

BMI and the Food Retail Environment in Melbourne, Australia: Associations and Temporal Trends
 , , , and
, , , and
Abstract
:1. Introduction
- Examine the association between the FRE at the postal code level and the BMI of a repeated cross-sectional sample of the adult population residing in those postal codes at four time points (2008, 2012, 2014, and 2016);
- Examine temporal trends at four time points over eight years in BMI across measures of the FRE.
2. Materials and Methods
2.1. Design
2.2. Study Region
2.3. Victorian Population Health Survey
2.4. Participants
2.5. Exposure Variables—Food Retail Environment
2.5.1. Data Collection and Definition of Measures
2.5.2. Geographical Area Level Definition
2.5.3. Food Retail Environment Measures of Accessibility and Availability
2.6. Outcome Measure and Potential Confounders
2.7. Statistical Analysis
3. Results
3.1. Food Environment Characteristics
3.2. Sample Characteristics
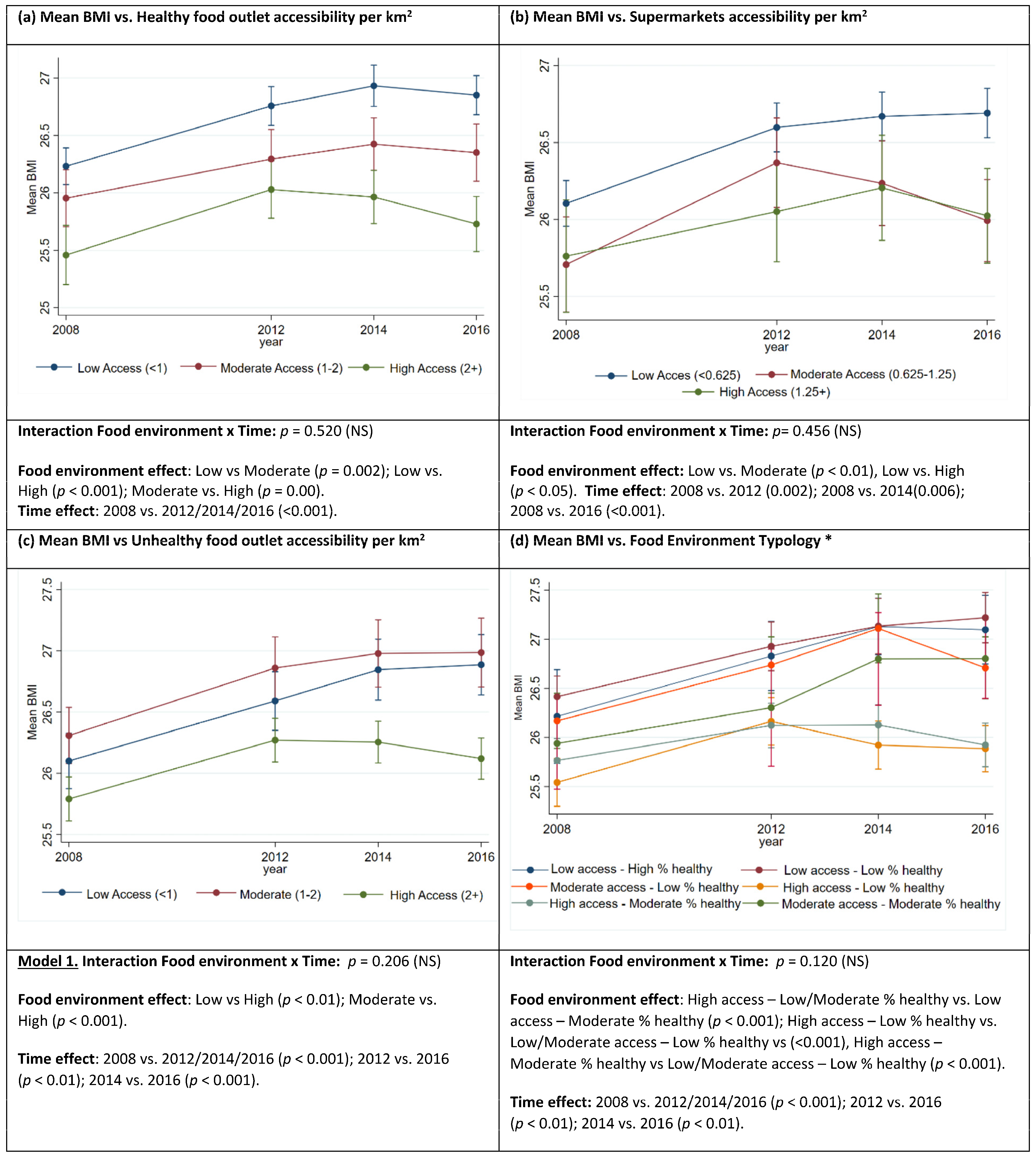
3.3. Relationship between BMI and Food Retail Environment Measures
3.4. Temporal Trends in BMI
4. Discussion
4.1. Strengths
4.2. Limitations
4.3. Implications for Population Health Policy and Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Development of an Implementation Roadmap 2023–2030 for the Global Action Plan for the Prevention and Control of NCDS 2013–2030; World Health Organization: Geneva, Switzerland, 2003.
- Swinburn, B.; Vandevijvere, S.; Kraak, V.; Sacks, G.; Snowdon, W.; Hawkes, C.; Barquera, S.; Friel, S.; Kelly, B.; Kumanyika, S.; et al. Monitoring and benchmarking government policies and actions to improve the healthiness of food environments: A proposed Government Healthy Food Environment Policy Index. Obes. Rev. 2013, 14 (Suppl. S1), 24–37. [Google Scholar] [CrossRef]
- Glanz, K.; Sallis, J.F.; Saelens, B.E.; Frank, L.D. Healthy nutrition environments: Concepts and measures. Am. J. Health Promot. 2005, 19, 330–333. [Google Scholar] [CrossRef]
- World Health Organization. Diet, Nutrition and the Prevention of Chronic Diseases; World Health Organization: Geneva, Switzerland, 2003.
- Swinburn, B.A.; Sacks, G.; Hall, K.D.; McPherson, K.; Finegood, D.T.; Moodie, M.L.; Gortmaker, S.L. The global obesity pandemic: Shaped by global drivers and local environments. Lancet 2011, 378, 804–814. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Care Excellence. Cardiovascular Disease Prevention; Public Health Guideline (PH25); National Institute for Care Excellence: London, UK, 2010. [Google Scholar]
- MHCLG. Planning Practice Guidance: Healthy and Safe Communities 2019. Available online: https://www.gov.uk/guidance/health-and-wellbeing (accessed on 13 October 2022).
- Public Health England. Using the planning system to promote healthier weight environments. In Guidance and Supplementary Planning Document Template for Local Authority Public Health and Planning Teams; Public Health England: London, UK, 2020. [Google Scholar]
- Brown, H.; Xiang, H.; Albani, V.; Goffe, L.; Akhter, N.; Lake, A.; Sorrell, S.; Gibson, E.; Wildman, J. No new fast-food outlets allowed! Evaluating the effect of planning policy on the local food environment in the North East of England. Soc. Sci. Med. 2022, 306, 115126. [Google Scholar] [CrossRef] [PubMed]
- Alston, L.; Raeside, R.; Jia, S.S.; Partridge, S.R. Underinvestment in nutrition research for atrisk populations: An analysis of research funding awarded in Australia from 2014 to 2021. Nutr. Diet. 2022, 79, 438–446. [Google Scholar] [CrossRef] [PubMed]
- Needham, C.; Sacks, G.; Orellana, L.; Robinson, E.; Allender, S.; Strugnell, C. A systematic review of the Australian food retail environment: Characteristics, variation by geographic area, socioeconomic position and associations with diet and obesity. Obes. Rev. 2019, 21, e12941. [Google Scholar] [CrossRef] [PubMed]
- Cobb, L.K.; Appel, L.J.; Franco, M.; Jones-Smith, J.C.; Nur, A.; Anderson, C.A.M. The relationship of the local food environment with obesity: A systematic review of methods, study quality, and results. Obesity 2015, 23, 1331–1344. [Google Scholar] [CrossRef] [PubMed]
- Gamba, R.J.; Schuchter, J.; Rutt, C.; Seto, E.Y.W. Measuring the food environment and its effects on obesity in the United States: A systematic review of methods and results. J. Community Health 2015, 40, 464–475. [Google Scholar] [CrossRef]
- Needham, C.; Strugnell, C.; Allender, S.; Orellana, L. Beyond food swamps and food deserts: Exploring urban Australian food retail environment typologies. Public Health Nutr. 2022, 25, 1140–1152. [Google Scholar] [CrossRef]
- Needham, C.; Orellana, L.; Allender, S.; Sacks, G.; Blake, M.R.; Strugnell, C. Food Retail Environments in Greater Melbourne 2008–2016: Longitudinal Analysis of Intra-City Variation in Density and Healthiness of Food Outlets. Int. J. Environ. Res. Public Health 2020, 17, 1321. [Google Scholar] [CrossRef]
- Lamb, K.E.; Thornton, L.E.; Olstad, D.L.; Cerin, E.; Ball, K. Associations between major chain fast-food outlet availability and change in body mass index: A longitudinal observational study of women from Victoria, Australia. BMJ Open 2017, 7, e016594. [Google Scholar] [CrossRef]
- Baldock, K.L.; Paquet, C.; Howard, N.J.; Coffee, N.T.; Taylor, A.W.; Daniel, M. Are Perceived and Objective Distances to Fresh Food and Physical Activity Resources Associated with Cardiometabolic Risk? Int. J. Environ. Res. Public Health 2018, 15, 224. [Google Scholar] [CrossRef]
- Feng, X.; Astell-Burt, T.; Badland, H.; Mavoa, S.; Giles-Corti, B. Modest ratios of fast food outlets to supermarkets and green grocers are associated with higher body mass index: Longitudinal analysis of a sample of 15,229 Australians aged 45 years and older in the Australian National Liveability Study. Health Place 2018, 49, 101–110. [Google Scholar] [CrossRef]
- Paquet, C.; Coffee, N.T.; Haren, M.T.; Howard, N.J.; Adams, R.J.; Taylor, A.W.; Daniel, M. Food environment, walkability, and public open spaces are associated with incident development of cardio-metabolic risk factors in a biomedical cohort. Health Place 2014, 28, 173–176. [Google Scholar] [CrossRef]
- Tseng, M.; Thornton, L.E.; Lamb, K.E.; Ball, K.; Crawford, D. Is neighbourhood obesogenicity associated with body mass index in women? Application of an obesogenicity index in socioeconomically disadvantaged neighbourhoods. Health Place 2014, 30, 20–27. [Google Scholar] [CrossRef]
- Walker, R.E.; Keane, C.R.; Burke, J.G. Disparities and access to healthy food in the United States: A review of food deserts literature. Health Place 2010, 16, 876–884. [Google Scholar] [CrossRef]
- Department of Health and Human Services. Victorian Population Health Survey: Victorian State Government. 2022. Available online: https://www.health.vic.gov.au/population-health-systems/victorian-population-health-survey (accessed on 1 August 2022).
- Department of Health and Human Services. Inequalities in the Social Determinants of Health and What It Means for the Health of Victorians: Findings from the 2014 Victorian Population Health Survey; Victorian State Government: Melbourne, Australia, 2014.
- Australian Bureau of Statistics. 3218.0—Regional Population Growth, Australia, 2008–2009; Commonwealth of Australia: Canberra, Australia, 2010. Available online: https://www.abs.gov.au/ausstats/abs@.nsf/Products/3218.0~2008-09~Main+Features~Main+Features?OpenDocument#:~:text=3218.0%20%2D%20Regional%20Population%20Growth%2C%20Australia%2C%202008%2D09&text=Australia’s%20estimated%20resident%20population%20(ERP,five%20years%20to%20June%202009 (accessed on 1 June 2019).
- Australian Bureau of Statistics. Census of Population and Housing: Socio-Economic Index for Areas (SEIFA), Australia, 2016; Commonwealth of Australia: Canberra, Australia, 2016.
- Department of Health and Human Services. Victorian Population Health Survey Victoria; Victorian State Government: Melbourne, Australia, 2021. Available online: https://www2.health.vic.gov.au/public-health/population-health-systems/health-status-of-victorians/survey-data-and-reports/victorian-population-health-survey (accessed on 12 January 2021).
- Department of Health and Human Services. Report 1: Victorian Population Health Survey 2014: Modifiable Risk Factors Contributing to Chronic Disease; Victorian State Government: Melbourne, Australia, 2014.
- Department of Health and Human Services. Victorian Population Health Survey 2016: Selected Survey Findings; Victorian State Government: Melbourne, Australia, 2018.
- Department of Health and Human Services. Victorian Population Health Survey 2008; State Government of Victoria: Melbourne, Australia, 2008.
- NBSP; Thornton, L.E.; Lamb, K.E.; Ball, K. Fast food restaurant locations according to socioeconomic disadvantage, urban–regional locality, and schools within Victoria, Australia. SSM—Popul. Health 2016, 2, 1–9. [Google Scholar] [CrossRef]
- Moayyed, H.; Kelly, B.; Feng, X.; Flood, V. Evaluation of a ‘healthiness’ rating system for food outlet types in Australian residential communities. Nutr. Diet. 2017, 74, 29–35. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. 1270.055.003—Australian Statistical Geography Standard (ASGS): Volume 2—Non ABS Structures, July 2016 Canberra. Available online: https://www.abs.gov.au/ausstats/abs@.nsf/Lookup/by%20Subject/1270.0.55.003~July%202016~Main%20Features~Postal%20Areas%20(POA)~8 (accessed on 25 May 2020).
- Raskind, I.G.; Kegler, M.C.; Girard, A.W.; Dunlop, A.L.; Kramer, M.R. An activity space approach to understanding how food access is associated with dietary intake and BMI among urban, low-income African American women. Health Place 2020, 66, 102458. [Google Scholar] [CrossRef]
- Wang, S.; Wang, M.; Liu, Y. Access to urban parks: Comparing spatial accessibility measures using three GIS-based approaches. Comput. Environ. Urban Syst. 2021, 90, 101713. [Google Scholar] [CrossRef]
- Zhang, X.; Lu, H.; Holt, J.B. Modeling spatial accessibility to parks: A national study. Int. J. Health Geogr. 2011, 10, 31. [Google Scholar] [CrossRef]
- Crothers, L. Australia Retail Foods: Retail Food Sector Report 2019. USDA Foreign Agricultural Service: Global Agricultural Information Network. 2019. Available online: https://apps.fas.usda.gov/newgainapi/api/report/downloadreportbyfilename?filename=Retail%20Foods_Canberra_Australia_6-27-2019.pdf (accessed on 18 July 2020).
- Thornton, L.E.; Lamb, K.E.; White, S.R. The use and misuse of ratio and proportion exposure measures in food environment research. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 118. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. 1270.0.55.001—Australian Statistical Geography Standard (ADGS): Volume 1—Main Structure and Greater Capital City Statistical Areas, July 2016: Australian Federal Government; 2016 [updated July 2016]. Available online: https://www.abs.gov.au/ausstats/abs@.nsf/Lookup/by%20Subject/1270.0.55.001~July%202016~Main%20Features~Statistical%20Area%20Level%202%20(SA2)~10014 (accessed on 25 May 2019).
- Australian Bureau of Statistics (ABS). Estimated Resident Population (ERP) and Components by LGA (ASGS 2018) 2001 to 2018; Commonwealth of Australia: Canberra, Australia, 2018.
- Miller, L.J.; Joyce, S.; Carter, S.; Yun, G. Associations between childhood obesity and the availability of food outlets in the local environment: A retrospective cross-sectional study. Am. J. Health Promot. 2014, 28, e137–e145. [Google Scholar] [CrossRef]
- Abbott, G.; Backholer, K.; Peeters, A.; Thornton, L.; Crawford, D.; Ball, K. Explaining educational disparities in adiposity: The role of neighborhood environments. Obesity 2014, 22, 2413–2419. [Google Scholar] [CrossRef]
- Thornton, L.E.; Crawford, D.A.; Ball, K. Neighbourhood-socioeconomic variation in women’s diet: The role of nutrition environments. Eur. J. Clin. Nutr. 2010, 64, 1423–1432. [Google Scholar] [CrossRef]
- Crawford, D.A.; Timperio, A.F.; Salmon, J.A.; Baur, L.; Giles-Corti, B.; Roberts, R.J.; Jackson, M.L.; Andrianopoulos, N.; Ball, K. Neighbourhood fast food outlets and obesity in children and adults: The CLAN Study. Pediatr. Obes. 2008, 3, 249–256. [Google Scholar] [CrossRef]
- Burgoine, T.; Sarkar, C.; Webster, C.J.; Monsivais, P. Examining the interaction of fast-food outlet exposure and income on diet and obesity: Evidence from 51,361 UK Biobank participants. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 71. [Google Scholar] [CrossRef]
- De Vogli, R.; Kouvonen, A.; Gimeno, D. ‘Globesization’: Ecological evidence on the relationship between fast food outlets and obesity among 26 advanced economies. Crit. Public Health 2011, 21, 395–402. [Google Scholar] [CrossRef]
- Wool, J.L.; Walkinshaw, L.P.; Spigner, C.; Thayer, E.K.; Jones-Smith, J.C. A Qualitative Study of Living in a Healthy Food Priority Area in One Seattle, WA, Neighborhood. Int. J. Environ. Res. Public Health 2021, 18, 12251. [Google Scholar] [CrossRef]
- Tach, L.; Amorim, M. Constrained, Convenient, and Symbolic Consumption: Neighborhood Food Environments and Economic Coping Strategies among the Urban Poor. J. Urban Health 2015, 92, 815–834. [Google Scholar] [CrossRef]
- Christian, T.J. Grocery Store Access and the Food Insecurity–Obesity Paradox. J. Hunger. Environ. Nutr. 2010, 5, 360–369. [Google Scholar] [CrossRef]
- Ng, S.P.; Korda, R.; Clements, M.; Latz, I.; Bauman, A.; Bambrick, H.; Liu, B.; Rogers, K.; Herbert, N.; Banks, E. Validity of self-reported height and weight and derived body mass index in middle-aged and elderly individuals in Australia. Aust. New Zealand J. Public Health 2011, 35, 557–563. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. Statistical Geography Explained: Australian Bureau of Statistics. 2022. Available online: https://www.abs.gov.au/statistics/statistical-geography/statistical-geography-explained (accessed on 7 November 2022).
- Dornelles, A. Impact of multiple food environments on body mass index. PLoS ONE 2019, 14, e0219365. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.; Badland, H.; Jordan, H.; Koohsari, M.J.; Giles-Corti, B. Local Food Environments, Suburban Development, and BMI: A Mixed Methods Study. Int. J. Environ. Res. Public Health 2018, 15, 1392. [Google Scholar] [CrossRef] [PubMed]
- Growth Areas Authority. Precinct Structure Planning Guidelines Part Two: Preparing the Precinct Structure Plan; Victorian State Government: Melbourne, Australia, 2013.


{kind=link}
| Measures | Classification | ||
|---|---|---|---|
| Relative healthy food availability (RHFA) | Proportion healthy food resources | Availability | |
| No food retail * ≤25% | Low | ||
| >25 to-≤50% | Moderate | ||
| >50% | High | ||
| Food retail accessibility measures (FRAMs) | Count per km2 | Access | |
| Healthy, less healthy, unhealthy | <1 | Low | |
| ≥1 to <2 | Moderate | ||
| ≥2 | High | ||
| Supermarkets | <0.625 | Low | |
| 0.625 to <1.25 | Moderate | ||
| ≥1.25 | High | ||
| Food environment typology ** | FRAMs *** | RHFA | Typology |
| Low | ≤25% | Low access—Low % healthy | |
| Low | >25% to ≤50% | Low access—Moderate % healthy | |
| Low | >50% | Low access—High % healthy | |
| Moderate | ≤25% | Moderate access—Low % healthy | |
| Moderate | >25% to ≤50% | Moderate access—Moderate % healthy | |
| Moderate | >50% | Moderate access—High % healthy | |
| High | ≤25% | High access—Low % healthy | |
| High | >25% to ≤50% | High access—Moderate % healthy | |
| High | >50% | High access—High % healthy | |
| Year | |||||
|---|---|---|---|---|---|
| Characteristics | Categories | 2008 (n = 12,526) | 2012 (n = 11,246) | 2014 (n = 11,760) | 2017 (n = 11,713) |
| Age (%) | 18–30 | 12.9 | 9.0 | 5.6 | 15.3 |
| 31–40 | 17.6 | 14.2 | 10.2 | 15.1 | |
| 41–50 | 19.9 | 20.3 | 17.0 | 15.4 | |
| 51–60 | 18.7 | 21.2 | 20.8 | 17.4 | |
| 61–70 | 16.5 | 19.4 | 23.7 | 19.6 | |
| 71+ | 14.4 | 16.0 | 22.8 | 17.2 | |
| Gender (%) | Male | 39.8 | 40.5 | 41.9 | 47.1 |
| Female | 60.2 | 59.6 | 58.1 | 52.9 | |
| Education (%) | Primary school/some-high school/other | 27.2 | 21.9 | 20.7 | 14.8 |
| Completed High school/TAFE */trade | 37.1 | 39.3 | 39.9 | 36.2 | |
| Tertiary | 35.7 | 38.9 | 39.4 | 49.0 | |
| Household income (%) | <$20,000 | 13.2 | 11.1 | 9.8 | 4.4 |
| ≥$20 to <40,000 | 17.1 | 15.3 | 17.0 | 16.4 | |
| ≥$40 to <60,000 | 12.9 | 12.0 | 12.0 | 11.6 | |
| ≥$60 to <80,000 | 11.6 | 9.7 | 8.8 | 9.3 | |
| ≥$80 to <100,000 | 8.1 | 9.5 | 8.3 | 8.6 | |
| ≥$100,000+ | 19.8 | 25.3 | 18.3 | 32.8 | |
| Unknown/not reported | 17.4 | 17.1 | 25.8 | 17.0 | |
| Employment status (%) | Employed ** | 55.6 | 56.1 | 49.2 | 58.0 |
| Unemployed | 3.1 | 3.4 | 3.3 | 3.7 | |
| Home duties | 8.8 | 6.5 | 5.0 | 4.4 | |
| Student | 3.3 | 3.1 | 2.4 | 3.8 | |
| Retired | 25.7 | 28.2 | 37.0 | 26.8 | |
| Unable to work | 3.4 | 2.6 | 2.7 | 2.7 | |
| Other | 0.3 | 0.1 | 0.5 | 0.7 | |
| Length of time lived in (%) neighbourhood/area/council/local government area. | <5 years | 27.3 | 17.4 | 17.3 | 32.2 |
| 5–10 years | 18.2 | 17.9 | 15.9 | 14.7 | |
| 10+ years | 54.5 | 64.8 | 66.8 | 53.2 | |
| BMI mean (standard deviation) | 26.0 (5.3) | 26.5 (5.3) | 26.6 (5.2) | 26.5 (5.4) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Needham, C.; Strugnell, C.; Allender, S.; Alston, L.; Orellana, L. BMI and the Food Retail Environment in Melbourne, Australia: Associations and Temporal Trends. Nutrients 2023, 15, 4503. https://doi.org/10.3390/nu15214503
Needham C, Strugnell C, Allender S, Alston L, Orellana L. BMI and the Food Retail Environment in Melbourne, Australia: Associations and Temporal Trends. Nutrients. 2023; 15(21):4503. https://doi.org/10.3390/nu15214503
Chicago/Turabian StyleNeedham, Cindy, Claudia Strugnell, Steven Allender, Laura Alston, and Liliana Orellana. 2023. "BMI and the Food Retail Environment in Melbourne, Australia: Associations and Temporal Trends" Nutrients 15, no. 21: 4503. https://doi.org/10.3390/nu15214503