

Assessing the Hepatic Safety of Epigallocatechin Gallate (EGCG) in Reproductive-Aged Women
 , and
, and
Abstract
:1. Introduction
1.1. Impact of Uterine Fibroids on Female Fertility
1.2. Currently Available Treatment Options for Uterine Fibroids in Women Desiring Future Fertility
1.3. EGCG (Green Tea Extract) and Uterine Fibroids
1.4. Previous EGCG Clinical Trial in Women with Symptomatic Uterine Fibroids
1.5. Green Tea Extracts and Hepatoxicity
1.6. Objective
2. Materials and Methods
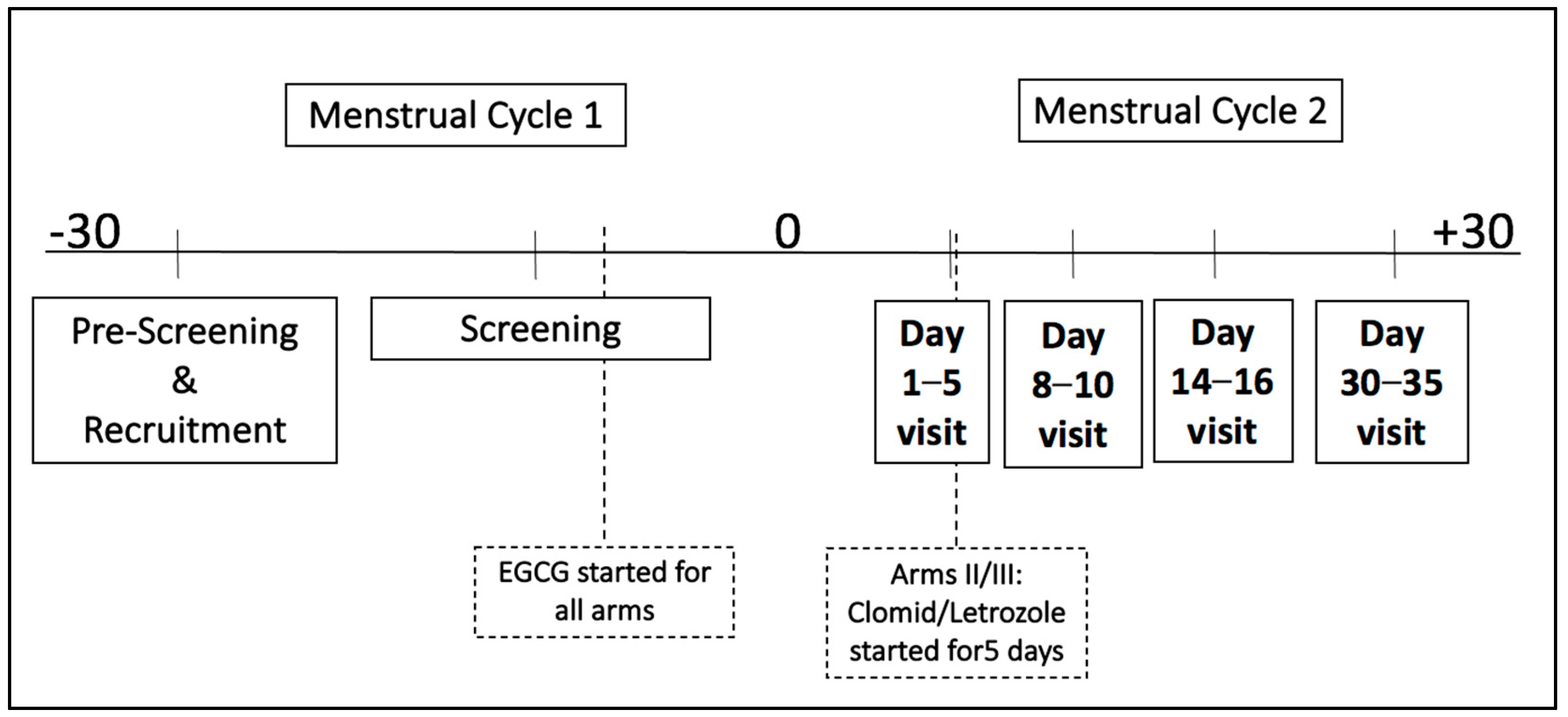
2.1. Study Design
2.2. Inclusion/Exclusion Criteria
2.3. Study Conduct
2.4. Data Management and Statistical Analysis
3. Results and Analysis
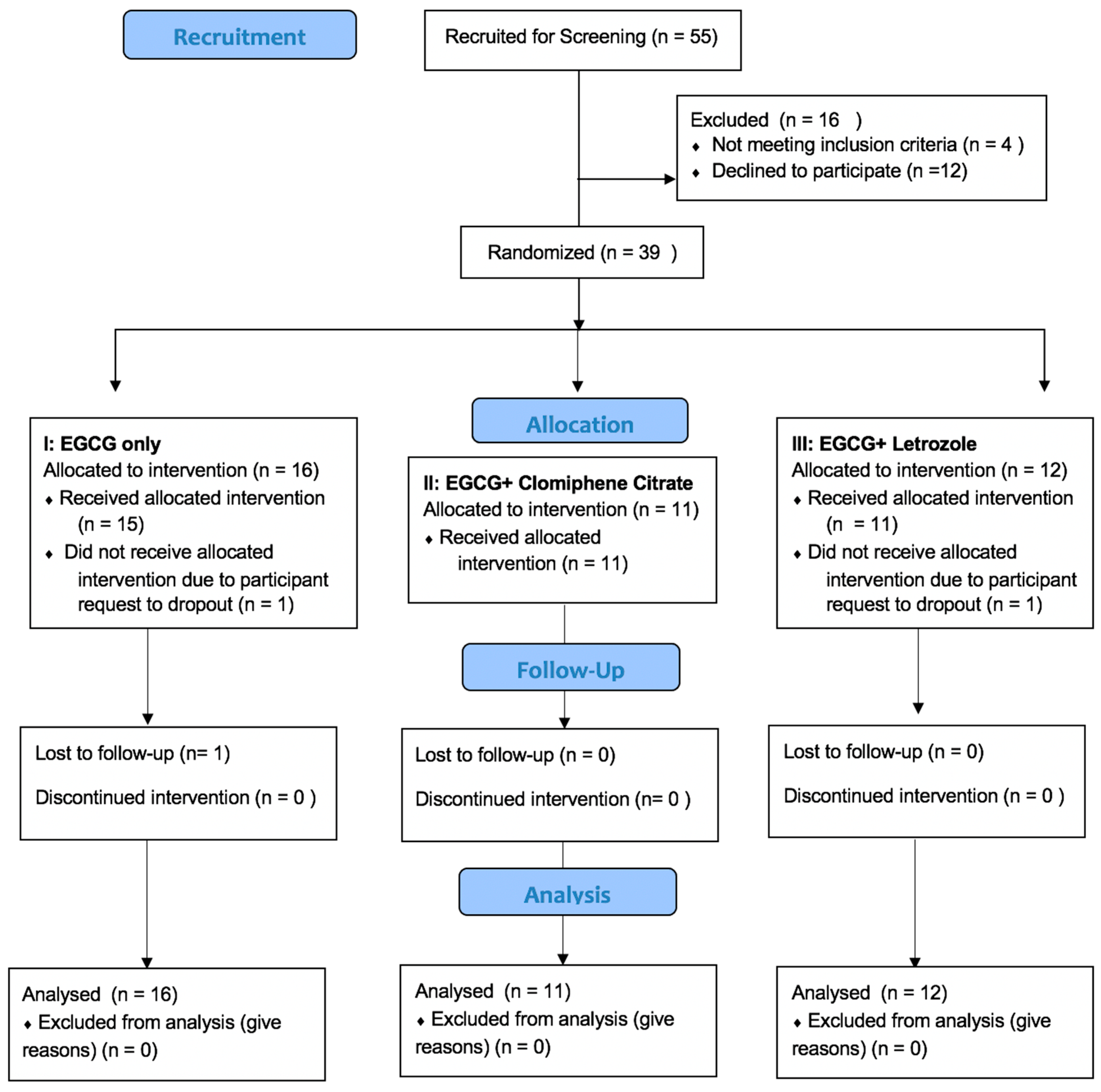
3.1. Participant Disposition
3.2. Demographics
3.3. Adverse Events
3.4. Liver Safety and Folate Levels at the End of the Study
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- ElKafas, H.; Ali, M.; Al-Hendy, A. Leiomyomas. In Encyclopedia of Reproduction; Academic Press: Cambridge, MA, USA, 2018; pp. 101–105. [Google Scholar]
- Whiteman, M.K.; Hillis, S.D.; Jamieson, D.J.; Morrow, B.; Podgornik, M.N.; Brett, K.M.; Marchbanks, P.A. Inpatient hysterectomy surveillance in the United States, 2000–2004. Am. J. Obstet. Gynecol. 2008, 198, 34.e1–34.e7. [Google Scholar] [CrossRef] [PubMed]
- Cardozo, E.R.; Clark, A.D.; Banks, N.K.; Henne, M.B.; Stegmann, B.J.; Segars, J.H. The estimated annual cost of uterine leiomyomata in the United States. Am. J. Obstet. Gynecol. 2012, 206, 211.e1–211.e9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radosa, M.; Owsianowski, Z.; Mothes, A.; Weisheit, A.; Vorwergk, J.; Asskaryar, F.; Camara, O.; Bernardi, T.; Runnebaum, I. Long-term risk of fibroid recurrence after laparoscopic myomectomy. Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 180, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Kotani, Y.; Tobiume, T.; Fujishima, R.; Shigeta, M.; Takaya, H.; Nakai, H.; Suzuki, A.; Tsuji, I.; Mandai, M.; Matsumura, N. Recurrence of uterine myoma after myomectomy: Open myomectomy versus laparoscopic myomectomy. J. Obstet. Gynaecol. Res. 2018, 44, 298–302. [Google Scholar] [CrossRef] [Green Version]
- Marshall, L.M.; Spiegelman, D.; Barbieri, R.L.; Goldman, M.B.; E Manson, J.; Colditz, G.; Willett, W.C.; Hunter, D.J. Variation in the incidence of uterine leiomyoma among premenopausal women by age and race. Obstet. Gynecol. 1997, 90, 967–973. [Google Scholar] [CrossRef]
- Catherino, W.H.; Eltoukhi, H.M.; Al-Hendy, A. Racial and ethnic differences in the pathogenesis and clinical manifestations of uterine leiomyoma. Semin. Reprod. Med. 2013, 31, 370–379. [Google Scholar] [CrossRef] [Green Version]
- Othman, E.E.; Al-Hendy, A. Molecular genetics and racial disparities of uterine leiomyomas. Best Pract. Res. Clin. Obstet. Gynaecol. 2008, 22, 589–601. [Google Scholar] [CrossRef] [Green Version]
- Cook, H.; Ezzati, M.; Segars, J.H.; McCarthy, K. The impact of uterine leiomyomas on reproductive outcomes. Minerva Ginecol. 2010, 62, 225–236. [Google Scholar]
- Guo, X.C.; Segars, J.H. The impact and management of fibroids for fertility: An evidence-based approach. Obstet. Gynecol. Clin. N. Am. 2012, 39, 521–533. [Google Scholar] [CrossRef] [Green Version]
- Divakar, H. Asymptomatic uterine fibroids. Best Pract. Res. Clin. Obstet. Gynaecol. 2008, 22, 643–654. [Google Scholar] [CrossRef]
- Ezzati, M.; Norian, J.M.; Segars, J.H. Management of uterine fibroids in the patient pursuing assisted reproductive technologies. Women’s Health 2009, 5, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Bulletti, C.; De Ziegler, D.; Levi Setti, P.; Cicinelli, E.; Polli, V.; Stefanetti, M. Myomas, pregnancy outcome, and in vitro fertilization. Ann. N. Y. Acad. Sci. 2004, 1034, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Donnez, J.; Jadoul, P. What are the implications of myomas on fertility? A need for a debate? Hum. Reprod. 2002, 17, 1424–1430. [Google Scholar] [CrossRef] [PubMed]
- Segars, J.H.; Parrott, E.C.; Nagel, J.D.; Guo, X.C.; Gao, X.; Birnbaum, L.; Pinn, V.W.; Dixon, D. Proceedings from the third national institutes of health international congress on advances in uterine leiomyoma research: Comprehensive review, conference summary and future recommendations. Hum. Reprod. Update 2014, 20, 309–333. [Google Scholar] [CrossRef]
- Donnez, J.; Dolmans, M.-M. Uterine fibroid management: From the present to the future. Hum. Reprod. Update 2016, 22, 665–686. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.; Al-Hendy, A. Selective progesterone receptor modulators for fertility preservation in women with symptomatic uterine fibroids. Biol. Reprod. 2017, 97, 337–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sangha, R.; Strickler, R.; Dahlman, M.; Havstad, S.; Wegienka, G. Myomectomy to conserve fertility: Seven-year follow-up. J. Obstet. Gynaecol. Can. 2015, 37, 46–51. [Google Scholar] [CrossRef] [Green Version]
- Claeys, J.; Hellendoorn, I.; Hamerlynck, T.; Bosteels, J.; Weyers, S.J.G.S. The risk of uterine rupture after myomectomy: A systematic review of the literature and meta-analysis. Gynecol. Surg. 2014, 11, 197–206. [Google Scholar] [CrossRef] [Green Version]
- Garmi, G.; Goldman, S.; Shalev, E.; Salim, R. The effects of decidual injury on the invasion potential of trophoblastic cells. Obstet. Gynecol. 2011, 117, 55–59. [Google Scholar] [CrossRef]
- Litta, P.; Conte, L.; De Marchi, F.; Saccardi, C.; Angioni, S. Pregnancy outcome after hysteroscopic myomectomy. Gynecol. Endocrinol. 2014, 30, 149–152. [Google Scholar] [CrossRef]
- Seracchioli, R.; Manuzzi, L.; Vianello, F.; Gualerzi, B.; Savelli, L.; Paradisi, R.; Venturoli, S. Obstetric and delivery outcome of pregnancies achieved after laparoscopic myomectomy. Fertil. Steril. 2006, 86, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Kan, Z.; Thompson, H.J.; Ling, T.; Ho, C.T.; Li, D.; Wan, X. Impact of six typical processing methods on the chemical composition of tea leaves using a single Camellia sinensis cultivar, Longjing 43. J. Agric. Food Chem. 2019, 67, 5423–5436. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.; Mukhtar, H. Tea polyphenols for health promotion. Life Sci. 2007, 81, 519–533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navarro, A.; Bariani, M.V.; Yang, Q.; Al-Hendy, A. Understanding the impact of uterine fibroids on human endometrium function. Front. Cell Dev. Biol. 2021, 9, 633180. [Google Scholar] [CrossRef]
- Doherty, L.F.; Taylor, H.S. Leiomyoma-derived transforming growth factor-β impairs bone morphogenetic protein-2-mediated endometrial receptivity. Fertil. Steril. 2015, 103, 845–852. [Google Scholar] [CrossRef] [Green Version]
- Sinclair, D.C.; Mastroyannis, A.; Taylor, H.S. Leiomyoma simultaneously impair endometrial BMP-2-mediated decidualization and anticoagulant expression through secretion of TGF-β3. J. Clin. Endocrinol. Metab. 2011, 96, 412–421. [Google Scholar] [CrossRef] [Green Version]
- Zhang, D.; Al-Hendy, M.; Richard-Davis, G.; Montgomery-Rice, V.; Sharan, C.; Rajaratnam, V.; Khurana, A.; Al-Hendy, A. Green tea extract inhibits proliferation of uterine leiomyoma cells in vitro and in nude mice. Am. J. Obstet. Gynecol. 2010, 202, e1–e289. [Google Scholar] [CrossRef] [Green Version]
- Roshdy, E.; Rajaratnam, V.; Maitra, S.; Sabry, M.; Allah, A.S.; Al-Hendy, A. Treatment of symptomatic uterine fibroids with green tea extract: A pilot randomized controlled clinical study. Int. J. Womens Health 2013, 5, 477–486. [Google Scholar] [CrossRef] [Green Version]
- Johnson, J.J.; Bailey, H.H.; Mukhtar, H. Green tea polyphenols for prostate cancer chemoprevention: A translational perspective. Phytomedicine 2010, 17, 3–13. [Google Scholar] [CrossRef] [Green Version]
- Oketch-Rabah, H.A.; Roe, A.L.; Rider, C.V.; Bonkovsky, H.L.; Giancaspro, G.I.; Navarro, V.; Paine, M.F.; Betz, J.M.; Marles, R.J.; Casper, S.; et al. United States Pharmacopeia (USP) comprehensive review of the hepatotoxicity of green tea extracts. Toxicol. Rep. 2020, 7, 386–402. [Google Scholar] [CrossRef]
- Naumovski, N.; Blades, B.L.; Roach, P.D. Food inhibits the oral bioavailability of the major green tea antioxidant epigallocatechin gallate in humans. Antioxid. Basel 2015, 4, 373–393. [Google Scholar] [CrossRef]
- Frank, J.; George, T.W.; Lodge, J.K.; Rodriguez-Mateos, A.M.; Spencer, J.P.; Minihane, A.M.; Rimbach, G. Daily consumption of an aqueous green tea extract supplement does not impair liver function or alter cardiovascular disease risk biomarkers in healthy men. J. Nutr. 2009, 139, 58–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, B.R.; Yu, C.J.; Chen, W.C.; Lee, H.S.; Chang, H.M.; Lee, Y.C.; Chien, C.T.; Chen, C.F. Green tea extract supplement reduces D-galactosamine-induced acute liver injury by inhibition of apoptotic and proinflammatory signaling. J. Biomed. Sci. 2009, 16, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chow, H.H.; Cai, Y.; Hakim, I.A.; Crowell, J.A.; Shahi, F.; Brooks, C.A.; Dorr, R.T.; Hara, Y.; Alberts, D.S. Pharmacokinetics and safety of green tea polyphenols after multiple-dose administration of epigallocatechin gallate and polyphenon E in healthy individuals. Clin. Cancer Res. 2003, 9, 3312–3319. [Google Scholar] [PubMed]
- Mazzanti, G.; Menniti-Ippolito, F.; Moro, P.A.; Cassetti, F.; Raschetti, R.; Santuccio, C.; Mastrangelo, S. Hepatotoxicity from green tea: A review of the literature and two unpublished cases. Eur. J. Clin. Pharmacol. 2009, 65, 331–341. [Google Scholar] [CrossRef] [Green Version]
- Yu, Z.; Samavat, H.; Dostal, A.M.; Wang, R.; Torkelson, C.J.; Yang, C.S.; Butler, L.M.; Kensler, T.W.; Wu, A.H.; Kurzer, M.S.; et al. Effect of green tea supplements on liver enzyme elevation: Results from a randomized intervention study in the United States. Cancer Prev. Res. 2017, 10, 571–579. [Google Scholar] [CrossRef] [Green Version]
- Sarma, D.N.; Barrett, M.L.; Chavez, M.L.; Gardiner, P.; Ko, R.; Mahady, G.B.; Marles, R.; Pellicore, L.S.; Giancaspro, G.I.; Dog, T.L. Safety of green tea extracts. Drug-Saf. 2008, 31, 469–484. [Google Scholar] [CrossRef]
- ACOG. Updated Cervical Cancer Screening Guidelines. (2021, April). Available online: https://www.acog.org/clinical/clinical-guidance/practice-advisory/articles/2021/04/updated-cervical-cancer-screening-guidelines (accessed on 15 December 2022).
- United States Food and Drug Administration. Drug-Induced Liver Injury Premarketing Clinical Evaluation. 2020. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/drug-induced-liver-injury-premarketing-clinical-evaluation (accessed on 1 December 2020).
- Robles-Diaz, M.; Lucena, M.I.; Kaplowitz, N.; Stephens, C.; Medina-Cáliz, I.; González-Jimenez, A.; Ulzurrun, E.; Gonzalez, A.F.; Fernandez, M.C.; Romero-Gómez, M.; et al. Use of Hy’s law and a new composite algorithm to predict acute liver failure in patients with drug-induced liver injury. Gastroenterology 2014, 147, 109–118. [Google Scholar] [CrossRef] [Green Version]
- Dou, Q.P. Tea in Health and Disease. Nutrients 2019, 11, 929. [Google Scholar] [CrossRef] [Green Version]
- EFSA Panel on Food Additives and Nutrient Sources added to Food (ANS); Younes, M.; Aggett, P.; Aguilar, F.; Crebelli, R.; Dusemund, B.; Filipič, M.; Frutos, M.J.; Galtier, P.; Gott, D.; et al. Scientific opinion on the safety of green tea catechins by panel on food additives nutrient sources added to food. EFSA J. 2018, 16, e05239. [Google Scholar]
- Imai, K.; Nakachi, K. Cross-sectional study of effects of drinking green tea on cardiovascular and liver diseases. BMJ 1995, 310, 693–696. [Google Scholar] [CrossRef] [Green Version]
- Chacko, S.M.; Thambi, P.T.; Kuttan, R.; Nishigaki, I. Beneficial effects of green tea: A literature review. Chin. Med. 2010, 5, 13, Published 2010 Apr 6. [Google Scholar] [CrossRef] [PubMed]
- Katiyar, S.K.; Mukhtar, H. Tea in chemoprevention of cancer: Epidemiologic and experimental studies. Int. J. Oncol. 1996, 8, 221–238. [Google Scholar]
- Dreosti, I.E.; Wargovich, M.J.; Yang, C.S. Inhibition of cancinogenesis by tea: The evidence from experimental studies. Crit. Rev. Food Sci. Nutr. 1997, 37, 761–770. [Google Scholar] [CrossRef]
- Graham, H.N. Green tea composition, consumption, and polyphenol chemistry. Prev. Med. 1992, 21, 334–350. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Jing, X.; Sheng, Y.; Zhang, J.; Hao, Z.; Wang, Z.; Ji, L. (-)-Epicatechin attenuates hepatic sinusoidal obstruction syndrome by inhibiting liver oxidative and inflammatory injury. Redox Biol. 2019, 22, 101117. [Google Scholar] [CrossRef]
- Janle, E.M.; Morré, D.M.; Morré, D.J.; Zhou, Q.; Zhu, Y. Pharmacokinetics of green tea catechins in extract and sustained-release preparations. J. Diet Suppl. 2008, 5, 248–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dostal, A.M.; Samavat, H.; Bedell, S.; Torkelson, C.; Wang, R.; Swenson, K.; Le, C.; Wu, A.H.; Ursin, G.; Yuan, J.M.; et al. The safety of green tea extract supplementation in postmenopausal women at risk for breast cancer: Results of the Minnesota Green Tea Trial. Food Chem. Toxicol. 2015, 83, 26–35. [Google Scholar] [CrossRef] [Green Version]
- ESCO (EFSA Scientific Cooperation). The EFSA Scientific Cooperation Working Group on Botanicals and Botanical Preparations. 2009. Available online: https://www.efsa.europa.eu/en/supporting/pub/rn-280 (accessed on 1 March 2022).
- Moustafa, S.M.; Garneau, A.S.; Goodman, L.R. Elusive effect of endometrial thickness: Through thick and thin. Fertil. Steril. 2021, 115, 89–90. [Google Scholar] [CrossRef]
- Weiss, N.S.; van Vliet, M.N.; Limpens, J.; Hompes, P.G.A.; Lambalk, C.B.; Mochtar, M.H.; van der Veen, F.; Mol, B.W.J.; van Wely, M. Endometrial thickness in women undergoing IUI with ovarian stimulation. How thick is too thin? A systematic review and meta-analysis. Hum. Reprod. 2017, 32, 1009–1018. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| EGCG | EGCG + Clomiphene | EGCG + Letrozole | All | p-Value for Comparison among Three Groups | |
|---|---|---|---|---|---|
| Age (years) | 16 29.6 ± 6.3 28.5 (24.0 to 35.5) | 11 27.2 ± 6.6 28.0 (19.0 to 34.0) | 12 29.3 ± 6.3 27.0 (25.0 to 34.5) | 39 28.8 ± 6.3 28.0 (24.0 to 34.0) | 0.675 |
| BMI (kg/m2) | 16 26.1 ± 6.8 24.3 (22.1 to 29.3) | 11 27.4 ± 5.7 28.3 (22.4 to 31.0) | 12 28.4 ± 9.5 25.0 (22.6 to 30.9) | 39 27.2 ± 7.3 25.0 (22.2 to 30.6) | 0.709 |
| Hip circumference (cm) | 16 112.9 ± 35.1 104.0 (95.5 to 112.5) | 10 103.6 ± 18.1 108.2 (90.0 to 116.0) | 12 106.2 ± 19.4 105.3 (92.0 to 120.0) | 38 108.4 ± 26.6 104.8 (94.0 to 116.0) | 0.946 |
| Waist circumference (cm) | 16 90.7 ± 27.0 80.5 (75.5 to 99.0) | 10 86.0 ± 13.4 89.8 (75.0 to 97.0) | 12 88.6 ± 21.0 88.2 (71.6 to 97.3) | 38 88.8 ± 21.8 84.1 (75.0 to 97.0) | 0.991 |
| Ethnicity | 1.000 | ||||
| Hispanic or Latino | 2/16 (12.5%) | 2/11 (18.2%) | 2/12 (16.7%) | 6/39 (15.4%) | |
| Non-Hispanic | 14/16 (87.5%) | 9/11 (81.8%) | 10/12 (83.3%) | 33/39 (84.6%) | |
| Race | 0.763 | ||||
| White | 11/16 (68.8%) | 6/11 (54.5%) | 6/12 (50.0%) | 23/39 (59.0%) | |
| Black | 2/16 (12.5%) | 2/11 (18.2%) | 1/12 (8.3%) | 5/39 (12.8%) | |
| Asian | 2/16 (12.5%) | 2/11 (18.2%) | 4/12 (33.3%) | 8/39 (20.5%) | |
| Native Hawaiian/Pacific Islander | 1/16 (6.3%) | 0/11 (0.0%) | 0/12 (0.0%) | 1/39 (2.6%) | |
| I prefer not to answer | 0/16 (0.0%) | 1/11 (9.1%) | 1/12 (8.3%) | 2/39 (5.1%) | |
| Have ever been diagnosed with fibroids | 3/16 (18.8%) | 2/11 (18.2%) | 1/12 (8.3%) | 6/39 (15.4%) | 0.742 |
| Have had endometriosis | 1/15 (6.7%) | 0/10 (0.0%) | 0/11 (0.0%) | 1/36 (2.8%) | 1.000 |
| History of smoking | 0.949 | ||||
| Never | 13/16 (81.3%) | 9/10 (90.0%) | 9/11 (81.8%) | 31/37 (83.8%) | |
| Current | 2/16 (12.5%) | 0/10 (0.0%) | 1/11 (9.1%) | 3/37 (8.1%) | |
| Former | 1/16 (6.3%) | 1/10 (10.0%) | 1/11 (9.1%) | 3/37 (8.1%) | |
| History of alcohol use | 0.642 | ||||
| Never | 1/16 (6.3%) | 1/11 (9.1%) | 3/12 (25.0%) | 5/39 (12.8%) | |
| Current | 14/16 (87.5%) | 9/11 (81.8%) | 8/12 (66.7%) | 31/39 (79.5%) |
| EGCG | EGCG + Clomiphene | EGCG + Letrozole | All | p-Value for Comparison among Three Groups | |
|---|---|---|---|---|---|
| ≥1 Adverse events | 2/16 (12.5%) | 4/11 (36.4%) | 6/12 (50.0%) | 12/39 (30.8%) | 0.083 |
| Abdominal discomfort and loose stool | 0/16 (0.0%) | 0/11 (0.0%) | 1/12 (8.3%) | 1/39 (2.6%) | 0.590 |
| Diarrhea | 1/16 (6.3%) | 0/11 (0.0%) | 0/12 (0.0%) | 1/39 (2.6%) | 1.000 |
| Dizziness | 0/16 (0.0%) | 1/11 (9.1%) | 0/12 (0.0%) | 1/39 (2.6%) | 0.282 |
| Facial flushing, muscle ache, and diarrhea after letrozole | 0/16 (0.0%) | 0/11 (0.0%) | 1/12 (8.3%) | 1/39 (2.6%) | 0.590 |
| Greenish discharge | 0/16 (0.0%) | 1/11 (9.1%) | 0/12 (0.0%) | 1/39 (2.6%) | 0.282 |
| Headaches | 1/16 (6.3%) | 0/11 (0.0%) | 0/12 (0.0%) | 1/39 (2.6%) | 1.000 |
| Insomnia | 0/16 (0.0%) | 1/11 (9.1%) | 1/12 (8.3%) | 2/39 (5.1%) | 0.503 |
| Kidney pain | 0/16 (0.0%) | 0/11 (0.0%) | 1/12 (8.3%) | 1/39 (2.6%) | 0.590 |
| Loose stool | 0/16 (0.0%) | 0/11 (0.0%) | 1/12 (8.3%) | 1/39 (2.6%) | 0.590 |
| Low mood | 0/16 (0.0%) | 1/11 (9.1%) | 0/12 (0.0%) | 1/39 (2.6%) | 0.282 |
| Migraine after vaccine | 1/16 (6.3%) | 0/11 (0.0%) | 0/12 (0.0%) | 1/39 (2.6%) | 1.000 |
| Nausea with EGCG | 0/16 (0.0%) | 1/11 (9.1%) | 1/12 (8.3%) | 2/39 (5.1%) | 0.503 |
| Pelvic cramps, dull and intermittent aching after letrozole | 0/16 (0.0%) | 0/11 (0.0%) | 1/12 (8.3%) | 1/39 (2.6%) | 0.590 |
| Vomiting and diarrhea after clomid | 0/16 (0.0%) | 1/11 (9.1%) | 0/12 (0.0%) | 1/39 (2.6%) | 0.282 |
| Arms | Label | Mean | Std Dev | Lower Quartile | Upper Quartile |
|---|---|---|---|---|---|
| EGCG n = 14 | ALT (U/L) | 18.8 | 13.5 | 12.0 | 23.0 |
| AST (U/L) | 19.6 | 6.9 | 15.0 | 25.0 | |
| Direct bilirubin (mg/dL) | 0.2 | 0.1 | 0.1 | 0.2 | |
| Total bilirubin (mg/dL) | 0.5 | 0.6 | 0.2 | 0.4 | |
| Mid-Cycle Endo thickness (mm) | 8.6 | 4.4 | 5.4 | 11.2 | |
| Folate (U/L) | 12.8 | 4.3 | 8.5 | 15.5 | |
| EGCG + Clomiphene n = 11 | ALT (U/L) | 18.6 | 9.6 | 12.0 | 23.0 |
| AST (U/L) | 28.3 | 25.5 | 16.0 | 28.0 | |
| Direct bilirubin (mg/dL) | 0.2 | 0.1 | 0.1 | 0.2 | |
| Total bilirubin (mg/dL) | 0.4 | 0.2 | 0.3 | 0.6 | |
| Mid-Cycle Endo thickness (mm) | 11.1 | 4.0 | 7.8 | 12.0 | |
| Folate (U/L) | 13.6 | 4.9 | 10.1 | 17.9 | |
| EGCG + Letrozole n = 11 | ALT (U/L) | 16.6 | 9.6 | 10.0 | 23.0 |
| AST (U/L) | 18.8 | 4.6 | 15.0 | 23.0 | |
| Direct bilirubin (mg/dL) | 0.2 | 0.1 | 0.1 | 0.2 | |
| Total bilirubin (mg/dL) | 0.5 | 0.4 | 0.3 | 0.6 | |
| Mid-Cycle Endo thickness (mm) | 8.8 | 3.6 | 5.7 | 9.7 | |
| Folate (U/L) | 10.3 | 4.0 | 7.3 | 12.6 |
| EGCG | EGCG + Clomiphene | EGCG + Letrozole | All | p-Value for Comparison among Three Groups | |
|---|---|---|---|---|---|
| Change in ALT/SGPT (U/L) | n = 15 1.1 ± 5.1 | 11 4.4 ± 11.7 | 12 −1.0 ± 7.6 | 38 0.5 ± 8.4 | 0.237 |
| Change in AST/SGOT (U/L) | 15 −3.8 ± 11.0 | 11 7.5 ± 27.9 | 12 −0.5 ± 4.4 | 38 0.5 ± 16.9 | 0.348 |
| Change in direct bilirubin (mg/dL) | 15 0.0 ± 0.1 | 10 −0.1 ± 0.1 | 12 0.0 ± 0.0 | 37 −0.0 ± 0.1 | 0.124 |
| Change in total bilirubin (mg/dL) | 15 0.1 ± 0.2 | 11 −0.0 ± 0.0 | 12 0.0 ± 0.1 | 38 0.0 ± 0.2 | 0.508 |
| Change in folate (ng/mL) | 14 −1.6 ± 4.0 | 10 −3.7 ± 4.3 * | 10 −1.3 ± 3.3 | 34 −2.1 ± 3.9 | 0.716 |
| Change in endometrial thickness from screening to mid-cycle (mm) | 13 −1.9 ± 4.3 | 11 1.4 ± 2.0 | 11 0.6 ± 2.7 | 35 −0.0 ± 3.6 | 0.146 |
| Liver Function Test | Screening (n = 39) | Visit 1 (n = 38) | Visit 2 (n = 36) | Visit 4 (n = 36) |
|---|---|---|---|---|
| ALT or AST ≥ 3×ULN | 0 | 0 | 0 | 0 |
| BILI ≥ 2×ULN | 0 | 0 | 0 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siblini, H.; Al-Hendy, A.; Segars, J.; González, F.; Taylor, H.S.; Singh, B.; Flaminia, A.; Flores, V.A.; Christman, G.M.; Huang, H.; et al. Assessing the Hepatic Safety of Epigallocatechin Gallate (EGCG) in Reproductive-Aged Women. Nutrients 2023, 15, 320. https://doi.org/10.3390/nu15020320
Siblini H, Al-Hendy A, Segars J, González F, Taylor HS, Singh B, Flaminia A, Flores VA, Christman GM, Huang H, et al. Assessing the Hepatic Safety of Epigallocatechin Gallate (EGCG) in Reproductive-Aged Women. Nutrients. 2023; 15(2):320. https://doi.org/10.3390/nu15020320
Chicago/Turabian StyleSiblini, Hiba, Ayman Al-Hendy, James Segars, Frank González, Hugh S. Taylor, Bhuchitra Singh, Ainna Flaminia, Valerie A. Flores, Gregory M. Christman, Hao Huang, and et al. 2023. "Assessing the Hepatic Safety of Epigallocatechin Gallate (EGCG) in Reproductive-Aged Women" Nutrients 15, no. 2: 320. https://doi.org/10.3390/nu15020320