
A Scoping Review of Nutrition Health for Older Adults: Does Technology Help?

Abstract
:1. Introduction
1.1. Biological Aging and Nutrition
1.2. The Nutrition Care Process
1.3. Accessing Nutrition Professionals and Services
1.4. Technology for Aging
1.5. Research Objective
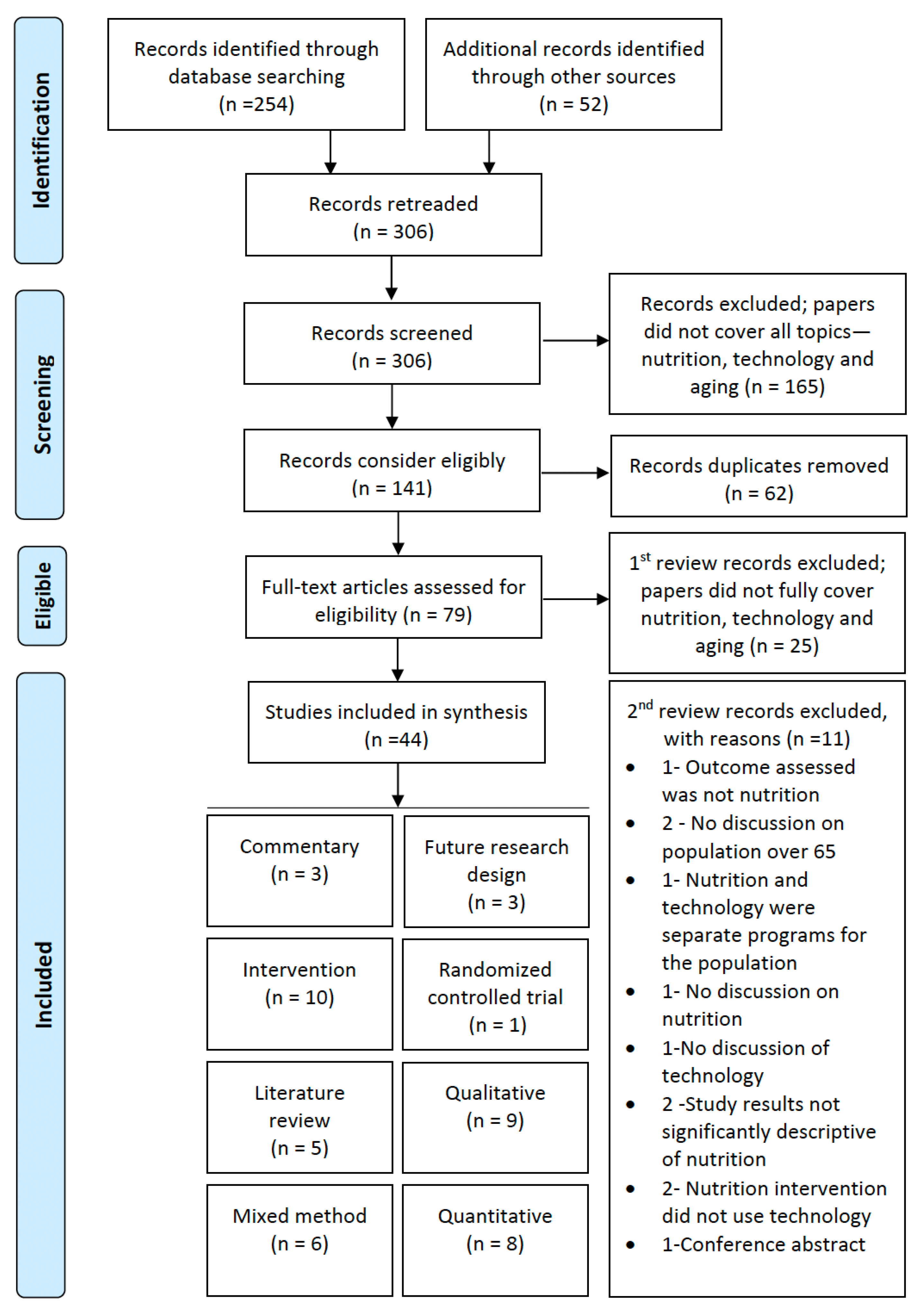
2. Materials and Methods
2.1. Research Methods
2.2. Eligibility Criteria
2.3. Study Selection
2.4. Data Charting

{kind=link}
{kind=link}
{kind=link}
| ID | Authors | Type of Study | Population | Type of Technology | Location | Purpose | Medical/Nutrition Outcomes |
|---|---|---|---|---|---|---|---|
| S1 | Ali et al., 2013 [52] | INT | Age 60–74 years, n = 6 | Computer, software (3D animation enhancement to existing software for nutritional education) via an information kiosk | Kuala Lumpur, Malaysia | Investigate 3D animation software to develop nutritional education software using interface user design guidelines specific to older adults. Lack of computer literacy and impaired perception and cognition create a limitation in older adults’ use of computers. Assisted computer interaction with 3D animation may address that concern. | The 3D animation software helped facilitate older adults understanding of nutritional education content. Compared with a control group that used booklets, each group completed tasks, and the digital software user explored content using the software package faster than those using the traditional booklet. |
| S2 | Angelini et al., 2016 [53] | Qual | Age 65 years and older aging at home, age 60 and older impending retirement, n = 100 | Various types of information communication and technology: senior living lab, promoting aging at home with multidisciplinary co-creation of social and technology innovative products, services, and practices for older adults | Romandy, Switzerland | Co-creation of services and products for older adults adheres to an ecological approach to promote healthy aging. Using technology in the background to support healthy nutrition to cope with frailty, improved autonomous mobility to foster independence, and social communication of older adults. This study describes the roles technologies can have when co-creating with older adults, the methods needed, and the challenges. | This study discusses challenges that emerged during the first year of creating this new platform for investigating the role of information communication and technology (ICT) when designing products and services for older adults. Older adults are insecure with ICTs. The causes vary with age, culture, health conditions, and application context. |
| S3 | Astell et al., 2014 [3] | Quant | Mean age 71.9 years (range 65–89), n = 40 | Touch screen tablet computer, webcam, software (NANA) | Sheffield and St. Andrews, U.K. | Novel Assessment of Nutrition and Aging (NANA) validation study of older adults self-reported diet intake using a touch screen computer. The study also examined if data collection can occur over several nonconsecutive weeks. Bland–Altman analysis was used to explore differences between energy and macronutrient intake data. | The NANA toolkit was compared with standard measures of diet (four-day food diary), cognitive ability (processing speed), and physical activity. Data collected with the NANA toolkit were significantly correlated with a standard food diary, cognitive processing speed, and physical activity measures. |
| S4 | Aure et al., 2020 [54] | Qual | Mean age 81 years (range, 68–95), n = 18 | Tablet computer, software (APPetitus), mobile internet access | Three Norwegian municipalities | Undernutrition remains a prevalent and persistent problem among older adults. This study explored whether a tablet-based application supported nutritional self-care among older adults. | The app served as a reminder of available, relevant food options. By the end of the day, it encouraged some participants to eat or drink more, whereas others became aware of food selection options to ensure sufficient protein, energy, and fluids. Some participants made no effort to change their diet despite feedback that they did not eat or drink enough. Findings confirm the feasibility of using technology in nutrition interventions for older adults. Technical support from health professionals facilitated app and tablet use. |
| S5 | Batsis et al., 2019 [55] | MM | Older adults, mean age 72.9 years (SD 4.6), n = 29; clinicians, mean age 47.7 years (SD 12.1), n = 7; community leaders, mean age 64.3 years (SD 8.73), n = 4; total n = 40 | Fitness device, home-based sensors | New Hampshire, U.S. | Mobile Health Obesity Wellness Intervention (MOWI) in rural older adults with obesity, consisting of nutrition and exercise sessions, could be helpful to improve physical function and create accountability. The study purpose was to explore how technology could improve the health of rural older adults with obesity. | Older rural adults with obesity are interested in using technologies to improve their health. Barriers to implementation exist based on technology complexity and access. Clinicians and community leaders believed that technology could help provide older adults insight into health, create accountability, and motivate behavior change. |
| S6 | Batsis et al., 2020 [56] | INT, Qual | Older adults, mean age 72.9 years (SD 4.6), n = 29; clinicians, mean age 47.7 years (SD 12.1), n = 7; community leaders, mean age 64.3 years (SD 8.73), n = 4; total n = 40 | Tablet computer, software, telehealth via internet video devices, fitness device (obesity wellness) | New Hampshire, U.S. | Patient-oriented feedback with self-aware messaging based on adaptable sensor technologies was promising for eliciting behavioral change and could improve physical function and reduce obesity. This study sought to understand how a potential Mobile Health Obesity Wellness Intervention (MOWI) among older adults with obesity could enhance physical functioning. The remote intervention consisted of weekly nutrition counseling and biweekly exercise sessions. | There is potential acceptability and value for implementing a rural, telehealth-delivered intervention for older adults with obesity. Participants saw the potential of MOWI in overcoming geographic barriers to accessing healthcare for rural communities and creating accountability for participants. Participant feedback about improving implementation included adding regular social connectedness to the program. |
| S7 | Beasley et al., 2019 [57] | INT, MM | Mean age 70.1 years (SD 5.6), n = 16 | Fitness device, videoconferencing | New York City, U.S. | As of 2018, Medicare has covered the Diabetes Prevention Program (DPP), making it more accessible to older adults. This study tested the feasibility and acceptability of implementing a telehealth-adapted 6-week DPP at a New York City senior center. Feedback can be incorporated to design an effective trial. | Of the 16 participants recruited, retention was 75%, and the attendance rate averaged 80% across the six sessions. Focus groups provided positive opinions and suggested a greater focus on dietary strategies. |
| S8 | Cabrita et al., 2019 [54] | Qual | Mean age 69 years (range 65–78), n = 12 | Mobile phone, fitness device, smart scale, software (Activity Coach) | Overijssel, Netherlands | Low adherence to technologies to self-manage health among older adults may occur because their preferences are not considered when designing new health care technologies. This study examined older adults’ (1) current practices in health management; (2) attitudes toward technology to support healthy behaviors, including nutrition, physical and cognitive functioning, and well-being; (3) wishes and expectations from technology; and (4) attitudes toward using technology in health management after monitoring weight, physical functioning, and daily emotions for 1 month. | Participants saw an added value of using technology. Attitudes and wishes for technology to support health differed by health domain (i.e., nutrition, cognition, physical functioning, well-being). All participants saw the importance of keeping track of their diet, but 50% of participants would not use a website or an app to monitor diet. Participants were not aware of how technology could manage nutrition. Some wished they could receive healthy recipes tailored to medical needs. Fears around technology included: identity theft, replacement of human touch, and disuse of existing abilities. After 1 month of using technology, attitudes improved. Technology that supports aging in place should target health literacy. |
| S9 | Chiu et al., 2019 [58] | INT, MM | Mean age 65.0 years (SD 8.33); group 1, age range 50–60 years, n = 6; group 2, age older than 65 years, n = 15; total n = 21 | Touch screen tablet computer, internet, software (health knowledge) | Taiwan | Understanding whether mobile technologies support self-directed learning for older adults is unclear. This study assessed if nutrition education combined with mobile technology-supported teaching increases participant knowledge of and self-efficacy for a healthy diet. | Participants’ nutrition knowledge significantly improved; self-efficacy about a healthy diet showed marginal improvement. Nutrition knowledge was positively correlated with intensity of surfing the Internet or reviewing the electronic course material. Participants reported feeling “freshness”, “joyfulness”, and “great achievement” because of the combined course. Those who reviewed the electronic course material or searched for health information online showed a significantly greater understanding of and self-efficacy for a healthy diet. |
| S10 | Dugas et al., 2018 [59] | Quant, INT | Mean age 67.6 years (SD 5.8), n = 27 | Tablet computer, fitness device, software (DiaSocial) | Maryland, U.S. | MHealth tools’ effectiveness in managing chronic diseases, such as diabetes, warrants further exploration. Investigate the effectiveness of the mHealth app—intended to track glucose, exercise, nutrition, and medication adherence—for improving health behaviors among older veterans with poorly controlled type 2 diabetes using a 13-week pilot study. | Effectiveness of an intervention is conditional on locomotion, whereas eagerness to engage is motivated by goal app settings. Program adherence was associated with a more significant reduction in glycated hemoglobin (HbA1c) levels. |
| S11 | Espín et al., 2016 [60] | FRD | Older adults | Computer, tablet computer, developed software (NutElCare) | Granada, Spain | This paper presents NutElCare, a nutritional recommendation system to help older adults develop healthy diet plans based on nutritional guidelines. This study highlights outcomes of nutritional recommender systems and the design and components of NutElCare; future directions are provided. | The research design for an app developed specifically for older adults provides recommendations based on expert guidelines for older adults to develop a diet plan. As an end-user influencer, the app includes adapting taste preferences. |
| S12 | Farsjø et al., 2019 [23] | Qual | Group 1, older adults, mean age 78 years (range 41–96), n = 29; group 2, health care professionals, mean age 43 years (range 23–65), n = 24 | Tablet computer, software (APPetitus), mobile internet access | Three Norwegian municipalities | Report the development of a nutrition application and the introduction of the app to healthcare professionals and older adults in-home care. Understand if healthcare professionals believe the apps are relevant and identify barriers to using the app for nutrition. | Access to technology enables older adults to take an active role in health monitoring. Goals for meeting enabled access include ease of use, support for the technology, and relevant app content. |
| S13 | Göransson et al., 2020 [61] | INT | Mean age 86.0 years (SD 6.5), n = 17 older adults receiving home care | Smartphone, tablet computer, developed software (Interaktor) | Southwestern Sweden | Despite the increased use of mHealth tools in various populations, few studies have targeted older adults receiving home care services. Determine areas relevant to older adults’ health and self-care for regular assessment of support using a developed application for older adults receiving home care. Describe older adults’ usage of the app and evaluate the impact on health and health literacy over 6 months. | Findings show that older adults increased their communication and literacy knowledge through the application. This study highlights the importance of applications specifically designed for older adults. However, overall health among older adults did not improve at six months. Common self-reported health concerns that could impact nutrition include: difficulty performing activities of daily living, constipation, diarrhea, loss of appetite, difficulty eating. |
| S14 | Hendrie et al., 2017 [62] | Quant | Group 1, age 18–30 years, n = 44,534; group 2, age 31–50 years; n = 52,599; group 3, age 51–70 years; n = 44,096; group 4, age 71+ years; total n = 145,975 | Online survey (CSIRO healthy diet score survey) | Australia | This paper describes the research and user experience of the survey and summarizes how compliant self-reported diets are with the Australian dietary guidelines. | The development of an online survey estimates user compliance with dietary guidelines using an established healthy diet score. The study provided a one-time assessment in three areas where the survey user could improve. Although not statistically significant, adults 51–70 years and 70+ years had higher dietary scores than adults 50 years and younger. |
| S15 | Hermann et al., 2012 [63] | Quant | Older adults, n = 100 | Devices (assistive technology and appropriate software) | Oklahoma, U.S. | This study was performed to empower older adults with technology to shop, cook, and eat using an education program. Evaluate the effectiveness of a curriculum to increase awareness of assistive technology to manage food and nutrition. | Significant increases in awareness of the importance of nutrition, understanding, and likeliness of using information, and awareness and use of assistive technology devices. Likelihood of older adult contacting a government-sponsored assistive technology program increased. |
| S16 | Kaddachi et al., 2018 [6] | Quant | Mean age 88.3 years (SD 4.5), n = 9 | Inconspicuous technologies:
| France | Identify significant behavior change indicators using statistical techniques that differentiate long-term and short-term changes in behavior. Early detection of long-term behavior changes in mobility, memory, nutrition, and social life indicators is important for improving older adults’ healthcare services. | Sensor data about the presence or absence of movements allows behavior change analysis, as seen in activity periods, room entries, sleep impairment, visits, time outdoors, and nutritional activities. |
| S17 | Kirkpatrick et al., 2017 [64] | Quant | Four-part study: S1, age 2–5 years, n = 40; S2, age 10–13 years, n = 294; S3, age 10–13 years, n = 98; S4, age 36–82 years, n = 331; S5, age 48–88 years, n = 264 | Various: smartphone, desktop, laptop, and tablet computer; internet; online survey (Automated Self-Administered 24 h) (ASA24) | Canada | Describe lessons learned from five studies that assessed the feasibility and validity of ASA24 for collecting dietary recall data among several population subgroups in Canada. | High acceptance of ASA24 was found among diverse samples. The ASA24 interface was not intuitive for young children and older adults; technological issues were encountered. The findings highlight the importance of piloting protocols and consideration of tailored resources to support participants. Older adults appeared to be more patient than younger adults by completing multiple passes to collect recall data. |
| S18 | LaMonica et al., 2017 [65] | Quant | Mean age 67.6 years (SD 8.5), n = 221 | Computer, smartphone, internet, website resources (health-related) | Sydney, Australia | The rapid increase in electronic health technologies warrants exploring whether these tools can be used for older adults with mild cognitive impairment. Describe patterns of Internet use and interest in and preferences for eHealth technologies among older adults with cognitive impairment. Prevalence data needed to determine the feasibility of future eHealth efforts for the aging population were collected. | Most participants used mobile phones (91.4%) and computers (86.1%) and had access to the Internet (92.6%). Preferences for other eHealth interventions varied with educational level; university-educated participants expressed greater interest in interventions related to mood (p = 0.01), socialization (p = 0.02), memory (p = 0.01), and computer-based exercises. eHealth preferences varied with the diagnosis for interventions targeting sleep, nutrition, vascular risk factors, and memory. |
| S19 | Lete et al., 2020 [66] | Lit Rev | Older adults | Wearable devices (e.g., physical, affective, cognitive, clinical), sensors (e.g., physical, affective, cognitive, clinical, furniture, objects) | Spain | Virtual coaching is a promising option to help extend older adults’ time to live interdependently. Present a survey of different approaches in virtual coaching for older adults. | Coaching should be considered holistically, including physical and cognitive training, nutrition (self-management of weight and healthy eating behavior), social interaction, and mood. |
| S20 | Lindhardt & Nielsen, 2017 [67] | MM, INT | Mean age 79.85 years (SD 7.85), n = 25 | Tablet computer, developed software (nutrition application), internet | Denmark | Weight loss and low dietary intake during and after hospitalization are common among older adults and can impact health outcomes. Assess the acceptability, feasibility, and preliminary efficacy of technology-supported energy- and protein-enforced home-delivered meals for older adults discharged from the hospital. | Participants were motivated and capable of using the device; technology challenges were related to the immaturity of the out-of-hospital app version. Inclusion and retention were challenged by exhaustion among patients and the acceptability of the nutrition intervention; the mortality rate was high. The intervention group increased their muscle strength more consistently than the control group. |
| S21 | Łukasik et al., 2018 [4] | MM | Group 1, older adults, mean age 75.3 years (SD 8.4), n = 126; group 2, caregivers, mean age 38.5 years (SD 13.0), n = 126; total n = 252 | Assistive robot | France, Greece, Italy, Poland, Great Britain | Rapid development of new technologies has sparked interest in the use of assistive robots in managing the care of older adults. The study aimed to answer how both older people and caregivers perceive the possibility of using an assistive robot for nutritional support. | The diet of older adults was improved by advice on healthy eating or monitoring to improve diet. An age-related difference was observed. Older adults less frequently accepted reminders of mealtimes or drinking liquids than younger adults. |
| S22 | Manea & Wac, 2020 [68] | Qual | Mean age 69.8 years (SD 7.4), n = 39 | Fitness device | Hungary, Spain | This study showed the feasibility of a co-calibration method, coQoL, by quantifying relationships between patient-reported outcomes (PROs) and technology-reported outcomes (TechROs); PROs included nutrition, physical activity, social support, anxiety, depression, memory, quality of life, and sleep. The study assessed the quality of data collected from a wearable technology fitness device, while participants’ daily lives unfolded to inform the design of personalized behavioral studies. | High PROs and TechROs correlated with physical activity, social support, anxiety, and sleep of various durations. The coQoL method feasibly co-calibrates constructs within seniors’ physical behaviors and psychological states. Some PRO nutrition outcomes assessing Mediterranean dietary patterns and malnutrition had strong correlations with TechRO data. |
| S23 | Marshall et al., 2017 [69] | Lit Rev | Age 65 years and older | Telehealth (nutrition care) | Australia | The demand for both domiciliary and family caregivers to provide in-home assistance for older adults, including food-related tasks, is increasing. A narrative review summarized the role of both domiciliary and family caregivers in providing individualized nutrition support for community-dwelling older adults with malnutrition. | Interventions reviewed including telehealth, group education, and skill development workshops show promise to improve outcomes of older adults. There is moderate evidence to support the inclusion of family caregivers as part of the nutrition care team. Moderate evidence supports the role of domiciliary caregivers in implementing nutrition screening and referrals and implementing malnutrition interventions with the support of health care professionals. |
| S24 | Marx et al., 2018 [70] | Lit Rev, MM | Age 65 years and older | Telehealth via telephone or internet video devices (malnutrition-related care) | Brisbane, Australia; Oslo, Norway; Greifswald, Germany; “possibly Singapore or Malaysia;” Aarhus, Denmark; Herlev, Denmark; Netherlands | The effectiveness of telehealth to improve malnutrition among older adults requires exploration and understanding if health care resources may be appropriately engaged. Deliver malnutrition-related interventions to a group of community-dwelling older adults. | Malnutrition-related telehealth interventions for older adults living at home may improve quality of life and dietary intake. The approach seems feasible and cost-effective. Data suggest telehealth may improve nutrition status, physical function, hospital readmission, and mortality. |
| S25 | McCabe et al., 2001 [24] | COM | Age 65 years and older | Telehealth via internet videoconferencing (medical nutrition therapy) | Arkansas, U.S. | Describe the use of telehealth for nutrition counseling of older adults in rural areas and the participation of dietitians in video technology for healthcare delivery. | Videoconferencing has provided rural hospitals with healthcare information and education for more than 6000 services to 45 rural facilities. Clinical consultations include access to information that may not have been otherwise available and access to specialists like dietitians for individual or group collaboration. A videoconferencing nutrition consultation is described, as is the role of the caregiver during these virtual nutrition consultations. |
| S26 | McCauley et al., 2019 [71] | COM | Age 65 years and older | Software (malnutrition quality improvement integrated into electronic health care records) | U.S. | The purpose of the Malnutrition Quality Improvement Initiative (MQii) is to: (1) serve as a toolkit used by an interdisciplinary team to improve the effectiveness and timeliness of malnutrition care; (2) facilitate the adoption of malnutrition electronic clinical quality measures (eCQMs) to help improve health outcomes; and (3) expand the availability of tools that can be integrated into electronic health record (HER) systems to minimize administrative burden and improve quality of care and documentation. | Innovations included the development of electronic clinical measures of malnutrition, such as global composite measures and a complementary interdisciplinary quality improvement toolkit. The initiative established the first nutrition-focused national learning collaborative. |
| S27 | Moguel et al., 2019 [72] | Lit Rev | Age 65 years and older | Food intake monitoring technology solutions:
| Spain | Studying the extant literature is necessary to understand if technology is a viable solution for older adults in rural settings. Evaluate the suitability of food intake monitoring systems for older adults in rural regions and existing technological proposals for food intake monitoring. | A complete solution for monitoring the diet of older adults in a rural setting does not exist. Future efforts should include technology that identifies the user, addresses a solution for uploading user data, enhances self-service treatment solutions, and incorporates self-adaptive demographic profiling solutions to bridge the gap between users and technology knowledge. |
| S28 | Ploeg et al., 2019 [73] | Qual | Mean age 78.7 years (SD 6.1), n = 32 | Tablet computer, software (collection of information health risk, needs, and goals); personal health records and secure messaging | Ontario, Canada | Person-centered health care warrants that patient care is directed toward capable people based on their preferences, needs, and values. Understand how a new multicomponent care program improves the quality of primary care. | The program was a valuable tool for assessments, seminars, and an interdisciplinary approach to care. How the information was shared, and the kind of benefit that could be expected were unclear. |
| S29 | Pownall et al., 2019 [74] | Qual | Care home staff, nursing, care assistant team, and catering staff, n = 37; care home managers, n = 4; quality managers, n = 4; residents, n = 6 | Tablet computer, software (education and monitoring application for staff for patient dysphagia) | England | Dysphagia (difficulty or discomfort in swallowing) is a risk factor for poor nutrition among older adults, but optimizing support for nursing home residents can be challenging. Evaluate use of a digital dysphagia guide in care homes. Data are based on a consensus from interviews and focus groups on prioritizing the need for information and exploring the acceptance of an education tool for care workers. | A tablet-based digital guide to dysphagia provides care homes with an applied, interactive, work-based approach to education and training of the entire workforce. Videos, text, and photos were valuable for addressing different learning styles. A resource accessible in snips of learning addresses a range of learning styles. The flexibility of computer-based content in real-time enhances knowledge and skill development for caregivers. |
| S30 | Qian & Gui, 2020 [75] | Quant | Age 60 years and older, n = 14,933; website posts | Website resource (development of senior online communities) (SOCs) | Wuhan, China | This study identified the health information needs of SOC users to help improve health information services for older adults. Three research questions were asked: (1) What type of health information is discussed in SOCs? (2) Based on the health information that users post in SOCs, do their health information needs change over time (including preference for traditional Chinese medicine (TCM) vs. Western medicine)? (3) How popular are different types of health information posted in SOCs? | Four types of health information were provided: “coping with aging, dietary nutrition, physical exercise, and mental health”. Older users reported comprehensive needs that involve various health issues, with the main concern being physical health. A larger number of posts were related to Western medicine than to TCM. Posts related to TCM mainly were associated with the categories “coping with aging” and “physical exercise”, whereas the proportion of “dietary nutrition” posts related to TCM was lower. Related to the category “dietary nutrition”, terms that came up in SOCs were “vitamins, fats, and proteins”, indicating that older adults may focus on problems with a healthy diet. |
| S31 | Recio-Rodríguez et al., 2019 [76] | FRD | Age 65–80 years, n = 160 | Smartphone, fitness device, software (activity and diet (Intellectual Property Registry No. 00/2017/2438)). | Spain | Evaluate the effectiveness of the combined use of smartphone and smart band technology for three months combined with counseling (intervention) vs. counseling alone (control) to increase physical activity levels and adherence to the Mediterranean diet. Assess the effect of the two interventions on body composition, cognitive performance, quality of life, and independence in activities of daily living. | The intervention group was instructed on how to use a smartphone application for three months. The application integrates physical activity information from a fitness bracelet and self-reported daily nutritional intake. Outcomes measured included: change in the number of steps measured with an accelerometer, adherence to the Mediterranean diet, sitting time, body composition, quality of life, cognitive performance, and independence in activities of daily living. All variables were measured at baseline and after three months. At six months, a follow-up telephone call collected dietary and physical activity data. |
| S32 | Roberts et al., 2020 [77] | Qual | Age 60–83 years, n = 11 | Touch screen tablet computer, software (ordering meals, self-monitored dietary intake, and guided nutrition goal setting) | Australia | This research was a sub-study of a feasibility study, with the primary aim to explore patient perceptions and acceptability of a health information technology intervention to improve the dietary intake of patients during hospitalization. | Two main themes emerged. The first theme captured experiences and perceptions of using technology to participate in nutrition care. Patients found the technology useful, valuable, and easy to use, but they valued interactions with staff. The second theme captured the spectrum of patient participation, ranging from learning about nutrition to self-monitoring and evaluating and showing behavior change. Patients enjoyed gaining nutrition awareness and knowledge. Most patients self-monitored food intake and goals being assessed, and some reported changing the foods they ordered based on the information learned. |
| S33 | Scott et al., 2018 [78] | Lit Rev | Older adults | Emerging technology:
| Australia | This study investigated the roles of assistive technology to overcome sarcopenia-related functional decline. Management components included poor strength and mobility and/or supporting health behaviors, including nutrition, which can help prevent sarcopenia progression. | There is limited evidence of the role of assistive technology for persons with sarcopenia. Promising areas for this population include smartphone applications, smart homes, wearables, robotics, and 3D food printers. Assistive technologies may contribute to maintaining adequate nutrition and physical activity, which may slow the condition’s progression. |
| S34 | Sheats et al., 2017 [79] | MM | Mean age 70.8 years (SD 7.7), n = 23 | Tablet computer, software (Discovery tool, application to collect data about aspects of the environment that may facilitate or hinder healthy living) | California, U.S. | The aging US population warrants a better understanding of ecological factors and their impact on older adults’ food environment. The goals of the Food Environment Assessment Study (FEAST) were to: (1) use the Healthy Neighborhood Discovery tool (Discovery tool) to collect data (geocoded photos, audio narratives) about aspects of the participants’ environmental facilitators and barriers to healthy living; food-related behaviors were also assessed and (2) use the findings to advocate for change in partnership with local decision-makers and policymakers. | Access to affordable, healthy food and transportation provided a significant barrier to healthy eating and navigating the local food environment. Participants were trained in advocacy skills and shared findings with relevant policymakers. At months 3, 6, 12, and 24, proximal and distal effects of the community-engagement process were documented and showed individual-, community-, and policy-level impacts. Findings add to the literature on how low-income, racially diverse, older adults are impacted at the individual, social, and environmental levels to access, choose, and purchase healthy foods. Multilevel solutions involving a variety of sectors are needed. |
| S35 | Singer et al., 2018 [80] | INT | Mean age 62.9 years (SD 5.7), n = 15 | Tablet computer, smartphone, fitness device, software (enhancement to existing software (AidcubeTM (www.aidcube.com)) for home exercise, diet, and dietary goals), telephone | San Francisco, California, U.S. | A pilot study to demonstrate feasibility and safety for improving frailty using a targeted two-phase intervention: (1) assessment, training, and baseline exercise prescription and (2) home-based exercise and nutrition recorded with software. | A home-based exercise and nutrition intervention is feasible, safe, and capable of improving frailty in adult candidates for a lung transplant. More than half of the participants improved their frailty scores by the minimum clinically important difference, and an equal number of participants went from frail to not frail. |
| S36 | Takemoto et al., 2018 [81] | COM | Age 65 years and older | Novel hardware and software technology (i.e., mobile devices, sensors, home-based sensors, software (monitoring, games), smartphones, webcams, tablets, telephone) | U.S. | Research focused on how novel technologies are applied with older adults and the many barriers when introducing technology within this demographic. Many technology applications are available to monitor health events and behaviors to aid with the changes associated with aging. | Findings on older adult lifestyle behavior and technology show that research is early and often found only in small pilot studies. More extensive trials are needed to understand better techniques and limitations to address the design of computer-based interventions using technology to assist with and easily collect accurate information about day-to-day quality of life. |
| S37 | Timon et al., 2015 [82] | INT | Study 1, mean age 72.0 years, n = 40; study 2, mean age 75.9 years, n = 18; study 3, mean age 71.8 years, n = 36; total n = 94 | Touch screen computer, software (record dietary intake and photo of food), and webcam | Sheffield and York, England | Many computer-based dietary assessment methods have been designed for children and the general adult population. There is a need for such an appropriately designed technology for older adults. Assess the validity of the Novel Assessment of Nutrition and Ageing (NANA) method for dietary recording and assessment in older adults using a touch-screen computer and webcam to understand an appropriate method for tracking nutrition among older adults. | Results indicate that the NANA method is appropriate for assessing dietary intake in older adults. The NANA method compares well with a four-day estimated food diary; potential technology-based food diary intake record for older adults. |
| S38 | van den Helder et al., 2018 [83] | FRD, MM | Age 55 years and older, n = 240 | Tablet computer, software (exercise application) | Amsterdam, Netherlands | An application was developed for a home-based vitamin program using a tablet computer. The study was based on content specific to safe exercise and vitamin and protein intake for older adults. It aimed to understand the impact of home-based exercise and protein intake through a technology tool for community-dwelling older adults. This paper describes the study protocol. | This is the first study to investigate the impact of home-based exercise, protein intake and technology for this population. |
| S39 | van Doorn-van Atten et al., 2019 [84] | INT, MM | Mean age 77.3 years (SD 7.2), n = 76 completers | Tablet computer, computer, software (diet and nutritional questionnaires) | Netherlands | Undernutrition can negatively impact health and quality of life in older adults. Better monitoring of community-dwelling older adults’ nutritional status is needed. Conduct a process evaluation of a multicomponent nutritional telemonitoring intervention. | Eighty percent of participants completed the intervention. Non-completers were older and had worse physical and cognitive functioning. There was better adherence to weight telemonitoring than to telemonitoring using questionnaires. The intervention was well-received by older adults, with high satisfaction; satisfaction was lower among nurses. |
| S40 | van Doorn-van Atten et al., 2018 [85] | INT, FRD | Age 65 years and older, n = 215 | Computer, tablet computer, Bluetooth, TV (Bluetooth-capable), software (diet and nutritional questionnaires) | Netherlands | Older adults are at risk for malnutrition, and there is a need for innovative resources to monitor and improve nutritional status. Describe an intervention study design that uses telemonitoring to improve the nutritional status of community-dwelling older adults. | The six-month intervention was evaluated using a parallel arm pretest. The intervention group received nutritional telemonitoring, television messages, and dietary advice from a nurse or a dietitian. The control group received usual care. Measurements collected at baseline, after 4.5 months, and at completion. Measures included: nutritional status, behavioral determinants, diet quality, appetite, body weight, physical activity, physical functioning, and quality of life. A process evaluation assessed delivery, feasibility, and acceptability. |
| S41 | van Doorn-van Atten et al., 2019 [40] | MM | Mean age 77.4 years (SD 9.3), n = 11 | Computer, tablet computer, TV, TV set-top box, internet, software | Netherlands | Evaluate the feasibility and effectiveness of a three-month telemonitoring intervention to improve community-dwelling older adults’ nutritional status and health outcomes. | This intervention was implemented by researchers and healthcare professionals as intended. Healthcare professionals found the intervention acceptable. Of 20 participants, 9 dropped out. Participant acceptance was low due to low usability of the telemonitoring television channel. Participants had good adherence but needed more help than anticipated with using technology. Compliance with several dietary guidelines was observed. No effects on nutritional status, physical functioning, or quality of life were found. |
| S42 | Ventura Marra et al., 2019 [86] | INT | Intervention group, mean age 58.6 years (SD 8.1), n = 29; enhanced usual care group, mean age 59.3 years (SD 7.4), n = 30; total n = 59 | Telehealth via internet videoconferencing and telephone (registered dietitian nutritionist) | U.S. | Overweight and obesity negatively impact health status, functionality, and quality of life of adults and older adults. Weight loss interventions have been predominantly conducted among women, and accessing nutrition services in rural communities can be challenging. Evaluate the feasibility and effectiveness of a 12-week primary care-referred telenutrition weight loss intervention. | Both groups saw a significant reduction in body weight, waist circumference, body fat percentage, calorie intake, and improved diet quality. After controlling for time, no difference was seen between groups. At 12 weeks, a more significant proportion of participants in the intervention group had lost at least 5% of their baseline weight than the enhanced usual care group. Retention rates and participant-reported satisfaction and adherence were greater than 80% in the telenutrition group. A larger trial over a more extended period is warranted. |
| S43 | Ward et al., 2019 [87] | MM | Age 67–77 years, n = 282 | Computer, tablet computer, internet, software (Myfood24, online 24 h dietary recall application, (www.myfood24.og)) | U.K. | Collecting accurate dietary assessment data is essential to understand diet–disease associations at different stages of life. Evaluate the feasibility of using Myfood24 as a dietary assessment tool for older adults. | Overall, 67% of participants completed at least one recall, and 48% completed two or more. Participants who completed multiple recalls reported higher self-confidence with technology and received a higher technology readiness score than those who did not complete any recalls. Additional support may be required to obtain multiple dietary recalls in an older adult population. |
| S44 | West et al., 2010 [88] | RCT | Age 55–64 years, 14.4%; age 65–69 years, 32.3%; age 70–74 years, 24.4%; age 75–79 years, 16.6%; age 80 years and older 12.3%; total n = 610 | Telehealth via internet videoconferencing (certified diabetes educator) | Rural upstate New York, U.S. | Understand the use of telemedicine for setting goals to address behavior change; examine progress toward these goals in underserved rural older adults with diabetes. | Telemedicine is an acceptable tool for consistent diabetes education, nutrition counseling, and diabetes monitoring. It offers access to diabetes support, resources, and feedback from the convenience of their home. Overall, 68% of behavioral goals set during the intervention were rated as “met” or “improved”. |
| Hardware | Software | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ID | Study | End-User | Home-Based Sensors | Smart Devices | Mobile Device Sensors | Fitness Devices | Robots or Assistive Robots | Tablet Computer | Desktop or Laptop Computer | Mobile or Smartphone | Telephone | Webcam | Internet Access | Videoconferencing | Applications | Various ICT |
| S1 | Ali et al., 2013 [52] | ART | √ | √ | ||||||||||||
| S2 | Angelini et al., 2016 [53] | SUT PUT | √ | |||||||||||||
| S3 | Astell et al., 2014 [3] | SUT | √ | √ | √ | |||||||||||
| S4 | Aure et al., 2020 [54] | SUT | √ | √ | √ | |||||||||||
| S5 | Batsis et al., 2019 [55] | SUT PUT | √ | √ | ||||||||||||
| S6 | Batsis et al., 2020 [56] | SUT PUT | √ | √ | √ | √ | ||||||||||
| S7 | Beasley et al., 2019 [57] | SUT | √ | √ | ||||||||||||
| S8 | Cabrita et al., 2019 [89] | SUT | √ | √ | √ | √ | ||||||||||
| S9 | Chiu et al., 2019 [58] | SUT | √ | √ | √ | |||||||||||
| S10 | Dugas et al., 2018 [59] | SUT | √ | √ | √ | |||||||||||
| S11 | Espín et al., 2016 [60] | SUT | √ | √ | √ | |||||||||||
| S12 | Farsjø et al., 2019 [23] | SUT PUT | √ | √ | √ | |||||||||||
| S13 | Göransson et al., 2020 [61] | SUT | √ | √ | √ | |||||||||||
| S14 | Hendrie et al., 2017 [62] | ART | √ | |||||||||||||
| S15 | Hermann et al., 2012 [63] | ART | √ | √ | ||||||||||||
| S16 | Kaddachi et al., 2018 [6] | PUT | √ | √ | √ | |||||||||||
| S17 | Kirkpatrick et al., 2017 [64] | PUT | √ | √ | √ | √ | √ | |||||||||
| S18 | LaMonica et al., 2017 [65] | ART | √ | √ | √ | √ | ||||||||||
| S19 | Lete et al., 2020 [66] | PUT | √ | √ | ||||||||||||
| S20 | Lindhardt & Nielsen, 2017 [67] | SUT PUT | √ | √ | √ | |||||||||||
| S21 | Łukasik et al., 2018 [4] | SUT, PUT | √ | |||||||||||||
| S22 | Manea & Wac, 2020 [68] | SUT PUT | √ | |||||||||||||
| S23 | Marshall et al., 2017 [69] | PUT | √ | |||||||||||||
| S24 | Marx et al., 2018 [70] | SUT PUT | √ | √ | ||||||||||||
| S25 | McCabe et al., 2001 [24] | SUT PUT | √ | |||||||||||||
| S26 | McCauley et al., 2019 [71] | PUT | √ | |||||||||||||
| S27 | Moguel et al., 2019 [72] | SUT PUT | √ | √ | √ | √ | √ | √ | ||||||||
| S28 | Ploeg et al., 2019 [73] | PUT SUT | √ | √ | ||||||||||||
| S29 | Pownall et al., 2019 [74] | PUT | √ | √ | ||||||||||||
| S30 | Qian & Gui, 2020 [75] | SUT | √ | |||||||||||||
| S31 | Recio-Rodríguez et al., 2019 [76] | SUT | √ | √ | √ | |||||||||||
| S32 | Roberts et al., 2020 [77] | SUT PUT | √ | √ | ||||||||||||
| S33 | Scott et al., 2018 [78] | SUT | √ | √ | √ | √ | √ | √ | √ | |||||||
| S34 | Sheats et al., 2017 [79] | SUT | √ | √ | ||||||||||||
| S35 | Singer et al., 2018 [80] | SUT PUT | √ | √ | √ | √ | √ | |||||||||
| S36 | Takemoto et al., 2018 [81] | ART | √ | √ | √ | √ | √ | √ | √ | √ | ||||||
| S37 | Timon et al., 2015 [82] | SUT | √ | √ | √ | |||||||||||
| S38 | van den Helder et al., 2018 [83] | SUT | √ | √ | ||||||||||||
| S39 | van Doorn-van Atten et al., 2019 [84] | SUT | √ | √ | √ | |||||||||||
| S40 | van Doorn-van Atten et al., 2018 [85] | SUT | √ | √ | √ | √ | √ | |||||||||
| S41 | van Doorn-van Atten et al., 2019 [40] | SUT | √ | √ | √ | √ | √ | |||||||||
| S42 | Ventura Marra et al., 2019 [86] | SUT | √ | √ | ||||||||||||
| S43 | Ward et al., 2019 [87] | SUT | √ | √ | √ | √ | ||||||||||
| S44 | West et al., 2010 [88] | SUT | √ | |||||||||||||
| Total: | 6 | 6 | 5 | 8 | 2 | 23 | 8 | 8 | 4 | 4 | 10 | 7 | 31 | 4 | ||
| Nutrition Area of Focus | Study Setting | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| ID | Study | Assessment, Monitoring, and/or Tracking | Weight and Body Composition | Nutrition Status | Education/ Counseling | Diet Intake/ Diet Quality | Activities of Daily Living | Acute/Long-Term Care | Community Dwelling |
| S1 | Ali et al., 2019 [52] | √ | √ | ||||||
| S2 | Angelini et al., 2016 [53] | √ | √ | √ frailty | √ | ||||
| S3 | Astell et al., 2014 [3] | √ detect for poor nutrition status to prevent frailty/sarcopenia | √ | √ | |||||
| S4 | Aure et al., 2020 [54] | √ | √ | √ | |||||
| S5 | Batsis et al., 2019 [55] | √ | √ | ||||||
| S6 | Batsis et al., 2020 [56] | √ | √ | √ | √ | ||||
| S7 | Beasley et al., 2019 [59] | √ | √ | √ | √ | ||||
| S8 | Cabrita et al., 2019 [89] | √ | √ | ||||||
| S9 | Chiu et al., 2019 [58] | √ | √ | ||||||
| S10 | Dugas et al., 2018 [59] | √ | √ | √ | √ | ||||
| S11 | Espín et al., 2018 [60] | √ | √ | √ | √ | √ | |||
| S12 | Farsjø et al., 2019 [23] | √ | √ | √ | √ | √ | √ | ||
| S13 | Göransson et al., 2020 [61] | √ | √ | √ | √ | ||||
| S14 | Hendrie et al., 2017 [62] | √ | √ | ||||||
| S15 | Hermann et al., 2012 [63] | √ | √ | √ | |||||
| S16 | Kaddachi et al., 2018 [6] | √ | √ | √ | |||||
| S17 | Kirkpatrick et al., 2017 [64] | √ | √ | √ | |||||
| S18 | LaMonica et al., 2017 [65] | √ | √ | √ | |||||
| S19 | Lete et al., 2020 [66] | √ | √ | √ | √ | ||||
| S20 | Lindhardt & Nielsen, 2017 [67] | √ | √ | √ | √ | √ | √ | ||
| S21 | Łukasik et al., 2018 [4] | √ | √ | √ | √ | √ | |||
| S22 | Manea & Wac, 2020 [68] | √ | √ | ||||||
| S23 | Marshall et al., 2017 [69] | √ | √ | √ | |||||
| S24 | Marx et al., 2018 [70] | √ | √ | ||||||
| S25 | McCabe et al., 2001 [24] | √ | √ | √ | |||||
| S26 | McCauley et al., 2019 [71] | √ | √ | ||||||
| S27 | Moguel et al., 2019 [72] | √ | |||||||
| S28 | Ploeg et al., 2019 [73] | √ | √ | √ | |||||
| S29 | Pownall et al., 2019 [74] | √ | √ hydration | √ | |||||
| S30 | Qian & Gui, 2020 [75] | √ | √ | ||||||
| S31 | Recio-Rodríguez et al., 2019 [76] | √ | √ | √ | |||||
| S32 | Roberts et al., 2020 [77] | √ screening | √ | √ | √ | √ | |||
| S33 | Scott et al., 2018 [78] | √ | √ sarcopenia | √ | √ | √ | |||
| S34 | Sheats et al., 2017 [79] | √environment | √ | ||||||
| S35 | Singer et al., 2018 [80] | √ frailty | √ | √ | |||||
| S36 | Takemoto et al., 2018 [81] | √ | √ | √ | √ | √ hydration | √ | ||
| S37 | Timon et al., 2015 [82] | √ | √ | √ | |||||
| S38 | van den Helder et al., 2018 [83] | √ | √ | √ | √ | ||||
| S39 | van Doorn-van Atten et al., 2019 [84] | √ | √ | √ | √ | √ | |||
| S40 | van Doorn-van Atten et al., 2018 [85] | √ | √ | √ | √ | √ | √ | ||
| S41 | van Doorn-van Atten et al., 2019 [40] | √ | √ | √ | √ | √ | √ | ||
| S42 | Ventura Marra et al., 2019 [86] | √ | √ | √ | √ | ||||
| S43 | Ward et al., 2019 [87] | √ | √ | ||||||
| S44 | West et al., 2010 [88] | √ | √ | √ | √ | ||||
| Total: | 27 | 13 | 13 | 27 | 23 | 6 | 3 | 41 | |
3. Results
3.1. Study Characterization
3.2. Participant Characterization
3.3. Technology Characterization
3.4. Nutrition Focus Characterization
4. Discussion
4.1. Software Applications Dominance
4.2. Tablet Computers Dominance
4.3. Notable Mention Technologies
5. Implications
Implications for Practical Utility and Effectiveness
6. Future Research and Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World’s Older Population Grows Dramatically. Available online: www.nih.gov/news-events/news-releases/worlds-older-population-grows-dramatically (accessed on 10 June 2023).
- Anderson, M.; Perrin, A. 10% of Americans Don’t Use the Internet. Who Are They? Pew Research Center. 2019. Available online: https://www.pewresearch.org/fact-tank/2019/04/22/some-americans-dont-use-the-internet-who-are-they/ (accessed on 6 July 2023).
- Astell, A.J.; Hwang, F.; Brown, L.J.E.; Timon, C.; Maclean, L.M.; Smith, T.; Adlam, T.; Khadra, H.; Williams, E.A. Validation of the NANA (Novel Assessment of Nutrition and Ageing) Touch Screen System for Use at Home by Older Adults. Exp. Gerontol. 2014, 60, 100–107. [Google Scholar] [CrossRef]
- Łukasik, S.; Tobis, S.; Wieczorowska-Tobis, K.; Suwalska, A. Could Robots Help Older People with Age-Related Nutritional Problems? Opinions of Potential Users. Int. J. Environ. Res. Public Health 2018, 15, 2535. [Google Scholar] [CrossRef] [PubMed]
- Magsamen-Conrad, K.; Upadhyaya, S.; Joa, C.Y.; Dowd, J. Bridging the Divide: Using UTAUT to Predict Multigenerational Tablet Adoption Practices. Comput. Hum. Behav. 2015, 50, 186–196. [Google Scholar] [CrossRef] [PubMed]
- Kaddachi, F.; Aloulou, H.; Abdulrazak, B.; Fraisse, P.; Mokhtari, M. Long-Term Behavior Change Detection Approach through Objective Technological Observations toward Better Adaptation of Services for Elderly People. Health Technol. 2018, 8, 329. [Google Scholar] [CrossRef]
- Granic, A.; Sayer, A.A.; Robinson, S.M. Dietary Patterns, Skeletal Muscle Health, and Sarcopenia in Older Adults. Nutrients 2019, 11, 745. [Google Scholar] [CrossRef]
- Dorner, B.; Friedrich, E.K. Position of the Academy of Nutrition and Dietetics: Individualized Nutrition Approaches for Older Adults: Long-Term Care, Post-Acute Care, and Other Settings. J. Acad. Nutr. Diet. 2018, 118, 724–735. [Google Scholar] [CrossRef]
- Somers, J.; Worsley, A.; McNaughton, S.A. The Association of Mavenism and Pleasure with Food Involvement in Older Adults. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 60. [Google Scholar] [CrossRef]
- Sahyoun, N.R. Chapter 18: Nutrition and Older Adults. In Nutrition through the Life Cycle; Brown, J., Ed.; Cengage Learning: Boston, MA, USA, 2017; pp. 480–508. [Google Scholar]
- Belsky, D.W.; Caspi, A.; Houts, R.; Cohen, H.J.; Corcoran, D.L.; Danese, A.; Harrington, H.; Israel, S.; Levine, M.E.; Schaefer, J.D.; et al. Quantification of Biological Aging in Young Adults. Proc. Natl. Acad. Sci. USA 2015, 112, E4104–E4110. [Google Scholar] [CrossRef]
- Burton, D.G.A.; Wilmot, C.; Griffiths, H.R. Personalising Nutrition for Older Adults: The InCluSilver Project. Nutr. Bull. 2018, 43, 442–455. [Google Scholar] [CrossRef]
- Crimmins, E.M. Lifespan and Healthspan: Past, Present, and Promise. Gerontologist 2015, 55, 901–911. [Google Scholar] [CrossRef]
- Sowa, A.; Tobiasz-Adamczyk, B.; Topór-Mądry, R.; Poscia, A.; la Milia, D.I. Predictors of Healthy Ageing: Public Health Policy Targets. BMC Health Serv. Res. 2016, 16, 289. [Google Scholar] [CrossRef] [PubMed]
- Reedy, J.; Krebs-Smith, S.M.; Miller, P.E.; Liese, A.D.; Kahle, L.L.; Park, Y.; Subar, A.F. Higher Diet Quality Is Associated with Decreased Risk of All-Cause, Cardiovascular Disease, and Cancer Mortality among Older Adults. J. Nutr. 2014, 144, 881–889. [Google Scholar] [CrossRef] [PubMed]
- Milte, C.M.; Thorpe, M.G.; Crawford, D.; Ball, K.; McNaughton, S.A. Associations of Diet Quality with Health-Related Quality of Life in Older Australian Men and Women. Exp. Gerontol. 2015, 64, 8–16. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Report on Ageing and Health; World Health Organization: Luxembourg, 2015. [Google Scholar]
- Saffel-Shrier, S.; Johnson, M.A.; Francis, S.L. Position of the Academy of Nutrition and Dietetics and the Society for Nutrition Education and Behavior: Food and Nutrition Programs for Community-Residing Older Adults. J. Acad. Nutr. Diet. 2019, 119, 1188–1204. [Google Scholar] [CrossRef]
- Healthy Places Terminology: Aging in Place. Available online: http://www.cdc.gov/healthyplaces/terminology.html (accessed on 8 July 2023).
- The Administration for Community Living. 2020 Profile of Older Americans; The Administration for Community Living: Chicago, IL, USA, 2021.
- Parsons, T.J.; Papachristou, E.; Atkins, J.L.; Papacosta, O.; Ash, S.; Lennon, L.T.; Whincup, P.H.; Ramsay, S.E.; Wannamethee, S.G. Healthier Diet Quality and Dietary Patterns Are Associated with Lower Risk of Mobility Limitation in Older Men. Eur. J. Nutr. 2019, 58, 2335–2343. [Google Scholar] [CrossRef]
- Thomas, K.S. The Relationship between Older Americans Act In-Home Services and Low-Care Residents in Nursing Homes. J. Aging Health 2014, 26, 250–260. [Google Scholar] [CrossRef]
- Farsjø, C.; Kluge, A.; Moen, A. Using a Tablet Application about Nutrition in Home Care—Experiences and Perspectives of Healthcare Professionals. Health Soc. Care Community 2019, 27, 683–692. [Google Scholar] [CrossRef]
- McCabe, B.J.; Copeland, N.P.; Shull, C.A.; Dictson, K.D. Telehealth and Telenutrition: The Use of Interactive Compressed Video for Nutrition Counseling of Rural Elderly. J. Nutr. Elder. 2001, 21, 73–84. [Google Scholar] [CrossRef]
- Goins, R.T.; Williams, K.A.; Carter, M.W.; Spencer, S.M.; Solovieva, T. Perceived Barriers to Health Care Access Among Rural Older Adults: A Qualitative Study. J. Rural Health 2005, 21, 206–213. [Google Scholar] [CrossRef]
- Beelen, J.; Vasse, E.; Ziylan, C.; Janssen, N.; de Roos, N.M.; de Groot, L.C.P.G.M. Undernutrition: Who Cares? Perspectives of Dietitians and Older Adults on Undernutrition. BMC Nutr. 2017, 3, 24. [Google Scholar] [CrossRef]
- Craven, D.L.; Lovell, G.P.; Pelly, F.E.; Isenring, E. Community-Living Older Adults’ Perceptions of Body Weight, Signs of Malnutrition and Sources of Information: A Descriptive Analysis of Survey Data. J. Nutr. Health Aging 2018, 22, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.S.; Payne, L.; Morrison, L.; Green, S.M.; Ghio, D.; Hallett, C.; Parsons, E.L.; Aveyard, P.; Roberts, H.C.; Sutcliffe, M.; et al. Barriers and Facilitators to Screening and Treating Malnutrition in Older Adults Living in the Community: A Mixed-Methods Synthesis. BMC Fam. Pract. 2019, 20, 100. [Google Scholar] [CrossRef]
- Medical Nutrition Therapy. Available online: https://www.medicare.gov/coverage/nutrition-therapy-services (accessed on 19 August 2023).
- National Diabetes Prevention Program. Available online: https://www.cdc.gov/diabetes/prevention/about.htm (accessed on 20 August 2023).
- Abruzzino, B.; Ventura Marra, M. Primary Care Providers’ Perceived Barriers to Referring Patients to Registered Dietitian Nutritionists for Weight Loss Counseling in West Virginia. J. Acad. Nutr. Diet. 2015, 115, A32. [Google Scholar] [CrossRef]
- Hersey, J.C.; Cates, S.C.; Blitstein, J.L.; Kosa, K.M.; Santiago Rivera, O.J.; Contreras, D.A.; Long, V.A.; Singh, A.; Berman, D.A. Eat Smart, Live Strong Intervention Increases Fruit and Vegetable Consumption Among Low-Income Older Adults. J. Nutr. Gerontol. Geriatr. 2015, 34, 66–80. [Google Scholar] [CrossRef] [PubMed]
- Alexander, G.L.; McClure, J.B.; Calvi, J.H.; Divine, G.W.; Stopponi, M.A.; Rolnick, S.J.; Heimendinger, J.; Tolsma, D.D.; Resnicow, K.; Campbell, M.K.; et al. A Randomized Clinical Trial Evaluating Online Interventions to Improve Fruit and Vegetable Consumption. Am. J. Public Health 2010, 100, 319–326. [Google Scholar] [CrossRef]
- Bonilla, C.; Brauer, P.; Royall, D.; Keller, H.; Hanning, R.M.; DiCenso, A. Use of Electronic Dietary Assessment Tools in Primary Care: An Interdisciplinary Perspective. BMC Med. Inform. Decis. Mak. 2015, 15, 14. [Google Scholar] [CrossRef] [PubMed]
- McCarroll, R.; Eyles, H.; Ni Mhurchu, C. Effectiveness of Mobile Health (mHealth) Interventions for Promoting Healthy Eating in Adults: A Systematic Review. Prev. Med. 2017, 105, 156–168. [Google Scholar] [CrossRef]
- Fallahzadeh, R.; Rokni, S.A.; Ghasemzadeh, H.; Soto-Perez-de-Celis, E.; Shahrokni, A. Digital Health for Geriatric Oncology. JCO Clin. Cancer Infor. 2018, 2, 1–12. [Google Scholar] [CrossRef]
- Animireddy, L. Healthy Ageing: An Explorative Study of Key Digital Technology Trends. 2020. Available online: https://www.researchgate.net/profile/Leela-Animireddy/publication/347438382_Healthy_Ageing_An_explorative_study_of_key_digital_technology_trends/links/5fdb874245851553a0c48222/Healthy-Ageing-An-explorative-study-of-key-digital-technology-trends.pdf (accessed on 18 September 2023).
- Pestine-Stevens, A.; Greenfield, E.A. The Need for Community Practice to Support Aging in Place during COVID-19. J. Gerontol. Soc. Work. 2020, 63, 631–634. [Google Scholar] [CrossRef]
- Digital Health. Medical Devices. Available online: https://www.fda.gov/MedicalDevices/DigitalHealth/default.htm (accessed on 6 September 2023).
- Van Doorn-Van Atten, M.N.; Haveman-Nies, A.; Heery, D.; De Vries, J.H.M.; De Groot, L.C.P.G.M. Feasibility and Effectiveness of Nutritional Telemonitoring for Home Care Clients: A Pilot Study. Gerontologist 2019, 59, 158–166. [Google Scholar] [CrossRef]
- Robbins, T.; Hudson, S.; Ray, P.; Sankar, S.; Patel, K.; Randeva, H.; Arvanitis, T.N. COVID-19: A New Digital Dawn? Digit. Health 2020, 6, 2055207620920083. [Google Scholar] [CrossRef] [PubMed]
- FAQs on Telehealth and HIPAA during the COVID-19 Nationwide Public Health Emergency. Available online: https://www.hhs.gov/sites/default/files/telehealth-faqs-508.pdf (accessed on 6 September 2023).
- List of Telehealth Services. Available online: https://www.cms.gov/Medicare/Medicare-general-information/telehealth/telehealth-codes (accessed on 6 September 2023).
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping Studies: Towards a Methodological Framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Grant, M.J.; Booth, A. A Typology of Reviews: An Analysis of 14 Review Types and Associated Methodologies. Health. Inf. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for Conducting Systematic Scoping Reviews. JBI Evid. Synth. 2015, 13, 141–146. [Google Scholar] [CrossRef]
- Research—Association for Information Systems (AIS). Available online: https://aisnet.org/page/SeniorScholarListofPremierJournals (accessed on 1 October 2023).
- Gorman, D.M.; Ferdinand, A.O. High Impact Nutrition and Dietetics Journals’ Use of Publication Procedures to Increase Research Transparency. Res. Integr. Peer. Rev. 2020, 5, 12. [Google Scholar] [CrossRef] [PubMed]
- LoBuono, D.L.; Milovich, M. Technology use in managing the nutrition health of older adults: A scoping review. In Proceedings of the 56th Hawaii International Conference on System Sciences, Maui, HI, USA, 3–6 January 2023; pp. 2901–2910. [Google Scholar]
- Ali, N.M.; Norizan, A.R.; Shahar, S. Enhancing User Interaction in a Nutritional Educational Package for the Elderly Using 3d Animation. J. Theor. Appl. Inf. Technol. 2013, 3, 1323–1330. [Google Scholar]
- Angelini, L.; Carrino, S.; Khaled, O.A.; Riva-Mossman, S.; Mugellini, E. Senior Living Lab: An Ecological Approach to Foster Social Innovation in an Ageing Society. Future Internet 2016, 8, 50. [Google Scholar] [CrossRef]
- Aure, C.F.; Kluge, A.; Moen, A. Promoting Dietary Awareness: Home-Dwelling Older Adults’ Perspectives on Using a Nutrition Application. Int. J. Older People Nurs. 2020, 15, e12332. [Google Scholar] [CrossRef]
- Batsis, J.A.; Naslund, J.A.; Zagaria, A.B.; Kotz, D.; Dokko, R.; Bartels, S.J.; Carpenter-Song, E. Technology for Behavioral Change in Rural Older Adults with Obesity. J. Nutr. Gerontol. Geriatr. 2019, 38, 130–148. [Google Scholar] [CrossRef] [PubMed]
- Batsis, J.A.; Dokko, R.; Naslund, J.A.; Zagaria, A.B.; Kotz, D.; Bartels, S.J.; Carpenter-Song, E. Opportunities to Improve a Mobile Obesity Wellness Intervention for Rural Older Adults with Obesity. J. Community Health 2020, 45, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Beasley, J.M.; Kirshner, L.; Wylie-Rosett, J.; Sevick, M.A.; Deluca, L.; Chodosh, J. BRInging the Diabetes Prevention Program to GEriatric Populations (BRIDGE): A Feasibility Study. Pilot. Feasibility Stud. 2019, 5, 129. [Google Scholar] [CrossRef]
- Chiu, C.-J.; Kuo, S.-E.; Lin, D.-C. Technology-Embedded Health Education on Nutrition for Middle-Aged and Older Adults Living in the Community. Glob. Health Promot. 2019, 26, 80–87. [Google Scholar] [CrossRef]
- Dugas, M.; Crowley, K.; Gao, G.G.; Xu, T.; Agarwal, R.; Kruglanski, A.W.; Steinle, N. Individual Differences in Regulatory Mode Moderate the Effectiveness of a Pilot mHealth Trial for Diabetes Management among Older Veterans. PLoS ONE 2018, 13, e0192807. [Google Scholar] [CrossRef] [PubMed]
- Espín, V.; Hurtado, M.V.; Noguera, M. Nutrition for Elder Care: A Nutritional Semantic Recommender System for the Elderly. Expert Syst. 2016, 33, 201–210. [Google Scholar] [CrossRef]
- Göransson, C.; Wengström, Y.; Hälleberg-Nyman, M.; Langius-Eklöf, A.; Ziegert, K.; Blomberg, K. An App for Supporting Older People Receiving Home Care—Usage, Aspects of Health and Health Literacy: A Quasi-Experimental Study. BMC Med. Inform. Decis. Mak. 2020, 20, 226. [Google Scholar] [CrossRef]
- Hendrie, G.A.; Baird, D.; Golley, R.K.; Noakes, M. The CSIRO Healthy Diet Score: An Online Survey to Estimate Compliance with the Australian Dietary Guidelines. Nutrients 2017, 9, 47. [Google Scholar] [CrossRef]
- Hermann, J.R.; Johnston, J.H.; Brosi, W.A.; Jaco, L. Evaluation of a Cooperative Extension Service Curriculum on Empowering Older Adults with Assistive Technology to Grocery Shop, Prepare Food, and Eat. J. Ext. 2012, 50, 12. [Google Scholar] [CrossRef]
- Kirkpatrick, S.I.; Gilsing, A.M.; Hobin, E.; Solbak, N.M.; Wallace, A.; Haines, J.; Mayhew, A.J.; Orr, S.K.; Raina, P.; Robson, P.J.; et al. Lessons from Studies to Evaluate an Online 24-Hour Recall for Use with Children and Adults in Canada. Nutrients 2017, 9, 100. [Google Scholar] [CrossRef]
- LaMonica, H.M.; English, A.; Hickie, I.B.; Ip, J.; Ireland, C.; West, S.; Shaw, T.; Mowszowski, L.; Glozier, N.; Duffy, S.; et al. Examining Internet and eHealth Practices and Preferences: Survey Study of Australian Older Adults With Subjective Memory Complaints, Mild Cognitive Impairment, or Dementia. J. Med. Internet Res. 2017, 19, e358. [Google Scholar] [CrossRef] [PubMed]
- Lete, N.; Beristain, A.; García-Alonso, A. Survey on Virtual Coaching for Older Adults. Health Inform. J. 2020, 26, 3231–3249. [Google Scholar] [CrossRef]
- Lindhardt, T.; Nielsen, M.H. Older Patients’ Use of Technology for a Post-Discharge Nutritional Intervention—A Mixed-Methods Feasibility Study. Int. J. Med. Inf. 2017, 97, 312–321. [Google Scholar] [CrossRef] [PubMed]
- Manea, V.; Wac, K. Co-Calibrating Physical and Psychological Outcomes and Consumer Wearable Activity Outcomes in Older Adults: An Evaluation of the coQoL Method. J. Pers. Med. 2020, 10, 203. [Google Scholar] [CrossRef] [PubMed]
- Marshall, S.; Agarwal, E.; Young, A.; Isenring, E. Role of Domiciliary and Family Carers in Individualised Nutrition Support for Older Adults Living in the Community. Maturitas 2017, 98, 20–29. [Google Scholar] [CrossRef]
- Marx, W.; Kelly, J.T.; Crichton, M.; Craven, D.; Collins, J.; Mackay, H.; Isenring, E.; Marshall, S. Is Telehealth Effective in Managing Malnutrition in Community-Dwelling Older Adults? A Systematic Review and Meta-Analysis. Maturitas 2018, 111, 31–46. [Google Scholar] [CrossRef] [PubMed]
- McCauley, S.M.; Mitchell, K.; Heap, A. The Malnutrition Quality Improvement Initiative: A Multiyear Partnership Transforms Care. J. Acad. Nutr. Diet. 2019, 119, S18–S24. [Google Scholar] [CrossRef]
- Moguel, E.; Berrocal, J.; García-Alonso, J. Systematic Literature Review of Food-Intake Monitoring in an Aging Population. Sensors 2019, 19, 3265. [Google Scholar] [CrossRef]
- Ploeg, J.; Valaitis, R.K.; Cleghorn, L.; Yous, M.-L.; Gaber, J.; Agarwal, G.; Kastner, M.; Mangin, D.; Oliver, D.; Parascandalo, F.; et al. Perceptions of Older Adults in Ontario, Canada on the Implementation and Impact of a Primary Care Programme, Health Teams Advancing Patient Experience: Strengthening Quality (Health TAPESTRY): A Descriptive Qualitative Study. BMJ Open 2019, 9, e026257. [Google Scholar] [CrossRef]
- Pownall, S.; Barnett, E.; Skilbeck, J.; Jimenez-Aranda, A.; Fowler-Davis, S. The Development of a Digital Dysphagia Guide with Care Homes: Co-Production and Evaluation of a Nutrition Support Tool. Geriatrics 2019, 4, 48. [Google Scholar] [CrossRef]
- Qian, Y.; Gui, W. Identifying Health Information Needs of Senior Online Communities Users: A Text Mining Approach. Aslib. J. Inf. Manag. 2020, 73, 5–24. [Google Scholar] [CrossRef]
- Recio-Rodríguez, J.I.; Lugones-Sanchez, C.; Agudo-Conde, C.; González-Sánchez, J.; Tamayo-Morales, O.; Gonzalez-Sanchez, S.; Fernandez-Alonso, C.; Maderuelo-Fernandez, J.A.; Mora-Simon, S.; Gómez-Marcos, M.A.; et al. Combined Use of Smartphone and Smartband Technology in the Improvement of Lifestyles in the Adult Population over 65 Years: Study Protocol for a Randomized Clinical Trial (EVIDENT-Age Study). BMC Geriatr. 2019, 19, 19. [Google Scholar] [CrossRef]
- Roberts, S.; Chaboyer, W.; Marshall, A.P. Hospital Patients’ Perceptions of Using a Technology-Based Intervention to Participate in Their Nutrition Care: A Qualitative Descriptive Study. Clin. Nutr. ESPEN 2020, 39, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Scott, R.A.; Callisaya, M.L.; Duque, G.; Ebeling, P.R.; Scott, D. Assistive Technologies to Overcome Sarcopenia in Ageing. Maturitas 2018, 112, 78–84. [Google Scholar] [CrossRef]
- Sheats, J.L.; Winter, S.J.; Romero, P.P.; King, A.C. FEAST: Empowering Community Residents to Use Technology to Assess and Advocate for Healthy Food Environments. J. Urban Health 2017, 94, 180–189. [Google Scholar] [CrossRef] [PubMed]
- Singer, J.P.; Soong, A.; Bruun, A.; Bracha, A.; Chin, G.; Hays, S.R.; Jasleen, K.; Rigler, J.; Golden, J.A.; Greenland, J.R.; et al. A Mobile Health Technology Enabled Home-Based Intervention to Treat Frailty in Adult Lung Transplant Candidates: A Pilot Study. Clin. Transpl. 2018, 32, e13274. [Google Scholar] [CrossRef] [PubMed]
- Takemoto, M.; Manini, T.M.; Rosenberg, D.E.; Lazar, A.; Zlatar, Z.Z.; Das, S.K.; Kerr, J. Diet and Activity Assessments and Interventions Using Technology in Older Adults. Am. J. Prev. Med. 2018, 55, e105–e115. [Google Scholar] [CrossRef]
- Timon, C.M.; Astell, A.J.; Hwang, F.; Adlam, T.D.; Smith, T.; Maclean, L.; Spurr, D.; Forster, S.E.; Williams, E.A. The Validation of a Computer-Based Food Record for Older Adults: The Novel Assessment of Nutrition and Ageing (NANA) Method. Br. J. Nutr. 2015, 113, 654–664. [Google Scholar] [CrossRef]
- Van Den Helder, J.; Van Dronkelaar, C.; Tieland, M.; Mehra, S.; Dadema, T.; Visser, B.; Kröse, B.J.A.; Engelbert, R.H.H.; Weijs, P.J.M. A Digitally Supported Home-Based Exercise Training Program and Dietary Protein Intervention for Community Dwelling Older Adults: Protocol of the Cluster Randomised Controlled VITAMIN Trial. BMC Geriatr. 2018, 18, 183. [Google Scholar] [CrossRef]
- Van Doorn-Van Atten, M.N.; De Groot, L.C.; Romea, A.C.; Schwartz, S.; De Vries, J.H.; Haveman-Nies, A. Implementation of a Multicomponent Telemonitoring Intervention to Improve Nutritional Status of Community-Dwelling Older Adults: A Process Evaluation. Public Health Nutr. 2019, 22, 363–374. [Google Scholar] [CrossRef]
- Van Doorn-Van Atten, M.N.; Haveman-Nies, A.; Pilichowski, P.; Roca, R.; De Vries, J.H.M.; De Groot, C.P.G.M. Telemonitoring to Improve Nutritional Status in Community-Dwelling Elderly: Design and Methods for Process and Effect Evaluation of a Non-Randomized Controlled Trial. BMC Geriatr. 2018, 18, 284. [Google Scholar] [CrossRef]
- Ventura Marra, M.; Lilly, C.L.; Nelson, K.R.; Woofter, D.R.; Malone, J. A Pilot Randomized Controlled Trial of a Telenutrition Weight Loss Intervention in Middle-Aged and Older Men with Multiple Risk Factors for Cardiovascular Disease. Nutrients 2019, 11, 229. [Google Scholar] [CrossRef] [PubMed]
- Ward, H.A.; McLellan, H.; Udeh-Momoh, C.; Giannakopoulou, P.; Robb, C.; Wark, P.A.; Middleton, L. Use of Online Dietary Recalls among Older UK Adults: A Feasibility Study of an Online Dietary Assessment Tool. Nutrients 2019, 11, 1451. [Google Scholar] [CrossRef]
- West, S.P.; Lagua, C.; Trief, P.M.; Izquierdo, R.; Weinstock, R.S. Goal Setting Using Telemedicine in Rural Underserved Older Adults with Diabetes: Experiences from the Informatics for Diabetes Education and Telemedicine Project. Telemed. e-Health 2010, 16, 405–416. [Google Scholar] [CrossRef] [PubMed]
- Cabrita, M.; Tabak, M.; Vollenbroek-Hutten, M.M.R. Older Adults’ Attitudes toward Ambulatory Technology to Support Monitoring and Coaching of Healthy Behaviors: Qualitative Study. JMIR Aging 2019, 2, e10476. [Google Scholar] [CrossRef] [PubMed]
- Lose It! Weight Loss That Fits. Available online: https://www.loseit.com/ (accessed on 1 July 2023).
- Fooducate. Eat Better. Lose Weight. Get Healthy: Fooducate Empowers You to Achieve Your Diet, Health, and Fitness Goals. Available online: http://www.fooducate.com/ (accessed on 8 July 2023).
- MyPlate. Start Simple with MyPlate App. Available online: https://www.myplate.gov/resources/tools/startsimple-myplate-app (accessed on 1 October 2023).
- Hingle, M.; Patrick, H. There Are Thousands of Apps for That: Navigating Mobile Technology for Nutrition Education and Behavior. J. Nutr. Educ. Behav. 2016, 48, 213–218.e1. [Google Scholar] [CrossRef]
- Shriver, B.J.; Roman-Shriver, C.R.; Long, J.D. Technology-Based Methods of Dietary Assessment: Recent Developments and Considerations for Clinical Practice. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 548–551. [Google Scholar] [CrossRef]
- U.S. Health Information Technology for Economic and Clinical Health (HITECH) Act. Title XIII of Division A and Title IV of Division B of the American Recovery and Reinvestment Act of 2009 (ARRA); Pub. L.; 2009. Available online: https://www.hhs.gov/sites/default/files/ocr/privacy/hipaa/understanding/coveredentities/hitechact.pdf (accessed on 11 October 2023).
- US Department of Health and Human Services (HHS). Older Adults: Overview. Healthy People 2030. Available online: https://health.gov/healthypeople/objectives-and-data/browse-objectives/older-adults (accessed on 11 October 2023).
- Nutrition Terminology Reference Manual (eNCPT): Dietetic Language for Nutrition Care. Available online: https://www.eatrightpro.org/practice/practice-resources/telehealth (accessed on 4 August 2023).
- Gjevjon, E.; Øderud, T.; Wensaas, G.; Moen, A. Toward a Typology of Technology Users: How Older People Experience Technology’s Potential for Active Aging. Stud. Health Technol. Inform. 2014, 201, 25–31. [Google Scholar] [CrossRef]
- Vogels, E. Some Digital Divides Persist between Rural, Urban and Suburban America. Pew Research Center. 2021. Available online: https://www.pewresearch.org/fact-tank/2021/08/19/some-digital-divides-persist-between-rural-urban-and-suburban-america/ (accessed on 6 July 2023).
- McKinnon, J.D.; Tracy, R. Pandemic Builds Momentum for Broadband Infrastructure Upgrade. The Wall Street Journal 23 April 2020; p. A5. Available online: https://www.wsj.com/articles/pandemic-builds-momentum-for-broadband-infrastructure-upgrade-11587461400?mod=Searchresults_pos1&page=1 (accessed on 9 August 2021).
- Batsis, J.A.; Daniel, K.; Eckstrom, E.; Goldlist, K.; Kusz, H.; Lane, D.; Loewenthal, J.; Coll, P.P.; Friedman, S.M. Promoting Healthy Aging During COVID-19. J. Am. Geriatr. Soc. 2021, 69, 572–580. [Google Scholar] [CrossRef]
- Stone, W. “Just Cruel”: Digital Race For COVID-19 Vaccines Leaves Many Seniors Behind. NPR 2021. Available online: https://www.npr.org/sections/health-shots/2021/02/04/963758458/digital-race-for-covid-19-vaccines-leaves-many-seniors-behind (accessed on 1 September 2023).
- LoBuono, D.L.; Shea, K.S.; Reed, M.; Tovar, A.; Leedahl, S.N.; Xu, F.; Mahler, L.; Lofgren, I.E. The Facilitators and Barriers to Digital Health for Managing Nutrition in People with Parkinson’s Disease and Their Caregivers: A Formative, Qualitative Study. JNEB 2023, 55, 553–563. [Google Scholar] [CrossRef]
- Grashuis, J.; Skevas, T.; Segovia, M.S. Grocery Shopping Preferences during the COVID-19 Pandemic. Sustainability 2020, 12, 5369. [Google Scholar] [CrossRef]
- Heidenstrøm, N.; Hebrok, M. Towards Realizing the Sustainability Potential within Digital Food Provisioning Platforms: The Case of Meal Box Schemes and Online Grocery Shopping in Norway. Sustain. Prod. Consum. 2021, 29, 831–850. [Google Scholar] [CrossRef]
- Denson, A.C.; Mahipal, A. Participation of the Elderly Population in Clinical Trials: Barriers and Solutions. Cancer Control 2014, 21, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Harper, L.; Ross, J. An Application of Knowles’ Theories of Adult Education to an Undergraduate Interdisciplinary Studies Degree Program. J. Contin. High. Educ. 2011, 59, 161–166. [Google Scholar] [CrossRef]



| Nutrition Journals | IS Journals |
|---|---|
| American Journal of Clinical Nutrition | European Journal of Information Systems |
| Journal of Nutrition Education and Behavior | Information Systems Journal |
| Journal of the Academy of Nutrition and Dietetic | Information Systems Research |
| The Journal of Nutrition | Journal of Association for Information Systems |
| The Journal of Nutrition in Gerontology and Geriatrics | Journal of Information Technology |
| Nutrients | Journal of Management Information Systems |
| Journal of Strategic Information Systems | |
| MIS Quarterly |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
LoBuono, D.L.; Milovich, M., Jr. A Scoping Review of Nutrition Health for Older Adults: Does Technology Help? Nutrients 2023, 15, 4402. https://doi.org/10.3390/nu15204402
LoBuono DL, Milovich M Jr. A Scoping Review of Nutrition Health for Older Adults: Does Technology Help? Nutrients. 2023; 15(20):4402. https://doi.org/10.3390/nu15204402
Chicago/Turabian StyleLoBuono, Dara L., and Michael Milovich, Jr. 2023. "A Scoping Review of Nutrition Health for Older Adults: Does Technology Help?" Nutrients 15, no. 20: 4402. https://doi.org/10.3390/nu15204402