


Association of a Combination of Sarcopenia and Type 2 Diabetes with Blood Parameters, Nutrient Intake, and Physical Activity: A Nationwide Population-Based Study

Abstract
:1. Introduction
2. Materials and Methods
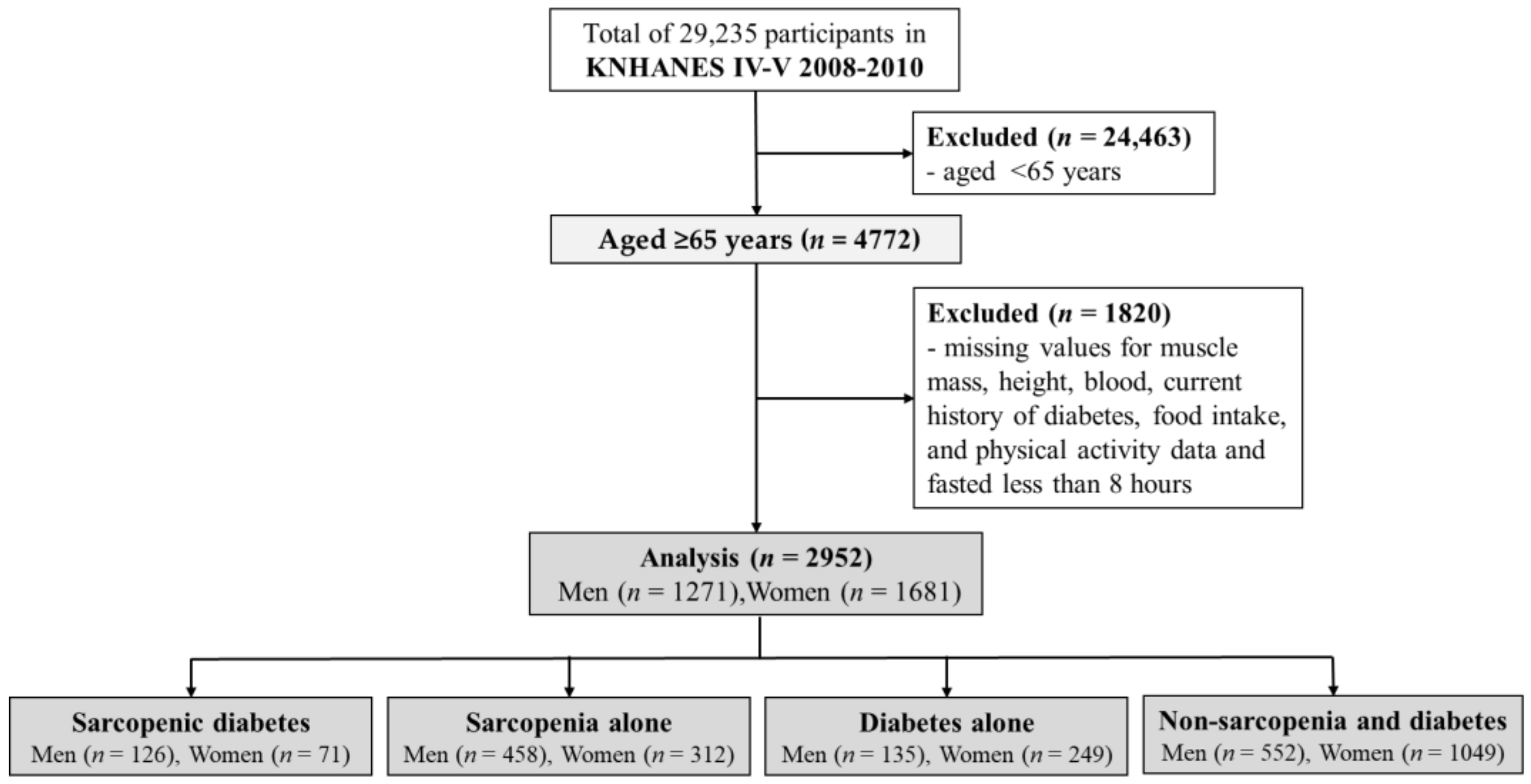
2.1. Study Design and Participants
2.2. Participant Characteristics
2.3. Measurement of Blood Parameters
2.4. Assessment of Dietary Intake
2.5. Assessment of Physical Activity
2.6. Definitions of Sarcopenia and T2D
2.7. Statistical Analyses
3. Results
3.1. Participant Characteristics
3.2. Blood Parameters
3.3. Nutrient Intakes
3.4. Physical Activities
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.N.; Mbanya, J.C.; et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef] [PubMed]
- Mayhew, A.J.; Amog, K.; Phillips, S.; Parise, G.; McNicholas, P.D.; de Souza, R.J.; Thabane, L.; Raina, P.; Raina, P. The prevalence of sarcopenia in community-dwelling older adults, an exploration of differences between studies and within definitions: A systematic review and meta-analyses. Age Ageing 2019, 48, 48–56. [Google Scholar] [CrossRef]
- Thomas, D.R. Loss of skeletal muscle mass in aging: Examining the relationship of starvation, sarcopenia and cachexia. Clin. Nutr. 2007, 26, 389–399. [Google Scholar] [CrossRef] [PubMed]
- Mithal, A.; Bonjour, J.P.; Boonen, S.; Burckhardt, P.; Degens, H.; El Hajj Fuleihan, G.; Josse, R.; Lips, P.; Morales Torres, J.; Rizzoli, R.; et al. Impact of nutrition on muscle mass, strength, and performance in older adults. Osteoporos. Int. 2013, 24, 1555–1566. [Google Scholar] [CrossRef]
- Ispoglou, T.; Wilson, O.; McCullough, D.; Aldrich, L.; Ferentinos, P.; Lyall, G.; Stavropoulos-Kalinoglou, A.; Duckworth, L.; Brown, M.A.; Sutton, L.; et al. A Narrative Review of Non-Pharmacological Strategies for Managing Sarcopenia in Older Adults with Cardiovascular and Metabolic Diseases. Biology 2023, 12, 892. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, I.H. Epidemiologic and methodologic problems in determining nutritional-status of older persons. Proceedings of the a Conference Held in Albuquerque, NM. Am. J. Clin. Nutr. 1989, 50, 1231–1233. [Google Scholar] [CrossRef]
- Baumgartner, R.N.; Koehler, K.M.; Gallagher, D.; Romero, L.; Heymsfield, S.B.; Ross, R.R.; Garry, P.J.; Lindeman, R.D.; Lindeman, R.D. Epidemiology of sarcopenia among the elderly in New Mexico. Am. J. Epidemiol. 1998, 147, 755–763. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Steffl, M.; Bohannon, R.W.; Sontakova, L.; Tufano, J.J.; Shiells, K.; Holmerova, I. Relationship between sarcopenia and physical activity in older people: A systematic review and meta-analysis. Clin. Interv. Aging 2017, 12, 835–845. [Google Scholar] [CrossRef]
- Xu, W.; Chen, T.; Cai, Y.; Hu, Y.; Fan, L.; Wu, C. Sarcopenia in community-dwelling oldest old is associated with disability and poor physical function. J. Nutr. Health Aging 2020, 24, 339–345. [Google Scholar] [CrossRef]
- Moorthi, R.N.; Avin, K.G. Clinical relevance of sarcopenia in chronic kidney disease. Curr. Opin. Nephrol. Hypertens. 2017, 26, 219–228. [Google Scholar] [CrossRef] [PubMed]
- Mesinovic, J.; Zengin, A.; De Courten, B.; Ebeling, P.R.; Scott, D. Sarcopenia and type 2 diabetes mellitus: A bidirectional relationship. Diabetes Metab. Syndr. Obes. 2019, 12, 1057–1072. [Google Scholar] [CrossRef]
- Chung, S.M.; Moon, J.S.; Chang, M.C. Prevalence of sarcopenia and its association with diabetes: A meta-analysis of community-dwelling Asian population. Front. Med. 2021, 8, 681232. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, B.B.; Fujita, S.; Wolfe, R.R.; Mittendorfer, B.; Roy, M.; Rowe, V.L.; Volpi, E. Insulin resistance of muscle protein metabolism in aging. FASEB J. 2006, 20, 768–769. [Google Scholar] [CrossRef] [PubMed]
- Guillet, C.; Prod’homme, M.; Balage, M.; Gachon, P.; Giraudet, C.; Morin, L.; Grizard, J.; Boirie, Y.; Boirie, Y. Impaired anabolic response of muscle protein synthesis is associated with S6K1 dysregulation in elderly humans. FASEB J. 2004, 18, 1586–1587. [Google Scholar] [CrossRef] [PubMed]
- Welch, A.A.; Hayhoe, R.P.G.; Cameron, D. The relationships between sarcopenic skeletal muscle loss during ageing and macronutrient metabolism, obesity and onset of diabetes. Proc. Nutr. Soc. 2020, 79, 158–169. [Google Scholar] [CrossRef] [PubMed]
- Okamura, T.; Miki, A.; Hashimoto, Y.; Kaji, A.; Sakai, R.; Osaka, T.; Hamaguchi, M.; Yamazaki, M.; Fukui, M.; Yamazaki, M.; et al. Shortage of energy intake rather than protein intake is associated with sarcopenia in elderly patients with type 2 diabetes: A cross-sectional study of the KAMOGAWA-DM cohort. J. Diabetes 2019, 11, 477–483. [Google Scholar] [CrossRef]
- He, Q.; Wang, X.; Yang, C.; Zhuang, X.; Yue, Y.; Jing, H.; Hu, J.; Sun, M.; Guo, L.; Sun, M.; et al. Metabolic and nutritional characteristics in middle-aged and elderly sarcopenia patients with Type 2 diabetes. J. Diabetes Res. 2020, 2020, 6973469. [Google Scholar] [CrossRef]
- Murata, Y.; Kadoya, Y.; Yamada, S.; Sanke, T. Sarcopenia in elderly patients with type 2 diabetes mellitus: Prevalence and related clinical factors. Diabetol. Int. 2018, 9, 136–142. [Google Scholar] [CrossRef]
- Fung, F.Y.; Koh, Y.L.E.; Malhotra, R.; Ostbye, T.; Lee, P.Y.; Shariff Ghazali, S.; Tan, N.C. Prevalence of and factors associated with sarcopenia among multi-ethnic ambulatory older Asians with type 2 diabetes mellitus in a primary care setting. BMC Geriatr. 2019, 19, 122. [Google Scholar] [CrossRef]
- Cui, M.; Gang, X.; Wang, G.; Xiao, X.; Li, Z.; Jiang, Z.; Wang, G. A cross-sectional study: Associations between sarcopenia and clinical characteristics of patients with type 2 diabetes. Medicine 2020, 99, e18708. [Google Scholar] [CrossRef] [PubMed]
- Sazlina, S.G.; Lee, P.Y.; Chan, Y.M.; Hamid, M.S.A.; Tan, N.C. The prevalence and factors associated with sarcopenia among community living elderly with type 2 diabetes mellitus in primary care clinics in Malaysia. PLoS ONE 2020, 15, e0233299. [Google Scholar] [CrossRef] [PubMed]
- Kweon, S.; Kim, Y.; Jang, M.J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.H.; Oh, K. Data resource profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef] [PubMed]
- Simental-Mendía, L.E.; Rodríguez-Morán, M.; Guerrero-Romero, F. The product of fasting glucose and triglycerides as surrogate for identifying insulin resistance in apparently healthy subjects. Metab. Syndr. Relat. Disord. 2008, 6, 299–304. [Google Scholar] [CrossRef]
- Park, S.; Ahn, J.; Lee, B.K. Self-rated subjective health status is strongly associated with sociodemographic factors, lifestyle, nutrient intakes, and biochemical indices, but not smoking status: KNHANES 2007–2012. J. Korean Med. Sci. 2015, 30, 1279–1287. [Google Scholar] [CrossRef]
- Ainsworth, B.E.; Haskell, W.L.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J.; O’Brien, W.L.; Bassett, D.R.; Schmitz, K.H.; Emplaincourt, P.O.; et al. Compendium of physical activities: An update of activity codes and MET intensities. Med. Sci. Sports Exerc. 2000, 32, S498–S504. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian working group for sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e2. [Google Scholar] [CrossRef]
- Ginsberg, H.N.; Zhang, Y.L.; Hernandez-Ono, A. Regulation of plasma triglycerides in insulin resistance and diabetes. Arch. Med. Res. 2005, 36, 232–240. [Google Scholar] [CrossRef]
- Grundy, S.M.; Benjamin, I.J.; Burke, G.L.; Chait, A.; Eckel, R.H.; Howard, B.V.; Mitch, W.; Smith, S.C.; Sowers, J.R.; Smith, S.C.; et al. Diabetes and cardiovascular disease: A statement for healthcare professionals from the American Heart Association. Circulation 1999, 100, 1134–1146. [Google Scholar] [CrossRef] [PubMed]
- Pan, D.A.; Lillioja, S.; Kriketos, A.D.; Milner, M.R.; Baur, L.A.; Bogardus, C.; Jenkins, A.B.; Storlien, L.H.; Storlien, L.H. Skeletal muscle triglyceride levels are inversely related to insulin action. Diabetes 1997, 46, 983–988. [Google Scholar] [CrossRef] [PubMed]
- Guerrero-Romero, F.; Simental-Mendía, L.E.; González-Ortiz, M.; Martínez-Abundis, E.; Ramos-Zavala, M.G.; Hernández-González, S.O.; Jacques-Camarena, O.; Rodríguez-Morán, M.; Rodríguez-Morán, M. The product of triglycerides and glucose, a simple measure of insulin sensitivity. Comparison with the euglycemic-hyperinsulinemic clamp. J. Clin. Endocrinol. Metab. 2010, 95, 3347–3351. [Google Scholar] [CrossRef] [PubMed]
- Nabipoorashrafi, S.A.; Seyedi, S.A.; Rabizadeh, S.; Ebrahimi, M.; Ranjbar, S.A.; Reyhan, S.K.; Meysamie, A.; Nakhjavani, M.; Esteghamati, A.; Nakhjavani, M.; et al. The accuracy of triglyceride-glucose (TyG) index for the screening of metabolic syndrome in adults: A systematic review and meta-analysis. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 2677–2688. [Google Scholar] [CrossRef] [PubMed]
- Mika, A.; Sledzinski, T. Alterations of specific lipid groups in serum of obese humans: A review. Obes. Rev. 2017, 18, 247–272. [Google Scholar] [CrossRef] [PubMed]
- Khadra, D.; Itani, L.; Tannir, H.; Kreidieh, D.; El Masri, D.; El Ghoch, M. Association between sarcopenic obesity and higher risk of type 2 diabetes in adults: A systematic review and meta-analysis. World J. Diabetes 2019, 10, 311–323. [Google Scholar] [CrossRef] [PubMed]
- Hori, T.; Nakamura, S.; Yamagami, H.; Yasui, S.; Hosoki, M.; Hara, T.; Mitsui, Y.; Masuda, S.; Kurahashi, K.; Yoshida, S.; et al. Phase angle and extracellular water-to-total body water ratio estimated by bioelectrical impedance analysis are associated with levels of hemoglobin and hematocrit in patients with diabetes. Heliyon 2023, 9, e14724. [Google Scholar] [CrossRef]
- Zeng, F.; Huang, L.; Zhang, Y.; Hong, X.; Weng, S.; Shen, X.; Zhao, F.; Yan, S.; Yan, S. Additive effect of sarcopenia and anemia on the 10-year risk of cardiovascular disease in patients with type 2 diabetes. J. Diabetes Res. 2022, 2022, 2202511. [Google Scholar] [CrossRef]
- Velázquez-Alva, M.C.; Irigoyen-Camacho, M.E.; Zepeda-Zepeda, M.A.; Lazarevich, I.; Arrieta-Cruz, I.; D’Hyver, C. Sarcopenia, nutritional status and type 2 diabetes mellitus: A cross-sectional study in a group of Mexican women residing in a nursing home. Nutr. Diet. 2020, 77, 515–522. [Google Scholar] [CrossRef]
- Mathieu, C.; Gysemans, C.; Giulietti, A.; Bouillon, R. Vitamin D and diabetes. Diabetologia 2005, 48, 1247–1257. [Google Scholar] [CrossRef]
- Adams, J.S.; Hewison, M. Update in vitamin D. J. Clin. Endocrinol. Metab. 2010, 95, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D status: Measurement, interpretation, and clinical application. Ann. Epidemiol. 2009, 19, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Lips, P. Vitamin D deficiency and secondary hyperparathyroidism in the elderly: Consequences for bone loss and fractures and therapeutic implications. Endocr. Rev. 2001, 22, 477–501. [Google Scholar] [CrossRef] [PubMed]
- Pfeifer, M.; Begerow, B.; Minne, H.W.; Schlotthauer, T.; Pospeschill, M.; Scholz, M.; Lazarescu, A.D.; Pollähne, W.; Pollähne, W. Vitamin D status, trunk muscle strength, body sway, falls, and fractures among 237 postmenopausal women with osteoporosis. Exp. Clin. Endocrinol. Diabetes 2001, 109, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Kristoffersson, A.; Boström, A.; Söderberg, T. Muscle strength is improved after parathyroidectomy in patients with primary hyperparathyroidism. Br. J. Surg. 1992, 79, 165–168. [Google Scholar] [CrossRef]
- Chang, E.; Donkin, S.S.; Teegarden, D. Parathyroid hormone suppresses insulin signaling in adipocytes. Mol. Cell Endocrinol. 2009, 307, 77–82. [Google Scholar] [CrossRef]
- World Health Organization. Protein and Amino Acid Requirements in Human Nutrition; WHO: Geneva, Switzerland, 2007. [Google Scholar]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-based recommendations for optimal dietary protein intake in older people: A position paper from the PROT-AGE Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef]
- Franz, M.J.; Bantle, J.P.; Beebe, C.A.; Brunzell, J.D.; Chiasson, J.L.; Garg, A.; Holzmeister, L.A.; Hoogwerf, B.; Mayer-Davis, E.; Mooradian, A.D.; et al. Evidence-based nutrition principles and recommendations for the treatment and prevention of diabetes and related complications. Diabetes Care 2002, 25, 148–198. [Google Scholar] [CrossRef]
- Yanai, H. Nutrition for sarcopenia. J. Clin. Med. Res. 2015, 7, 926–931. [Google Scholar] [CrossRef]
- World Health Organization. Diet, Nutrition and the Prevention of Chronic Diseases; WHO: Geneva, Switzerland, 2003. [Google Scholar]
- DeFronzo, R.A. The effect of insulin on renal sodium metabolism. A review with clinical implications. Diabetologia 1981, 21, 165–171. [Google Scholar] [CrossRef]
- Sigal, R.J.; Kenny, G.P.; Wasserman, D.H.; Castaneda-Sceppa, C. Physical activity/exercise and type 2 diabetes. Diabetes Care 2004, 27, 2518–2539. [Google Scholar] [CrossRef] [PubMed]
- Evans, W.J. Skeletal muscle loss: Cachexia, sarcopenia, and inactivity. Am. J. Clin. Nutr. 2010, 91, 1123S–1127S. [Google Scholar] [CrossRef] [PubMed]
- Nelson, M.E.; Rejeski, W.J.; Blair, S.N.; Duncan, P.W.; Judge, J.O.; King, A.C.; Macera, C.A.; Castaneda-Sceppa, C.; Castaneda-Sceppa, C. Physical activity and public health in older adults: Recommendation from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 2007, 39, 1435–1445. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]


{kind=link}
| Men | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variables (Unit) | Sarcopenic Diabetes a (n = 126) | Sarcopenia Alone b (n = 458) | Diabetes Alone c (n = 135) | Non-Sarcopenia and Non-Diabetes d (n = 552) | K-W Test | |||||
| Median | (IQR: Q1–Q3) | Median | (IQR: Q1–Q3) | Median | (IQR: Q1–Q3) | Median | (IQR: Q1–Q3) | H-Value | p-Value | |
| Age (year) | 72.0 | (69.0–75.0) c,d | 73.0 | (69.0–76.0) c,d | 69.0 | (67.0–73.0) a,b | 70.0 | (67.0–74.0) a,b | 66.7 | <0.01 |
| SBP (mmHg) | 131.0 | (114.0–145.0) | 129.0 | (117.0–141.0) | 130.0 | (121.0–141.0) | 129.0 | (118.0–141.0) | 1.5 | 0.69 |
| DBP (mmHg) | 74.0 | (69.0–82.0) d | 77.0 | (70.0–82.0) d | 77.0 | (70.0–83.0) | 79.0 | (70.0–84.0) a,b | 15.9 | <0.01 |
| WC (cm) | 84.2 | (79.1–88.7) b,c,d | 79.3 | (73.4–85.3) a,c,d | 91.7 | (85.2–95.0) a,b,d | 87.6 | (82.7–92.3) a,b,c | 279.5 | <0.01 |
| BMI (kg/m2) | 22.2 | (20.9–23.6) b,c,d | 21.0 | (19.4–22.5) a,c,d | 25.4 | (23.5–26.9) a,b,d | 24.3 | (22.9–25.9) a,b,c | 479.7 | <0.01 |
| Fat mass (kg) | 15.3 | (11.7–18.1) b | 12.2 | (9.0–15.7) a,c,d | 15.6 | (13.3–19.9) b,d | 15.0 | (11.9–18.2) b,c | 101.7 | <0.01 |
| LBM (kg) | 43.4 | (39.6–46.1) b,c,d | 41.5 | (38.8–44.0) a,c,d | 50.0 | (46.6–53.7) a,b,d | 48.1 | (45.3–51.8) a,b,c | 568.5 | <0.01 |
| Bone mass (g) | 2261.4 | (2013.0–2563.3) b,c,d | 2142.2 | (1927.2–2363.3) a,c,d | 2480.7 | (2273.9–2748.7) a,b | 2410.9 | (2194.5–2652.6) a,b | 160.7 | <0.01 |
| Bone area (cm2) | 2005.3 | (1884.7–2112.0) b,c,d | 1960.6 | (1830.1–2057.9) a,c,d | 2123.5 | (2011.9–2234.1) a,b | 2093.2 | (1996.7–2196.1) a,b | 221.2 | <0.01 |
| BMD (g/cm2) | 1.13 | (1.0–1.2) c | 1.10 | (1.0–1.2) c,d | 1.16 | (1.1–1.2) a,b | 1.15 | (1.1–1.2) b | 59.4 | <0.01 |
| AMI (kg/cm2) | 6.50 | (6.1–6.8) c,d | 6.55 | (6.2–6.8) c,d | 7.61 | (7.3–8.1) a,b | 7.62 | (7.3–8.0) a,b | 946.5 | <0.01 |
| Sleep duration (hour) | 7.0 | (6.0–8.0) | 7.0 | (6.0–8.0) | 7.0 | (6.0–8.0) | 7.0 | (6.0–8.0) | 7.1 | 0.07 |
| † Drinking (yes, n(%)) | 77 (61.1) | 282 (61.6) d | 94 (69.6) | 390 (70.7) b | <0.01 | |||||
| † Smoking (yes, n(%)) | 70 (55.6) | 280 (61.1) | 80 (59.3) | 344 (62.3) | 0.54 | |||||
| Women | ||||||||||
| Variables (Unit) | Sarcopenic diabetes a (n = 71) | Sarcopenia alone b (n = 312) | Diabetes alone c (n = 249) | Non-sarcopenia and non-diabetes d (n = 1049) | K-W test | |||||
| Median | (IQR: Q1–Q3) | Median | (IQR: Q1–Q3) | Median | (IQR: Q1–Q3) | Median | (IQR: Q1–Q3) | H-value | p-value | |
| Age (year) | 73.0 | (68.0–77.0) c | 72.0 | (68.0–76.0) c,d | 70.0 | (67.0–75.0) a,b | 71.0 | (68.0–75.0) b | 23.5 | <0.01 |
| SBP (mmHg) | 137.5 | (122.5–150.5) b | 131.0 | (118.0–142.0) a | 133.0 | (120.0–144.0) | 132.0 | (120.0–144.0) | 8.4 | 0.04 |
| DBP (mmHg) | 76.0 | (69.0–82.0) | 75.0 | (70.0–82.0) c | 76.0 | (70.0–82.0) | 79.0 | (71.0–85.0) b | 18.3 | <0.01 |
| WC (cm) | 81.2 | (74.3–85.8) b,c | 77.1 | (71.1–84.2) a,c,d | 89.4 | (83.2–95.2) a,b,d | 83.6 | (77.4–89.9) b,c | 228.6 | <0.01 |
| BMI (kg/m2) | 22.4 | (20.6–24.0) c,d | 21.4 | (19.6–23.2) c,d | 25.8 | (23.8–27.9) a,b,d | 24.5 | (22.5–26.5) a,b,c | 324.2 | <0.01 |
| Fat mass (kg) | 18.3 | (14.5–22.2) c | 16.7 | (13.3–20.1) c,d | 20.8 | (17.6–24.7) a,b,d | 19.0 | (15.2–22.7) b,c | 87.8 | <0.01 |
| LBM (kg) | 30.7 | (28.9–32.4) c,d | 29.9 | (28.2–31.5) c,d | 36.3 | (34.2–39.7) a,b,d | 34.5 | (32.4–37.0) a,b,c | 560.7 | <0.01 |
| Bone mass (g) | 1524.4 | (1299.3–1727.5) c | 1437.1 | (1252.9–1646.0) c,d | 1676.9 | (1484.6–1842.5) a,b,d | 1580.8 | (1406.2–1774.2) b,c | 91.2 | <0.01 |
| Bone area (cm2) | 1557.3 | (1440.9–1678.9) c,d | 1552.7 | (1450.5–1676.9) c,d | 1706.7 | (1595.7–1820.3) a,b,d | 1666.0 | (1562.4–1768.3) a,b,c | 148.1 | <0.01 |
| BMD (g/cm2) | 0.96 | (0.9–1.0) | 0.92 | (0.9–1.0) c,d | 0.97 | (0.9–1.0) b,d | 0.94 | (0.9–1.0) b,c | 30.4 | <0.01 |
| AMI (kg/cm2) | 5.15 | (4.9–5.3) c,d | 5.15 | (4.9–5.3) c,d | 6.22 | (5.9–6.6) a,b | 6.07 | (5.8–6.4) a,b | 896.6 | <0.01 |
| Sleep duration (hour) | 7.0 | (6.0–8.0) c,d | 6.0 | (5.0–8.0) | 6.0 | (5.0–8.0) a | 6.0 | (5.0–7.0) a | 10.5 | 0.01 |
| † Drinking (yes, n (%)) | 20 (28.2) | 94 (30.1) | 83 (33.3) | 374 (35.7) | 0.21 | |||||
| † Smoking (yes, n (%)) | 7 (9.9) | 36 (11.5) | 20 (8.0) | 84 (8.0) | 0.26 | |||||
| Men | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variables (Unit) | Sarcopenic Diabetes a (n = 126) | Sarcopenia Alone b (n = 458) | Diabetes Alone c (n = 135) | Non-Sarcopenia and Non-Diabetes d (n = 552) | K-W Test | |||||
| Median | (IQR: Q1–Q3) | Median | (IQR: Q1–Q3) | Median | (IQR: Q1–Q3) | Median | (IQR: Q–Q3) | H-Value | p-Value | |
| TC (mg/dL) | 172.0 | (148.8–195.3) | 176.0 | (155.0–201.0) | 172.0 | (153.0–198.0) | 182.0 | (158.0–203.0) | 7.9 | 0.05 |
| HDL-C (mg/dL) | 41.7 | (35.6–48.9) b | 45.2 | (38.2–53.9) a,c,d | 39.1 | (33.0–45.2) b,d | 42.6 | (36.5–49.5) b,c | 43.8 | <0.01 |
| LDL-C (mg/dL) | 101.7 | (78.0–124.3) | 106.3 | (87.5–131.0) | 103.7 | (82.9–129.1) | 110.7 | (88.9–130.8) | 9.6 | 0.02 |
| Triglyceride (mg/dL) | 120.0 | (83.0–184.5) c | 107.0 | (76.0–154.3) c,d | 147.0 | (111.0–215.0) a,b,d | 119.5 | (84.0–168.0) b,c | 38.2 | <0.01 |
| Hemoglobin (g/dL) | 14.0 | (13.2–15.3) c,d | 14.3 | (13.4–15.1) c,d | 14.7 | (13.9–15.5) a,b | 14.8 | (14.0–15.4) a,b | 46.7 | <0.01 |
| Hematocrit (%) | 41.6 | (39.1–44.8) c,d | 42.5 | (40.0–44.6) c,d | 43.4 | (41.1–45.6) a,b | 43.5 | (41.5–45.5 )a,b | 39.3 | <0.01 |
| Ferritin (ng/mL) | 97.2 | (58.8–168.1) | 88.1 | (52.4–150.1) | 98.6 | (57.4–184.0) | 89.5 | (53.5–157.4) | 4.6 | 0.20 |
| Urea nitrogen (mg/dL) | 17.0 | (14.0–21.0) | 16.0 | (14.0–19.0) | 18.0 | (14.0–21.0) | 16.0 | (14.0–19.0) | 8.3 | 0.04 |
| Creatinine (mg/dL) | 1.00 | (0.8–1.1) | 0.90 | (0.8–1.0) c | 1.00 | (0.9–1.1) b | 0.93 | (0.8–1.1) | 16.9 | <0.01 |
| Vitamin D (ng/mL) | 17.5 | (13.8–23.2) b,d | 21.8 | (16.5–27.7) a | 20.3 | (14.9–26.5) | 22.7 | (17.8–27.5) a | 33.7 | <0.01 |
| PH (pg/mL) | 64.3 | (50.4–79.1) | 64.1 | (50.7–81.1) | 63.8 | (47.8–78.7) | 61.4 | (49.7–77.4) | 3.3 | 0.35 |
| Insulin (μU/mL) | 9.1 | (6.7–11.6) b | 7.4 | (5.8–9.7) a,c,d | 9.0 | (7.7–13.2) b,d | 8.4 | (6.7–11.5) b,c | 69.0 | <0.01 |
| HOMA-IR | 2.98 | (2.2–4.2) b | 1.75 | (1.3–2.3) a,c,d | 3.13 | (2.3–4.5) b,d | 2.04 | (1.6–2.8) a,b,c | 215.7 | <0.01 |
| TyG Index | 4.80 | (4.6–5.1) b,c,d | 4.61 | (4.4–4.8) a,c,d | 4.93 | (4.8–5.2) a,b,d | 4.67 | (4.5–4.9) a,b,c | 130.0 | <0.01 |
| FPG (mg/dL) | 131.0 | (113.8–150.5) b,d | 94.0 | (88.0–102.0) a,c | 129.0 | (108.0–148.0) b,d | 96.0 | (90.0–103.8) a,c | 360.7 | <0.01 |
| HbA1C (%) | 6.8 | (6.2–8.1) | 6.8 | (6.2–7.6) | ||||||
| Women | ||||||||||
| Variables (Unit) | Sarcopenic diabetes a (n = 71) | Sarcopenia alone b (n = 312) | Diabetes alone c (n = 249) | Non-sarcopenia Band non-diabetes d (n = 1049) | K-W test | |||||
| Median | (IQR: Q1-Q3) | Median | (IQR: Q1-Q3) | Median | (IQR: Q1-Q3) | Median | (IQR: Q1-Q3) | H-value | p-value | |
| TC (mg/dL) | 197.0 | (161.0–225.0) | 198.5 | (180.0–222.0) | 195.0 | (166.0–220.0) | 199.0 | (176.0–223.0) | 4.4 | 0.22 |
| HDL-C (mg/dL) | 44.3 | (38.2–51.3) | 46.1 | (39.1–53.0) c | 44.3 | (36.5–50.4) b,d | 45.2 | (39.1–52.2) c | 10.0 | 0.02 |
| LDL-C (mg/dL) | 116.7 | (87.8–157.5) | 126.2 | (105.9–144.8) | 123.3 | (93.5–144.4) | 125.8 | (104.3–147.3) | 4.5 | 0.21 |
| Triglyceride (mg/dL) | 151.0 | (106.0–219.0) b,d | 125.0 | (86.0–175.0) a,c | 135.0 | (99.0–191.0) b,d | 122.0 | (88.0–177.0) a,c | 18.5 | <0.01 |
| Hemoglobin (g/dL) | 12.8 | (12.2–13.6) | 12.9 | (12.1–13.6) | 13.1 | (12.3–13.8) | 13.0 | (12.3–13.7) | 9.5 | 0.02 |
| Hematocrit (%) | 38.4 | (36.5–40.4) | 38.7 | (36.5–40.8) | 39.4 | (36.9–41.3) | 39.3 | (37.2–41.1) | 8.8 | 0.03 |
| Ferritin (ng/mL) | 50.1 | (26.9–89.2) | 58.9 | (38.2–90.2) | 62.8 | (36.6–94.1) | 60.5 | (37.5–90.7) | 3.0 | 0.40 |
| Urea nitrogen (mg/dL) | 15.0 | (12.0–19.0) | 15.0 | (12.0–18.0) c | 16.0 | (13.0–19.5) b | 15.0 | (13.0–19.0) | 10.3 | 0.02 |
| Creatinine (mg/dL) | 0.80 | (0.7–0.9) b,d | 0.70 | (0.6–0.8) a,c | 0.77 | (0.7–0.9) b,d | 0.70 | (0.6–0.8) a,c | 28.6 | <0.01 |
| Vitamin D (ng/mL) | 17.4 | (14.6–22.5) | 16.9 | (12.8–23.1) | 17.4 | (13.7–23.4) | 18.5 | (13.7–24.4) | 6.2 | 0.10 |
| PH (pg/mL) | 61.3 | (46.0–74.9) d | 63.7 | (49.8–84.4) | 66.7 | (50.7–84.9) | 66.9 | (53.0–85.3) a | 8.9 | 0.03 |
| Insulin (μU/mL) | 10.1 | (7.1–13.5) b | 8.7 | (6.9–10.7) a,c,d | 11.4 | (8.7–15.3) b,d | 9.2 | (7.3–11.9) b,c | 75.4 | <0.01 |
| HOMA-IR | 3.31 | (2.2–4.3) b,d | 2.00 | (1.6–2.5) a,c,d | 3.67 | (2.7–5.0) b,d | 2.15 | (1.6–2.8) a,b,c | 271.4 | <0.01 |
| TyG Index | 4.93 | (4.7–5.1) b,d | 4.69 | (4.5–4.9) a,c | 4.90 | (4.7–5.1) b,d | 4.68 | (4.5–4.9) a,c | 143.9 | <0.01 |
| FPG (mg/dL) | 130.0 | (98.0–159.0) b,d | 93.0 | (88.0–100.8) a,c | 129.0 | (113.5–144.5) b,d | 94.0 | (89.0–101.0) a,c | 479.1 | <0.01 |
| HbA1 C (%) | 6.9 | (6.2–7.9) | 6.9 | (6.4–7.6) | ||||||
| Men | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variables (Unit) | Sarcopenic Diabetes a (n = 126) | Sarcopenia Alone b (n = 458) | Diabetes Alone c (n = 135) | Non-Sarcopenia and Non-Diabetes d (n = 552) | K-W Test | |||||
| Median | (IQR: Q1–Q3) | Median | (IQR: Q1–Q3) | Median | (IQR: Q1–Q3) | Median | (IQR: Q1–Q3) | H-Value | p-Value | |
| Total energy (kcal) | 1680.2 | (1349.3–2142.9) d | 1729.8 | (1378.7–2071.3) c,d | 1919.5 | (1395.1–2305.4) b | 1832.5 | (1550.2–2336.6) a,b | 32.5 | <0.01 |
| Carbohydrate (g) | 298.4 | (242.9–354.5) d | 304.3 | (250.7–378.7) d | 333.4 | (248.2–395.5) | 325.8 | (274.3–399.8) a,b | 23.0 | <0.01 |
| Protein (g) | 52.0 | (37.6–73.2) c,d | 53.0 | (40.2–69.5) c,d | 65.1 | (44.5–82.8) a,b | 60.5 | (46.0–83.2) a,b | 34.6 | <0.01 |
| Fat (g) | 21.4 | (11.8–32.8) | 17.8 | (11.4–29.3) c,d | 25.1 | (13.9–41.4) b | 21.8 | (13.8–37.1) b | 25.8 | <0.01 |
| Crude Fiber (g) | 6.52 | (4.1–9.0) c | 6.15 | (4.3–8.8) c,d | 8.10 | (5.6–11.0) a,b | 6.75 | (4.7–10.1) b | 23.2 | <0.01 |
| Calcium (mg) | 364.8 | (213.1–600.5) | 354.1 | (220.4–535.1) c,d | 453.7 | (283.8–699.6) b | 407.2 | (283.1–609.6) b | 23.0 | <0.01 |
| Phosphorus (mg) | 990.1 | (707.1–1324.6) c,d | 976.1 | (768.0–1251.2) c,d | 1138.1 | (886.9–1434.0) a,b | 1117.2 | (875.4–1443.1) a,b | 37.4 | <0.01 |
| Iron (mg) | 11.2 | (6.7–17.2) c | 10.7 | (7.0–16.9) c,d | 14.4 | (8.9–19.3) a,b | 12.3 | (8.3–18.7) b | 23.3 | <0.01 |
| Sodium (mg) | 3668.3 | (2247.9–5374.8) c,d | 4044.6 | (2599.8–5681.0) d | 4213.6 | (2848.0–6560.1) a | 4466.3 | (3139.6–6285.3) a,b | 17.9 | <0.01 |
| Potassium (mg) | 2462.1 | (1627.4–3312.2) c,d | 2412.3 | (1784.8–3269.5) c,d | 2989.0 | (2143.0–4305.9) a,b | 2780.6 | (2031.3–3750.6) a,b | 36.9 | <0.01 |
| Thiamine (mg) | 0.93 | (0.7–1.4) c,d | 0.94 | (0.7–1.3) c,d | 1.07 | (0.8–1.6) a,b | 1.05 | (0.8–1.4) a,b | 30.6 | <0.01 |
| Riboflavin (mg) | 0.80 | (0.6–1.2) c | 0.79 | (0.5–1.1) c,d | 1.04 | (0.7–1.5) a,b | 0.89 | (0.6–1.3) b | 31.7 | <0.01 |
| Niacin (mg) | 11.5 | (8.4–17.3) c,d | 12.2 | (9.1–16.9) c,d | 14.9 | (10.9–19.8) a,b | 13.8 | (10.4–19.6) a,b | 35.6 | <0.01 |
| Vitamin A (μgRE) | 428.1 | (216.5–776.6) c | 388.4 | (197.8–780.6) c,d | 632.7 | (351.8–1032.0) a,b | 487.7 | (257.1–889.1) b | 28.5 | <0.01 |
| Vitamin C (mg) | 78.5 | (32.9–121.3) | 64.4 | (35.2–104.3) c,d | 88.3 | (55.1–147.1) b | 74.5 | (45.9–121.7) b | 19.6 | <0.01 |
| † Comparison of food intake over 24 h with usual intake (yes, n (%)) | Ate more than usual | 12 (9.5) | 24 (5.2) | 11 (8.1) | 31 (5.6) | 0.40 | ||||
| Ate the same as usual | 107 (84.9) | 417 (91.0) | 116 (85.9) | 503 (91.1) | ||||||
| Ate less than usual | 7 (5.6) | 17 (3.7) | 8 (5.9) | 17 (3.1) | ||||||
| Women | ||||||||||
| Variables (Unit) | Sarcopenic diabetes a (n = 71) | Sarcopenia alone b (n = 312) | Diabetes alone c (n = 249) | Non-sarcopenia and non-diabetes d (n = 1049) | K-W test | |||||
| Median | (IQR: Q1–Q3) | Median | (IQR: Q1–Q3) | Median | (IQR: Q1–Q3) | Median | (IQR: Q1–Q3) | H-value | p-value | |
| Total energy (kcal) | 1274.3 | (1072.1–1609.6) | 1273.5 | (975.4–1590.6) c,d | 1418.0 | (1125.1–1746.6) b | 1411.2 | (1109.1–1774.7) b | 27.9 | <0.01 |
| Carbohydrate (g) | 248.1 | (206.8–310.3) | 242.2 | (186.8–304.0) c,d | 279.5 | (212.5–340.2) b | 277.4 | (214.7–343.6) b | 35.1 | <0.01 |
| Protein (g) | 37.3 | (26.0–51.1) | 37.0 | (26.9–52.7) c,d | 43.0 | (31.6–57.1) b | 42.0 | (30.2–56.4) b | 16.7 | <0.01 |
| Fat (g) | 11.3 | (7.2–20.8) | 12.6 | (7.9–21.9) | 14.7 | (8.7–21.4) | 13.6 | (7.7–22.6) | 2.8 | 0.42 |
| Crude Fiber (g) | 4.76 | (3.4–7.4) | 4.29 | (2.8–6.9) c,d | 5.50 | (3.6–8.7) b | 5.25 | (3.4–8.1) b | 24.1 | <0.01 |
| Calcium (mg) | 260.1 | (144.6–451.2) | 272.5 | (153.4–437.5) c | 314.9 | (189.6–523.0) b | 292.8 | (176.1–449.7) | 10.1 | 0.02 |
| Phosphorus (mg) | 738.1 | (576.0–1002.8) | 713.3 | (527.5–985.8) c,d | 823.3 | (627.0–1060.6) b | 809.9 | (604.1–1047.7) b | 17.8 | <0.01 |
| Iron (mg) | 7.9 | (4.7–12.5) | 7.5 | (4.7–12.0) c,d | 9.8 | (6.2–16.2) b | 8.7 | (5.6–13.9) b | 21.2 | <0.01 |
| Sodium (mg) | 2364.9 | (1442.4–3450.6) c,d | 2605.3 | (1581.6–3905.1) c,d | 2963.5 | (2024.5–4377.5) a,b | 2895.2 | (1876.1–4451.9) a,b | 17.6 | <0.01 |
| Potassium (mg) | 1850.4 | (1366.3–2517.5) | 1754.1 | (1170.9–2514.5) c,d | 2008.1 | (1614.4–2986.4) b | 2064.6 | (1413.1–2900.5) b | 26.2 | <0.01 |
| Thiamine (mg) | 0.66 | (0.5–0.8) | 0.67 | (0.5–1.0) c,d | 0.75 | (0.6–1.0) b | 0.77 | (0.6–1.1) b | 20.6 | <0.01 |
| Riboflavin (mg) | 0.50 | (0.3–0.8) | 0.58 | (0.3–0.9) c | 0.69 | (0.5–1.0) b | 0.63 | (0.4–0.9) | 12.3 | <0.01 |
| Niacin (mg) | 8.4 | (6.5–11.1) | 8.2 | (6.0–12.0) c,d | 9.8 | (7.3–13.6) b | 9.7 | (7.0–13.2) b | 23.0 | <0.01 |
| Vitamin A (μgRE) | 268.0 | (132.4–599.4) | 330.1 | (137.6–654.3) c | 410.7 | (204.6–819.2) b | 357.2 | (151.5–685.6) | 9.3 | 0.03 |
| Vitamin C (mg) | 50.0 | (27.1–69.3) | 48.9 | (24.2–83.1) c,d | 60.2 | (28.1–98.4) b | 60.4 | (31.0–104.1) b | 19.4 | <0.01 |
| † Comparison of food intake over 24 h with usual intake (yes, n (%)) | Ate more than usual | 4 (5.6) | 13 (4.2) | 15 (6.0) | 80 (7.6) | 0.31 | ||||
| Ate the same as usual | 61 (85.9) | 282 (90.4) | 210 (84.3) | 887 (84.6) | ||||||
| Ate less than usual | 6 (8.5) | 16 (5.1) | 24 (9.6) | 80 (7.6) | ||||||
| Variables | Men | p-Value | |||
|---|---|---|---|---|---|
| Sarcopenic Diabetes a (n = 126) | Sarcopenia Alone b (n = 458) | Diabetes Alone c (n = 135) | Non-Sarcopenia and Non-Diabetes d (n = 552) | ||
| n (%) | n (%) | n (%) | n (%) | ||
| Flexibility exercise ≥ 2 days/week (yes) | 48 (38.1) | 160 (34.9) d | 60 (44.4) | 238 (43.1) b | 0.04 |
| Resistance training ≥ 2 days/week (yes) | 26 (20.6) | 87 (19.0) c,d | 43 (31.9) b | 155 (28.1) b | <0.01 |
| Moderate-intensity physical activity ≥ 150 min/week (yes) | 29 (23.0) | 109 (23.8) | 38 (28.1) | 161 (29.2) | 0.19 |
| Vigorous-intensity physical activity ≥ 75 min/week (yes) | 11 (8.7) c,d | 74 (16.2) c | 40 (29.6) a,b | 107 (19.4) a | <0.01 |
| Variables | Women | p-value | |||
| Sarcopenic diabetes a (n = 71) | Sarcopenia alone b (n = 312) | Diabetes alone c (n = 249) | Non-sarcopenia and non-diabetes d (n = 1049) | ||
| n (%) | n (%) | n (%) | n (%) | ||
| Flexibility exercise ≥ 2 days/week (yes) | 17 (23.9) | 98 (31.4) | 89 (35.7) | 311 (29.6) | 0.16 |
| Resistance training ≥ 2 days/week (yes) | 7 (9.9) | 20 (6.4) | 15 (6.0) | 82 (7.8) | 0.57 |
| Moderate-intensity physical activity ≥ 150 min/week (yes) | 5 (7.0) d | 58 (18.6) | 51(20.5) | 249 (23.7) a | <0.01 |
| Vigorous-intensity physical activity ≥ 75 min/week (yes) | 5 (7.0) | 34 (10.9) | 29 (11.6) | 149 (14.2) | 0.16 |
| Crude OR | (95% CI) | p-Value | Model 1 OR † | (95% CI) | p-Value | Model 2 OR ‡ | (95% CI) | p-Value | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Vigorous-intensity physical inactivity | ||||||||||
| Men | Non-sarcopenia and non-diabetes | 1.00 (reference) | ||||||||
| Sarcopenic diabetes | 2.87 | (1.54–5.37) | <0.01 | 2.78 | (1.47–5.33) | <0.01 | 2.68 | (1.42–5.19) | <0.01 | |
| Sarcopenia alone | 1.43 | (1.00–1.85) | 0.03 | 1.30 | (0.86–1.82) | 0.17 | 1.25 | (0.83–1.76) | 0.25 | |
| Diabetes alone | 0.65 | (0.43–0.98) | 0.04 | 0.66 | (0.44–1.01) | 0.06 | 0.66 | (0.43–1.01) | 0.05 | |
| Women | Non-sarcopenia and non-diabetes | 1.00 (reference) | ||||||||
| Sarcopenic diabetes | 2.15 | (0.87–4.26) | 0.08 | 1.96 | (0.78–3.89) | 0.13 | 1.93 | (0.76–3.84) | 0.14 | |
| Sarcopenia alone | 1.39 | (0.97–2.05) | 0.08 | 1.38 | (0.92–2.04) | 0.11 | 1.36 | (0.91–2.03) | 0.13 | |
| Diabetes alone | 1.35 | (0.90–2.00) | 0.15 | 1.35 | (0.91–2.04) | 0.15 | 1.35 | (0.90–2.04) | 0.15 | |
| Moderate-intensity physical inactivity | ||||||||||
| Men | Non-sarcopenia and non-diabetes | 1.00 (reference) | ||||||||
| Sarcopenic diabetes | 1.52 | (1.02–2.34) | 0.05 | 1.70 | (1.11–2.66) | 0.02 | 1.61 | (1.06–2.55) | 0.03 | |
| Sarcopenia alone | 1.39 | (1.05–1.76) | 0.01 | 1.57 | (1.12–2.09) | <0.01 | 1.49 | (1.06–1.99) | 0.02 | |
| Diabetes alone | 1.01 | (0.70–1.51) | 0.96 | 0.99 | (0.68–1.49) | 0.97 | 0.98 | (0.67–1.47) | 0.90 | |
| Women | Non-sarcopenia and non-diabetes | 1.00 (reference) | ||||||||
| Sarcopenic diabetes | 3.52 | (1.91–7.39) | <0.01 | 3.63 | (1.93–7.62) | <0.01 | 3.58 | (1.91–7.56) | <0.01 | |
| Sarcopenia alone | 1.34 | (1.02–1.74) | 0.04 | 1.40 | (1.02–1.84) | 0.03 | 1.37 | (1.01–1.81) | 0.04 | |
| Diabetes alone | 1.09 | (0.79–1.40) | 0.54 | 1.07 | (0.77–1.38) | 0.67 | 1.07 | (0.77–1.38) | 0.67 | |
| Not walking | ||||||||||
| Men | Non-sarcopenia and non-diabetes | 1.00 (reference) | ||||||||
| Sarcopenic diabetes | 0.91 | (0.54–1.57) | 0.74 | 0.94 | (0.55–1.68) | 0.83 | 0.91 | (0.53–1.64) | 0.75 | |
| Sarcopenia alone | 0.85 | (0.62–1.23) | 0.35 | 0.85 | (0.59–1.36) | 0.44 | 0.82 | (0.57–1.33) | 0.37 | |
| Diabetes alone | 0.50 | (0.30–1.02) | 0.03 | 0.51 | (0.30–1.03) | 0.04 | 0.50 | (0.30–1.03) | 0.04 | |
| Women | Non-sarcopenia and non-diabetes | 1.00 (reference) | ||||||||
| Sarcopenic diabetes | 1.99 | (1.34–3.54) | <0.01 | 1.69 | (1.14–3.18) | 0.05 | 1.70 | (1.14–3.19) | 0.05 | |
| Sarcopenia alone | 0.82 | (0.60–1.13) | 0.22 | 0.76 | (0.55–1.08) | 0.12 | 0.77 | (0.55–1.09) | 0.13 | |
| Diabetes alone | 1.09 | (0.83–1.57) | 0.59 | 1.11 | (0.84–1.62) | 0.55 | 1.11 | (0.84–1.62) | 0.55 | |
| <600 METs | ||||||||||
| Men | Non-sarcopenia and non-diabetes | 1.00 (reference) | ||||||||
| Sarcopenic diabetes | 1.70 | (1.14–2.61) | 0.01 | 1.69 | (1.14–2.71) | 0.02 | 1.61 | (1.08–2.58) | 0.03 | |
| Sarcopenia alone | 1.41 | (1.05–1.83) | 0.02 | 1.37 | (0.99–1.95) | 0.07 | 1.30 | (0.94–1.85) | 0.13 | |
| Diabetes alone | 0.86 | (0.56–1.39) | 0.51 | 0.87 | (0.56–1.40) | 0.56 | 0.85 | (0.55–1.38) | 0.51 | |
| Women | Non-sarcopenia and non-diabetes | 1.00 (reference) | ||||||||
| Sarcopenic diabetes | 2.48 | (1.58–4.15) | <0.01 | 2.41 | (1.53–4.15) | <0.01 | 2.37 | (1.50–4.07) | <0.01 | |
| Sarcopenia alone | 1.09 | (0.83–1.38) | 0.52 | 1.14 | (0.86–1.49) | 0.35 | 1.12 | (0.84–1.46) | 0.43 | |
| Diabetes alone | 1.17 | (0.87–1.50) | 0.28 | 1.13 | (0.83–1.46) | 0.41 | 1.12 | (0.83–1.46) | 0.43 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, M.; Kobori, T. Association of a Combination of Sarcopenia and Type 2 Diabetes with Blood Parameters, Nutrient Intake, and Physical Activity: A Nationwide Population-Based Study. Nutrients 2023, 15, 4955. https://doi.org/10.3390/nu15234955
Kim M, Kobori T. Association of a Combination of Sarcopenia and Type 2 Diabetes with Blood Parameters, Nutrient Intake, and Physical Activity: A Nationwide Population-Based Study. Nutrients. 2023; 15(23):4955. https://doi.org/10.3390/nu15234955
Chicago/Turabian StyleKim, Mijin, and Toshiro Kobori. 2023. "Association of a Combination of Sarcopenia and Type 2 Diabetes with Blood Parameters, Nutrient Intake, and Physical Activity: A Nationwide Population-Based Study" Nutrients 15, no. 23: 4955. https://doi.org/10.3390/nu15234955