci, C.; Kara, M.; Güngör, A.E.; Ayçiçek, G.Ş.; Çalışkan, H.; Doğu, B.B.; Cankurtaran, M.; Halil, M.G. Relationship between chewing ability and malnutrition, sarcopenia, and frailty in older adults. Nutr. Clin. Pract. 2022, 37, 1409–1417. [Google Scholar] [CrossRef]
- Hakeem, F.F.; Bernabé, E.; Sabbah, W. Association between oral health and frailty: A systematic review of longitudinal studies. Gerodontology 2019, 36, 205–215. [Google Scholar] [CrossRef]
- Horibe, Y.; Ueda, T.; Watanabe, Y.; Motokawa, K.; Edahiro, A.; Hirano, H.; Shirobe, M.; Ogami, K.; Kawai, H.; Obuchi, S.; et al. A 2-year longitudinal study of the relationship between masticatory function and progression to frailty or pre-frailty among community-dwelling Japanese aged 65 and older. J. Oral Rehabil. 2018, 45, 864–870. [Google Scholar] [CrossRef]
- Senoo, S.; Iwasaki, M.; Kimura, Y.; Kakuta, S.; Masaki, C.; Wada, T.; Sakamoto, R.; Ishimoto, Y.; Fujisawa, M.; Okumiya, K.; et al. Combined effect of poor appetite and low masticatory function on sarcopenia in community-dwelling Japanese adults aged ≥ 75 years: A 3-year cohort study. J. Oral Rehabil. 2020, 47, 643–650. [Google Scholar] [CrossRef]
- Tanaka, T.; Takahashi, K.; Hirano, H.; Kikutani, T.; Watanabe, Y.; Ohara, Y.; Furuya, H.; Tetsuo, T.; Akishita, M.; Iijima, K. Oral frailty as a risk factor for physical frailty and mortality in community-dwelling elderly. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 1661–1667. [Google Scholar] [CrossRef]
- Jung, Y.S.; Park, T.; Kim, E.K.; Jeong, S.H.; Lee, Y.E.; Cho, M.J.; Song, K.B.; Choi, Y.H. Influence of chewing ability on elderly adults’ cognitive functioning: The mediating effects of the ability to perform daily life activities and nutritional status. Int. J. Environ. Res. Public Health 2022, 19, 1236. [Google Scholar] [CrossRef]
- Motokawa, K.; Mikami, Y.; Shirobe, M.; Edahiro, A.; Ohara, Y.; Iwasaki, M.; Watanabe, Y.; Kawai, H.; Kera, T.; Obuchi, S.; et al. Relationship between chewing ability and nutritional status in Japanese older adults: A cross-sectional study. Int. J. Environ. Res. Public Health 2021, 18, 1216. [Google Scholar] [CrossRef]
- Uesugi, H.; Shiga, H. Relationship between masticatory performance using a gummy jelly and masticatory movement. J. Prosthodont. Res. 2017, 61, 419–425. [Google Scholar] [CrossRef]
- Arai, H.; Satake, S. English translation of the Kihon Checklist. Geriatr. Gerontol. Int. 2015, 15, 518–519. [Google Scholar] [CrossRef]
- Sewo Sampaio, P.Y.; Sampaio, R.A.; Yamada, M.; Arai, H. Systematic review of the Kihon Checklist: Is it a reliable assessment of frailty? Geriatr. Gerontol. Int. 2016, 16, 893–902. [Google Scholar] [CrossRef]
- Kobayashi, S.; Honda, S.; Murakami, K.; Sasaki, S.; Okubo, H.; Hirota, N.; Notsu, A.; Fukui, M.; Date, C. Both comprehensive and brief self-administered diet history questionnaires satisfactorily rank nutrient intakes in Japanese adults. J. Epidemiol. 2012, 22, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, S.; Murakami, K.; Sasaki, S.; Okubo, H.; Hirota, N.; Notsu, A.; Fukui, M.; Date, C. Comparison of relative validity of food group intakes estimated by comprehensive and brief-type self-administered diet history questionnaires against 16 d dietary records in Japanese adults. Public Health Nutr. 2011, 14, 1200–1211. [Google Scholar] [CrossRef] [PubMed]
- Satake, S.; Arai, H. The revised Japanese version of the Cardiovascular Health Study criteria (revised J-CHS criteria). Geriatr. Gerontol. Int. 2020, 20, 992–993. [Google Scholar] [CrossRef] [PubMed]
- Minakuchi, S.; Tsuga, K.; Ikebe, K.; Ueda, T.; Tamura, F.; Nagao, K.; Furuya, J.; Matsuo, K.; Yamamoto, K.; Kanazawa, M.; et al. Oral hypofunction in the older population: Position paper of the Japanese Society of Gerodontology in 2016. Gerodontology 2018, 35, 317–324. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare. Dietary Reference Intakes for Japanese. 2020. Available online: http://mhlw.go.jp/content/10904750/000586553.pdf (accessed on 29 July 2023).
- Kim, K.M.; Jang, H.C.; Lim, S. Differences among skeletal muscle mass indices derived from height-, weight-, and body mass index-adjusted models in assessing sarcopenia. Korean J. Intern. Med. 2016, 31, 643–650. [Google Scholar] [CrossRef] [PubMed]
- Yamanashi, H.; Shimizu, Y.; Nelson, M.; Koyamatsu, J.; Nagayoshi, M.; Kadota, K.; Tamai, M.; Ariyoshi, K.; Maeda, T. The association between living alone and frailty in a rural Japanese population: The Nagasaki Islands study. J. Prim. Health Care 2015, 7, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Peduzzi, P.; Concato, J.; Kemper, E.; Holford, T.R.; Feinstein, A.R. A simulation study of the number of events per variable in logistic regression analysis. J. Clin. Epidemiol. 1996, 49, 1373–1379. [Google Scholar] [CrossRef]
- Chang, C.I.; Chan, D.C.D.; Kuo, K.N.; Hsiung, C.A.; Chen, C.Y. Vitamin D insufficiency and frailty syndrome in older adults living in a Northern Taiwan community. Arch. Gerontol. Geriatr. 2010, 50 (Suppl. S1), S17–S21. [Google Scholar] [CrossRef]
- Nanri, H.; Yamada, Y.; Yoshida, T.; Okabe, Y.; Nozawa, Y.; Itoi, A.; Yoshimura, E.; Watanabe, Y.; Yamaguchi, M.; Yokoyama, K.; et al. Sex difference in the association between protein intake and frailty: Assessed using the kihon checklist indexes among older adults. J. Am. Med. Dir. Assoc. 2018, 19, 801–805. [Google Scholar] [CrossRef]
- Chen, Y.; Capuano, E.; Stieger, M. Chew on it: Influence of oral processing behaviour on in vitro protein digestion of chicken and soya-based vegetarian chicken. Br. J. Nutr. 2021, 126, 1408–1419. [Google Scholar] [CrossRef]
- Forde, C.G.; Bolhuis, D. Interrelations between food form, texture, and matrix influence energy intake and metabolic responses. Curr. Nutr. Rep. 2022, 11, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Goh, A.T.; Chatonidi, G.; Choy, M.; Ponnalagu, S.; Stieger, M.; Forde, C.G. Impact of individual differences in eating rate on oral processing, bolus properties and post-meal glucose responses. Physiol. Behav. 2021, 238, 113495. [Google Scholar] [CrossRef] [PubMed]
- Murakami, M.; Watanabe, Y.; Edahiro, A.; Ohara, Y.; Obuchi, S.; Kawai, H.; Kim, H.; Fujiwara, Y.; Ihara, K.; Murakami, M.; et al. Factors related to dissociation between objective and subjective masticatory function in Japanese community-dwelling elderly adults. J. Oral Rehabil. 2018, 45, 598–604. [Google Scholar] [CrossRef]
- Hori, S.; Hori, K.; Yoshimura, S.; Uehara, F.; Sato, N.; Hasegawa, Y.; Akazawa, K.; Ono, T. Masticatory behavior change with a wearable chewing counter: A randomized controlled trial. J. Dent. Res. 2023, 102, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Lee, E.; Jang, I.Y. Frailty and comprehensive geriatric assessment. J. Korean Med. Sci. 2020, 35, e16. [Google Scholar] [CrossRef] [PubMed]
- Walston, J.; Buta, B.; Xue, Q.L. Frailty screening and interventions: Considerations for clinical practice. Clin. Geriatr. Med. 2018, 34, 25–38. [Google Scholar] [CrossRef]
- Quach, L.T.; Primack, J.; Bozzay, M.; Madrigal, C.; Erqou, S.; Rudolph, J.L. The intersection of physical and social frailty in older adults. R. I. Med. J. 2021, 104, 16–19. [Google Scholar]
- Mikami, Y.; Watanabe, Y.; Motokawa, K.; Shirobe, M.; Motohashi, Y.; Edahiro, A.; Nakajima, J.; Osuka, Y.; Inagaki, H.; Fujiwara, Y.; et al. Association between decrease in frequency of going out and oral function in older adults living in major urban areas. Geriatr. Gerontol. Int. 2019, 19, 792–797. [Google Scholar] [CrossRef]


{kind=link}
| n | All (n = 182) | Robust Group (n = 93) | Frailty Group (n = 89) | p-Value | |
|---|---|---|---|---|---|
| Age (years) | 74.0 (70.0, 78.3) | 74.0 (71.0, 77.5) | 74.0 (69.0, 80.0) | ||
| Younger (≦79) | 144 (79.1%) | 78 (83.9%) | 66 (74.2%) | ||
| Older (> 79) | 38 (20.9%) | 15 (16.1%) | 23 (25.8%) | 0.11 | |
| Sex | |||||
| Women | 104 (57.1%) | 55 (59.1%) | 49 (55.0%) | ||
| Men | 78 (42.9%) | 38 (40.9%) | 40 (45.0%) | 0.58 | |
| Living alone | |||||
| Living together | 149 (81.9%) | 14 (15.1%) | 19 (21.3%) | ||
| Living alone | 33 (18.1%) | 79 (84.9%) | 70 (78.7%) | 0.27 | |
| SMI (kg/m2) | 6.3 (5.6, 7.3) | 6.2 (5.8, 7.2) | 6.3 (5.5, 7.4) | ||
| High (> 5.7) | 126 (69.2%) | 70 (75.3%) | 56 (62.9%) | ||
| Low (≦ 5.7) | 56 (30.8%) | 23 (24.7%) | 33 (37.1%) | 0.07 | |
| Energy (kcal) | 1818.0 (1488.0, 2186.4) | 1817.6 (1526.5, 2213.1) | 1824.3 (1466.9, 2170.6) | ||
| High (> 1547.3) | 127 (69.8%) | 69 (74.2%) | 58 (65.2%) | ||
| Low (≦ 1547.3) | 55 (30.2%) | 24 (25.8%) | 31 (34.8%) | 0.18 | |
| Protein (% energy) | 17.3 (16.9–17.8) | 18.0 (17.4–18.7) | 16.6 (15.9–17.3) | ||
| High (> 19.4) | 46 (25.3%) | 32 (34.4%) | 14 (15.7%) | ||
| Low (≦ 19.4) | 136 (74.7%) | 61 (65.6%) | 75 (84.3%) | 0.003 * | |
| Vitamin D (μg) | 17.0 (10.1, 25.7) | 19.1 (10.5, 27.3) | 13.6 (8.9, 24.7) | ||
| High (> 9.5) | 144 (79.1%) | 81 (87.1%) | 63 (70.8%) | ||
| Low (≦ 9.5) | 38 (20.9%) | 12 (12.9%) | 26 (29.2%) | 0.006 * | |
| Subjective masticatory performance | |||||
| No (good) | 156 (85.7%) | 85 (91.4%) | 71 (79.8%) | ||
| Yes (bad) | 26 (14.3%) | 8 (8.6%) | 18 (20.2%) | 0.02 * | |
| Objective masticatory performance (mg/dL) | 160.5 (121.0, 203.2) | 171.0 (127.0, 217.0) | 150.0 (116.5, 195.5) | ||
| High (> 155) | 95 (52.2%) | 58 (62.4%) | 37 (41.6%) | ||
| Low (≦ 155) | 87 (47.8%) | 35 (37.6%) | 52 (58.4%) | 0.005 * | |
| OR (95% CI) | p-Values | VIF | ||
|---|---|---|---|---|
| Age (years) | ||||
| Younger (≦79) | 1 | |||
| Older (>79) | 1.45 [0.62–3.36] | 0.39 | 1.13 | |
| Sex | ||||
| Women | 1 | |||
| Men | 1.92 [0.84–4.42] | 0.12 | 1.59 | |
| Living alone | ||||
| Living together | 1 | |||
| Living alone | 1.40 [0.61–3.25] | 0.40 | 1.05 | |
| SMI (kg/m2) | ||||
| High (>5.7) | 1 | |||
| Low (≦5.7) | 2.50 [1.07–5.88] | 0.03 * | 1.46 | |
| Energy (kcal) | ||||
| High (>1547.3) | 1 | |||
| Low (≦1547.3) | 1.63 [0.76–3.50] | 0.21 | 1.18 | |
| Protein (% energy) | ||||
| High (>19.4) | 1 | |||
| Low (≦19.4) | 2.47 [1.10–5.55] | 0.02 * | 1.15 | |
| Vitamin D (μg) | ||||
| High (>9.5) | 1 | |||
| Low (≦9.5) | 2.11 [0.90–4.96] | 0.08 | 1.16 | |
| Subjective masticatory performance | ||||
| No (good) | 1 | |||
| Yes (bad) | 2.40 [0.90–6.44] | 0.08 | 1.07 | |
| Objective masticatory performance (mg/dL) | ||||
| High (>155) | 1 | |||
| Low (≦155) | 2.06 [1.07–3.97] | 0.03 * | 1.07 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okada, M.; Hama, Y.; Futatsuya, R.; Sasaki, Y.; Noritake, K.; Yamaguchi, K.; Matsuzaki, M.; Kubota, C.; Hosoda, A.; Minakuchi, S. Association between Masticatory Performance, Nutritional Intake, and Frailty in Japanese Older Adults. Nutrients 2023, 15, 5075. https://doi.org/10.3390/nu15245075
Okada M, Hama Y, Futatsuya R, Sasaki Y, Noritake K, Yamaguchi K, Matsuzaki M, Kubota C, Hosoda A, Minakuchi S. Association between Masticatory Performance, Nutritional Intake, and Frailty in Japanese Older Adults. Nutrients. 2023; 15(24):5075. https://doi.org/10.3390/nu15245075
Chicago/Turabian StyleOkada, Mitsuzumi, Yohei Hama, Ryota Futatsuya, Yoshiyuki Sasaki, Kanako Noritake, Kohei Yamaguchi, Mayuko Matsuzaki, Chieko Kubota, Akemi Hosoda, and Shunsuke Minakuchi. 2023. "Association between Masticatory Performance, Nutritional Intake, and Frailty in Japanese Older Adults" Nutrients 15, no. 24: 5075. https://doi.org/10.3390/nu15245075