
Interrelationships between Dietary Outcomes, Readmission Rates and Length of Stay in Hospitalised Oncology Patients: A Scoping Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Information Sources and Search Strategy
2.2. Eligibility Criteria and Study Selection
2.3. Synthesis of Results
3. Results
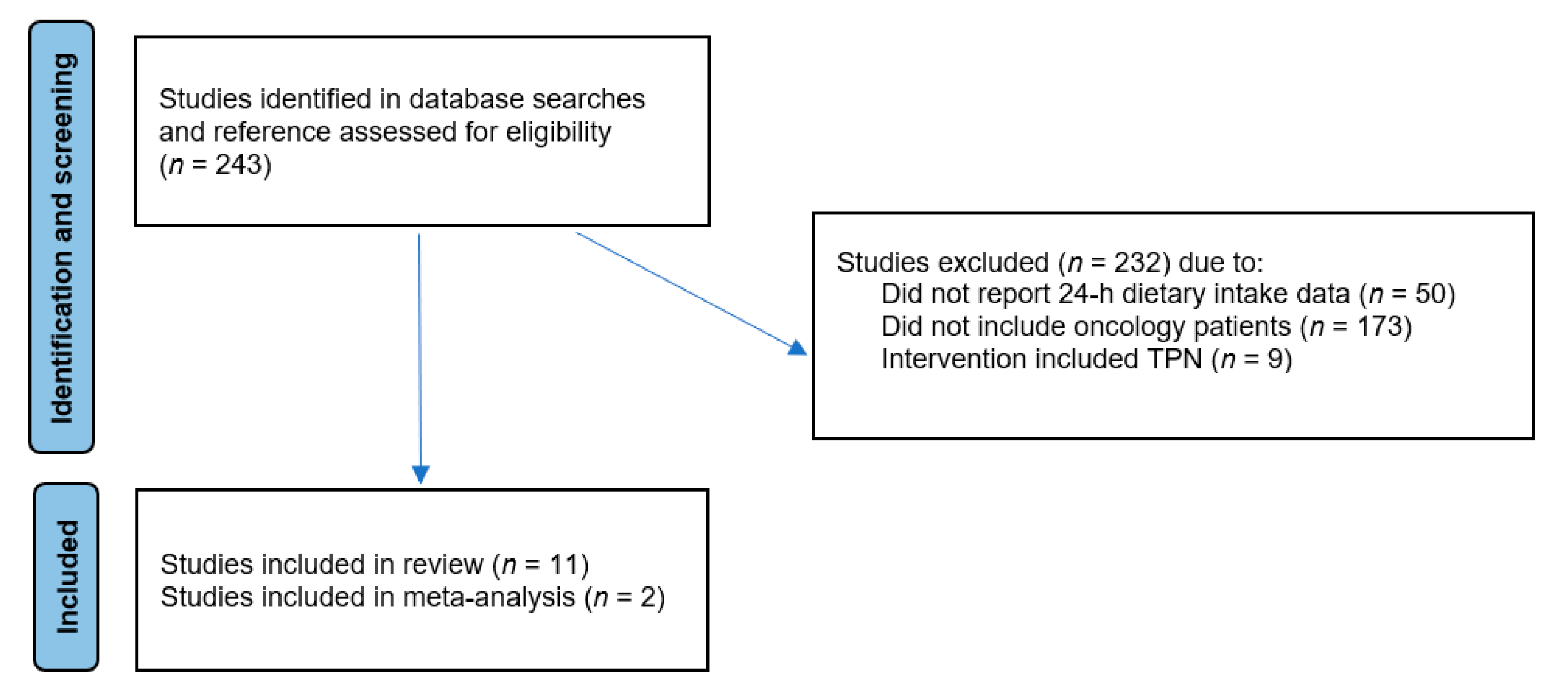
3.1. Study Selection
3.2. Characteristics of Included Studies
3.3. Energy and Protein Intakes
3.4. Length of Stay
3.5. Hospital Readmissions
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maunder, K.; Marshall, K.; Syed, K.; Smilevska, S.; Beck, E.; Mak, M.; Barrington, V. Validation of an electronic food intake tool and its usability and efficacy in the healthcare setting. J. Hum. Nutr. Diet. 2021, 35, 613–620. [Google Scholar] [CrossRef]
- Khorasanchi, A.; Nemani, S.; Pandey, S.; Del Fabbro, E. Managing Nutrition Impact Symptoms in Cancer Cachexia: A Case Series and Mini Review. Front. Nutr. 2022, 9, 831934. [Google Scholar] [CrossRef] [PubMed]
- Ravasco, P. Nutrition in Cancer Patients. J. Clin. Med. 2019, 8, 1211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Fearon, K.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN guidelines on nutrition in cancer patients. Clin. Nutr. 2017, 36, 11–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deftereos, I.; Yeung, J.M.C.; Arslan, J.; Carter, V.M.; Isenring, E.; Kiss, N.; on behalf of The NOURISH Point Prevalence Study Group. Assessment of Nutritional Status and Nutrition Impact Symptoms in Patients Undergoing Resection for Upper Gastrointestinal Cancer: Results from the Multi-Centre NOURISH Point Prevalence Study. Nutrients 2021, 13, 3349. [Google Scholar] [CrossRef] [PubMed]
- Ukovic, B.; Porter, J. Nutrition interventions to improve the appetite of adults undergoing cancer treatment: A systematic review. Support. Care Cancer 2020, 28, 4575–4583. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, I.L. Learned Food Aversions in the Progression of Cancer and Its Treatment. Ann. N. Y. Acad. Sci. 1985, 443, 365–380. [Google Scholar] [CrossRef] [PubMed]
- Boltong, A.; Keast, R. The influence of chemotherapy on taste perception and food hedonics: A systematic review. Cancer Treat. Rev. 2012, 38, 152–163. [Google Scholar] [CrossRef]
- Van der Werf, A.; Arthey, K.; Hiesmayr, M.; Sulz, I.; Schindler, K.; Laviano, A.; Langius, J.; de van der Schueren, M. The determinants of reduced dietary intake in hospitalised colorectal cancer patients. Support. Care Cancer 2018, 26, 2039–2047. [Google Scholar] [CrossRef] [Green Version]
- Ravasco, P.; Monteiro-Grillo, I.; Vidal, P.; Camilo, M. Nutritional Deterioration in Cancer: The Role of Disease and Diet. Clin. Oncol. 2003, 15, 443–450. [Google Scholar] [CrossRef]
- Campos, J.A.D.B.; Da Silva, W.R.; Spexoto, M.C.B.; Serrano, S.V.; Marôco, J. Clinical, dietary and demographic characteristics interfering on quality of life of cancer patients. Einstein 2018, 16, eAO4368. [Google Scholar] [CrossRef] [PubMed]
- Kontogianni, M.D.; Poulia, K.A.; Bersimis, F.; Sulz, I.; Schindler, K.; Hiesmayr, M.; Chourdakis, M. Exploring factors influencing dietary intake during hospitalization: Results from analyzing nutritionDay’s database (2006–2013). Clin. Nutr. ESPEN 2020, 38, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Navarro, D.A.; Boaz, M.; Krause, I.; Elis, A.; Chernov, K.; Giabra, M.; Levy, M.; Giboreau, A.; Kosak, S.; Mouhieddine, M.; et al. Improved meal presentation increases food intake and decreases readmission rate in hospitalized patients. Clin. Nutr. 2016, 35, 1153–1158. [Google Scholar] [CrossRef] [PubMed]
- Sathiaraj, E.; Priya, K.; Chakraborthy, S.; Rajagopal, R. Patient-Centered Foodservice Model Improves Body Weight, Nutritional Intake and Patient Satisfaction in Patients Undergoing Cancer Treatment. Nutr. Cancer 2019, 71, 418–423. [Google Scholar] [CrossRef]
- McCray, S.; Maunder, K.; Barsha, L.; MacKenzie-Shalders, K. Room service in a public hospital improves nutritional intake and increases patient satisfaction while decreasing food waste and cost. J. Hum. Nutr. Diet. 2018, 31, 734–741. [Google Scholar] [CrossRef]
- Cheung, G.; Pizzola, L.; Keller, H. Dietary, Food Service, and Mealtime Interventions to Promote Food Intake in Acute Care Adult Patients. J. Nutr. Gerontol. Geriatr. 2013, 32, 175–212. [Google Scholar] [CrossRef]
- Kiss, N.; Hiesmayr, M.; Sulz, I.; Bauer, P.; Heinze, G.; Mouhieddine, M.; Schuh, C.; Tarantino, S.; Simon, J. Predicting Hospital Length of Stay at Admission Using Global and Country-Specific Competing Risk Analysis of Structural, Patient, and Nutrition-Related Data from nutritionDay 2007–2015. Nutrients 2021, 13, 4111. [Google Scholar] [CrossRef]
- Laky, B.; Janda, M.; Kondalsamy-Chennakesavan, S.; Cleghorn, G.; Obermair, A. Pretreatment malnutrition and quality of life association with prolonged length of hospital stay among patients with gynecological cancer: A cohort study. BMC Cancer 2010, 10, 232. [Google Scholar] [CrossRef] [Green Version]
- Gupta, D.; Vashi, P.G.; Lammersfeld, C.A.; Braun, D.P. Role of Nutritional Status in Predicting the Length of Stay in Cancer: A Systematic Review of the Epidemiological Literature. Ann. Nutr. Metab. 2011, 59, 96–106. [Google Scholar] [CrossRef]
- Bell, J.F.; Whitney, R.L.; Reed, S.C.; Poghosyan, H.; Lash, R.S.; Kim, K.; Davis, A.; Bold, R.J.; Joseph, J.G. Systematic Review of Hospital Readmissions Among Patients With Cancer in the United States. Oncol. Nurs. Forum 2017, 44, 176–191. [Google Scholar] [CrossRef]
- Lai, J.K.; Martin, M.A.; Meyricke, R.; O’Neill, T.; Roberts, S. Factors Associated with Short-term Hospital Readmission Rates for Breast Cancer Patients in Western Australia: An Observational Study. J. Am. Coll. Surg. 2007, 204, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Ghiam, M.K.; Langerman, A.; Sargi, Z.; Rohde, S. Head and Neck Cancer Patients: Rates, Reasons, and Risk Factors for 30-Day Unplanned Readmission. Otolaryngol. Neck Surg. 2018, 159, 149–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muscaritoli, M.; Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN practical guideline: Clinical Nutrition in cancer. Clin. Nutr. 2021, 40, 2898–2913. [Google Scholar] [CrossRef] [PubMed]
- Deftereos, I.; Yeung, J.M.-C.; Arslan, J.; Carter, V.M.; Isenring, E.; Kiss, N.; on behalf of The Nourish Point Prevalence Study Group. Preoperative Nutrition Intervention in Patients Undergoing Resection for Upper Gastrointestinal Cancer: Results from the Multi-Centre NOURISH Point Prevalence Study. Nutrients 2021, 13, 3205. [Google Scholar] [CrossRef] [PubMed]
- Deftereos, I.; Yeung, J.M.; Arslan, J.; Carter, V.M.; Isenring, E.; Kiss, N.; Cardamis, A.; Dorey, A.; Ottaway, A.; Maguire, B.; et al. Adherence to ESPEN guidelines and associations with postoperative outcomes in upper gastrointestinal cancer resection: Results from the multi-centre NOURISH point prevalence study. Clin. Nutr. ESPEN 2022, 47, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [Green Version]
- Deeks, J.J.; Higgins, J.P.T.; Altman, D.G. Chapter 10: Analysing Data and Undertaking Meta-Analyses. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (Updated February 2022); Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: Chichester, UK, 2022; Available online: www.training.cochrane.org/handbook (accessed on 5 December 2022).
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, E.; Ferguson, M.; Banks, M.; Batterham, M.; Bauer, J.; Capra, S.; Isenring, E. Malnutrition and poor food intake are associated with prolonged hospital stay, frequent readmissions, and greater in-hospital mortality: Results from the Nutrition Care Day Survey 2010. Clin. Nutr. 2013, 32, 737–745. [Google Scholar] [CrossRef] [Green Version]
- Sharma, M.; Wahed, S.; O’Dair, G.; Gemmell, L.; Hainsworth, P.; Horgan, A.F. A randomized controlled trial comparing a standard postoperative diet with low-volume high-calorie oral supplements following colorectal surgery. Color. Dis. 2013, 15, 885–891. [Google Scholar] [CrossRef]
- Munk, T.; Beck, A.M.; Holst, M.; Rosenbom, E.; Rasmussen, H.H.; Nielsen, M.A.; Thomsen, T. Positive effect of protein-supplemented hospital food on protein intake in patients at nutritional risk: A randomised controlled trial. J. Hum. Nutr. Diet. 2014, 27, 122–132. [Google Scholar] [CrossRef]
- Calleja Fernández, A.; Pintor de la Maza, B.; Vidal Casariego, A.; Villar Taibo, R.; López Gómez, J.J.; Cano Rodríguez, I.; Bal-lesteros Pomar, M.D. Food intake and nutritional status influence outcomes in hospitalized hematology-oncology patients. Nutr. Hosp. 2015, 31, 2598–2605. [Google Scholar] [CrossRef] [PubMed]
- Maunder, K.; Lazarus, C.; Walton, K.; Williams, P.; Ferguson, M.; Beck, E. Energy and protein intake increases with an electronic bedside spoken meal ordering system compared to a paper menu in hospital patients. Clin. Nutr. ESPEN 2015, 10, e134–e139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villar-Taibo, R.; Calleja-Fernández, A.; Vidal-Casariego, A.; Pintor-De-La-Maza, B.; Álvarez-Del-Campo, C.; Arias-García, R.; Cano-Rodríguez, I.; Ballesteros-Pomar, M.D. A short nutritional intervention in a cohort of hematological inpatients improves energy and protein intake and stabilizes nutritional status. Nutr. Hosp. 2016, 33, 1347–1353. [Google Scholar] [CrossRef] [PubMed]
- Munk, T.; Bruun, N.; Nielsen, M.A.; Thomsen, T. From Evidence to Clinical Practice: Positive Effect of Implementing a Protein-Enriched Hospital Menu in Conjunction With Individualized Dietary Counseling. Nutr. Clin. Pract. 2017, 32, 420–426. [Google Scholar] [CrossRef]
- Yeung, S.E.; Hilkewich, L.; Gillis, C.; Heine, J.A.; Fenton, T.R. Protein intakes are associated with reduced length of stay: A comparison between Enhanced Recovery After Surgery (ERAS) and conventional care after elective colorectal surgery. Am. J. Clin. Nutr. 2017, 106, 44–51. [Google Scholar]
- Ramos Martínez, T.; Villar Taibo, R.; Vidal-Casariego, A.; Pintor-De-La-Maza, B.; Alejo-Ramos, M.; García-Pérez, M.P.; Álvarez-Del-Campo, C.; Cano-Rodríguez, I.; Ballesteros-Pomar, M.D. The appearance of malnutrition in hematological inpatients prolongs hospital stay: The need for nutritional surveillance during hospitalization. Nutr. Hosp. Organo Of. Soc. Esp. Nutr. Parenter. Enter. 2019, 36, 372–378. [Google Scholar] [CrossRef]
- Schuetz, P.; Fehr, R.; Baechli, V.; Geiser, M.; Deiss, M.; Gomes, F.; Kutz, A.; Tribolet, P.; Bregenzer, T.; Braun, N.; et al. Individualised nutritional support in medical inpatients at nutritional risk: A randomised clinical trial. Lancet 2019, 393, 2312–2321. [Google Scholar] [CrossRef]
- Hsieh, L.-C.; Chang, P.-S.; Wu, P.-J.; Huang, Y.-T.; Lin, P.-T. An early moderate recommendation for energy intake based on nutritional status and clinical outcomes in patients with cancer: A retrospective study. Nutrition 2020, 79–80, 110997. [Google Scholar] [CrossRef]
- Deftereos, I.; Kiss, N.; Isenring, E.; Carter, V.M.; Yeung, J.M. A systematic review of the effect of preoperative nutrition support on nutritional status and treatment outcomes in upper gastrointestinal cancer resection. Eur. J. Surg. Oncol. (EJSO) 2020, 46, 1423–1434. [Google Scholar] [CrossRef]
- Feinberg, J.; Nielsen, E.E.; Korang, S.K.; Engell, K.H.; Nielsen, M.S.; Zhang, K.; Didriksen, M.; Lund, L.; Lindahl, N.; Hallum, S.; et al. Nutrition support in hospitalised adults at nutritional risk. Cochrane Database Syst. Rev. 2017, 2017, CD011598. [Google Scholar] [CrossRef]
- Gomes, F.; Baumgartner, A.; Bounoure, L.; Bally, M.; Deutz, N.E.; Greenwald, J.L.; Stanga, Z.; Mueller, B.; Schuetz, P. Association of Nutritional Support with Clinical Outcomes among Medical Inpatients Who Are Malnourished or at Nutritional Risk: An Updated Systematic Review and Meta-analysis. JAMA Netw. Open 2019, 2, e1915138. [Google Scholar] [CrossRef]
- Jeejeebhoy, K.N.; Keller, H.; Gramlich, L.; Allard, J.P.; Laporte, M.; Duerksen, D.R.; Payette, H.; Bernier, P.; Vesnaver, E.; Davidson, B.; et al. Nutritional assessment: Comparison of clinical assessment and objective variables for the prediction of length of hospital stay and readmission. Am. J. Clin. Nutr. 2015, 101, 956–965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leandro-Merhi, V.A.; de Aquino, J.L.B.; Chagas, J.F.S. Nutrition Status and Risk Factors Associated With Length of Hospital Stay for Surgical Patients. J. Parenter. Enter. Nutr. 2010, 35, 241–248. [Google Scholar] [CrossRef]
- Almeida, A.I.; Correia, M.; Camilo, M.; Ravasco, P. Length of stay in surgical patients: Nutritional predictive parameters revisited. Br. J. Nutr. 2012, 109, 322–328. [Google Scholar] [CrossRef] [Green Version]
- Horsley, P.; Bauer, J.; Gallagher, B. Poor nutritional status prior to peripheral blood stem cell transplantation is associated with increased length of hospital stay. Bone Marrow Transplant. 2005, 35, 1113–1116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, M.; Jacobson, T.; Torres, J.; Wann, A. Potential reduction of hospital stay length with outpatient management of low-risk febrile neutropenia in a regional cancer center. Cancer Rep. 2021, 4, e1345. [Google Scholar] [CrossRef]
- Downing, A.; Lansdown, M.; West, R.M.; Thomas, J.D.; Lawrence, G.; Forman, D. Changes in and predictors of length of stay in hospital after surgery for breast cancer between 1997/98 and 2004/05 in two regions of England: A population-based study. BMC Health Serv. Res. 2009, 9, 202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bs, S.K.; Kafle, S.; Earles, J.; Rahmati, R.; Mehra, S.; Judson, B.L. Prolonged inpatient stay after upfront total laryngectomy is associated with overall survival. Laryngoscope Investig. Otolaryngol. 2021, 6, 94–102. [Google Scholar] [CrossRef]
- Rana, R.H.; Alam, K.; Gow, J.; Ralph, N. Predictors of health care use in Australian cancer patients. Cancer Manag. Res. 2019, 11, 6941–6957. [Google Scholar] [CrossRef] [Green Version]
- Loerzel, V.W.; Hines, R.B.; Deatrick, C.W.; Geddie, P.I.; Clochesy, J.M. Unplanned emergency department visits and hospital admissions of older adults under treatment for cancer in the ambulatory/community setting. Support. Care Cancer 2021, 29, 7525–7533. [Google Scholar] [CrossRef]
- Solomon, R.; Egorova, N.; Adelson, K.; Smith, C.B.; Franco, R.; Bickell, N.A. Thirty-Day Readmissions in Patients With Metastatic Cancer: Room for Improvement? J. Oncol. Pract. 2019, 15, e410–e419. [Google Scholar] [CrossRef]
- King, M.; Kerr, A.; Dixon, S.; Taylor, S.; Smith, A.; Merriman, C.; Mitchell, J.; Canavan, J.; Hunter, V. Multicentre review of readmission rates within 30 days of discharge following lung cancer surgery. Br. J. Nurs. 2019, 28, S16–S22. [Google Scholar] [CrossRef]
- Hari, M.; Rosenzweig, M. Incidence of Preventable Postoperative Readmissions Following Pancreaticoduodenectomy: Implications for Patient Education. Oncol. Nurs. Forum 2012, 39, 408–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, M.M.; Orosco, R.K.; Harris, J.P.; Porter, J.B.; Rosenthal, E.L.; Hara, W.; Divi, V. Predictors of readmissions after head and neck cancer surgery: A national perspective. Oral Oncol. 2017, 71, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Sharma, Y.; Miller, M.; Kaambwa, B.; Shahi, R.; Hakendorf, P.; Horwood, C.; Thompson, C. Factors influencing early and late readmissions in Australian hospitalised patients and investigating role of admission nutrition status as a predictor of hospital readmissions: A cohort study. BMJ Open 2018, 8, e022246. [Google Scholar] [CrossRef] [Green Version]
- Burhenn, P.; Sun, C.-L.; Scher, K.S.; Hsu, J.; Pandya, P.; Chui, C.-Y.; Arsenyan, A.; Mitani, D.; Morrison, R.; Katheria, V.; et al. Predictors of hospital readmission among older adults with cancer. J. Geriatr. Oncol. 2020, 11, 1108–1114. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author, Date, Location | Study Design | Population Details | Results |
|---|---|---|---|
| Agarwal et al., (2013) [29] Australia and New Zealand | Multicenter cohort (56 hospitals) Duration: t = 90 days Outcomes: in-hospital mortality, LOS and 30-day readmissions | Total n = 3017 Mean age = 65 ± 18 years 47% female Oncology n = 199 (6.6%) | Longer median LOS for malnourished patients = 15 d vs. 10 d Longer median LOS (2 d) with ≤25% intake LOS = 13 (2–158) d vs. LOS = 11 (2–119) d ≥50% intake (p < 0.0001). Food intake % was not significant Overall HR = 30%, malnourished patients 36% UHR vs. well-nourished patients 30% UHR (p = 0.001). No association between food intake and UHR Oncology HR:_total n = 35 (43%) |
| Sharma et al., (2013) [30] United Kingdom | Single-center, RCT Duration: t = 3.5 years Outcomes: HGS, LOS | Total n = 55 Median age: IG = 61.5 years, CG = 71 years 64% male Oncology: colorectal surgical | Average daily energy intake was higher in the IG: IG = 3421 kJ/d, CG = 2207 kJ/d No difference in average daily protein intakes: IG = 23.25 g/d, CG = 24 g/d No difference in post-operative HGS or bowel activity. Median LOS was shorter in the IG: IG = 6.5 d, CG = 9 d |
| Munk et al., (2014) [31] Denmark | Single-blinded RCT Duration: 18 weeks Secondary outcomes: body weight, HGS, LOS | Total n = 84 at nutritional risk IG: n = 41, CG: n = 40 Mean age = 74 years Oncology n = 29 Orthopedics n = 22 Urology n = 30 | Mean energy intakes were 693 kJ higher in the IG (p = 0.8, not significant), mean energy intake per body weight was 20 kJ/kg significantly higher in IG (p = 0.013) Mean protein intakes were 9.6 d/d in IG (p = 0.011), mean protein intake per body weight was 0.2 g/kg significantly higher in IG (p = 0.003) No significant differences between LOS (mean ± SD) of (15 d ± 10 d) IG vs. (14 d ± 8 d) CG (p = 0.38). |
| Calleja-Fernandez et al., (2015) [32] Spain | Observational cohort study Duration t = 30 days Outcomes: LOS, HR, mortality | Total n = 73 at admission and n = 29 at day 7 (60.3% loss) Mixed cancer patients Observational, no intervention | No significant difference between energy or protein intakes between day 1 and day 7 (p = 0.12) Prevalence of malnutrition was 47.7% HR was greater for malnourished patients (35.1%) than well-nourished (8%) (p = 0.014) |
| Maunder et al., (2015) [33] Australia | Quasi-experimental pre-test, post-test cohort Paper menu (CG) vs. BMOS (IG) Duration: 2 × 48-h periods Secondary Outcomes: LOS | CG: n = 54 (75% response rate) IG: n = 65 (95% response rate) Oncology patients paper = 6, BMOS = 10 Mean age = 65.1 years 64% female | Mean energy intakes increased significantly between the CG = 6273 kJ/day and the IG = 8273 kJ/d (p = 0.000) Mean protein intakes increased significantly between the CG = 66 g/d and the IG = 83 g/d (p = 0.001) Mean LOS was −1 d IG vs. CG (p = 0.01) Mean LOS was 9.8 ± 9.7 d CG vs. 8.5 ± 11.9 d IG |
| Villar-Taibo et al. (2016) [34] Spain | Prospective 2-year study Intervention duration t = 1 week Outcomes: LOS and nutritional status | n = 792 patients screened 37.8% n = 218 at risk Haematology inpatients recruited (83% oncology) Median LOS: 11.5 d | After 7 days intake had increased from 80 to 90% of RDI (p < 0.001) Increase in energy of 407.4 kcal/d and 17.6 g/d protein Median LOS = 11.5 d A trend towards a shorter LOS (3.5–4.5 d fewer) was observed in patients with higher dietary intakes |
| Munk et al., (2017) [35] Denmark | RCT with comparison to a historical intervention group (HIG) Duration: Jan–Aug 2014 Secondary outcomes: HR | Total n = 91, HIC: n = 41, IG: n = 50 Mean age: 74 years 65% female Oncology patients: surgical and non-surgical | Mean energy intake was greater in the IG (6763 kJ/kg) vs. HIG (5814 kJ/kg) (p = 0.001) Mean protein intake was greater in the IG (63 g/kg) vs. HIG (53 g/kg) (p = <0.001) HR did not differ between groups: mean IG: 16 d; HIG: 14 d; no SD reported. |
| Yeung et al. (2017) [36] Canada | Prospective cohort study, 2-centre study Duration: March 2014–April 2015 Outcomes: LOS, HR | CG: n = 46, female 46%, mean age = 57 ± 13 years IG (ERAS): n = 69, female 39%, mean age = 61 ± 14 years Diagnoses: colon cancer, rectal cancer | Total mean protein intakes were higher in the IG (0.54 g/kg/d) compared to the CG (0.33 g/kg/d) (p < 0.02) Oral food intake did not differ between groups IG had shorter LOS 6.5 d vs. 9.7 d CG (p = 0.049) No differences in 30-day HR found (p = 0.31) |
| Ramos-Martinez et al. (2019) [37] Spain | Prospective one-year study (January–December 2016) Secondary Outcomes: LOS, HR | n = 133 well-nourished at admission n = 28 (21%) developed malnutrition during LOS total n = 276 Oncology n = 20 (71.8%) Mean age = 63.4 ± 18.5 years 60.7% male | Energy intakes increased by 623 kg/d after intervention Protein intake increased by 27.3 g/d Long median LOS = 22.5 d in malnourished patients (vs 14 d well-nourished) (p < 0.01) No difference in 30-d HR (p = 0.254) |
| Schuetz et al., (2019) [38] Switzerland | Pragmatic, investigator-initiated, open-label, non-blinded, non-commercial multicenter RCT April 2014-Feb 2018 Outcomes: UHR, LOS | Total n = 2088 CG: n = 1050 (-n = 35), mean age = 72.4 ± 14.1 years cancer n = 201 (20%) IG: n = 1038 (-n = 25), mean age = 72.8 ± 14.2 years Oncology: n = 173 (17%) Expected LOS > 4 days | Energy intakes were higher in the IG (6274 kJ/d) vs. CG (5061 kJ/d) Protein intakes were higher in the IG (57 g/d) vs. CG (47 g/d) No difference in mean ± SD LOS: IG: 9.5 ± 7.0 d vs. CG: 9.6 ± 6.1 d (p = 0.46) No difference in UHR between groups. IG: n = 89 (9%) vs. CG: n = 91 (9%) (p = 0.96) |
| Hsieh et al. (2020) [39] Taiwan | Retrospective study Outcomes: mortality and LOS | n = 111 (57% male) Mean age = 58 years Mixed cancer patients 3 groups based on energy intake IEI: <50% RDI, n = 28 MEI: 50–79% RDI, n = 47 AEI: >80% RDI, n = 36 | Energy intakes increased (p < 0.001) AEI: increased from 6381 to 6588 kJ/kg/d, MEI: increased from 4910 to 5924 kJ/kg/d IEI: increased from 1158 to 4261 kJ/kg/d Protein intakes increased (p < 0.001) AEI: increased from 1.27 to 1.36 g/kg/d MEI: increased from 0.87 to 1.17 g/kg/d IEI: increased from 0.22 to 0.89 g/kg/d LOS was shorter in patients who had adequate intakes (7.9 d) vs. patients who had inadequate intakes (14.7 d) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MacFarling Meure, C.; Steer, B.; Porter, J. Interrelationships between Dietary Outcomes, Readmission Rates and Length of Stay in Hospitalised Oncology Patients: A Scoping Review. Nutrients 2023, 15, 400. https://doi.org/10.3390/nu15020400
MacFarling Meure C, Steer B, Porter J. Interrelationships between Dietary Outcomes, Readmission Rates and Length of Stay in Hospitalised Oncology Patients: A Scoping Review. Nutrients. 2023; 15(2):400. https://doi.org/10.3390/nu15020400
Chicago/Turabian StyleMacFarling Meure, Cecelia, Belinda Steer, and Judi Porter. 2023. "Interrelationships between Dietary Outcomes, Readmission Rates and Length of Stay in Hospitalised Oncology Patients: A Scoping Review" Nutrients 15, no. 2: 400. https://doi.org/10.3390/nu15020400